Embed Size (px)
Citation preview
Chest Physiotherapy and Airway Clearance in Pediatrics
Rob DiBlasi RRT-NPS, FAARCProgram Manager Research/QI, Respiratory TherapyPrinciple Investigator, SCRIMarch 22, 2017
Conflict of Interest
I have no real or perceived conflict of interest that relates to this presentation. Any use of brand names is not in any way meant to be an endorsement of a specific product, but to
merely illustrate a point of emphasis.

Objectives
Learning objectives for this presentation:• Discuss different forms of airway clearance
therapies (ACTs) • Review the literature related to the use of
ACTs in pediatric lung disease• Discuss ways to embrace judicious use of
ACTs in patients using evidence-based approaches

Background
Airway Clearance Techniques (ACTs) are used in variety of settings for a variety of clinical ailments:
1) evidence of retained pulmonary secretions 2) weak or ineffective cough 3) focal lung opacity on chest x-ray consistent with mucous plugging and/or atelectasis and 4) intrapulmonary shunt requiring oxygen
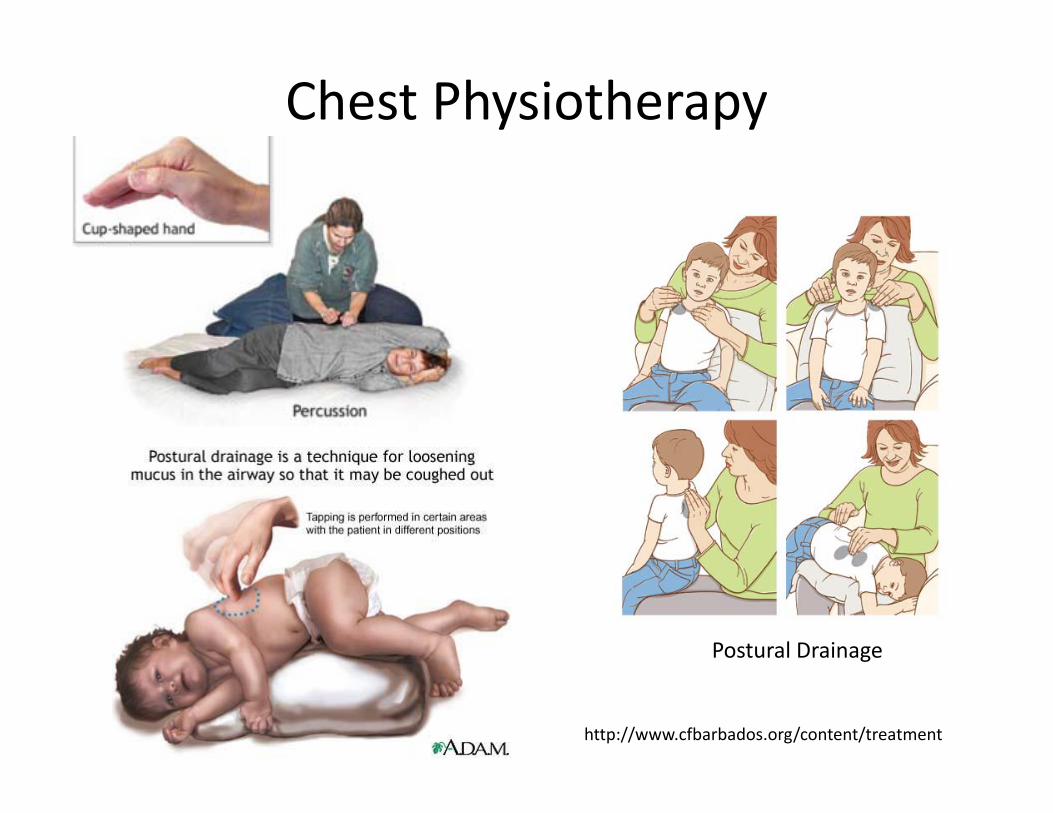
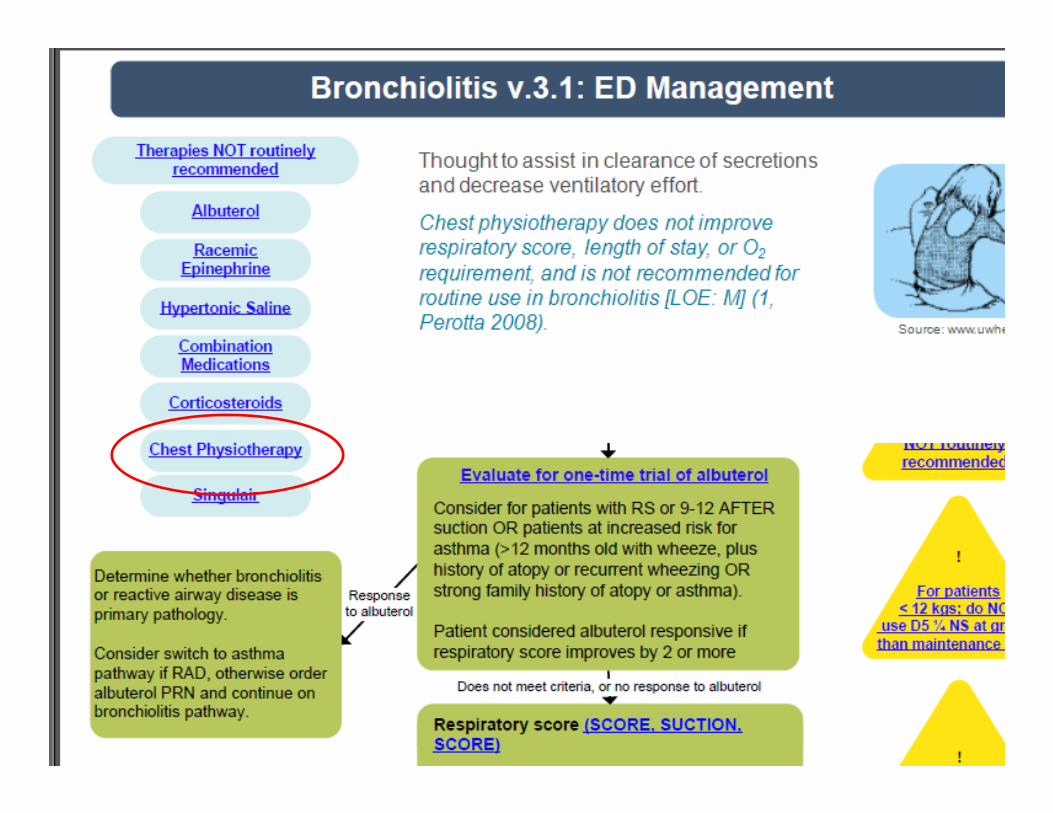
Chest Physiotherapy
Postural Drainage
http://www.cfbarbados.org/content/treatment
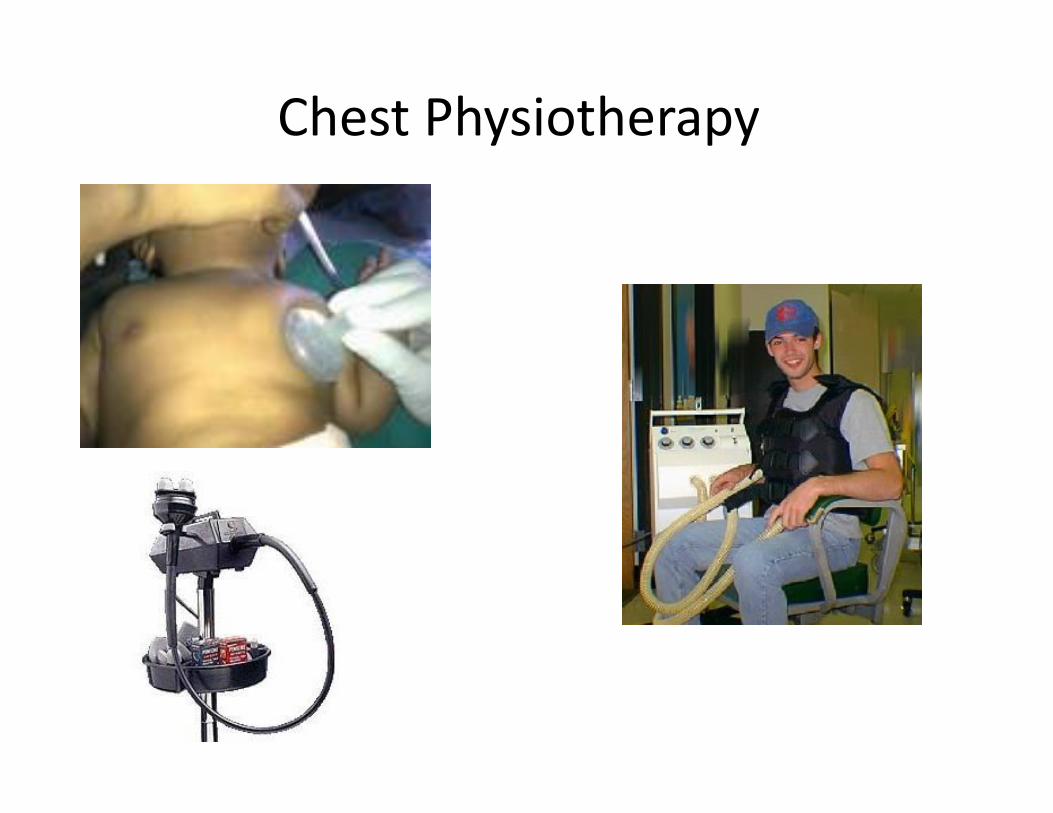
Chest Physiotherapy

Other Airway Clearance Options: ACTs
Therapy Vest
Hand-Held Airway Clearance
Cough Assist
Nasotracheal Sx
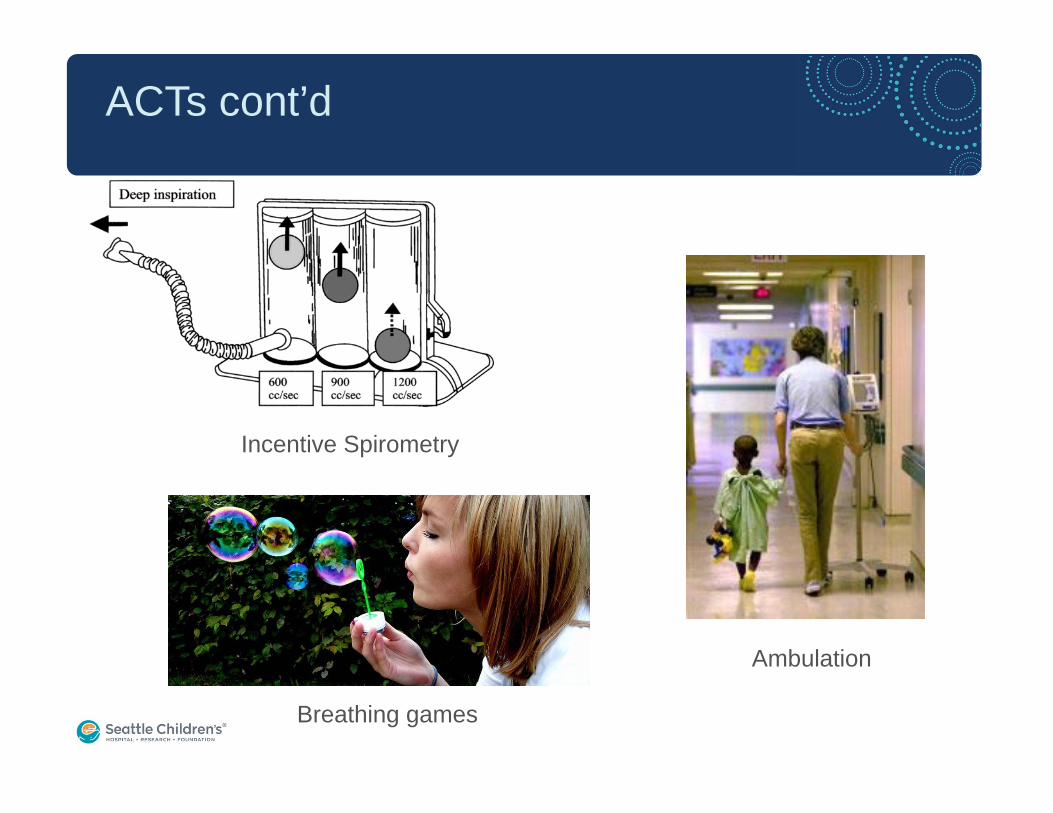
ACTs cont’d
Incentive Spirometry
Ambulation
Breathing games
Literature Search
• ACTs have only been shown to be effective in children with CF, Bronchiectasis and neuromuscular weakness
• Lack of definitive data for ACT for common forms of pediatric respiratory failure• Pneumonia (may cause patients condition to worsen)• Bronchiolitis, asthma, pleural effusion• Prevention of atelectasis
Bronchiolitis
• Systematic review to determine efficacy of CPT in infants with acute viral bronchiolitis <2 years old
• Reviewed improvement in disease severity, LOS, and oxygen use
• Nine clinical trials including 891 participants were included comparing CPT with no intervention
• CPT was not found to improve the severity of the disease, respiratory parameters, or reduce length of hospital stay or oxygen requirements in infants
Roqué i Figuls Chest physiotherapy for acute bronchiolitis in paediatric patients between 0 and 24 months old. Cochrane Database Syst Rev. 2012
Are ACTs a useful option with pneumonia?
Pneumonia
• RCT with children (29 d to 12 y old) hospitalized with acute pneumonia, and compared twice-daily CPT and standard pneumonia therapy (n =51) to standard treatment alone (n =47)• The CPT group had a longer median duration
of coughing (5.0 d vs 4.0 d, P =0.04) and longer duration of rhonchi (median 2.0 d vs 0.5 d, P= 0.03) than the medical treatment only group
Paloudo, Thorax, 2008

ACT in Asthma
• Randomized Placebo Controlled Trial • 38 children aged 6 to 13 years with severe
asthma • 19 children received chest physical therapy
(PT) and 19 children received placebo visits• Lung function at the end of the study was
similar in both groups
Asher I et al., Pediatr Pulmonol, 1990
Can ACT resolve acute lobar atelectasis during mechanical ventilation?
• Larger ventilated patients (Templeton M et al., Intensive Care Med,2007)• CPT may be useful for acute lobar or segmental
atelectasis based on radiographic evidence• Neonates-post-extubation (Flenady et al.,
Cochrane 2002)• No benefit to peri-extubation CPT• No decrease in post-extubation lobar collapse• Lower re-intubation rate in babies treated with CPT
Can CPT and other ACTs prevent atelectasis?
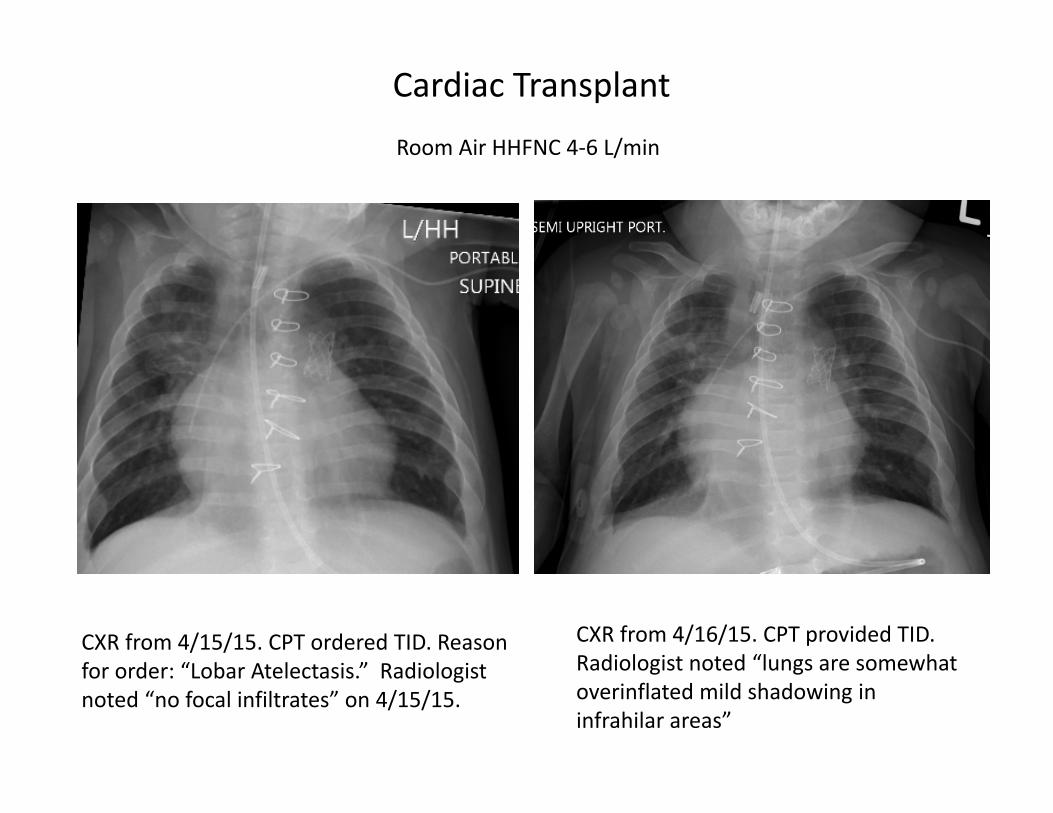
Cardiac Transplant
CXR from 4/15/15. CPT ordered TID. Reason for order: “Lobar Atelectasis.” Radiologist noted “no focal infiltrates” on 4/15/15.
CXR from 4/16/15. CPT provided TID. Radiologist noted “lungs are somewhat overinflated mild shadowing in infrahilar areas”
Room Air HHFNC 4‐6 L/min
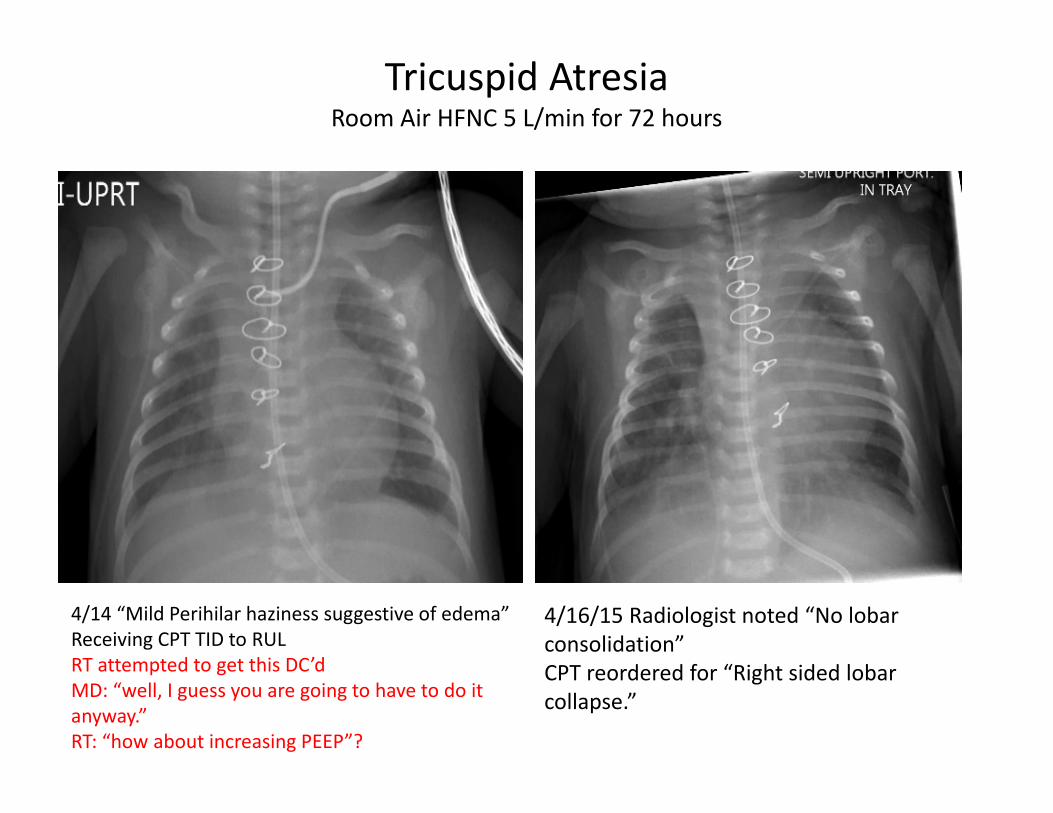
Tricuspid AtresiaRoom Air HFNC 5 L/min for 72 hours
4/14 “Mild Perihilar haziness suggestive of edema” Receiving CPT TID to RULRT attempted to get this DC’dMD: “well, I guess you are going to have to do it anyway.”RT: “how about increasing PEEP”?
4/16/15 Radiologist noted “No lobar consolidation” CPT reordered for “Right sided lobar collapse.”
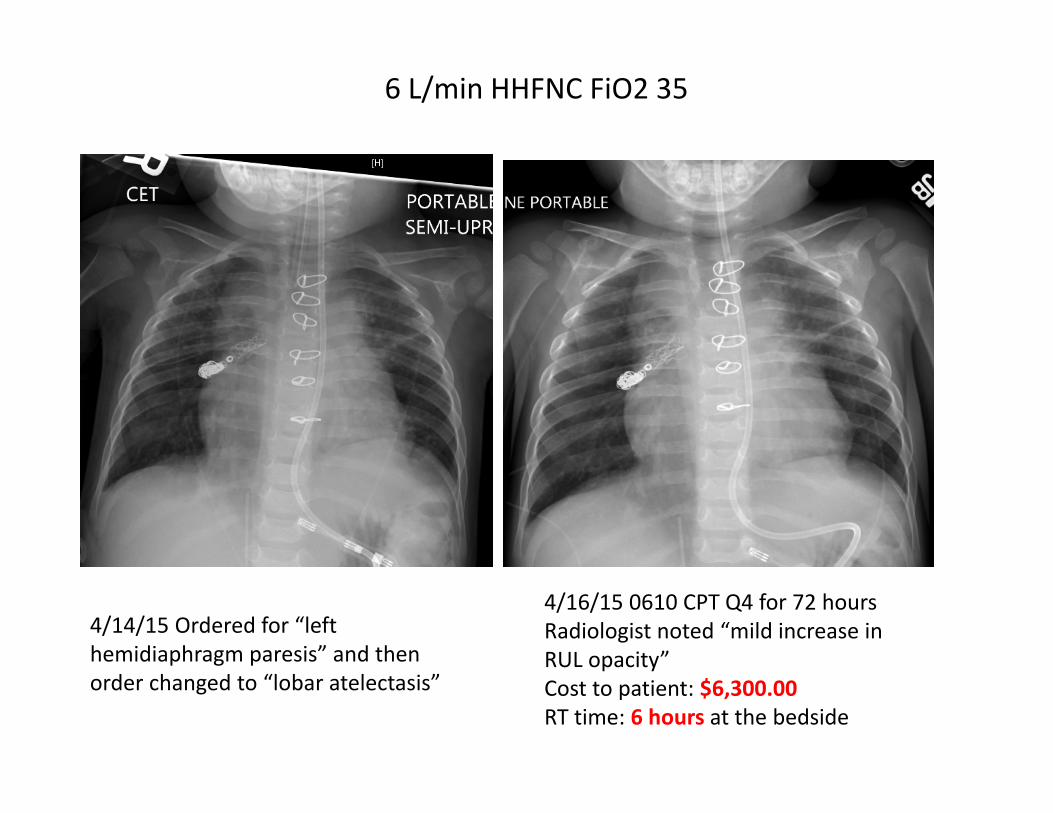
4/16/15 0610 CPT Q4 for 72 hours Radiologist noted “mild increase in RUL opacity”Cost to patient: $6,300.00RT time: 6 hours at the bedside
6 L/min HHFNC FiO2 35
4/14/15 Ordered for “left hemidiaphragm paresis” and then order changed to “lobar atelectasis”
Can ACT prevent lobar atelectasis or VAP?
• Mechanically ventilated adult patients (Chen YC, J Clin Med Assoc, 2009)• No differences in VAP between CPT and no intervention
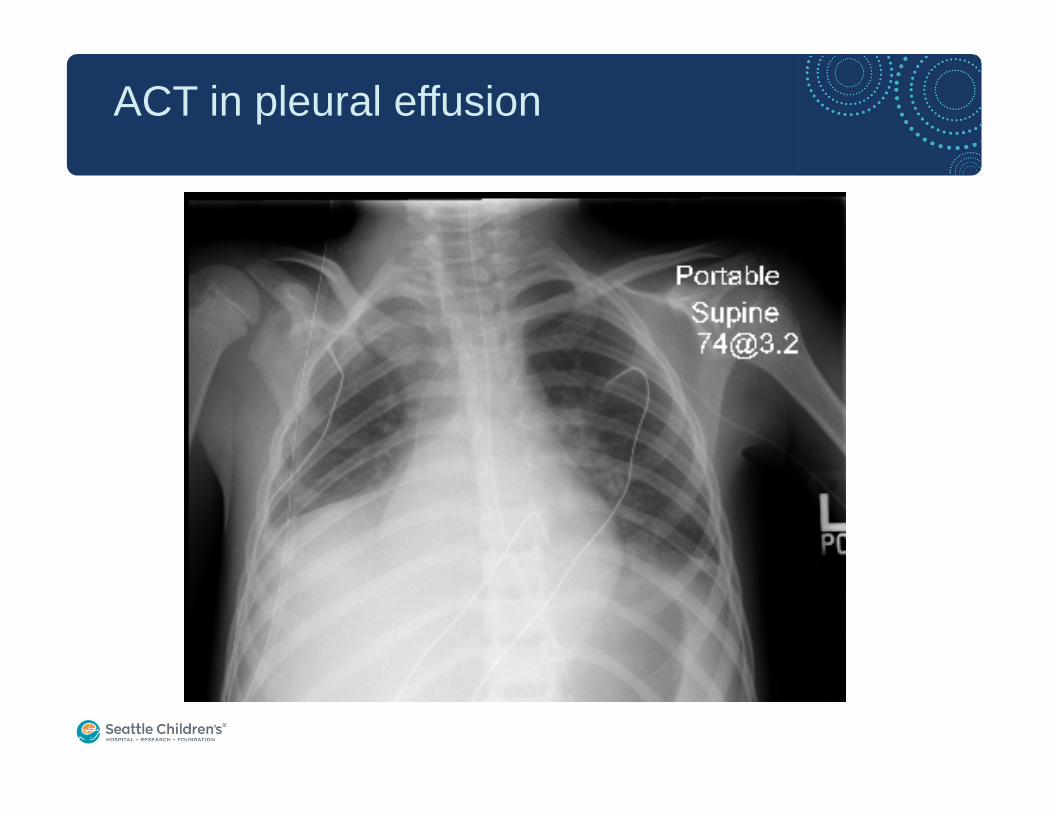
ACT in pleural effusion
Systematic Review
• Included 24 RCTs, seven crossover RCTs, and one prospective cohort study in adults and patients (n=2,453)
• Patients with CF and neuromuscular disease were excluded
• Based on these data, this review found no evidence from RCTs to support the use of CPT or any other form of ACT in adults or pediatrics to:• improve oxygenation, reduce length of time on the ventilator, reduce
stay in the ICU, resolve atelectasis/consolidation, and/or improve respiratory mechanics versus usual care in this population
Andrews et al., Resp Care, 2013
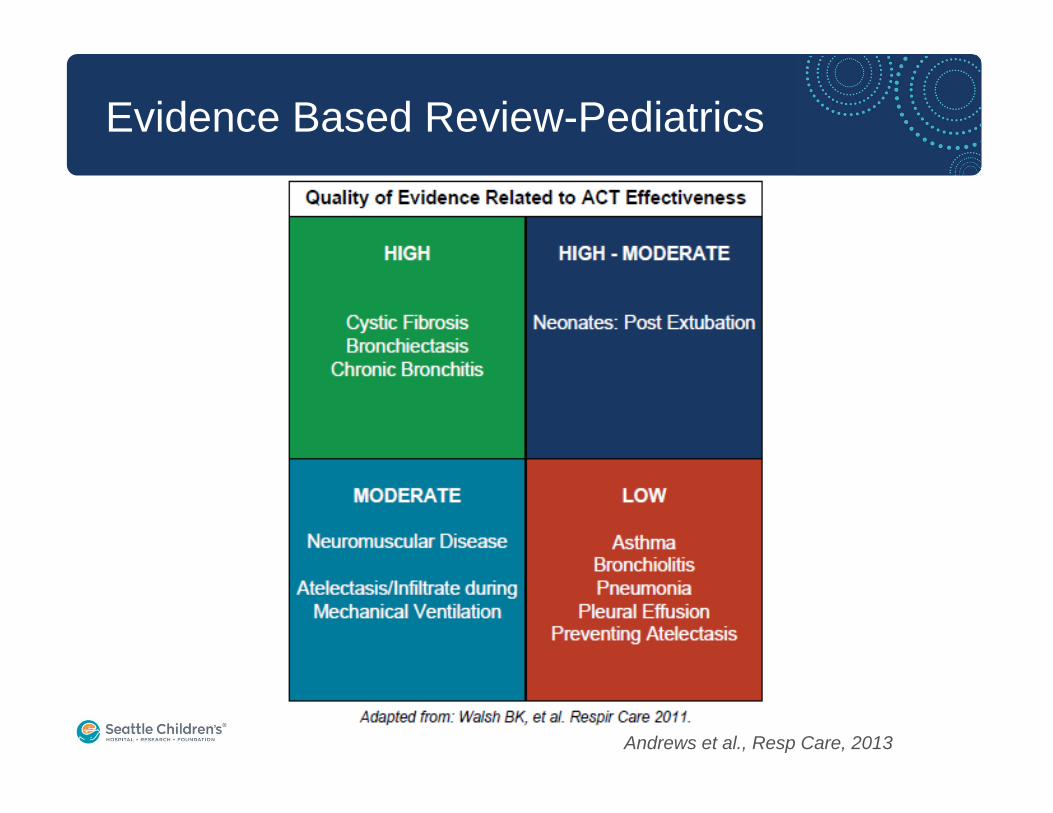
Evidence Based Review-Pediatrics
Andrews et al., Resp Care, 2013

Risks Associated with ACT
• Gastroesophageal reflux (Button BM, Pediatr Res 1994)
• Decreased oxygenation and increased oxygenation requirements (Hough JL, Cochrane, 2008)
• Rib fracture (Purchit DM, Am J Dis Child, 1975)
• Increased intracranial pressure and intracranial bleeding (Harding JE, J Pediatr, 1998)
• Longer duration of fever (Britton S, BMJ, 1985)
• Increased vomiting and respiratory instability (Roque et al., Cochrane, 2012)
• Increased SOB, arrhythmia, bronchospasm, thoracic hematoma (Andrews J, Resp Care, 2013)
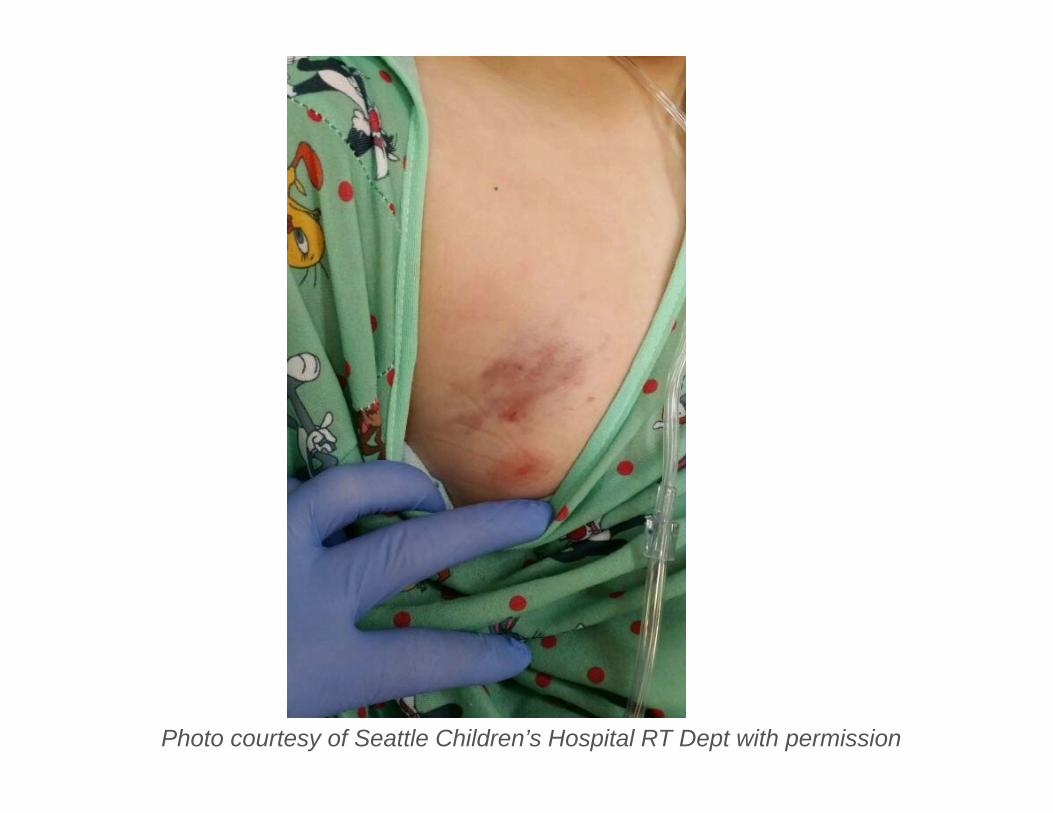
Photo courtesy of Seattle Children’s Hospital RT Dept with permission
-2
2
6
10
14
18
1/1/
2009
2/2/
2009
3/7/
2009
4/8/
2009
5/10
/200
96/
11/2
009
7/13
/200
98/
15/2
009
9/16
/200
910
/19/
2009
11/2
0/20
0912
/23/
2009
1/24
/201
02/
26/2
010
3/30
/201
05/
2/20
106/
3/20
107/
5/20
108/
6/20
109/
8/20
1010
/11/
2010
11/1
2/20
1012
/15/
2010
1/16
/201
12/
20/2
011
3/25
/201
14/
26/2
011
5/31
/201
17/
4/20
118/
5/20
119/
8/20
1110
/14/
2011
11/2
0/20
1112
/23/
2011
2/3/
2012
3/18
/201
24/
28/2
012
6/2/
2012
7/13
/201
28/
19/2
012
9/25
/201
211
/13/
2012
12/2
5/20
121/
29/2
013
3/3/
2013
4/10
/201
35/
17/2
013
6/27
/201
38/
3/20
139/
7/20
1310
/16/
2013
12/1
1/20
131/
24/2
014
3/12
/201
44/
16/2
014
5/24
/201
46/
26/2
014
7/29
/201
4
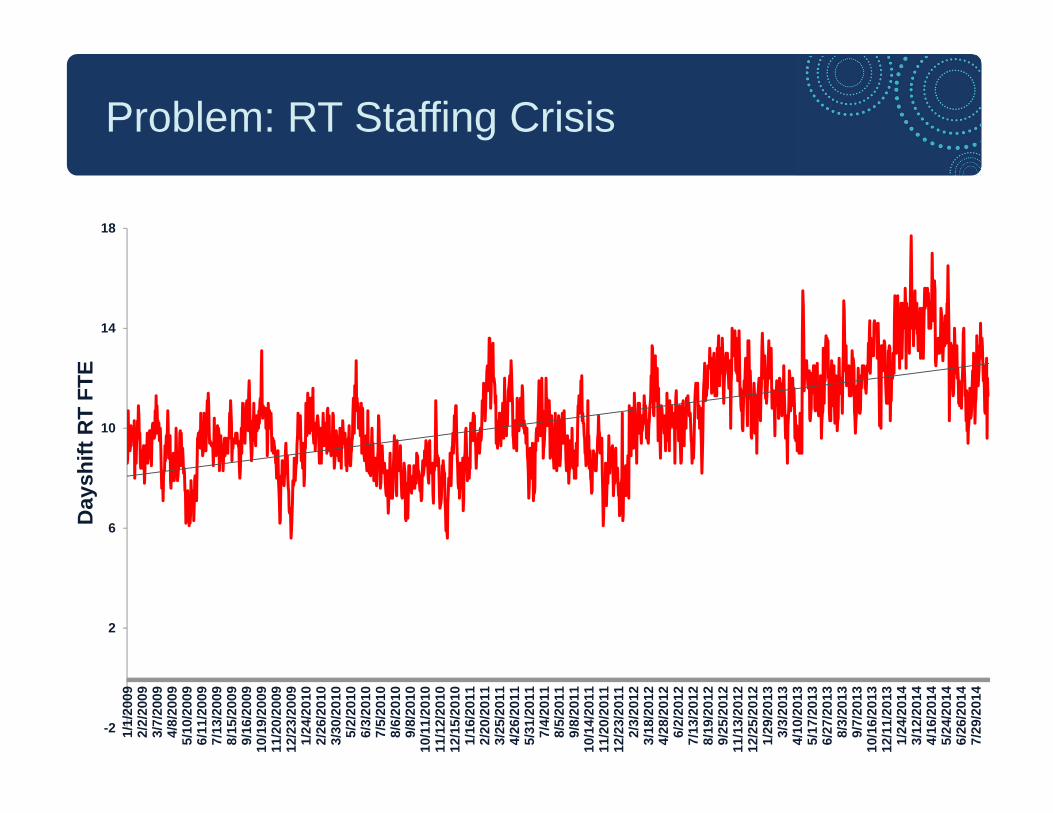
Problem: RT Staffing CrisisD
aysh
ift R
T FT
E

0
400
800
1200
1600
2000
2400
2011 2012 2013 2014
# C
hest
Phy
siot
hera
py C
harg
es
JanFebMarApr
Allocation of RT resources: Airway Clearance
$548,310
$908,670 $1,017,660
$1,431,150
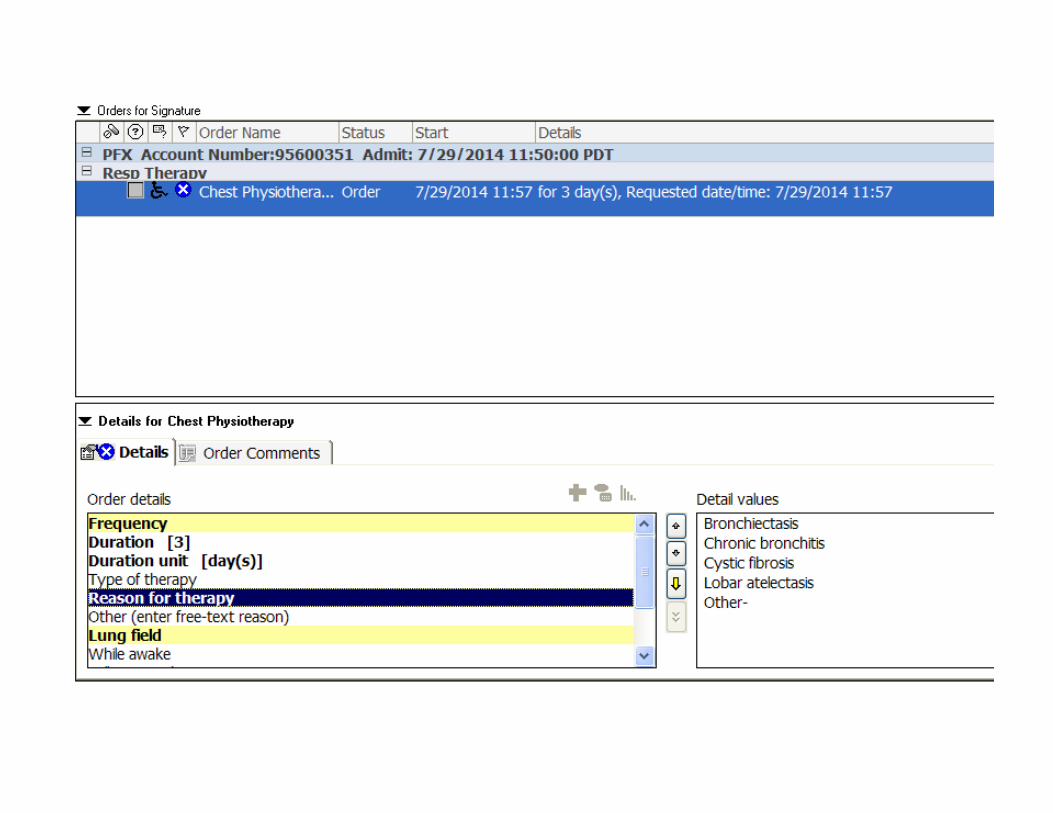
Reasons “other” than those indicated in the order set
“prevention of lobar atelectasis, diffuse pneumonia, increased work of breathing, inability to clear secretions, obstruction of V-P shunt and pleural effusion, complete lung opacification while on extracorporeal life support, wheezing, microaspiration, comfort (soothing), decreased breath sounds, no abdominal domain, poor pulmonary compliance, bronchiolitis, excessive nasal and/or oral pooling, junky breath sounds, , post-operative fever and paroxysmal cough.”
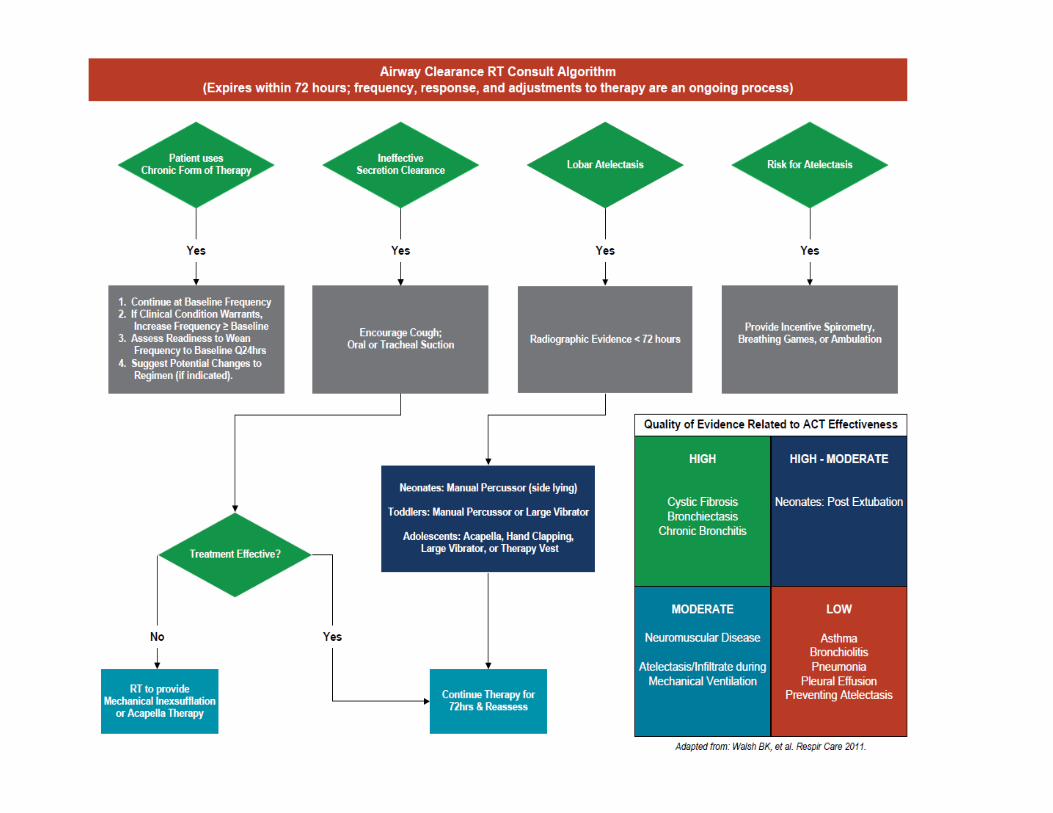
Goal
• We proposed a therapist‐driven protocol that allows RTs to provide appropriate and judicious ACT care to patients– Less risk to the patient– Less expense to payers– Less strain on RT resources– Improved job satisfaction for RTs
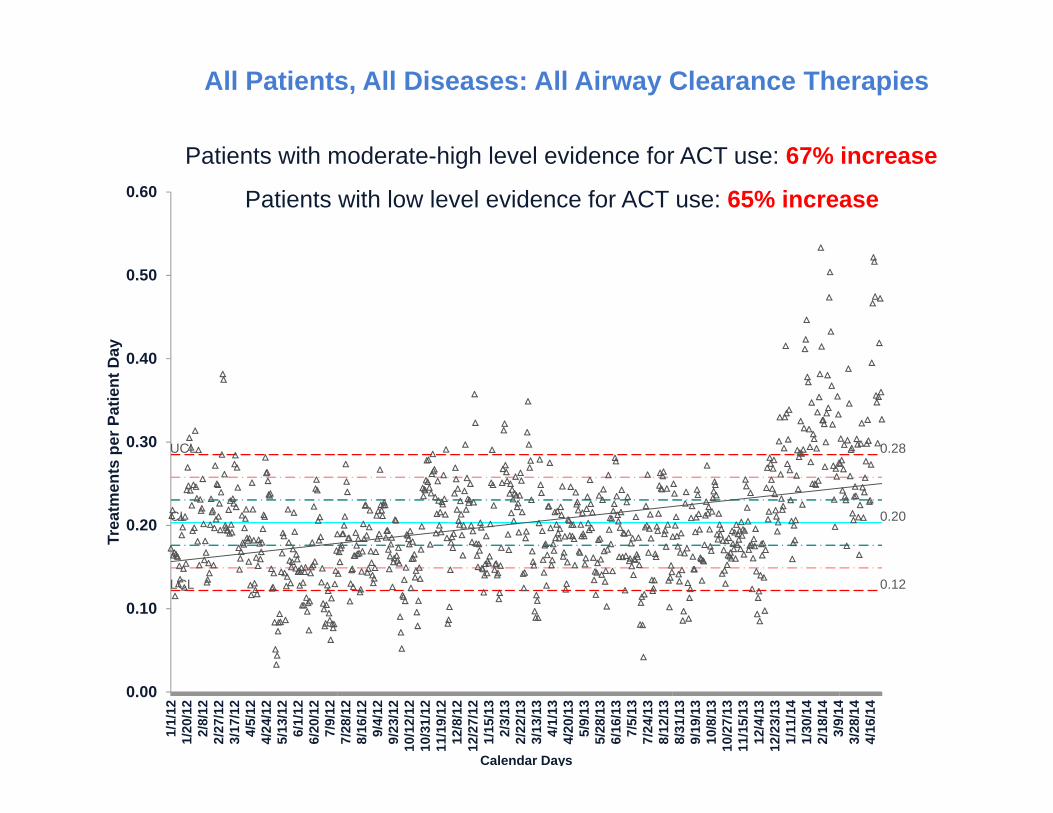
UCL 0.28
CL 0.20
LCL 0.12
0.00
0.10
0.20
0.30
0.40
0.50
0.601/
1/12
1/20
/12
2/8/
122/
27/1
23/
17/1
24/
5/12
4/24
/12
5/13
/12
6/1/
126/
20/1
27/
9/12
7/28
/12
8/16
/12
9/4/
129/
23/1
210
/12/
1210
/31/
1211
/19/
1212
/8/1
212
/27/
121/
15/1
32/
3/13
2/22
/13
3/13
/13
4/1/
134/
20/1
35/
9/13
5/28
/13
6/16
/13
7/5/
137/
24/1
38/
12/1
38/
31/1
39/
19/1
310
/8/1
310
/27/
1311
/15/
1312
/4/1
312
/23/
131/
11/1
41/
30/1
42/
18/1
43/
9/14
3/28
/14
4/16
/14
Trea
tmen
ts p
er P
atie
nt D
ay
Calendar Days
Total Tx Per Patient Day- All PatientsPatients with moderate-high level evidence for ACT use: 67% increase
All Patients, All Diseases: All Airway Clearance Therapies
Patients with low level evidence for ACT use: 65% increase
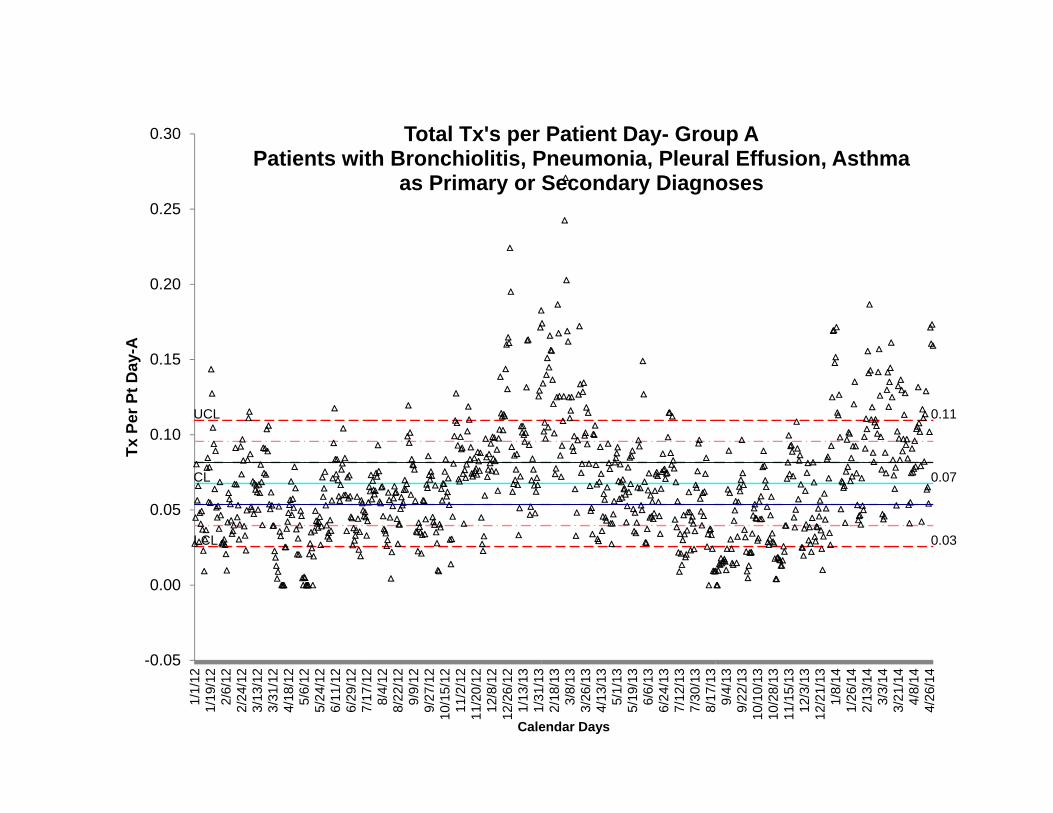
UCL 0.11
CL 0.07
LCL 0.03
-0.05
0.00
0.05
0.10
0.15
0.20
0.25
0.30
1/1/
121/
19/1
22/
6/12
2/24
/12
3/13
/12
3/31
/12
4/18
/12
5/6/
125/
24/1
26/
11/1
26/
29/1
27/
17/1
28/
4/12
8/22
/12
9/9/
129/
27/1
210
/15/
1211
/2/1
211
/20/
1212
/8/1
212
/26/
121/
13/1
31/
31/1
32/
18/1
33/
8/13
3/26
/13
4/13
/13
5/1/
135/
19/1
36/
6/13
6/24
/13
7/12
/13
7/30
/13
8/17
/13
9/4/
139/
22/1
310
/10/
1310
/28/
1311
/15/
1312
/3/1
312
/21/
131/
8/14
1/26
/14
2/13
/14
3/3/
143/
21/1
44/
8/14
4/26
/14
Tx P
er P
t Day
-A
Calendar Days
Total Tx's per Patient Day- Group APatients with Bronchiolitis, Pneumonia, Pleural Effusion, Asthma
as Primary or Secondary Diagnoses

UCL 0.20
CL 0.14
LCL 0.07
-0.05
0.05
0.15
0.25
0.35
0.45
0.55
1/1/
121/
20/1
22/
8/12
2/27
/12
3/17
/12
4/5/
124/
24/1
25/
13/1
26/
1/12
6/20
/12
7/9/
127/
28/1
28/
16/1
29/
4/12
9/23
/12
10/1
2/12
10/3
1/12
11/1
9/12
12/8
/12
12/2
7/12
1/15
/13
2/3/
132/
22/1
33/
13/1
34/
1/13
4/20
/13
5/9/
135/
28/1
36/
16/1
37/
5/13
7/24
/13
8/12
/13
8/31
/13
9/19
/13
10/8
/13
10/2
7/13
11/1
5/13
12/4
/13
12/2
3/13
1/11
/14
1/30
/14
2/18
/14
3/9/
143/
28/1
44/
16/1
4
Tx P
er P
t Day
-B
Calendar Days
Tx's per Patient DayPatients without Pneumonia, Bronchitis, Bronchiolitis or Asthma
as Primary or Secondary Dx
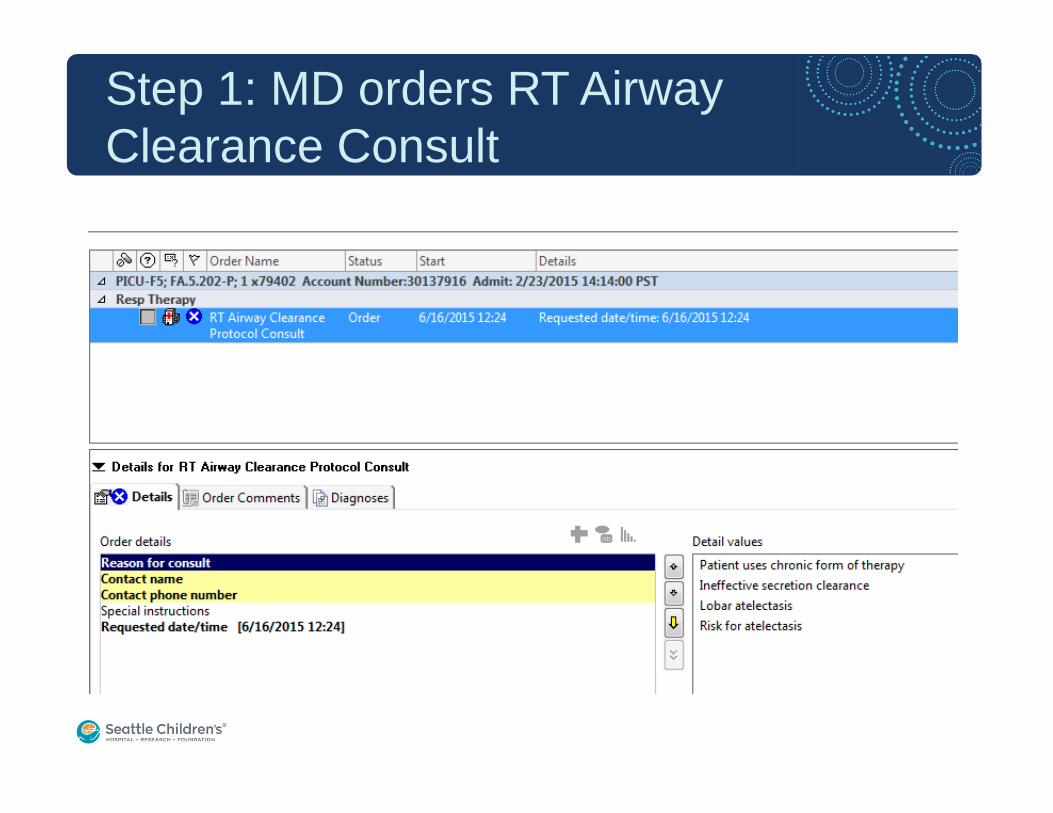
Step 1: MD orders RT Airway Clearance Consult
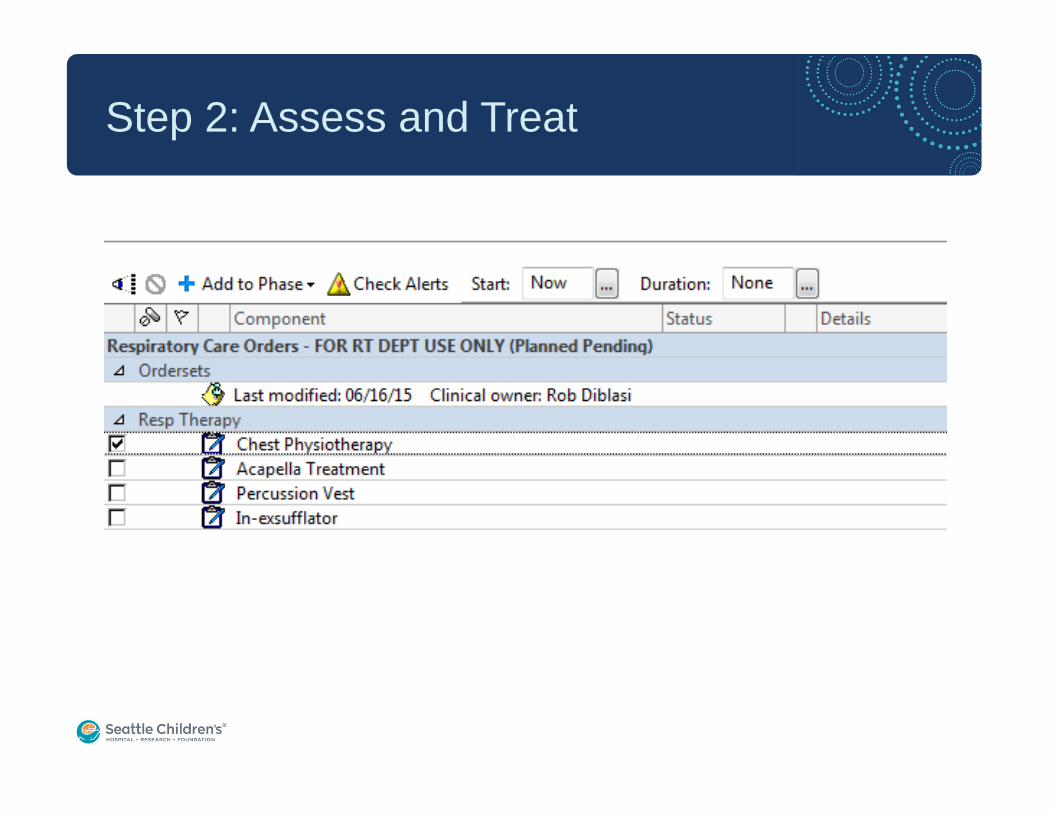
Step 2: Assess and Treat
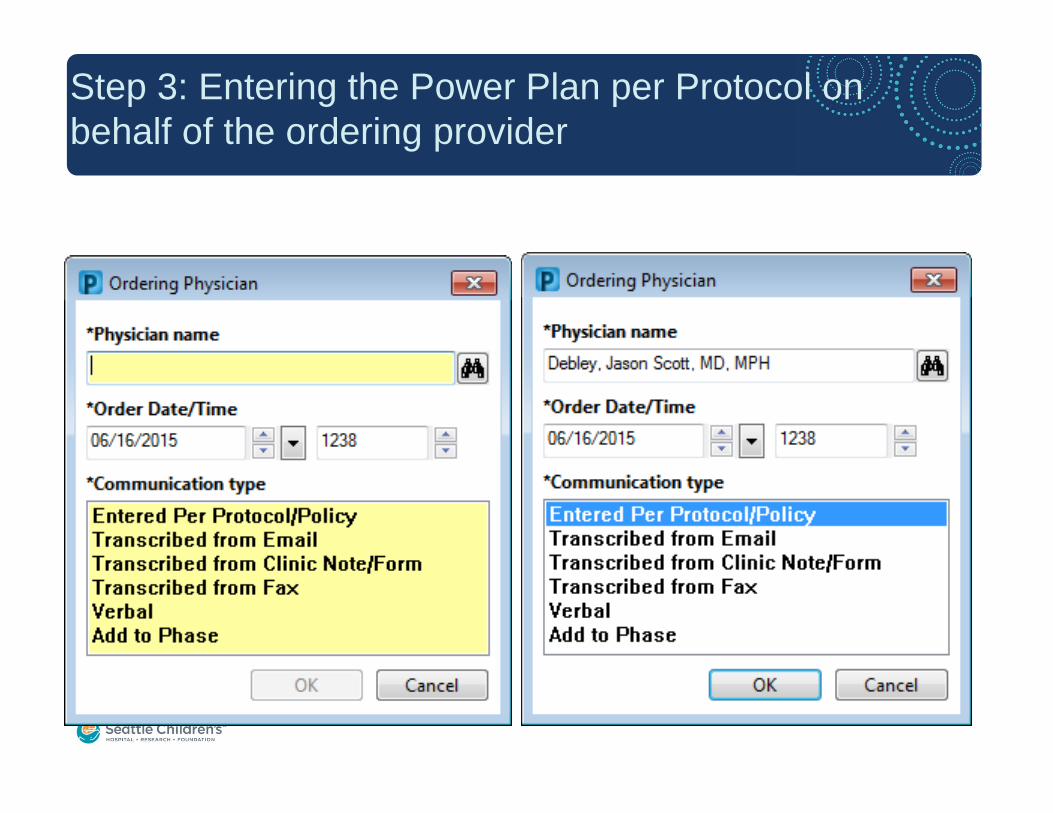
Step 3: Entering the Power Plan per Protocol on behalf of the ordering provider
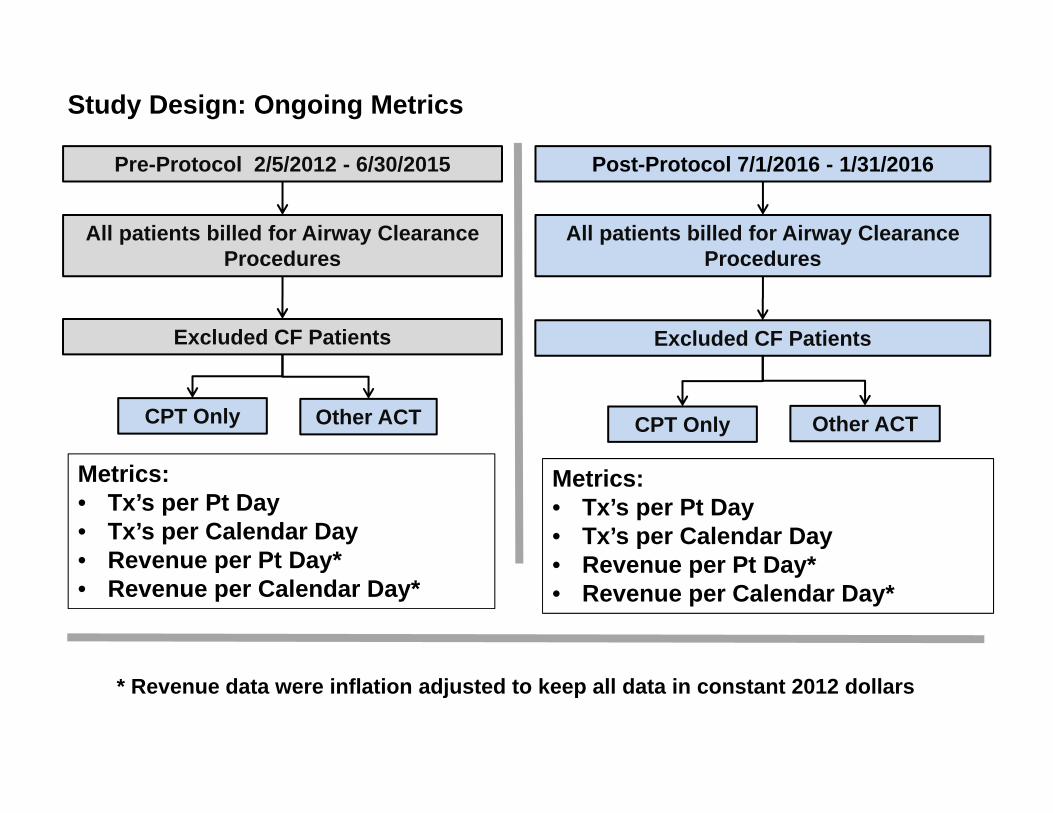
Post-Protocol 7/1/2016 - 1/31/2016
All patients billed for Airway Clearance Procedures
Excluded CF Patients
Pre-Protocol 2/5/2012 - 6/30/2015
All patients billed for Airway Clearance Procedures
Excluded CF Patients
CPT Only Other ACT
Metrics:• Tx’s per Pt Day• Tx’s per Calendar Day• Revenue per Pt Day*• Revenue per Calendar Day*
Study Design: Ongoing Metrics
CPT Only Other ACT
* Revenue data were inflation adjusted to keep all data in constant 2012 dollars
Metrics:• Tx’s per Pt Day• Tx’s per Calendar Day• Revenue per Pt Day*• Revenue per Calendar Day*
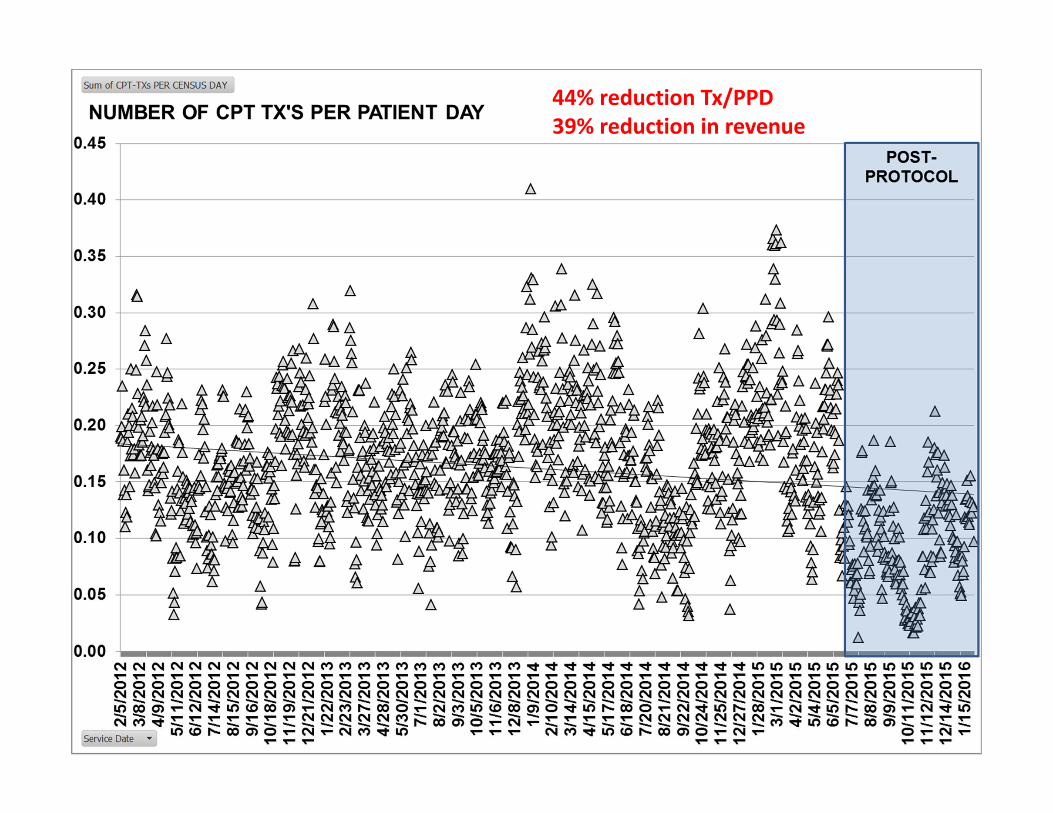
44% reduction Tx/PPD39% reduction in revenue
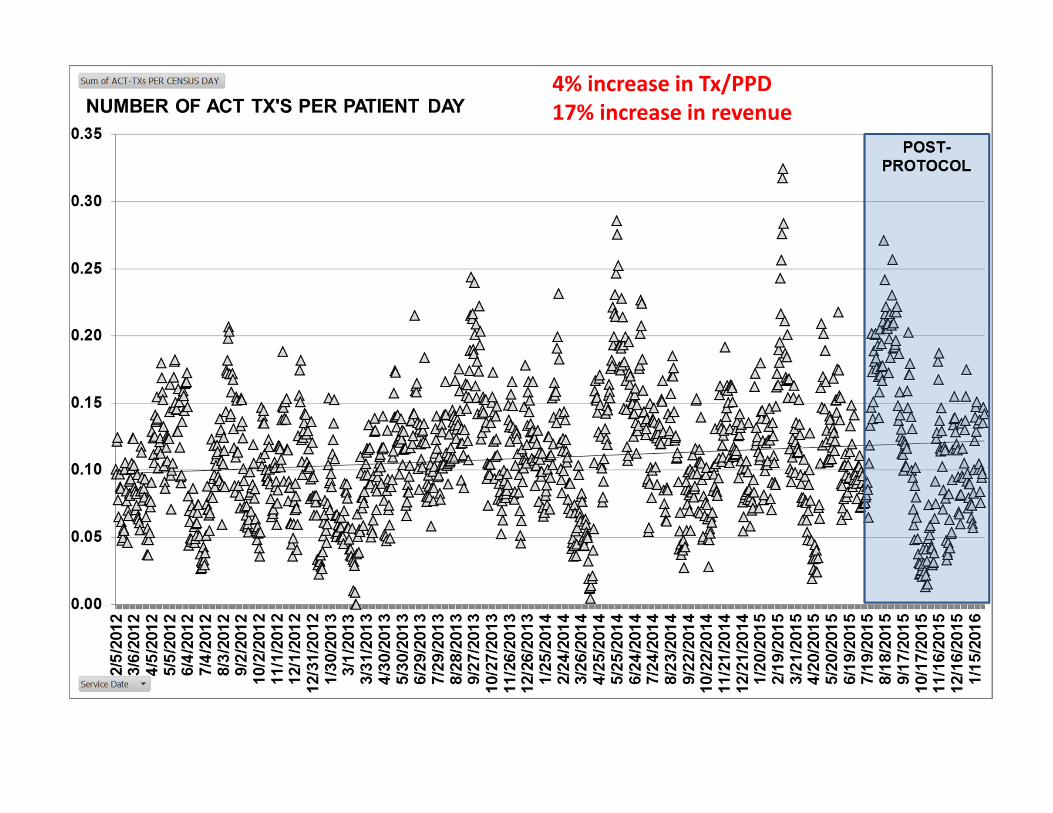
4% increase in Tx/PPD17% increase in revenue
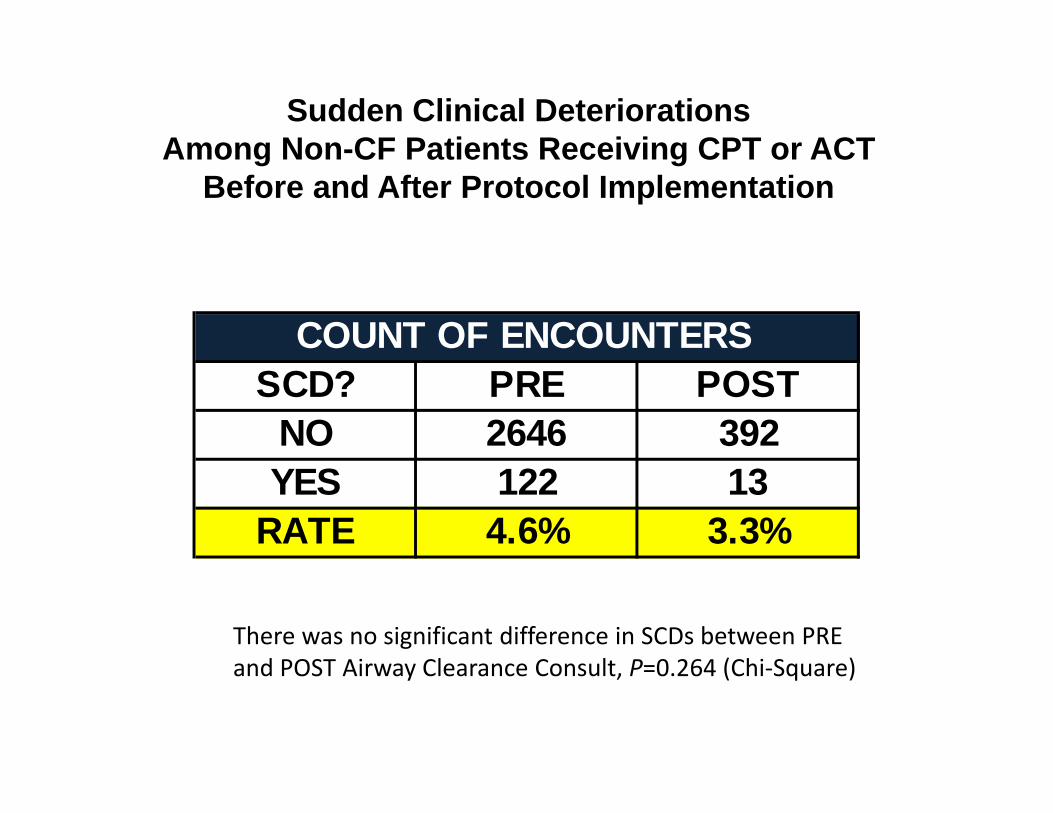
Sudden Clinical DeteriorationsAmong Non-CF Patients Receiving CPT or ACT
Before and After Protocol Implementation
SCD? PRE POSTNO 2646 392YES 122 13
RATE 4.6% 3.3%
COUNT OF ENCOUNTERS
There was no significant difference in SCDs between PRE and POST Airway Clearance Consult, P=0.264 (Chi‐Square)
Shared Learnings
• Developing a hospital-wide RT Driven Protocol (clinical standard work) is not EASY work
• Clinical Standard Work can result in significant cost savings and potentially lower risk to the patient
• Must engage/include key stakeholders from multiple disciplines• Share evidence-based data and publications• Solicit input from RN, MD, RT leadership• Work with IS to develop an appropriate order set
• Ongoing assessment of metrics is necessary to evaluate the success of our efforts

Conclusion
• The effectiveness of airway clearance therapy lacks definitive data in different pediatric populations
• CPT may do more harm than good in some patients and clinicians should weigh risk vs benefit with tx• Bronchiolitis, post-op, pneumonia, prevention of atelectasis
• Educating clinicians and patients on ACTs is essential• Not all patients can be managed with a standardized
ACT protocol and care may need to be modified or individualized





























