Embed Size (px)
DESCRIPTION
HS162 Health Organization; Dr. Santiago
Citation preview
Health Information
Technology
Harry J. MartinInformation Systems Manager
Public Health Department
Santa Clara Valley Health & Hospital System
Fall Semester 2014
Goals for talk
High-level overview
Describe concepts of HIT
What are the needs for HIT workforce
What role does HIT play in Health Care Reform
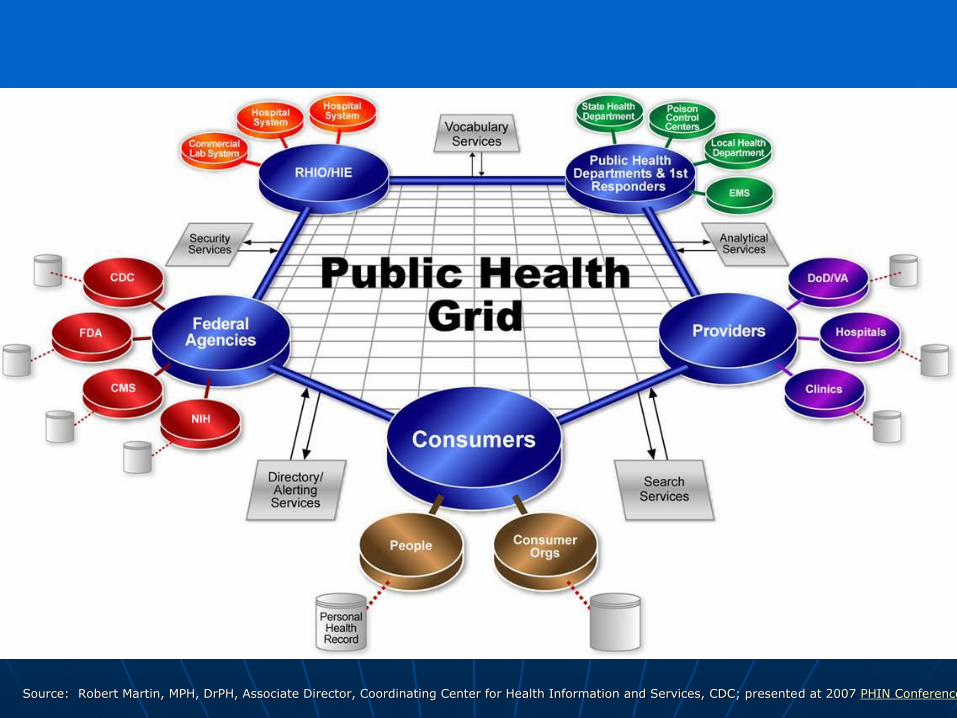
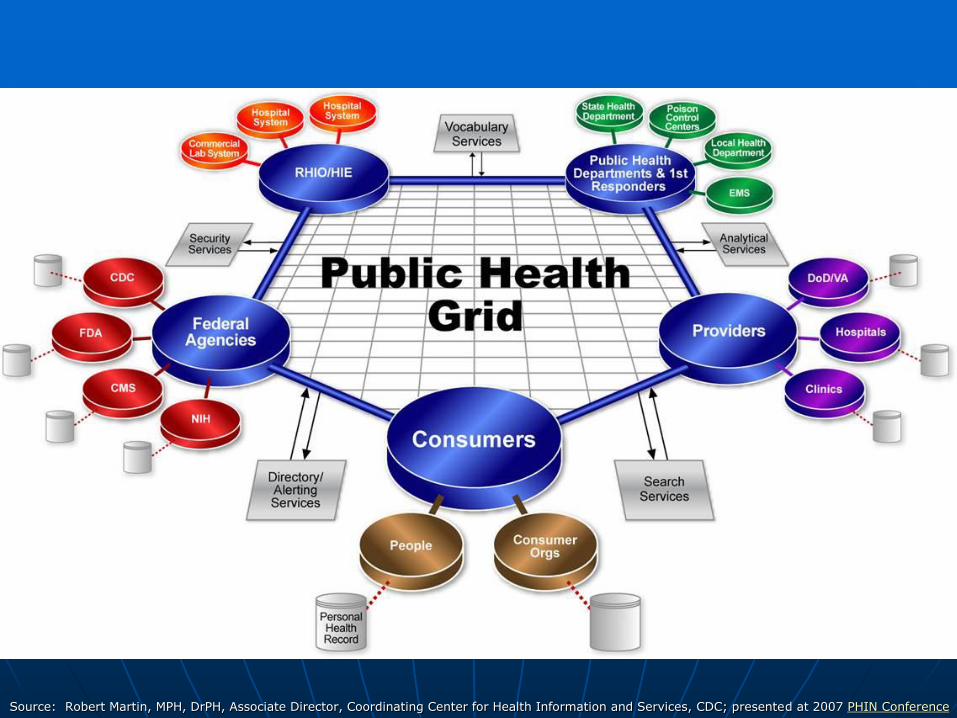
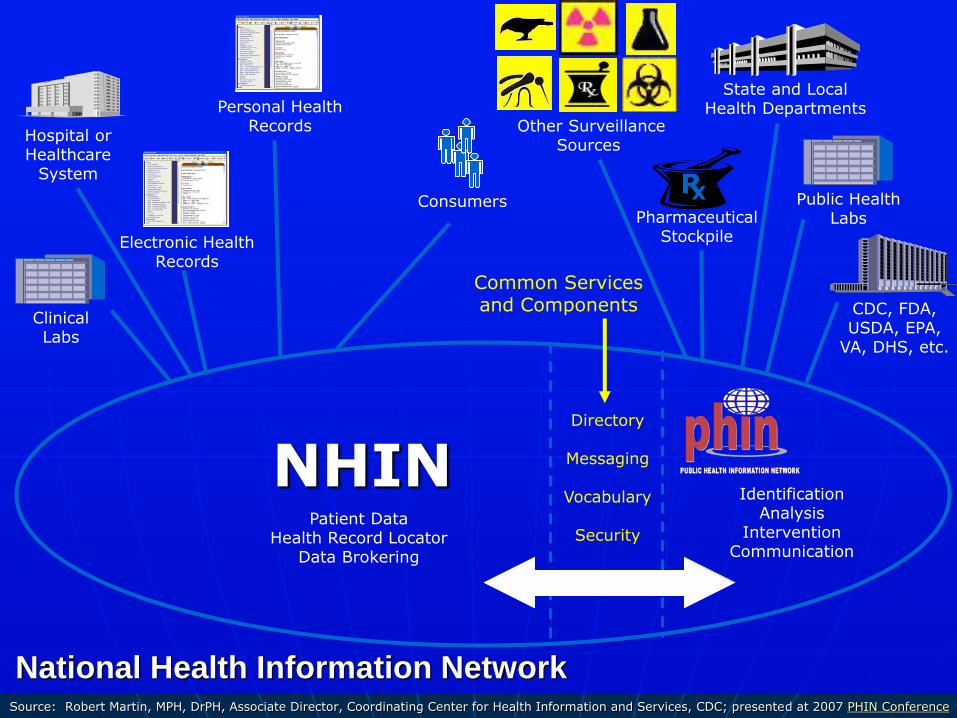
Source: Robert Martin, MPH, DrPH, Associate Director, Coordinating Center for Health Information and Services, CDC; presented at 2007 PHIN Conference
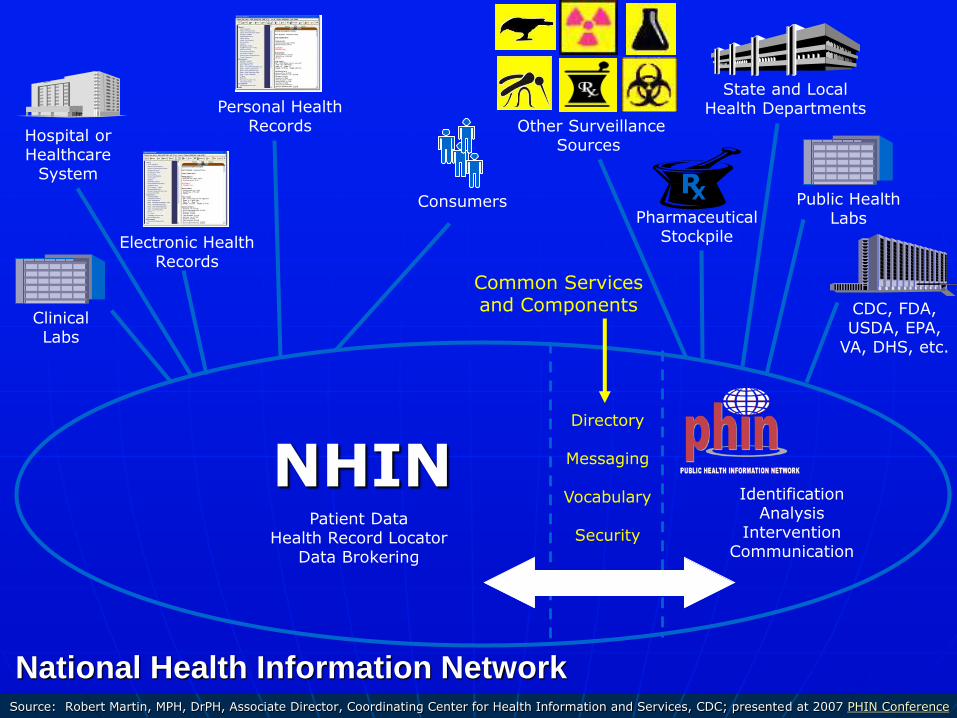
Consumers
Hospital orHealthcare
System
Electronic HealthRecords
ClinicalLabs
Personal HealthRecords
CDC, FDA, USDA, EPA,
VA, DHS, etc.
RX
PharmaceuticalStockpile
State and Local Health Departments
Public HealthLabs
Other SurveillanceSources
Directory
Messaging
Vocabulary
Security
Common Servicesand Components
Data & Information
IdentificationAnalysis
InterventionCommunication
NHINPatient Data
Health Record LocatorData Brokering
National Health Information NetworkSource: Robert Martin, MPH, DrPH, Associate Director, Coordinating Center for Health Information and Services, CDC; presented at 2007 PHIN Conference
Terms
Electronic Medical Record (EMR)
Electronic Health Record (EHR)
Personal Health Record (PHR)
Terms (cont.)
• ONC - Office of the National Coordinator for HIT
• CMS – Centers for Medicare and Medicaid Services
• Meaningful use
• ACO – Accountable Care Organization
Terms (cont.)
Interoperability
Health Information Exchange (HIE)
Computerized Physician Order Entry (CPOE)
E-Prescribing
Clinical Decision Support System (CDSS)
Terms (cont.)
HIE - Health Information Exchange
• Federated Model
• Monolithic Model
RHIO
HITECH Act
But first for a little history….
Bush Administration
Executive orders
• April 2004
Commitment to achieving widespread use of EMRs by 2014
• August 2006
Directs HHS and all federal agencies to ensure that internal programs and external contracts implement relevant HHS recognized interoperability standards
Obama Administration
“To improve the quality of our health care while lowering its cost, we will make the immediate investments necessary to ensure that within five years, all of America’s medical records are computerized … It just won’t save billions of dollars and thousands of jobs – it will save lives by reducing the deadly but preventable medical errors that pervade our health care system.” • January, 2009
Barack Obama: "Address at George Mason University in Fairfax, Virginia," January 8, 2009. Online by Gerhard Peters and John T. Woolley, The American Presidency Project. http://www.presidency.ucsb.edu/ws/?pid=85361.
HITECH
Health Information Technology for Economic and Clinical Health (HITECH) Act of the American Recovery and Reinvestment Act (ARRA)
• Incentives for EHR adoption ($30B, offset by $20B in savings)
• Direct grants administered by federal agencies ($2B) – ONC-coordinated
HITECH
Other provisions in other areas of ARRA
• Comparative effectiveness research
• NIH and other research funding
• Broadband and other infrastructure funding
Motivations
• Quality – not as good as it could be
• Safety – IOM 2000: 44-98K deaths/yr
• Cost – rising costs are not sustainable
• Inaccessible information – missing information frequent in primary health care
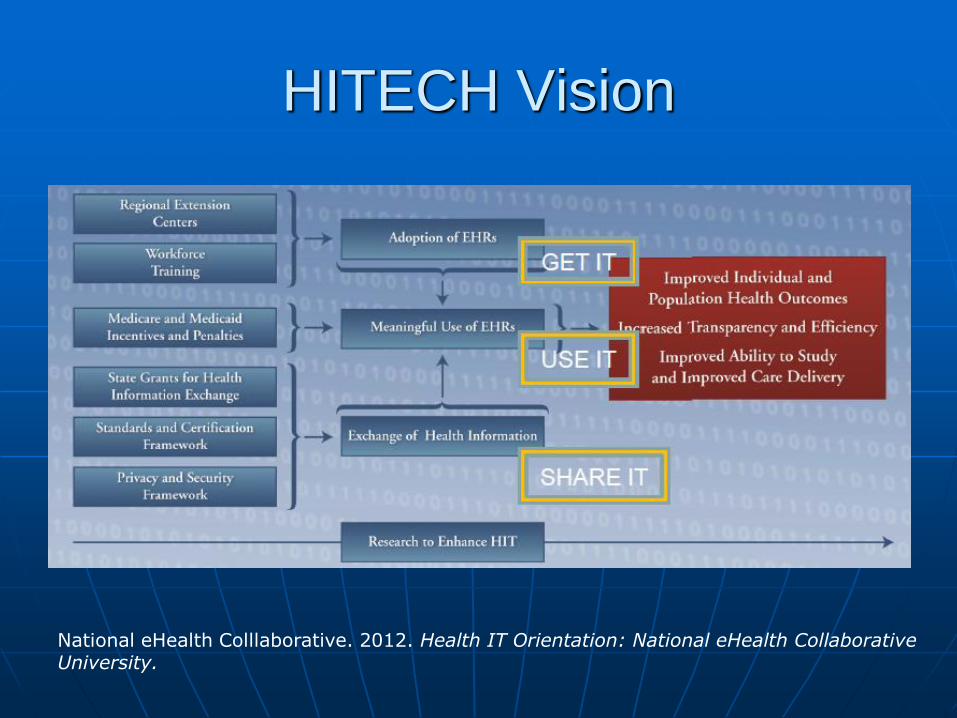
HITECH Vision
National eHealth Colllaborative. 2012. Health IT Orientation: National eHealth Collaborative University.
Where are we today?
CMS and the ONC give providers an additional year to meet MU requiremetns
CMS 2015 payment schedule
• market basket update of 2.9% for providers who in 2013
Submitted QoC data
Demonstrated MU

Just what is “HIT” anyway
Biomedical and health informatics (BMHI)
• Field that seeks the optimal use of information, often aided by technology, to improve individual health, health care, public health, and biomedical research
It’s about information, not technology
Technology is a relatively small piece
• Science behind the application of IT to healthcare
• Practitioners are usually called informaticians
The HIT Equation
Health (people) + information + technology
=
HIT
Expanded use of HIT
Benefits for individual patient care• Improve quality of patient care
• Reduce medical errors
• Reduce health care costs
• Increase administrative efficiencies
• Eliminate duplication of information gathering and testing
• Promote care coordination
• Expand access to affordable care
Expanded use of HIT
Public sector benefits
• Early detection of infectious disease outbreaks around the country
• Improved tracking of chronic disease management
• Evaluation of health care –
determine the value derived from collection of de-identified price and quality information

Health Record
Definitions
Types of Health Records
Electronic Medical Record (EMR)
• Early EMRs – clinicians for Dx and Tx
Maintained by physicians
Electronic Health Record (EHR)
• Longitudinal, full record
Maintained by providers
Personal Health Record (PHR)
• Not covered by HIPAA
Maintained by patient
Organizations
• ONC - Office of the National Coordinator for HIT
• CMS – Centers for Medicare and Medicaid Services
• ACO – Accountable Care Organization
• Meaningful use
Building Blocks
Interoperability
Health Information Exchange (HIE)
Computerized Physician Order Entry (CPOE)
Clinical Decision Support (CDS)
E-Prescribing

Meaningful Use
Meaningful Use
HITECH provides financial incentives for “meaningful use” of HIT
• Incentives for EHR adoption ($36-40B)
• Direct grants ($2B)
Office of the National Coordinator for Health IT (ONC)
EHR Certification and
Meaningful Use
ONC – Office of the National Coordinator for
Health Information Technology - defines the certification criteria for Electronic Health Records (how the EHR must work)
CMS – Centers for Medicare and Medicaid
Services define meaningful use (how the EHR must be used)
What is “meaningful use” of an EHR
Five basic goals for healthcare system1. Improving quality, safety and efficiency
Use CPOE
2. Engaging patients in their care Provide patients with a copy of their PHI
3. Increasing coordination of care Exchange key clinical information with other providers
4. Improving health status of the population Submit electronic data to immunization registries
5. Ensuring privacy and security Protect electronic health information created or maintained in
the EHR
What is “meaningful use” of an EHR
Three requirements:
• Use of certified EHR technology in a meaningful manner
• Utilize certified EHR technology connected for health information exchange (HIE)
• Use of certified EHR technology to submit information on clinical quality measures
Timeline for implementation
Timeframe for implementation of meaningful use criteria
• 2009 – HITECH policies
• 2011 – Stage 1 capture/share data
• 2014 – Stage 2 advanced care with decision support
• 2016 and beyond – Stage 3 Improved Outcomes
Implementation of meaningful use
Implemented through Medicare or Medicaid reimbursement to
• Eligible professionals – up to $44K
(Roughly equal to the cost of converting a physician practice from paper to EHRs.)
• Eligible hospitals - $2 – $9 million or $17,500 / bed
Timeframe for full implementation
• 2014 – advanced care with decision support
Stage 1 Requirements
15 Mandatory Core Measures
5 0f 10 Menu Measures
6 Clinical Quality Measures
• 3 core, 3 menu from a list of 41
Stage 1 Core Measures(15 required)
Improve Quality, Safety and Efficiency, and Reduce Health Disparities
• At least 40% of prescriptions transmitted electronically to the patient’s pharmacy
Engage Patients and Families
• Provide patients clinical summaries within 3 business days for over 50 percent of all office visits
Stage 1 Core Measures(cont.)
Improve Care Coordination
• Perform at least one test to demonstrate the ability to exchange key clinical information with other providers
Privacy and Security
• Conduct or review a security risk analysis and implement security updates as necessary
Menu Set Measures
Improve Quality, Safety, and Efficiency, and Reduce Health Disparities
• Generate at least one report listing patients with a specific condition
Engage Patients and Families
• Send reminders, if desired, for preventive/follow-up care for specified minimum percentages of adult and pediatric patients
Menu Set Measures(cont.)
Improve Care Coordination
• Perform medication reconciliation for more than 50 percent of patient transitions into the care of the physician
Improve Population and Public Health
• Perform at least one test of EHR‘s capability to provide syndromicsurveillance data to public health agencies, and perform a follow-up submission if the test is successful
Clinical Quality Measures(3 core) …
Adult Weight Screening
• % of patients with calculated BMI
• Plan to follow-up if above criteria
Diagnosed Hypertension
• At least 2 Blood Pressure readings
Preventive Care and Screening
• Ask about tobacco usage
• Cessation intervention for smokers
Other Clinical Quality Measures(3 of 41)
Several cancer screening
Anti-platelet therapy for CAD patients
Quality Measures for MU
September 4, 2012 CMS releases final rules for Stage 2:
• Eligible professionals
Need to meet 17 core objectives and 3 of 6 menu objectives = 20 objectives total
• Hospitals
Need to meet 16 core objectives and 3 of 6 menu objectives
Stage 2 Core Measures
Raised the goals
Consolidated Stage 1 Menu Set into Core
• e.g. measures may now have additional components
Stage 2 Core Measures(cont.)
New and Important:
• 5% of patients digitally accessed health information
How: Transferring a CCD to PHR
• 5% sent secure messages to provider
How:DIRECT
Stage 2 vs. Stage 1
Menu set (3 of 6)
All new
More clinically sophisticated
Submit cancer cases to a registry
Electronic access to scans and images
Quality Measures – 9 of 64 required
• Was 6 of 44 in Stage 1)

Funding Initiatives
Funding initiatives
HIT Regional Extension Centers (RECs)
• $643M – 70 RECs; provide guidance, mainly to primary care practices, in achieving meaningful use
State-based health information exchange (HIE)
• $564M – to states to develop HIE programs
Funding initiatives
Beacon Communities
• $235 M to fund 15 communities that provide exemplary demonstration of meaningful use of EHRs
• Awards were announced last year
Strategic health information advanced research projects (SHARP)
• $60 M for 4 collaborative research centers
Funding for Health IT workforce
Key to implementation
• ONC estimates at least 50,000 workers needed to implement the federal HIT agenda
• ONC is funding $118 million for
Community college consortia - $70M
Curriculum Development Centers - $10M
University training grants ($32M)
Competency testing ($6M)
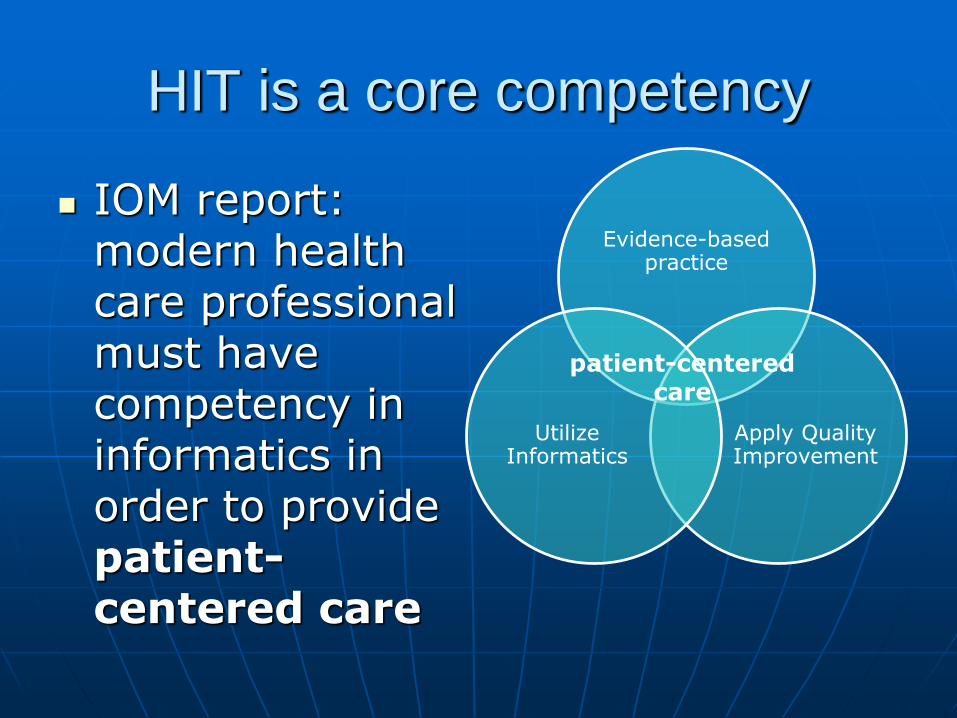
HIT is a core competency
IOM report: modern health care professional must have competency in informatics in order to provide patient-centered care
Evidence-based practice
Apply Quality Improvement
Utilize Informatics
patient-centered care
Who is the health IT workforce?
Historically, three groups of HIT professionals
• Information technology (IT) – usually with computer science or information systems background
• Health information management (HIM) – focus on medical records
• Clinical informatics (CI) – often from healthcare backgrounds (MDs, nurses)
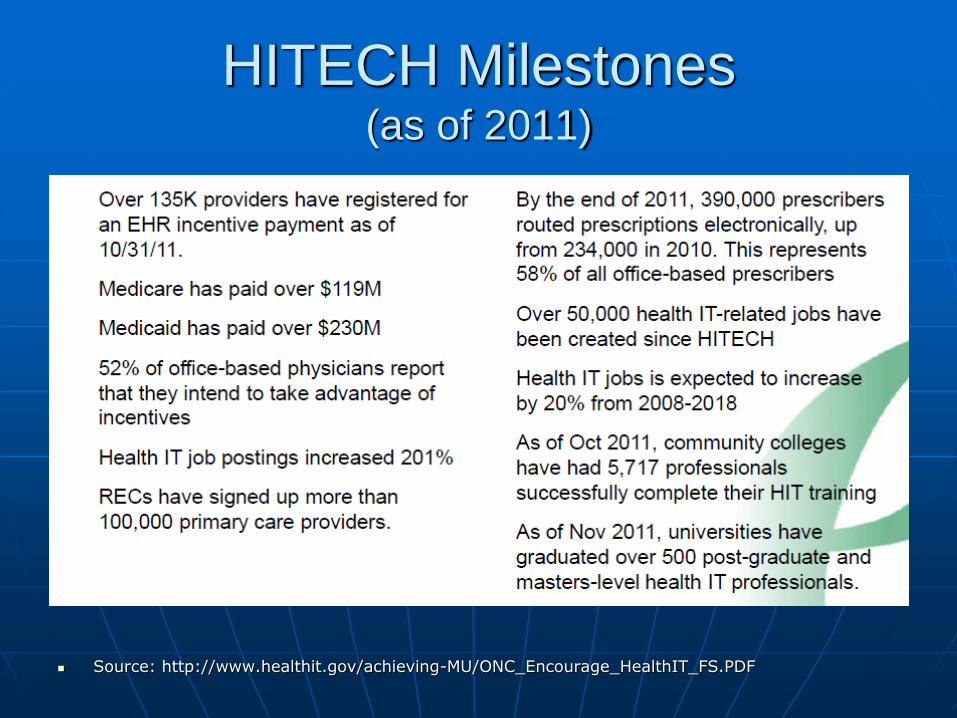
HITECH Milestones(as of 2011)
Source: http://www.healthit.gov/achieving-MU/ONC_Encourage_HealthIT_FS.PDF
2013 Progress Report
EHR Incentive program
• Eligible Hospitals (EH)
85% of eligible hospitals participate
75% have received payments for MU
• Eligible Professionals (EP)
More than 388,000 have registered (73% of all eligible to participate)
More than 230,000 have received payments (44%)
2013 Progress Report
EHR Incentive program
• $12.6 billion paid as of February 2013
• $14.6 billion paid as of April 2013
Progress (cont.)
RECs
• Providing assistance to more than
44% (130K) primary care providers
48% (20K) of nurse practitioners
Health IT marketplace
• Robust market for eHealth IT products
As of March 2013 – 941 vendors with more than 1,700 unique certified EHR products
Progress (cont.)
Rapid Adoption of Advanced Technology
• E-Prescribing – office-based physicians
0.8% in December 2006
53% in January 2013
More than 94% of all pharmacies
Progress (cont.)
Rapid Adoption of Advanced Technology (beyond MU requirements)
• Hospitals
2008 – 9.4 % using advanced functionality
2012 – 44 percent
• Doctors
2008 – 17% using same advanced functionality
2012 – 40 %
Progress (cont.)
Workforce Development
• Community colleges – 17,049 HIT professionals trained (January 2013)
• Universities – 820 post-graduate and masters-level HIT professionals (September 2012)
50,000 HIT jobs created under HITECH
Blue Button
Web-based utility that allows patients to download and share their health information
Developed by VA and HHS for Veterans and Medicare recipients
Simple text file – easier to share
• Human- and
• Machine-readable format
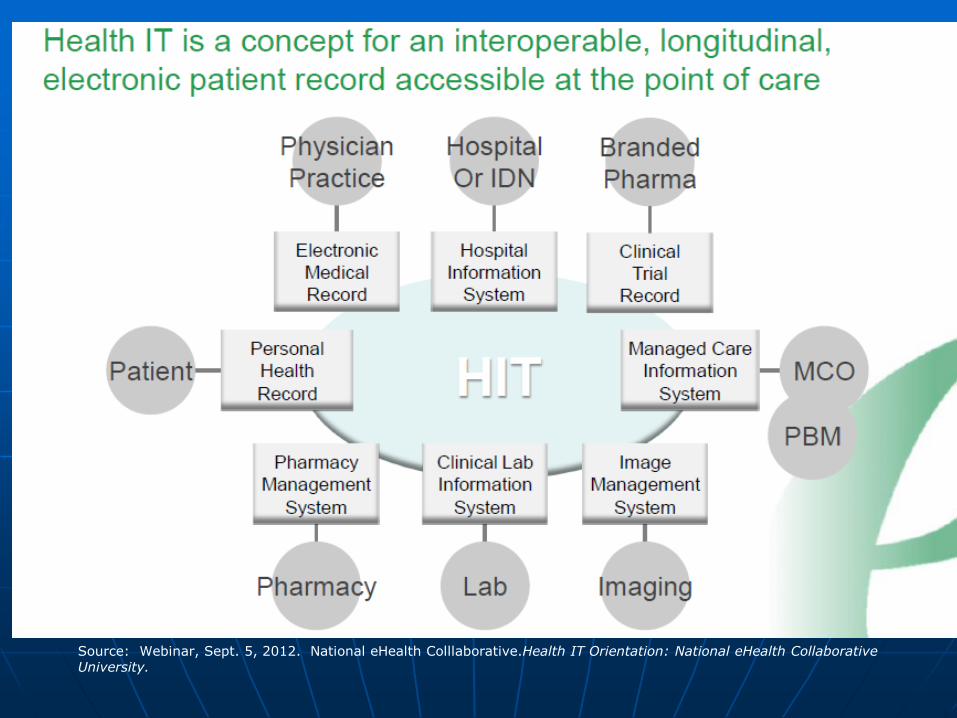
Source: Webinar, Sept. 5, 2012. National eHealth Colllaborative.Health IT Orientation: National eHealth Collaborative University.
Source: Robert Martin, MPH, DrPH, Associate Director, Coordinating Center for Health Information and Services, CDC; presented at 2007 PHIN Conference
Consumers
Hospital orHealthcare
System
Electronic HealthRecords
ClinicalLabs
Personal HealthRecords
CDC, FDA, USDA, EPA,
VA, DHS, etc.
RX
PharmaceuticalStockpile
State and Local Health Departments
Public HealthLabs
Other SurveillanceSources
Directory
Messaging
Vocabulary
Security
Common Servicesand Components
Data & Information
IdentificationAnalysis
InterventionCommunication
NHINPatient Data
Health Record LocatorData Brokering
National Health Information NetworkSource: Robert Martin, MPH, DrPH, Associate Director, Coordinating Center for Health Information and Services, CDC; presented at 2007 PHIN Conference

Merged with HIMSS
Foundation late 2013
Public-private partnership
• Secure and interoperable nationwide health information exchange
• Advance health and improve health care.
Stakeholders
government agencies
health systems
health professionals
academic medicine
patient and consumer
advocates
major payers and
employers
non-profits
technology providers
How IT projects fail
Problematic health IT implementations are well known, with failure often attributable to the lack of understanding of clinical environment
• Ensure all key players are involved from front-line staff to executive management, from programmers to IT project management
Immunization Registry
Incentives / Free-rider problem
Key support from motivated providers
County mandate as a condition of receiving funds for community clinics
HEDIS
Some physicians were concerned about IPAs getting information on their practices (performance measurement reporting) that they could use to penalize them.

Sources
Logos hyperlink to websites.

Websites for HIT Jobs &
Training Health IT No. 1 on list of top 10 'hot' careers
Healthcare information technology tops the list of top 10 'hot careers' for college graduates in 2011, according to a new study from the University of San Diego Extension.
Jobs
Training


HIT Blogs
John Halamka: http://geekdoctor.blogspot.com/
Wes Rishel: http://blogs.gartner.com/wes_rishel/
EMR and HIPAA: http://www.emrandhipaa.com/
HISTalk (ads): http://histalk2.com/
Sphere by Shahid N. Shah, (ads): http://hitsphere.com
The End





























