-
Bard Access Systems
Central Venous CathetersInstructions For Use
PowerHohn* Central Venous Catheter Placement Procedure1. The
procedure is performed using sterile surgical technique including
the use of gloves,
masks, gowns, and sterile drapes and equipment throughout all
steps listed below.2. Place the patient in the Trendelenburg
position. Prep the insertion site using standard
surgical technique.3. The subclavian veins and the internal and
external jugular veins are the most common
vessels used for catheter insertion. The femoral vein may also
be used.4. Administer local anesthesia at the venous entry site,
the underlying subcutaneous tissue,
and where the wing will be sutured or the StatLock* device
secured.5. Catheters can be cut to length if a different length is
desired due to patient size and
desired point of insertion. 6. Enter the vein chosen for
insertion of the catheter using the introducer needle and
syringe or sheath over the needle. (Refer to figure 2)Caution:
When inserting the catheter via a subclavian approach, maintain a
horizontaltrajectory when introducing the needle beneath the
clavicle. Vertical needle passage mayincrease the risk of
pneumothorax. Refer to “Warnings” section concerning Catheter
Pinch-off.
7. Aspirate gently as the needle is introduced. Warning: If the
artery is entered, withdrawthe needle and apply manual pressure for
several minutes. If the pleural space is entered,withdraw needle
and observe patient for signs of pneumothorax. (Refer to figure
3)
8. When the vein has been entered, remove the syringe leaving
the needle in place. If usingthe sheath over the needle, insert the
assembly and withdraw the needle and syringeleaving the sheath
indwelling. Place a finger over the needle or sheath hub to
minimizeblood loss and risk of air aspiration. The risk of air
aspiration is reduced by performingthis part of the procedure with
the patient performing the Valsalva maneuver. (Refer tofigure
4)
9. Insert tapered end of the tip straightener into the needle
(or sheath). Advance theguidewire to the superior vena cava. (Refer
to figure 5)Caution: To help avoid possible severing of the
guidewire, do not withdraw the guidewireback against the needle
bevel.
10. Withdraw and remove needle (or sheath) while holding the
guidewire in place. Maintainslight pressure on the puncture site
after the needle is withdrawn. (Refer to figure 6)
10a. For catheters with VitaCuff* antimicrobial cuff: use the
supplied scalpel, if needed, to makea skin nick at the insertion
site to accommodate the antimicrobial cuff. (Refer to figure 7)
11. A skin nick may be made adjacent to the insertion site to
facilitate tip insertion.12. Advance the dilator over the exposed
wire using a rotational motion to develop a tunnel
for the catheter. Gentle counter traction on the skin may
facilitate smooth passage of thedilator. Several passes with the
dilator are recommended. (Refer to figure 8)
13. Withdraw the dilator.Note: Patients with thick muscular
chest walls or extensive scar tissue may require theuse of a
percutaneous introducer for catheter insertion.
14. For the dual lumen catheter, clamp and attach an end cap to
the one luer adapter toavoid possible air embolus.
15. Thread the catheter over the guidewire and advance the
catheter to the insertion site.The guidewire must extend out from
the luer adapter.
16. Advance the catheter and wire assembly together as a unit
with a rotational motion. Thisis best accomplished by gently
squeezing the catheter against the wire and rotating dur-ing
advancement until the catheter is fully inserted. Gentle counter
traction on the skinmay also facilitate smooth catheter passage.
(Refer to figure 9)Caution: Do not attempt to slide the catheter
over the wire separately into the vein. Thismay cause the catheter
to bunch up on the wire making advancement of the catheter intothe
vessel more difficult.
17. To help prevent advancement of the wire into the right
atrium during insertion, pause atleast twice and pull the wire back
while stabilizing the catheter. Then continue to advancethe
catheter and wire assembly together as a unit until the catheter is
completely inserted.
18. When the catheter has been inserted, hold it firmly in
position and slowly withdraw theguidewire. Have the patient perform
the Valsalva maneuver as the end of the wire iswithdrawn, and then
clamp the catheter. (Refer to figure 10)
19. Check for blood return. Then flush the lumen(s) with heparin
solution or normal salineand attach end cap.
20. Suture the catheter in place by passing the suture through
the eyes of the cathetersuture wing. Place the ties in the
direction of the insertion site to help prevent cathetermigration.
Tie with at least four throws. (Refer to figure 11) Alternatively,
the suture wing may be fixed to the patient with aStatLock*
device.
21. Cleanse and dress insertion site according to approved
technique. (Refer to figure 12)22. Obtain a chest x-ray to confirm
correct catheter position and absence of pneumothorax.Note: The
PowerHohn* catheter testing included 10 power injection cycles.
Tunneling Procedure (If Applicable)
1. Measure catheter against chest wall or upper arm of patient
to determine desired location of VitaCuff* Antimicrobial Cuff
andexit site. Mark locations, or make a skin nick at insertion site
to accommodate the VitaCuff* Antimicrobial Cuff.
2. Tunneling procedure. Note: The VitaCuff* Antimicrobial Cuff
should be positioned in the tunnel. The cuff will be less
promi-nent if positioned over an intercostal space. Create
subcutaneous tunnel from skin exit site to venous entrance using
tunneler or long forceps.a. Grasp the tunneler at the end.b. Insert
the rounded tip of the tunneler into a small incision at the
desired catheter exit.c. Form tunnel by advancing the tip of the
tunneler from the skin exit site up to the venous entry site.
Caution: Avoid inadver-
tent puncture of the skin or fascia with the tip of the
tunneler.d. Attach the lumen tip or one of the lumen tips of the
dual lumen catheter onto the tunneler
barb with a twisting motion. Barb threads must be completely
covered by the catheter tip toadequately secure the catheter as it
is pulled through the tunnel. A suture may be tiedaround the
catheter between the tunneler body and large barb to hold it more
securely.
e. Pull the catheter up through the tunnel to the venous entry
site. (Initial resistance may bemet as the VitaCuff* Antimicrobial
Cuff first enters the tunnel.) Gently holding the catheterproximal
to the cuff while pulling the tunneler and catheter through the
subcutaneous tunnelshould result in smooth passage of the cuff into
the subcutaneous tunnel. Caution: Whentunneling, the catheter must
not be forced.
f. Remove the catheter tip from the tunneler barb. Cutoff the
end tied by suture.
Catheter Exchange1. Any damaged, ruptured, or leaking catheter
must be replaced immediately to prevent blood loss and/or air
embolus. The
catheter should be clamped proximal to the damaged area close to
the chest wall.2. The catheter exchange technique is designed to
replace an indwelling PowerHohn* central venous catheter with a
new
catheter, using the existing venous entry site. Establish a full
sterile field and use mask and gloves.3. Insert the guidewire
through the indwelling catheter and remove the indwelling catheter
by pulling it back over the wire.4. Advance the new catheter over
the wire as instructed in the previous section, and remove the
guidewire.5. Suture the new catheter in place through the eyes of
the suture wing. Alternatively, the suture wing may be fixed to
the
patient with a StatLock* device. Cover with a sterile dressing
according to approved technique.
FlushingFlushing frequencies from once daily to once weekly have
been found to be effective when the catheter is not in use. Flush
withheparin after IV administration of TPN, IV fluids, or after
medications.Note: For frequently accessed catheters (accessed at
least every 8 hours), flushing with 5 ml of normal saline without
heparinbetween infusions has been found to be effective.
References1. Aitken, D.R. and Minton, J.P. “The Pinch-Off Sign:
A Subclavian Catheters”, American Journal of Surgery, Vol. 148,
Nov. 1984,
pp. 633-636.2. Rubenstein, R.B., Alberty, R.E., et al. “Hickman*
Catheter Separation”, JPEN, Vol. 9, No. 6, Nov./Dec. 1985, pp.
754-757.3. Hinke, D.H.; Zandt-Stastny, D.A.; Goodman, L.R.; et al.
Pinch-off syndrome: A complication of implantable subclavian
venous
access devices. Radiology 177: 353-356, 1990.4. Ingle, Rebecca,;
Nace, Corinne, Venous Access Devices: Catheter Pinch-off and
Fracture, 1993, Bard Access Systems, Inc.
Bard Access Systems, Inc. warrants to the first purchaser of
this product that this product will be free from defects in
materials andworkmanship for a period of one year from the date of
first purchase and liability under this limited product warranty
will be limited torepair or replacement of the defective product,
in Bard Access Systems, Inc. sole discretion or refunding your net
price paid. Wearand tear from normal use or defects resulting from
misuse of this product are not covered by this limited
warranty.
TO THE EXTENT ALLOWABLE BY APPLICABLE LAW, THIS LIMITED PRODUCT
WARRANTY IS IN LIEU OF ALL OTHERWARRANTIES, WHETHER EXPRESS OR
IMPLIED, INCLUDING, BUT NOT LIMITED TO, ANY IMPLIED WARRANTY OF
MER-CHANTABILITY OR FITNESS FOR A PARTICULAR PURPOSE. IN NO EVENT
WILL BARD ACCESS SYSTEMS, INC. BELIABLE TO YOU FOR ANY INCIDENTAL
OR CONSEQUENTIAL DAMAGES RESULTING FROM YOUR HANDLING OR USE OFTHIS
PRODUCT.
Some states/countries do not allow an exclusion of implied
warranties, incidental or consequential damages. You may be
entitledto additional remedies under the laws of your
state/country.
An issued or revision date for these instructions is included
for the user’s information. In the event two years have
elapsedbetween this date and product use, the user should contact
Bard Access Systems, Inc. to see if additional product information
isavailable.
Revised Date: February, 2007
*Bard, Hickman, Hohn, PowerHohn and StatLock are trademarks
and/or registered trademarks of C. R. Bard, Inc. or an affiliate.
*VitaCuff and VitaGuard are registered trademarks of Integra
LifeSciences, Corporation.
U.S. Patent Pending.
© 2007 C. R. Bard, Inc. All rights reserved.
Bard Access Systems, Inc.Salt Lake City, UT 84116 USA
1-801-595-0700Clinical Information Hotline: 1-800-443-3385Ordering
Information: 1-800-545-0890
www.bardaccess.com
PK0714238 / 0702R
5
6
7
8
9
10
11
12
3456
78910
1112
3456
78910
1112
2
3
4
The Power of Purple*
-
the catheter is being pinched between the clavicle and first rib
(the “Pinch-off” sign). Do not continue pulling against resistance
as thismay cause catheter breakage and embolism. Free up the
resistance (e.g. by repositioning the patient) before proceeding
further.
• If the artery is entered, withdraw the needle and apply manual
pressure for several minutes. If the pleural space is entered,
with-draw the needle and evaluate patient for possible
pneumothorax.
• Alcohol should not be used to soak or declot polyurethane
catheters because alcohol is known to degrade polyurethane
cathetersover time with repeated and prolonged exposure.
• Acetone and polyethylene glycol containing ointments should
not be used with polyurethane catheters, as they may damage the
device.• Failure to warm contrast media to body temperature prior
to power injection may result in catheter failure.• Failure to
ensure patency of the catheter prior to power injection studies may
result in catheter failure.• Power injector machine pressure
limiting feature may not prevent over pressurization of an occluded
catheter.• Exceeding the maximum flow rate of 5ml/sec, and the
maximum pressure of power injectors of 300 psi, may result in
catheter fail-
ure and/or catheter tip displacement.• PowerHohn* catheter
indication for power injection of contrast media implies the
catheter’s ability to withstand the procedure, but
does not imply appropriateness of the procedure for a particular
patient. A suitably trained clinician is responsible for
evaluatingthe health status of a patient as it pertains to a power
injection procedure.
• Pinch-off Prevention: Catheters placed percutaneously or
through a cut-down, into the subclavian vein, should be inserted at
thejunction of the outer and middle thirds of the clavicle, lateral
to the thoracic outlet. The catheter should not be inserted into
thesubclavian vein medially, because such placement can lead to
compression of the catheter between the first rib and the
clavicle,which can cause damage and even severance of the catheter.
A radiographic confirmation of catheter placement should be madeto
ensure that the catheter is not being pinched by the first rib and
clavicle. 1,2
Signs of Pinch-offClinical:• Difficulty with blood withdrawal•
Resistance to infusion of fluids• Patient position changes required
for infusion of fluids or blood withdrawalRadiologic:• Grade 1 or 2
distortion on chest X-ray.
Pinch-off should be evaluated for degree of severity prior to
explantation.Patients indicating any degree of catheter distortion
at the clavicle/first ribarea should be followed diligently. There
are grades of Pinch-off that shouldbe recognized with appropriate
chest x-ray as follows: 3,4
Precaut ions:• Carefully read and follow all instructions prior
to use.• Federal (U.S.A.) law restricts this device to sale by or
on the order of a physician.• Only qualified healthcare
practitioners should insert, manipulate and remove this catheter.•
When inserting the catheter via a subclavian approach, maintain a
horizontal trajectory when introducing the needle beneath
the clavicle. Vertical needle passage may increase the risk of
pneumothorax.• If an artery is entered, withdraw the needle and
apply manual pressure for several minutes. If the pleural space is
entered,
withdraw needle and observe patient for signs of pneumothorax.•
If the guidewire must be withdrawn while the needle is inserted,
remove both the needle and guidewire as a unit to help pre-
vent the needle from damaging or shearing the guidewire.• Do not
attempt to slide the catheter over the wire separately into the
vein. This may cause the catheter to bunch up on the wire
making advancement of the catheter into the vessel more
difficult.• Contrast media should be warmed before power injection.
• Do not grasp the catheter with any instrument that might sever or
damage the catheter. • Do not cut the catheter before removal from
vein to avoid catheter embolism.• The catheter must be secured in
place to minimize the risk of catheter breakage and embolization.•
Only medical practitioners licensed by law, trained and experienced
in proper positioning of catheters in the central venous
system using percutaneous entry (Seldinger technique) should
place this catheter.• Follow Universal Precautions when inserting
and maintaining the catheter.
Grade
Grade 0
Grade 1
Grade 2
Grade 3
Severity
No distortion
Distortion presentwithout luminalnarrowing
Distortion presentwith luminal nar-rowing
Catheter transec-tion or fracture
Recommended Action
No action.
Chest x-ray should be taken every oneto three months to monitor
progressionof pinch off to grade 2 distortion.Shoulder positioning
during chest x-rays should be noted as it can contributeto changes
in distortion grades.
Removal of the catheter should beconsidered.
Prompt removal of the catheter.
Indications For Use:PowerHohn* catheters are indicated for short
or long term access to the central venous system. They are designed
for adminis-tering I.V. fluids, blood products, drugs and
parenteral nutrition solutions, as well as blood withdrawal and
power injection ofcontrast media. The maximum recommended infusion
rate is 5ml/sec. The maximum pressure of power injectors used with
thePowerHohn* catheter may not exceed 300psi.
VitaCuff* Antimicrobial CuffDescription
The VitaCuff* device is designed to help provide protection
against infections related tovascular access catheters. The outer,
tissue-interfacing surface of the VitaCuff* device mayhelp reduce
the incidence of infection by incorporating an antimicrobial agent
into theporous collagen matrix.
The VitaCuff* device is comprised of two concentric layers of
material. The internal layer is constructed of specially
formulatedand processed medical grade silicone. The external,
tissue-interfacing layer is VitaGuard* antimicrobial collagen
matrix. Theantimicrobial activity of the VitaGuard* material is
attributable to the silver ions bound to the collagen matrix. The
activity lastsuntil the VitaGuard* matrix is completely absorbed by
the tissue in four to six weeks. (Refer to figure 1)The VitaGuard*
collagen sponge is initially in a compressed state for ease of
insertion. After placement, the matrix absorbsphysiological fluids,
quickly expands to approximately twice its original size, and helps
provide an antimicrobial barrier and aphysical barrier at the exit
site. Tissue ingrowth into the VitaGuard* collagen matrix occurs in
a few days, further securing thecatheter in place, and reducing
catheter movement.
Proper VitaCuff* Positioning
Caution: The antimicrobial cuff is not intended to be used as a
treatment for catheter related infections. The antimicrobial
cuffdoes not provide protection against “blood seeding” infection
or infusate-related infection. It is not intended to provide
protectionfrom bacteria for longer than one month. The
antimicrobial cuff should not be used on patients with known
sensitivities to silverions or collagen.
Contraindications:The device is contraindicated whenever:• The
presence of device related infection, bacteremia, or septicemia is
known or suspected.• The patient’s body size is insufficient to
accommodate the size of the implanted device.• The patient is known
or is suspected to be allergic to materials contained in the
device.• Severe chronic obstructive lung disease exists
(percutaneous subclavian placement only).• There has been past
irradiation of prospective insertion site.• There have been
previous episodes of venous thrombosis or vascular surgical
procedures at the prospective placement site.• There are local
tissue factors which prevent proper device stabilization and/or
access.• Do not use the antimicrobial cuff in patients with known
sensitivities to silver ions or collagen.
Warnings:• Intended for Single Patient Use. DO NOT REUSE. Bard
Access Systems products are single use devices and should never
be
reimplanted. Reuse carries with it the attendant concern of
cross-infection regardless of the cleaning or sterilization
method.Resterilization of incompletely cleaned devices may not be
effective. Any device that has been contaminated by blood should
notbe reused or resterilized.
• After use, this product may be a potential biohazard. Handle
and dispose of in accordance with accepted medical practice
andapplicable local, state and federal laws and regulations.
• This is not a right atrium catheter. Avoid positioning the
catheter tip in the right atrium. Placement or migration of the
catheter tipinto the right atrium may cause cardiac arrhythmia,
myocardial erosion or cardiac tamponade.
• Do not use the catheter if there is any evidence of mechanical
damage or leaking. Damage to the catheter may lead to
rupture,fragmentation, possible embolism, and surgical removal.
• If signs of extravasation exist, discontinue injections. Begin
appropriate medical intervention immediately.• The fluid level in
the catheter will drop if the catheter connector is held above the
level of the patient’s heart and opened to air. To
help prevent a drop in the fluid level (allowing air entry)
while changing injection caps, hold the connector below the level
of thepatient’s heart before removing the injection cap.
• Place a finger over the needle to minimize blood loss and risk
of air aspiration. The risk of air aspiration is reduced by
performingthis part of the procedure with the patient holding their
breath until the guidewire is inserted into the needle.
• When using alcohol or alcohol containing antiseptics with
polyurethane catheters, care should be taken to avoid prolonged
orexcessive contact. Solutions should be allowed to completely dry
before applying an occlusive dressing. Chlorhexidine glu-conate
and/or povidone iodine are the suggested antiseptics to use.
• You should not feel any resistance when withdrawing the
catheter from the vein. If you do encounter resistance, this may
indicate that
VitaCuff*AntimicrobialCuff
Exit Site
New Important Information:• Contrast media should be warmed to
body temperature prior to power injection.
Warning: Failure to warm contrast media to body temperature
prior to power injection may result incatheter failure.
• Vigorously flush the PowerHohn* catheter using a 10ml or
larger syringe and sterile normal saline priorto and immediately
following the completion of power injection studies. This will
ensure the patency ofthe PowerHohn* catheter and prevent damage to
the catheter. Resistance to flushing may indicatepartial or
complete catheter occlusion. Do not proceed with power injection
study until occlusion hasbeen cleared. Warning: Failure to ensure
patency of the catheter prior to power injection studies may result
incatheter failure.
• Do not exceed the maximum flow rate of 5ml/sec. Warning: Power
injector machine pressure limiting feature may not prevent over
pressurization of anoccluded catheter. Warning: Exceeding the
maximum flow rate of 5ml/sec may result in catheter failure and/or
cathetertip displacement.
• Warning: PowerHohn* catheter indication for power injection of
contrast media implies the catheter’sability to withstand the
procedure, but does not imply appropriateness of the procedure for
a particularpatient. A suitably trained clinician is responsible
for evaluating the health status of a patient as it pertains to a
power injection procedure.
Power Injection Procedure1. Remove the end cap(s) from the
PowerHohn* catheter.2. Attach a 10ml or larger syringe filled with
sterile normal saline.3. Aspirate for adequate blood return and
vigorously flush the catheter with the full 10ml of sterile normal
saline.
Warning: Failure to ensure patency of the catheter prior to
power injection studies may result in catheter failure.
4. Detach syringe.5. Attach the power injection device to the
PowerHohn* catheter per manufacturer’s recommendations.6. Complete
power injection study taking care not to exceed the flow rate
limits.
Warning: Exceeding the maximum flow rate of 5ml/sec may result
in catheter failure and/or catheter tip displacement.7. Disconnect
the power injection device.8. Flush the PowerHohn* catheter with
10ml of sterile normal saline, using a 10ml or larger syringe.9.
Replace the end cap(s) on the PowerHohn* catheter.
DescriptionPowerHohn* Central Venous Catheters are constructed
of specially formulated and processed polyurethane and are designed
forover-the-wire insertion into the central venous system.
PowerHohn* catheters have a kink-resistant, reverse-tapered design.
Thecatheters are radiopaque with female luer locking adapters and
StatLock* device compatible suture wings for fixation. Eachcatheter
is provided in a sterile package. Catheters are available with or
without VitaCuff* antimicrobial cuff.
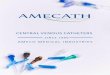
PlacementThe catheter is placed into one of the central veins so
the tip lies in the superior vena cava above the right atrium.
Schematics:
Ne
w I
mp
ort
an
t In
form
ati
on
:New Important Information:
• Follow all contraindications, warnings, cautions, precautions
and instructions for all infusates, including contrast media,
asspecified by its manufacturer.
• Use aseptic techniques whenever the catheter lumen is opened
or connected to other devices. Povidone-iodine or chlorhexa-dine
gluconate are the suggested antiseptics to use with this device and
components. Acetone and tincture of iodine shouldnot be used
because they could adversely affect the performance of the catheter
and connectors. 10% acetone/70% isopropylalcohol swabsticks used
for dressing changes should not adversely affect the catheter.
• Patients with thick muscular chest walls or extensive scar
tissue may require the use of a percutaneous introducer for
catheterinsertion.
• Catheters can be cut to length if a different length is
desired due to patient size and desired point of insertion
according to hos-pital protocol. Catheter depth markings are in
centimeters. Use caution when using scissors or any sharp-edged
instruments asthey could damage the catheter.
• Examine package carefully before opening to confirm its
integrity and that the expiration date has not passed. The catheter
issupplied in a double sterile package and is non-pyrogenic. Do not
use if package is damaged, opened or the expiration datehas passed.
Sterilized by ethylene oxide. Do not resterilize.
• Inspect kit for inclusion of all components. • When device
includes an antimicrobial cuff, do not expose the cuff to fluids
prior to insertion. Handle carefully to avoid cuff damage. • Fill
(prime) the device with sterile heparinized saline or normal saline
solution to help avoid air embolism. • When using an introducer
kit, verify that the catheter fits easily through the introducer
sheath.
• Avoid accidental device contact with sharp instruments and
mechanical damage to the catheter material. Use only smooth-edged
atraumatic clamps or forceps.
• Avoid perforating, tearing or fracturing the catheter when
using a guidewire. • Do not use the catheter if there is any
evidence of mechanical damage or leaking.• Avoid sharp or acute
angles during implantation which could compromise the patency of
the catheter lumen(s).• Sutures should not be tied around the
catheter itself. The suture wings will secure the catheter without
compromising catheter
patency. • When using percutaneous introducers:
- Carefully insert the introducer and catheter to avoid
inadvertent penetration to vital structures in the thorax.- To
avoid blood vessel damage, do not allow the percutaneous introducer
sheath to remain indwelling in the blood vessel
without the internal support of a catheter or dilator. -
Simultaneously advance the dilator with rotational motion to help
prevent damage.
• During insertion of catheter with antimicrobial cuff:-
Minimize the exposure of the cuff to pooled blood by sponging the
intended cuff placement site. - The entire collagen (tan) portion
of the cuff must be in the subcutaneous tissue at the catheter exit
site.
• Do not use the catheter if there is any evidence of mechanical
damage or leaking. Damage to the catheter may lead to rup-ture,
fragmentation and possible embolism and surgical removal.
• Accessories and components used in conjunction with this
device should incorporate luer lock connections.• If signs of
extravasation exist, discontinue injections. Begin appropriate
medical intervention immediately.• Prolonged infusion pressure
greater than 25 psi (172 kPa) may damage blood vessels and viscus
and is not recommended.
Do not use a syringe smaller than 10 ml!
Possible ComplicationsThe potential exists for serious
complications including the following.
• Air Embolism• Allergic Reaction to Silver or Collagen
(Catheters with VitaCuff* AntimicrobialCuff Only)
• Bleeding• Brachial Plexus Injury• Cardiac Arrhythmia• Cardiac
Tamponade• Catheter or Cuff Erosion Through
the Skin• Catheter Embolism• Catheter Occlusion• Catheter
Occlusion, Damage or
Breakage due to Compression betweenthe Clavicle and First Rib
(Pinch-off)
• Catheter-related Sepsis• Endocarditis• Exit Site Infection•
Exit Site Necrosis• Extravasation• Fibrin Sheath Formation•
Hematoma• Hemothroax• Hydrothorax• Intolerance Reaction to
Implanted
Device• Laceration of Vessels or Viscus• Myocardial Erosion •
Perforation of Vessels or Viscus• Phlebitis
• Pneumothorax• Spontaneous Catheter Tip Malposition
or Retraction• Thromboembolism• Thoracic Duct Injury• Venous
Thrombosis• Ventricular Thrombosis• Vessel Erosion• Risks Normally
Associated with Local
or General Anesthesia, Surgery, andPost-Operative Recovery
III. After placement:
II. During placement:
I. Prior to placement:
Hubs Thumb Clamps
ID Tags
ID Tags
Molded Junction Reverse Taper TubingVitaCuff * Antimicrobial
Cuff
1
First RibSubclavian Vein
Clavicle
Vertebra
Internal Jugular Vein
Superior Vena Cava
SternumPinch-off Area
Infraclavicular Fossa
Axillary Vein
-
the catheter is being pinched between the clavicle and first rib
(the “Pinch-off” sign). Do not continue pulling against resistance
as thismay cause catheter breakage and embolism. Free up the
resistance (e.g. by repositioning the patient) before proceeding
further.
• If the artery is entered, withdraw the needle and apply manual
pressure for several minutes. If the pleural space is entered,
with-draw the needle and evaluate patient for possible
pneumothorax.
• Alcohol should not be used to soak or declot polyurethane
catheters because alcohol is known to degrade polyurethane
cathetersover time with repeated and prolonged exposure.
• Acetone and polyethylene glycol containing ointments should
not be used with polyurethane catheters, as they may damage the
device.• Failure to warm contrast media to body temperature prior
to power injection may result in catheter failure.• Failure to
ensure patency of the catheter prior to power injection studies may
result in catheter failure.• Power injector machine pressure
limiting feature may not prevent over pressurization of an occluded
catheter.• Exceeding the maximum flow rate of 5ml/sec, and the
maximum pressure of power injectors of 300 psi, may result in
catheter fail-
ure and/or catheter tip displacement.• PowerHohn* catheter
indication for power injection of contrast media implies the
catheter’s ability to withstand the procedure, but
does not imply appropriateness of the procedure for a particular
patient. A suitably trained clinician is responsible for
evaluatingthe health status of a patient as it pertains to a power
injection procedure.
• Pinch-off Prevention: Catheters placed percutaneously or
through a cut-down, into the subclavian vein, should be inserted at
thejunction of the outer and middle thirds of the clavicle, lateral
to the thoracic outlet. The catheter should not be inserted into
thesubclavian vein medially, because such placement can lead to
compression of the catheter between the first rib and the
clavicle,which can cause damage and even severance of the catheter.
A radiographic confirmation of catheter placement should be madeto
ensure that the catheter is not being pinched by the first rib and
clavicle. 1,2
Signs of Pinch-offClinical:• Difficulty with blood withdrawal•
Resistance to infusion of fluids• Patient position changes required
for infusion of fluids or blood withdrawalRadiologic:• Grade 1 or 2
distortion on chest X-ray.
Pinch-off should be evaluated for degree of severity prior to
explantation.Patients indicating any degree of catheter distortion
at the clavicle/first ribarea should be followed diligently. There
are grades of Pinch-off that shouldbe recognized with appropriate
chest x-ray as follows: 3,4
Precaut ions:• Carefully read and follow all instructions prior
to use.• Federal (U.S.A.) law restricts this device to sale by or
on the order of a physician.• Only qualified healthcare
practitioners should insert, manipulate and remove this catheter.•
When inserting the catheter via a subclavian approach, maintain a
horizontal trajectory when introducing the needle beneath
the clavicle. Vertical needle passage may increase the risk of
pneumothorax.• If an artery is entered, withdraw the needle and
apply manual pressure for several minutes. If the pleural space is
entered,
withdraw needle and observe patient for signs of pneumothorax.•
If the guidewire must be withdrawn while the needle is inserted,
remove both the needle and guidewire as a unit to help pre-
vent the needle from damaging or shearing the guidewire.• Do not
attempt to slide the catheter over the wire separately into the
vein. This may cause the catheter to bunch up on the wire
making advancement of the catheter into the vessel more
difficult.• Contrast media should be warmed before power injection.
• Do not grasp the catheter with any instrument that might sever or
damage the catheter. • Do not cut the catheter before removal from
vein to avoid catheter embolism.• The catheter must be secured in
place to minimize the risk of catheter breakage and embolization.•
Only medical practitioners licensed by law, trained and experienced
in proper positioning of catheters in the central venous
system using percutaneous entry (Seldinger technique) should
place this catheter.• Follow Universal Precautions when inserting
and maintaining the catheter.
Grade
Grade 0
Grade 1
Grade 2
Grade 3
Severity
No distortion
Distortion presentwithout luminalnarrowing
Distortion presentwith luminal nar-rowing
Catheter transec-tion or fracture
Recommended Action
No action.
Chest x-ray should be taken every oneto three months to monitor
progressionof pinch off to grade 2 distortion.Shoulder positioning
during chest x-rays should be noted as it can contributeto changes
in distortion grades.
Removal of the catheter should beconsidered.
Prompt removal of the catheter.
Indications For Use:PowerHohn* catheters are indicated for short
or long term access to the central venous system. They are designed
for adminis-tering I.V. fluids, blood products, drugs and
parenteral nutrition solutions, as well as blood withdrawal and
power injection ofcontrast media. The maximum recommended infusion
rate is 5ml/sec. The maximum pressure of power injectors used with
thePowerHohn* catheter may not exceed 300psi.
VitaCuff* Antimicrobial CuffDescription
The VitaCuff* device is designed to help provide protection
against infections related tovascular access catheters. The outer,
tissue-interfacing surface of the VitaCuff* device mayhelp reduce
the incidence of infection by incorporating an antimicrobial agent
into theporous collagen matrix.
The VitaCuff* device is comprised of two concentric layers of
material. The internal layer is constructed of specially
formulatedand processed medical grade silicone. The external,
tissue-interfacing layer is VitaGuard* antimicrobial collagen
matrix. Theantimicrobial activity of the VitaGuard* material is
attributable to the silver ions bound to the collagen matrix. The
activity lastsuntil the VitaGuard* matrix is completely absorbed by
the tissue in four to six weeks. (Refer to figure 1)The VitaGuard*
collagen sponge is initially in a compressed state for ease of
insertion. After placement, the matrix absorbsphysiological fluids,
quickly expands to approximately twice its original size, and helps
provide an antimicrobial barrier and aphysical barrier at the exit
site. Tissue ingrowth into the VitaGuard* collagen matrix occurs in
a few days, further securing thecatheter in place, and reducing
catheter movement.
Proper VitaCuff* Positioning
Caution: The antimicrobial cuff is not intended to be used as a
treatment for catheter related infections. The antimicrobial
cuffdoes not provide protection against “blood seeding” infection
or infusate-related infection. It is not intended to provide
protectionfrom bacteria for longer than one month. The
antimicrobial cuff should not be used on patients with known
sensitivities to silverions or collagen.
Contraindications:The device is contraindicated whenever:• The
presence of device related infection, bacteremia, or septicemia is
known or suspected.• The patient’s body size is insufficient to
accommodate the size of the implanted device.• The patient is known
or is suspected to be allergic to materials contained in the
device.• Severe chronic obstructive lung disease exists
(percutaneous subclavian placement only).• There has been past
irradiation of prospective insertion site.• There have been
previous episodes of venous thrombosis or vascular surgical
procedures at the prospective placement site.• There are local
tissue factors which prevent proper device stabilization and/or
access.• Do not use the antimicrobial cuff in patients with known
sensitivities to silver ions or collagen.
Warnings:• Intended for Single Patient Use. DO NOT REUSE. Bard
Access Systems products are single use devices and should never
be
reimplanted. Reuse carries with it the attendant concern of
cross-infection regardless of the cleaning or sterilization
method.Resterilization of incompletely cleaned devices may not be
effective. Any device that has been contaminated by blood should
notbe reused or resterilized.
• After use, this product may be a potential biohazard. Handle
and dispose of in accordance with accepted medical practice
andapplicable local, state and federal laws and regulations.
• This is not a right atrium catheter. Avoid positioning the
catheter tip in the right atrium. Placement or migration of the
catheter tipinto the right atrium may cause cardiac arrhythmia,
myocardial erosion or cardiac tamponade.
• Do not use the catheter if there is any evidence of mechanical
damage or leaking. Damage to the catheter may lead to
rupture,fragmentation, possible embolism, and surgical removal.
• If signs of extravasation exist, discontinue injections. Begin
appropriate medical intervention immediately.• The fluid level in
the catheter will drop if the catheter connector is held above the
level of the patient’s heart and opened to air. To
help prevent a drop in the fluid level (allowing air entry)
while changing injection caps, hold the connector below the level
of thepatient’s heart before removing the injection cap.
• Place a finger over the needle to minimize blood loss and risk
of air aspiration. The risk of air aspiration is reduced by
performingthis part of the procedure with the patient holding their
breath until the guidewire is inserted into the needle.
• When using alcohol or alcohol containing antiseptics with
polyurethane catheters, care should be taken to avoid prolonged
orexcessive contact. Solutions should be allowed to completely dry
before applying an occlusive dressing. Chlorhexidine glu-conate
and/or povidone iodine are the suggested antiseptics to use.
• You should not feel any resistance when withdrawing the
catheter from the vein. If you do encounter resistance, this may
indicate that
VitaCuff*AntimicrobialCuff
Exit Site
New Important Information:• Contrast media should be warmed to
body temperature prior to power injection.
Warning: Failure to warm contrast media to body temperature
prior to power injection may result incatheter failure.
• Vigorously flush the PowerHohn* catheter using a 10ml or
larger syringe and sterile normal saline priorto and immediately
following the completion of power injection studies. This will
ensure the patency ofthe PowerHohn* catheter and prevent damage to
the catheter. Resistance to flushing may indicatepartial or
complete catheter occlusion. Do not proceed with power injection
study until occlusion hasbeen cleared. Warning: Failure to ensure
patency of the catheter prior to power injection studies may result
incatheter failure.
• Do not exceed the maximum flow rate of 5ml/sec. Warning: Power
injector machine pressure limiting feature may not prevent over
pressurization of anoccluded catheter. Warning: Exceeding the
maximum flow rate of 5ml/sec may result in catheter failure and/or
cathetertip displacement.
• Warning: PowerHohn* catheter indication for power injection of
contrast media implies the catheter’sability to withstand the
procedure, but does not imply appropriateness of the procedure for
a particularpatient. A suitably trained clinician is responsible
for evaluating the health status of a patient as it pertains to a
power injection procedure.
Power Injection Procedure1. Remove the end cap(s) from the
PowerHohn* catheter.2. Attach a 10ml or larger syringe filled with
sterile normal saline.3. Aspirate for adequate blood return and
vigorously flush the catheter with the full 10ml of sterile normal
saline.
Warning: Failure to ensure patency of the catheter prior to
power injection studies may result in catheter failure.
4. Detach syringe.5. Attach the power injection device to the
PowerHohn* catheter per manufacturer’s recommendations.6. Complete
power injection study taking care not to exceed the flow rate
limits.
Warning: Exceeding the maximum flow rate of 5ml/sec may result
in catheter failure and/or catheter tip displacement.7. Disconnect
the power injection device.8. Flush the PowerHohn* catheter with
10ml of sterile normal saline, using a 10ml or larger syringe.9.
Replace the end cap(s) on the PowerHohn* catheter.
DescriptionPowerHohn* Central Venous Catheters are constructed
of specially formulated and processed polyurethane and are designed
forover-the-wire insertion into the central venous system.
PowerHohn* catheters have a kink-resistant, reverse-tapered design.
Thecatheters are radiopaque with female luer locking adapters and
StatLock* device compatible suture wings for fixation. Eachcatheter
is provided in a sterile package. Catheters are available with or
without VitaCuff* antimicrobial cuff.
PlacementThe catheter is placed into one of the central veins so
the tip lies in the superior vena cava above the right atrium.
Schematics:
Ne
w I
mp
ort
an
t In
form
ati
on
:
New Important Information:• Follow all contraindications,
warnings, cautions, precautions and instructions for all infusates,
including contrast media, as
specified by its manufacturer. • Use aseptic techniques whenever
the catheter lumen is opened or connected to other devices.
Povidone-iodine or chlorhexa-
dine gluconate are the suggested antiseptics to use with this
device and components. Acetone and tincture of iodine shouldnot be
used because they could adversely affect the performance of the
catheter and connectors. 10% acetone/70% isopropylalcohol
swabsticks used for dressing changes should not adversely affect
the catheter.
• Patients with thick muscular chest walls or extensive scar
tissue may require the use of a percutaneous introducer for
catheterinsertion.
• Catheters can be cut to length if a different length is
desired due to patient size and desired point of insertion
according to hos-pital protocol. Catheter depth markings are in
centimeters. Use caution when using scissors or any sharp-edged
instruments asthey could damage the catheter.
• Examine package carefully before opening to confirm its
integrity and that the expiration date has not passed. The catheter
issupplied in a double sterile package and is non-pyrogenic. Do not
use if package is damaged, opened or the expiration datehas passed.
Sterilized by ethylene oxide. Do not resterilize.
• Inspect kit for inclusion of all components. • When device
includes an antimicrobial cuff, do not expose the cuff to fluids
prior to insertion. Handle carefully to avoid cuff damage. • Fill
(prime) the device with sterile heparinized saline or normal saline
solution to help avoid air embolism. • When using an introducer
kit, verify that the catheter fits easily through the introducer
sheath.
• Avoid accidental device contact with sharp instruments and
mechanical damage to the catheter material. Use only smooth-edged
atraumatic clamps or forceps.
• Avoid perforating, tearing or fracturing the catheter when
using a guidewire. • Do not use the catheter if there is any
evidence of mechanical damage or leaking.• Avoid sharp or acute
angles during implantation which could compromise the patency of
the catheter lumen(s).• Sutures should not be tied around the
catheter itself. The suture wings will secure the catheter without
compromising catheter
patency. • When using percutaneous introducers:
- Carefully insert the introducer and catheter to avoid
inadvertent penetration to vital structures in the thorax.- To
avoid blood vessel damage, do not allow the percutaneous introducer
sheath to remain indwelling in the blood vessel
without the internal support of a catheter or dilator. -
Simultaneously advance the dilator with rotational motion to help
prevent damage.
• During insertion of catheter with antimicrobial cuff:-
Minimize the exposure of the cuff to pooled blood by sponging the
intended cuff placement site. - The entire collagen (tan) portion
of the cuff must be in the subcutaneous tissue at the catheter exit
site.
• Do not use the catheter if there is any evidence of mechanical
damage or leaking. Damage to the catheter may lead to rup-ture,
fragmentation and possible embolism and surgical removal.
• Accessories and components used in conjunction with this
device should incorporate luer lock connections.• If signs of
extravasation exist, discontinue injections. Begin appropriate
medical intervention immediately.• Prolonged infusion pressure
greater than 25 psi (172 kPa) may damage blood vessels and viscus
and is not recommended.
Do not use a syringe smaller than 10 ml!
Possible ComplicationsThe potential exists for serious
complications including the following.
• Air Embolism• Allergic Reaction to Silver or Collagen
(Catheters with VitaCuff* AntimicrobialCuff Only)
• Bleeding• Brachial Plexus Injury• Cardiac Arrhythmia• Cardiac
Tamponade• Catheter or Cuff Erosion Through
the Skin• Catheter Embolism• Catheter Occlusion• Catheter
Occlusion, Damage or
Breakage due to Compression betweenthe Clavicle and First Rib
(Pinch-off)
• Catheter-related Sepsis• Endocarditis• Exit Site Infection•
Exit Site Necrosis• Extravasation• Fibrin Sheath Formation•
Hematoma• Hemothroax• Hydrothorax• Intolerance Reaction to
Implanted
Device• Laceration of Vessels or Viscus• Myocardial Erosion •
Perforation of Vessels or Viscus• Phlebitis
• Pneumothorax• Spontaneous Catheter Tip Malposition
or Retraction• Thromboembolism• Thoracic Duct Injury• Venous
Thrombosis• Ventricular Thrombosis• Vessel Erosion• Risks Normally
Associated with Local
or General Anesthesia, Surgery, andPost-Operative Recovery
III. After placement:
II. During placement:
I. Prior to placement:
Hubs Thumb Clamps
ID Tags
ID Tags
Molded Junction Reverse Taper TubingVitaCuff * Antimicrobial
Cuff
1
First RibSubclavian Vein
Clavicle
Vertebra
Internal Jugular Vein
Superior Vena Cava
SternumPinch-off Area
Infraclavicular Fossa
Axillary Vein
-
the catheter is being pinched between the clavicle and first rib
(the “Pinch-off” sign). Do not continue pulling against resistance
as thismay cause catheter breakage and embolism. Free up the
resistance (e.g. by repositioning the patient) before proceeding
further.
• If the artery is entered, withdraw the needle and apply manual
pressure for several minutes. If the pleural space is entered,
with-draw the needle and evaluate patient for possible
pneumothorax.
• Alcohol should not be used to soak or declot polyurethane
catheters because alcohol is known to degrade polyurethane
cathetersover time with repeated and prolonged exposure.
• Acetone and polyethylene glycol containing ointments should
not be used with polyurethane catheters, as they may damage the
device.• Failure to warm contrast media to body temperature prior
to power injection may result in catheter failure.• Failure to
ensure patency of the catheter prior to power injection studies may
result in catheter failure.• Power injector machine pressure
limiting feature may not prevent over pressurization of an occluded
catheter.• Exceeding the maximum flow rate of 5ml/sec, and the
maximum pressure of power injectors of 300 psi, may result in
catheter fail-
ure and/or catheter tip displacement.• PowerHohn* catheter
indication for power injection of contrast media implies the
catheter’s ability to withstand the procedure, but
does not imply appropriateness of the procedure for a particular
patient. A suitably trained clinician is responsible for
evaluatingthe health status of a patient as it pertains to a power
injection procedure.
• Pinch-off Prevention: Catheters placed percutaneously or
through a cut-down, into the subclavian vein, should be inserted at
thejunction of the outer and middle thirds of the clavicle, lateral
to the thoracic outlet. The catheter should not be inserted into
thesubclavian vein medially, because such placement can lead to
compression of the catheter between the first rib and the
clavicle,which can cause damage and even severance of the catheter.
A radiographic confirmation of catheter placement should be madeto
ensure that the catheter is not being pinched by the first rib and
clavicle. 1,2
Signs of Pinch-offClinical:• Difficulty with blood withdrawal•
Resistance to infusion of fluids• Patient position changes required
for infusion of fluids or blood withdrawalRadiologic:• Grade 1 or 2
distortion on chest X-ray.
Pinch-off should be evaluated for degree of severity prior to
explantation.Patients indicating any degree of catheter distortion
at the clavicle/first ribarea should be followed diligently. There
are grades of Pinch-off that shouldbe recognized with appropriate
chest x-ray as follows: 3,4
Precaut ions:• Carefully read and follow all instructions prior
to use.• Federal (U.S.A.) law restricts this device to sale by or
on the order of a physician.• Only qualified healthcare
practitioners should insert, manipulate and remove this catheter.•
When inserting the catheter via a subclavian approach, maintain a
horizontal trajectory when introducing the needle beneath
the clavicle. Vertical needle passage may increase the risk of
pneumothorax.• If an artery is entered, withdraw the needle and
apply manual pressure for several minutes. If the pleural space is
entered,
withdraw needle and observe patient for signs of pneumothorax.•
If the guidewire must be withdrawn while the needle is inserted,
remove both the needle and guidewire as a unit to help pre-
vent the needle from damaging or shearing the guidewire.• Do not
attempt to slide the catheter over the wire separately into the
vein. This may cause the catheter to bunch up on the wire
making advancement of the catheter into the vessel more
difficult.• Contrast media should be warmed before power injection.
• Do not grasp the catheter with any instrument that might sever or
damage the catheter. • Do not cut the catheter before removal from
vein to avoid catheter embolism.• The catheter must be secured in
place to minimize the risk of catheter breakage and embolization.•
Only medical practitioners licensed by law, trained and experienced
in proper positioning of catheters in the central venous
system using percutaneous entry (Seldinger technique) should
place this catheter.• Follow Universal Precautions when inserting
and maintaining the catheter.
Grade
Grade 0
Grade 1
Grade 2
Grade 3
Severity
No distortion
Distortion presentwithout luminalnarrowing
Distortion presentwith luminal nar-rowing
Catheter transec-tion or fracture
Recommended Action
No action.
Chest x-ray should be taken every oneto three months to monitor
progressionof pinch off to grade 2 distortion.Shoulder positioning
during chest x-rays should be noted as it can contributeto changes
in distortion grades.
Removal of the catheter should beconsidered.
Prompt removal of the catheter.
Indications For Use:PowerHohn* catheters are indicated for short
or long term access to the central venous system. They are designed
for adminis-tering I.V. fluids, blood products, drugs and
parenteral nutrition solutions, as well as blood withdrawal and
power injection ofcontrast media. The maximum recommended infusion
rate is 5ml/sec. The maximum pressure of power injectors used with
thePowerHohn* catheter may not exceed 300psi.
VitaCuff* Antimicrobial CuffDescription
The VitaCuff* device is designed to help provide protection
against infections related tovascular access catheters. The outer,
tissue-interfacing surface of the VitaCuff* device mayhelp reduce
the incidence of infection by incorporating an antimicrobial agent
into theporous collagen matrix.
The VitaCuff* device is comprised of two concentric layers of
material. The internal layer is constructed of specially
formulatedand processed medical grade silicone. The external,
tissue-interfacing layer is VitaGuard* antimicrobial collagen
matrix. Theantimicrobial activity of the VitaGuard* material is
attributable to the silver ions bound to the collagen matrix. The
activity lastsuntil the VitaGuard* matrix is completely absorbed by
the tissue in four to six weeks. (Refer to figure 1)The VitaGuard*
collagen sponge is initially in a compressed state for ease of
insertion. After placement, the matrix absorbsphysiological fluids,
quickly expands to approximately twice its original size, and helps
provide an antimicrobial barrier and aphysical barrier at the exit
site. Tissue ingrowth into the VitaGuard* collagen matrix occurs in
a few days, further securing thecatheter in place, and reducing
catheter movement.
Proper VitaCuff* Positioning
Caution: The antimicrobial cuff is not intended to be used as a
treatment for catheter related infections. The antimicrobial
cuffdoes not provide protection against “blood seeding” infection
or infusate-related infection. It is not intended to provide
protectionfrom bacteria for longer than one month. The
antimicrobial cuff should not be used on patients with known
sensitivities to silverions or collagen.
Contraindications:The device is contraindicated whenever:• The
presence of device related infection, bacteremia, or septicemia is
known or suspected.• The patient’s body size is insufficient to
accommodate the size of the implanted device.• The patient is known
or is suspected to be allergic to materials contained in the
device.• Severe chronic obstructive lung disease exists
(percutaneous subclavian placement only).• There has been past
irradiation of prospective insertion site.• There have been
previous episodes of venous thrombosis or vascular surgical
procedures at the prospective placement site.• There are local
tissue factors which prevent proper device stabilization and/or
access.• Do not use the antimicrobial cuff in patients with known
sensitivities to silver ions or collagen.
Warnings:• Intended for Single Patient Use. DO NOT REUSE. Bard
Access Systems products are single use devices and should never
be
reimplanted. Reuse carries with it the attendant concern of
cross-infection regardless of the cleaning or sterilization
method.Resterilization of incompletely cleaned devices may not be
effective. Any device that has been contaminated by blood should
notbe reused or resterilized.
• After use, this product may be a potential biohazard. Handle
and dispose of in accordance with accepted medical practice
andapplicable local, state and federal laws and regulations.
• This is not a right atrium catheter. Avoid positioning the
catheter tip in the right atrium. Placement or migration of the
catheter tipinto the right atrium may cause cardiac arrhythmia,
myocardial erosion or cardiac tamponade.
• Do not use the catheter if there is any evidence of mechanical
damage or leaking. Damage to the catheter may lead to
rupture,fragmentation, possible embolism, and surgical removal.
• If signs of extravasation exist, discontinue injections. Begin
appropriate medical intervention immediately.• The fluid level in
the catheter will drop if the catheter connector is held above the
level of the patient’s heart and opened to air. To
help prevent a drop in the fluid level (allowing air entry)
while changing injection caps, hold the connector below the level
of thepatient’s heart before removing the injection cap.
• Place a finger over the needle to minimize blood loss and risk
of air aspiration. The risk of air aspiration is reduced by
performingthis part of the procedure with the patient holding their
breath until the guidewire is inserted into the needle.
• When using alcohol or alcohol containing antiseptics with
polyurethane catheters, care should be taken to avoid prolonged
orexcessive contact. Solutions should be allowed to completely dry
before applying an occlusive dressing. Chlorhexidine glu-conate
and/or povidone iodine are the suggested antiseptics to use.
• You should not feel any resistance when withdrawing the
catheter from the vein. If you do encounter resistance, this may
indicate that
VitaCuff*AntimicrobialCuff
Exit Site
New Important Information:• Contrast media should be warmed to
body temperature prior to power injection.
Warning: Failure to warm contrast media to body temperature
prior to power injection may result incatheter failure.
• Vigorously flush the PowerHohn* catheter using a 10ml or
larger syringe and sterile normal saline priorto and immediately
following the completion of power injection studies. This will
ensure the patency ofthe PowerHohn* catheter and prevent damage to
the catheter. Resistance to flushing may indicatepartial or
complete catheter occlusion. Do not proceed with power injection
study until occlusion hasbeen cleared. Warning: Failure to ensure
patency of the catheter prior to power injection studies may result
incatheter failure.
• Do not exceed the maximum flow rate of 5ml/sec. Warning: Power
injector machine pressure limiting feature may not prevent over
pressurization of anoccluded catheter. Warning: Exceeding the
maximum flow rate of 5ml/sec may result in catheter failure and/or
cathetertip displacement.
• Warning: PowerHohn* catheter indication for power injection of
contrast media implies the catheter’sability to withstand the
procedure, but does not imply appropriateness of the procedure for
a particularpatient. A suitably trained clinician is responsible
for evaluating the health status of a patient as it pertains to a
power injection procedure.
Power Injection Procedure1. Remove the end cap(s) from the
PowerHohn* catheter.2. Attach a 10ml or larger syringe filled with
sterile normal saline.3. Aspirate for adequate blood return and
vigorously flush the catheter with the full 10ml of sterile normal
saline.
Warning: Failure to ensure patency of the catheter prior to
power injection studies may result in catheter failure.
4. Detach syringe.5. Attach the power injection device to the
PowerHohn* catheter per manufacturer’s recommendations.6. Complete
power injection study taking care not to exceed the flow rate
limits.
Warning: Exceeding the maximum flow rate of 5ml/sec may result
in catheter failure and/or catheter tip displacement.7. Disconnect
the power injection device.8. Flush the PowerHohn* catheter with
10ml of sterile normal saline, using a 10ml or larger syringe.9.
Replace the end cap(s) on the PowerHohn* catheter.
DescriptionPowerHohn* Central Venous Catheters are constructed
of specially formulated and processed polyurethane and are designed
forover-the-wire insertion into the central venous system.
PowerHohn* catheters have a kink-resistant, reverse-tapered design.
Thecatheters are radiopaque with female luer locking adapters and
StatLock* device compatible suture wings for fixation. Eachcatheter
is provided in a sterile package. Catheters are available with or
without VitaCuff* antimicrobial cuff.
PlacementThe catheter is placed into one of the central veins so
the tip lies in the superior vena cava above the right atrium.
Schematics:
Ne
w I
mp
ort
an
t In
form
ati
on
:
New Important Information:• Follow all contraindications,
warnings, cautions, precautions and instructions for all infusates,
including contrast media, as
specified by its manufacturer. • Use aseptic techniques whenever
the catheter lumen is opened or connected to other devices.
Povidone-iodine or chlorhexa-
dine gluconate are the suggested antiseptics to use with this
device and components. Acetone and tincture of iodine shouldnot be
used because they could adversely affect the performance of the
catheter and connectors. 10% acetone/70% isopropylalcohol
swabsticks used for dressing changes should not adversely affect
the catheter.
• Patients with thick muscular chest walls or extensive scar
tissue may require the use of a percutaneous introducer for
catheterinsertion.
• Catheters can be cut to length if a different length is
desired due to patient size and desired point of insertion
according to hos-pital protocol. Catheter depth markings are in
centimeters. Use caution when using scissors or any sharp-edged
instruments asthey could damage the catheter.
• Examine package carefully before opening to confirm its
integrity and that the expiration date has not passed. The catheter
issupplied in a double sterile package and is non-pyrogenic. Do not
use if package is damaged, opened or the expiration datehas passed.
Sterilized by ethylene oxide. Do not resterilize.
• Inspect kit for inclusion of all components. • When device
includes an antimicrobial cuff, do not expose the cuff to fluids
prior to insertion. Handle carefully to avoid cuff damage. • Fill
(prime) the device with sterile heparinized saline or normal saline
solution to help avoid air embolism. • When using an introducer
kit, verify that the catheter fits easily through the introducer
sheath.
• Avoid accidental device contact with sharp instruments and
mechanical damage to the catheter material. Use only smooth-edged
atraumatic clamps or forceps.
• Avoid perforating, tearing or fracturing the catheter when
using a guidewire. • Do not use the catheter if there is any
evidence of mechanical damage or leaking.• Avoid sharp or acute
angles during implantation which could compromise the patency of
the catheter lumen(s).• Sutures should not be tied around the
catheter itself. The suture wings will secure the catheter without
compromising catheter
patency. • When using percutaneous introducers:
- Carefully insert the introducer and catheter to avoid
inadvertent penetration to vital structures in the thorax.- To
avoid blood vessel damage, do not allow the percutaneous introducer
sheath to remain indwelling in the blood vessel
without the internal support of a catheter or dilator. -
Simultaneously advance the dilator with rotational motion to help
prevent damage.
• During insertion of catheter with antimicrobial cuff:-
Minimize the exposure of the cuff to pooled blood by sponging the
intended cuff placement site. - The entire collagen (tan) portion
of the cuff must be in the subcutaneous tissue at the catheter exit
site.
• Do not use the catheter if there is any evidence of mechanical
damage or leaking. Damage to the catheter may lead to rup-ture,
fragmentation and possible embolism and surgical removal.
• Accessories and components used in conjunction with this
device should incorporate luer lock connections.• If signs of
extravasation exist, discontinue injections. Begin appropriate
medical intervention immediately.• Prolonged infusion pressure
greater than 25 psi (172 kPa) may damage blood vessels and viscus
and is not recommended.
Do not use a syringe smaller than 10 ml!
Possible ComplicationsThe potential exists for serious
complications including the following.
• Air Embolism• Allergic Reaction to Silver or Collagen
(Catheters with VitaCuff* AntimicrobialCuff Only)
• Bleeding• Brachial Plexus Injury• Cardiac Arrhythmia• Cardiac
Tamponade• Catheter or Cuff Erosion Through
the Skin• Catheter Embolism• Catheter Occlusion• Catheter
Occlusion, Damage or
Breakage due to Compression betweenthe Clavicle and First Rib
(Pinch-off)
• Catheter-related Sepsis• Endocarditis• Exit Site Infection•
Exit Site Necrosis• Extravasation• Fibrin Sheath Formation•
Hematoma• Hemothroax• Hydrothorax• Intolerance Reaction to
Implanted
Device• Laceration of Vessels or Viscus• Myocardial Erosion •
Perforation of Vessels or Viscus• Phlebitis
• Pneumothorax• Spontaneous Catheter Tip Malposition
or Retraction• Thromboembolism• Thoracic Duct Injury• Venous
Thrombosis• Ventricular Thrombosis• Vessel Erosion• Risks Normally
Associated with Local
or General Anesthesia, Surgery, andPost-Operative Recovery
III. After placement:
II. During placement:
I. Prior to placement:
Hubs Thumb Clamps
ID Tags
ID Tags
Molded Junction Reverse Taper TubingVitaCuff * Antimicrobial
Cuff
1
First RibSubclavian Vein
Clavicle
Vertebra
Internal Jugular Vein
Superior Vena Cava
SternumPinch-off Area
Infraclavicular Fossa
Axillary Vein
-
the catheter is being pinched between the clavicle and first rib
(the “Pinch-off” sign). Do not continue pulling against resistance
as thismay cause catheter breakage and embolism. Free up the
resistance (e.g. by repositioning the patient) before proceeding
further.
• If the artery is entered, withdraw the needle and apply manual
pressure for several minutes. If the pleural space is entered,
with-draw the needle and evaluate patient for possible
pneumothorax.
• Alcohol should not be used to soak or declot polyurethane
catheters because alcohol is known to degrade polyurethane
cathetersover time with repeated and prolonged exposure.
• Acetone and polyethylene glycol containing ointments should
not be used with polyurethane catheters, as they may damage the
device.• Failure to warm contrast media to body temperature prior
to power injection may result in catheter failure.• Failure to
ensure patency of the catheter prior to power injection studies may
result in catheter failure.• Power injector machine pressure
limiting feature may not prevent over pressurization of an occluded
catheter.• Exceeding the maximum flow rate of 5ml/sec, and the
maximum pressure of power injectors of 300 psi, may result in
catheter fail-
ure and/or catheter tip displacement.• PowerHohn* catheter
indication for power injection of contrast media implies the
catheter’s ability to withstand the procedure, but
does not imply appropriateness of the procedure for a particular
patient. A suitably trained clinician is responsible for
evaluatingthe health status of a patient as it pertains to a power
injection procedure.
• Pinch-off Prevention: Catheters placed percutaneously or
through a cut-down, into the subclavian vein, should be inserted at
thejunction of the outer and middle thirds of the clavicle, lateral
to the thoracic outlet. The catheter should not be inserted into
thesubclavian vein medially, because such placement can lead to
compression of the catheter between the first rib and the
clavicle,which can cause damage and even severance of the catheter.
A radiographic confirmation of catheter placement should be madeto
ensure that the catheter is not being pinched by the first rib and
clavicle. 1,2
Signs of Pinch-offClinical:• Difficulty with blood withdrawal•
Resistance to infusion of fluids• Patient position changes required
for infusion of fluids or blood withdrawalRadiologic:• Grade 1 or 2
distortion on chest X-ray.
Pinch-off should be evaluated for degree of severity prior to
explantation.Patients indicating any degree of catheter distortion
at the clavicle/first ribarea should be followed diligently. There
are grades of Pinch-off that shouldbe recognized with appropriate
chest x-ray as follows: 3,4
Precaut ions:• Carefully read and follow all instructions prior
to use.• Federal (U.S.A.) law restricts this device to sale by or
on the order of a physician.• Only qualified healthcare
practitioners should insert, manipulate and remove this catheter.•
When inserting the catheter via a subclavian approach, maintain a
horizontal trajectory when introducing the needle beneath
the clavicle. Vertical needle passage may increase the risk of
pneumothorax.• If an artery is entered, withdraw the needle and
apply manual pressure for several minutes. If the pleural space is
entered,
withdraw needle and observe patient for signs of pneumothorax.•
If the guidewire must be withdrawn while the needle is inserted,
remove both the needle and guidewire as a unit to help pre-
vent the needle from damaging or shearing the guidewire.• Do not
attempt to slide the catheter over the wire separately into the
vein. This may cause the catheter to bunch up on the wire
making advancement of the catheter into the vessel more
difficult.• Contrast media should be warmed before power injection.
• Do not grasp the catheter with any instrument that might sever or
damage the catheter. • Do not cut the catheter before removal from
vein to avoid catheter embolism.• The catheter must be secured in
place to minimize the risk of catheter breakage and embolization.•
Only medical practitioners licensed by law, trained and experienced
in proper positioning of catheters in the central venous
system using percutaneous entry (Seldinger technique) should
place this catheter.• Follow Universal Precautions when inserting
and maintaining the catheter.
Grade
Grade 0
Grade 1
Grade 2
Grade 3
Severity
No distortion
Distortion presentwithout luminalnarrowing
Distortion presentwith luminal nar-rowing
Catheter transec-tion or fracture
Recommended Action
No action.
Chest x-ray should be taken every oneto three months to monitor
progressionof pinch off to grade 2 distortion.Shoulder positioning
during chest x-rays should be noted as it can contributeto changes
in distortion grades.
Removal of the catheter should beconsidered.
Prompt removal of the catheter.
Indications For Use:PowerHohn* catheters are indicated for short
or long term access to the central venous system. They are designed
for adminis-tering I.V. fluids, blood products, drugs and
parenteral nutrition solutions, as well as blood withdrawal and
power injection ofcontrast media. The maximum recommended infusion
rate is 5ml/sec. The maximum pressure of power injectors used with
thePowerHohn* catheter may not exceed 300psi.
VitaCuff* Antimicrobial CuffDescription
The VitaCuff* device is designed to help provide protection
against infections related tovascular access catheters. The outer,
tissue-interfacing surface of the VitaCuff* device mayhelp reduce
the incidence of infection by incorporating an antimicrobial agent
into theporous collagen matrix.
The VitaCuff* device is comprised of two concentric layers of
material. The internal layer is constructed of specially
formulatedand processed medical grade silicone. The external,
tissue-interfacing layer is VitaGuard* antimicrobial collagen
matrix. Theantimicrobial activity of the VitaGuard* material is
attributable to the silver ions bound to the collagen matrix. The
activity lastsuntil the VitaGuard* matrix is completely absorbed by
the tissue in four to six weeks. (Refer to figure 1)The VitaGuard*
collagen sponge is initially in a compressed state for ease of
insertion. After placement, the matrix absorbsphysiological fluids,
quickly expands to approximately twice its original size, and helps
provide an antimicrobial barrier and aphysical barrier at the exit
site. Tissue ingrowth into the VitaGuard* collagen matrix occurs in
a few days, further securing thecatheter in place, and reducing
catheter movement.
Proper VitaCuff* Positioning
Caution: The antimicrobial cuff is not intended to be used as a
treatment for catheter related infections. The antimicrobial
cuffdoes not provide protection against “blood seeding” infection
or infusate-related infection. It is not intended to provide
protectionfrom bacteria for longer than one month. The
antimicrobial cuff should not be used on patients with known
sensitivities to silverions or collagen.
Contraindications:The device is contraindicated whenever:• The
presence of device related infection, bacteremia, or septicemia is
known or suspected.• The patient’s body size is insufficient to
accommodate the size of the implanted device.• The patient is known
or is suspected to be allergic to materials contained in the
device.• Severe chronic obstructive lung disease exists
(percutaneous subclavian placement only).• There has been past
irradiation of prospective insertion site.• There have been
previous episodes of venous thrombosis or vascular surgical
procedures at the prospective placement site.• There are local
tissue factors which prevent proper device stabilization and/or
access.• Do not use the antimicrobial cuff in patients with known
sensitivities to silver ions or collagen.
Warnings:• Intended for Single Patient Use. DO NOT REUSE. Bard
Access Systems products are single use devices and should never
be
reimplanted. Reuse carries with it the attendant concern of
cross-infection regardless of the cleaning or sterilization
method.Resterilization of incompletely cleaned devices may not be
effective. Any device that has been contaminated by blood should
notbe reused or resterilized.
• After use, this product may be a potential biohazard. Handle
and dispose of in accordance with accepted medical practice
andapplicable local, state and federal laws and regulations.
• This is not a right atrium catheter. Avoid positioning the
catheter tip in the right atrium. Placement or migration of the
catheter tipinto the right atrium may cause cardiac arrhythmia,
myocardial erosion or cardiac tamponade.
• Do not use the catheter if there is any evidence of mechanical
damage or leaking. Damage to the catheter may lead to
rupture,fragmentation, possible embolism, and surgical removal.
• If signs of extravasation exist, discontinue injections. Begin
appropriate medical intervention immediately.• The fluid level in
the catheter will drop if the catheter connector is held above the
level of the patient’s heart and opened to air. To
help prevent a drop in the fluid level (allowing air entry)
while changing injection caps, hold the connector below the level
of thepatient’s heart before removing the injection cap.
• Place a finger over the needle to minimize blood loss and risk
of air aspiration. The risk of air aspiration is reduced by
performingthis part of the procedure with the patient holding their
breath until the guidewire is inserted into the needle.
• When using alcohol or alcohol containing antiseptics with
polyurethane catheters, care should be taken to avoid prolonged
orexcessive contact. Solutions should be allowed to completely dry
before applying an occlusive dressing. Chlorhexidine glu-conate
and/or povidone iodine are the suggested antiseptics to use.
• You should not feel any resistance when withdrawing the
catheter from the vein. If you do encounter resistance, this may
indicate that
VitaCuff*AntimicrobialCuff
Exit Site
New Important Information:• Contrast media should be warmed to
body temperature prior to power injection.
Warning: Failure to warm contrast media to body temperature
prior to power injection may result incatheter failure.
• Vigorously flush the PowerHohn* catheter using a 10ml or
larger syringe and sterile normal saline priorto and immediately
following the completion of power injection studies. This will
ensure the patency ofthe PowerHohn* catheter and prevent damage to
the catheter. Resistance to flushing may indicatepartial or
complete catheter occlusion. Do not proceed with power injection
study until occlusion hasbeen cleared. Warning: Failure to ensure
patency of the catheter prior to power injection studies may result
incatheter failure.
• Do not exceed the maximum flow rate of 5ml/sec. Warning: Power
injector machine pressure limiting feature may not prevent over
pressurization of anoccluded catheter. Warning: Exceeding the
maximum flow rate of 5ml/sec may result in catheter failure and/or
cathetertip displacement.
• Warning: PowerHohn* catheter indication for power injection of
contrast media implies the catheter’sability to withstand the
procedure, but does not imply appropriateness of the procedure for
a particularpatient. A suitably trained clinician is responsible
for evaluating the health status of a patient as it pertains to a
power injection procedure.
Power Injection Procedure1. Remove the end cap(s) from the
PowerHohn* catheter.2. Attach a 10ml or larger syringe filled with
sterile normal saline.3. Aspirate for adequate blood return and
vigorously flush the catheter with the full 10ml of sterile normal
saline.
Warning: Failure to ensure patency of the catheter prior to
power injection studies may result in catheter failure.
4. Detach syringe.5. Attach the power injection device to the
PowerHohn* catheter per manufacturer’s recommendations.6. Complete
power injection study taking care not to exceed the flow rate
limits.
Warning: Exceeding the maximum flow rate of 5ml/sec may result
in catheter failure and/or catheter tip displacement.7. Disconnect
the power injection device.8. Flush the PowerHohn* catheter with
10ml of sterile normal saline, using a 10ml or larger syringe.9.
Replace the end cap(s) on the PowerHohn* catheter.
DescriptionPowerHohn* Central Venous Catheters are constructed
of specially formulated and processed polyurethane and are designed
forover-the-wire insertion into the central venous system.
PowerHohn* catheters have a kink-resistant, reverse-tapered design.
Thecatheters are radiopaque with female luer locking adapters and
StatLock* device compatible suture wings for fixation. Eachcatheter
is provided in a sterile package. Catheters are available with or
without VitaCuff* antimicrobial cuff.
PlacementThe catheter is placed into one of the central veins so
the tip lies in the superior vena cava above the right atrium.
Schematics:
Ne
w I
mp
ort
an
t In
form
ati
on
:
New Important Information:• Follow all contraindications,
warnings, cautions, precautions and instructions for all infusates,
including contrast media, as
specified by its manufacturer. • Use aseptic techniques whenever
the catheter lumen is opened or connected to other devices.
Povidone-iodine or chlorhexa-
dine gluconate are the suggested antiseptics to use with this
device and components. Acetone and tincture of iodine shouldnot be
used because they could adversely affect the performance of the
catheter and connectors. 10% acetone/70% isopropylalcohol
swabsticks used for dressing changes should not adversely affect
the catheter.
• Patients with thick muscular chest walls or extensive scar
tissue may require the use of a percutaneous introducer for
catheterinsertion.
• Catheters can be cut to length if a different length is
desired due to patient size and desired point of insertion
according to hos-pital protocol. Catheter depth markings are in
centimeters. Use caution when using scissors or any sharp-edged
instruments asthey could damage the catheter.
• Examine package carefully before opening to confirm its
integrity and that the expiration date has not passed. The catheter
issupplied in a double sterile package and is non-pyrogenic. Do not
use if package is damaged, opened or the expiration datehas passed.
Sterilized by ethylene oxide. Do not resterilize.
• Inspect kit for inclusion of all components. • When device
includes an antimicrobial cuff, do not expose the cuff to fluids
prior to insertion. Handle carefully to avoid cuff damage. • Fill
(prime) the device with sterile heparinized saline or normal saline
solution to help avoid air embolism. • When using an introducer
kit, verify that the catheter fits easily through the introducer
sheath.
• Avoid accidental device contact with sharp instruments and
mechanical damage to the catheter material. Use only smooth-edged
atraumatic clamps or forceps.
• Avoid perforating, tearing or fracturing the catheter when
using a guidewire. • Do not use the catheter if there is any
evidence of mechanical damage or leaking.• Avoid sharp or acute
angles during implantation which could compromise the patency of
the catheter lumen(s).• Sutures should not be tied around the
catheter itself. The suture wings will secure the catheter without
compromising catheter
patency. • When using percutaneous introducers:
- Carefully insert the introducer and catheter to avoid
inadvertent penetration to vital structures in the thorax.- To
avoid blood vessel damage, do not allow the percutaneous introducer
sheath to remain indwelling in the blood vessel
without the internal support of a catheter or dilator. -
Simultaneously advance the dilator with rotational motion to help
prevent damage.
• During insertion of catheter with antimicrobial cuff:-
Minimize the exposure of the cuff to pooled blood by sponging the
intended cuff placement site. - The entire collagen (tan) portion
of the cuff must be in the subcutaneous tissue at the catheter exit
site.
• Do not use the catheter if there is any evidence of mechanical
damage or leaking. Damage to the catheter may lead to rup-ture,
fragmentation and possible embolism and surgical removal.
• Accessories and components used in conjunction with this
device should incorporate luer lock connections.• If signs of
extravasation exist, discontinue injections. Begin appropriate
medical intervention immediately.• Prolonged infusion pressure
greater than 25 psi (172 kPa) may damage blood vessels and viscus
and is not recommended.
Do not use a syringe smaller than 10 ml!
Possible ComplicationsThe potential exists for serious
complications including the following.
• Air Embolism• Allergic Reaction to Silver or Collagen
(Catheters with VitaCuff* AntimicrobialCuff Only)
• Bleeding• Brachial Plexus Injury• Cardiac Arrhythmia• Cardiac
Tamponade• Catheter or Cuff Erosion Through
the Skin• Catheter Embolism• Catheter Occlusion• Catheter
Occlusion, Damage or
Breakage due to Compression betweenthe Clavicle and First Rib
(Pinch-off)
• Catheter-related Sepsis• Endocarditis• Exit Site Infection•
Exit Site Necrosis• Extravasation• Fibrin Sheath Formation•
Hematoma• Hemothroax• Hydrothorax• Intolerance Reaction to
Implanted
Device• Laceration of Vessels or Viscus• Myocardial Erosion •
Perforation of Vessels or Viscus• Phlebitis
• Pneumothorax• Spontaneous Catheter Tip Malposition
or Retraction• Thromboembolism• Thoracic Duct Injury• Venous
Thrombosis• Ventricular Thrombosis• Vessel Erosion• Risks Normally
Associated with Local
or General Anesthesia, Surgery, andPost-Operative Recovery
III. After placement:
II. During placement:
I. Prior to placement:
Hubs Thumb Clamps
ID Tags
ID Tags
Molded Junction Reverse Taper TubingVitaCuff * Antimicrobial
Cuff
1
First RibSubclavian Vein
Clavicle
Vertebra
Internal Jugular Vein
Superior Vena Cava
SternumPinch-off Area
Infraclavicular Fossa
Axillary Vein
-
Bard Access Systems
Central Venous CathetersInstructions For Use
PowerHohn* Central Venous Catheter Placement Procedure1. The
procedure is performed using sterile surgical technique including
the use of gloves,
masks, gowns, and sterile drapes and equipment throughout all
steps listed below.2. Place the patient in the Trendelenburg
position. Prep the insertion site using standard
surgical technique.3. The subclavian veins and the internal and
external jugular veins are the most common
vessels used for catheter insertion. The femoral vein may also
be used.4. Administer local anesthesia at the venous entry site,
the underlying subcutaneous tissue,
and where the wing will be sutured or the StatLock* device
secured.5. Catheters can be cut to length if a different length is
desired due to patient size and
desired point of insertion. 6. Enter the vein chosen for
insertion of the catheter using the introducer needle and
syringe or sheath over the needle. (Refer to figure 2)Caution:
When inserting the catheter via a subclavian approach, maintain a
horizontaltrajectory when introducing the needle beneath the
clavicle. Vertical needle passage mayincrease the risk of
pneumothorax. Refer to “Warnings” section concerning Catheter
Pinch-off.
7. Aspirate gently as the needle is introduced. Warning: If the
artery is entered, withdrawthe needle and apply manual pressure for
several minutes. If the pleural space is entered,withdraw needle
and observe patient for signs of pneumothorax. (Refer to figure
3)
8. When the vein has been entered, remove the syringe leaving
the needle in place. If usingthe sheath over the needle, insert the
assembly and withdraw the needle and syringeleaving the sheath
indwelling. Place a finger over the needle or sheath hub to
minimizeblood loss and risk of air aspiration. The risk of air
aspiration is reduced by performingthis part of the procedure with
the patient performing the Valsalva maneuver. (Refer tofigure
4)
9. Insert tapered end of the tip straightener into the needle
(or sheath). Advance theguidewire to the superior vena cava. (Refer
to figure 5)Caution: To help avoid possible severing of the
guidewire, do not withdraw the guidewireback against the needle
bevel.
10. Withdraw and remove needle (or sheath) while holding the
guidewire in place. Maintainslight pressure on the puncture site
after the needle is withdrawn. (Refer to figure 6)
10a. For catheters with VitaCuff* antimicrobial cuff: use the
supplied scalpel, if needed, to makea skin nick at the insertion
site to accommodate the antimicrobial cuff. (Refer to figure 7)
11. A skin nick may be made adjacent to the insertion site to
facilitate tip insertion.12. Advance the dilator over the exposed
wire using a rotational motion to develop a tunnel
for the catheter. Gentle counter traction on the skin may
facilitate smooth passage of thedilator. Several passes with the
dilator are recommended. (Refer to figure 8)
13. Withdraw the dilator.Note: Patients with thick muscular
chest walls or extensive scar tissue may require theuse of a
percutaneous introducer for catheter insertion.
14. For the dual lumen catheter, clamp and attach an end cap to
the one luer adapter toavoid possible air embolus.
15. Thread the catheter over the guidewire and advance the
catheter to the insertion site.The guidewire must extend out from
the luer adapter.
16. Advance the catheter and wire assembly together as a unit
with a rotational motion. Thisis best accomplished by gently
squeezing the catheter against the wire and rotating