Embed Size (px)
Citation preview
Cauda Equina Pseudoclaudication Syndrome
Takehisa IWAI, M. D.
ABSTRACT: Intermit tent claudication is known as a specific symptom in patients with chronic occlusive arterial lesions. Clinically it is important that neurogenic intermittent pseudo-claudication should be differentiated from true intermittent claudication. Nevertheless confusion still exists in differen- tial diagnosis between these two entities. This paper deals with general review of intermittent pseudo-claudication and a particular emphasis is placed on the different concepts of the pathophysiology and the differential diagnosis from the standpoint of vascular surgery. Recently one case of the neurogenic intermittent pseudo-claudication was encountered and presented in this paper.
KEY W O R D S : cauda equina, intermittent claudication, pseudo-claudi- cation, small lumbar canal, aorto-iliac occlusive disease, protrusion of the disk.
INTRODUCTION
Intermittent claudication is one of the most specific symptoms in clinical medicine 22. Usually it is easily recognized in a patient with chronic arterial occlusive disease and is seldom confused with other conditions such as musculoskeletal disorder, chronic venous insufficiency or systemic disease such as anemia. Nevertheless a smaller group of chronic aorto-i]iac disease (about 15 per cent of terminal aorta to i]io-femoral-popliteal lesion 27) is often mistaken for the syndrome referred to as intermittent claudication of the cauda equina a or neurogenic intermittent claudication 16, or pseudo-claudication syndrome 2a because of the presence of the buttocks and thighs claudication with a cycle of exercise- pain-relief 18 and high incidence in the similar age group. The cause of this simulating intermittent claudication may result from the compression of the cauda equina region most often by the protruding intervertcbral disk closely associated with a0, a6, a7 or with- out a, 16 a narrow spinal canal. The narrowing of spinal canal is caused by degenerative changes such as spondylosis 8, 15, congenital anomaly 5, 28, rarely spondylolisthcsis 26, arachnoiditis 18, iatrogenic s or above combinations. Even though the pathophysiologic mechanism remains obscure, ischemic process may play a great role in this syndrome, either primarily or secondarily aT. The most important to be differentiated diagnosis is the aorto-i]iac occlusive disease, especially Leriche syndrome 25 in which patients may not always complain of typical pain and may have palpable collateral pulses distally. In addition to accurate history and usual physical examination, it is important to search reflex changes by exertion or absence of loud bruits over the groin during or after leg exercise. Sensory predominant claudication and shortening claudication distance following continuous wa]king arc valuable for diagnosis or suspicion of this syndrome. However,
From the 1st Department of Surgery (Professor: Tadashige Murakami) Tokyo Medical and Dental University 1-5-45, Yushima, Bunkyo-ku, Tokyo, Japan 113.
JAPANESE JOURNAL OF SUROERY, VOL. 5, No. 3, pp 164-174, 1975
Volume 5 Pseudoclaudication 165 Number 3
sometimes it is extremely difficult to make a diagnosis, especially when there is a concomi- tant peripheral vascular disease a6 or history of the back t rauma is. Aortography and myelography are the final accurate diagnostic measures. Surgical decompression is the best management with a good result. A term "Cauda Equina Pseudoclaudication Syndrome" seems to be preferable, because intermittent claudication-like symptom may be encoun- tered in several other conditions besides a cauda equina origin. Precise and experienced physical examination will reveal definite differences between true and pseudoclaudication,
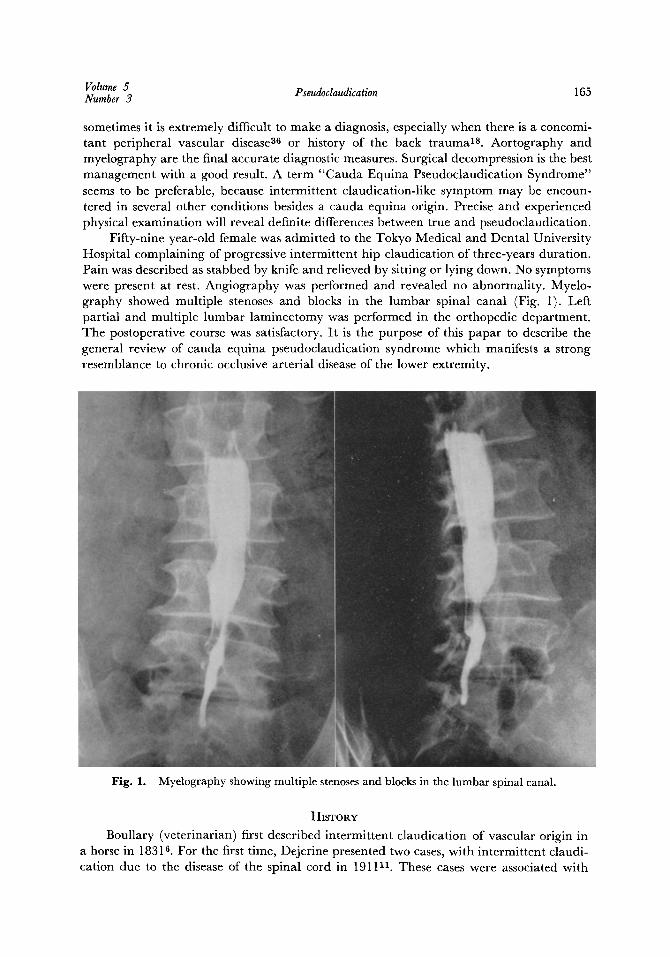
Fifty-nine year-old female was admitted to the Tokyo Medical and Dental University Hospital complaining of progressive intermittent hip claudication of three-years duration. Pain was described as stabbed by knife and relieved by sitting or lying down. No symptoms were present at rest. Angiography was performed and revealed no abnormality. Myelo- graphy showed multiple stenoses and blocks in the lumbar spinal canal (Fig. 1). Left partial and multiple lumbar laminectomy was performed in the orthopedic department. The postoperative course was satisfactory. I t is the purpose of this papar to describe the general review of cauda equina pseudoclaudication syndrome which manifests a strong resemblance to chronic occlusive arterial disease of the lower extremity.
Fig. 1. Myelography showing multiple stenoses and blocks in the lumbar spinal canal.
HISTORY
Boullary (veterinarian) first described intermittent claudication of vascular origin in a horse in 1831B. For the first time, Dejerine presented two cases, with intermittent claudi- cation due to the disease of the spinal cord in 191111 . These cases were associated with
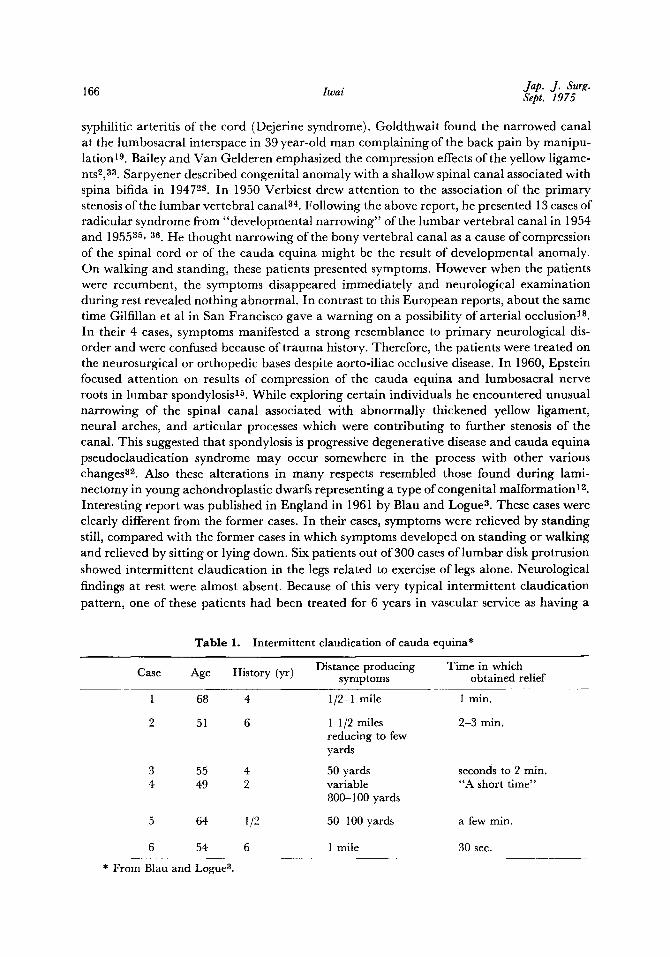
166 Iwai Jap. J. Surg. Sept. 1975
syphilitic arteritis of the cord (Dejerine syndrome). Goldthwait found the narrowed canal at the lumbosacral interspace in 39 year-old man complaining of the back pain by manipu- lation 19. Bailey and Van Gelderen emphasized the compression effects of the yellow ligame- nts2, 33. Sarpyener described congenital anomaly with a shallow spinal canal associated with spina bifida in 1947 zs. In 1950 Verbiest drew attention to the association of the pr imary stenosis of the lumbar vertebral canal 84. Following the above report, he presented 13 cases of radicular syndrome from "developmental narrowing" of the lumbar vertebral canal in 1954 and 195535, 36. He thought narrowing of the bony vertebral canal as a cause of compression of the spinal cord or of the cauda equina might be the result of developmental anomaly. On walking and standing, these patients presented symptoms. However when the patients were recumbent, the symptoms disappeared immediately and neurological examination during rest revealed nothing abnormal. In contrast to this European reports, about the same time Gilfillan et al in San Francisco gave a warning on a possibility of arterial occlusion 18. In their 4 cases, symptoms manifested a strong resemblance to pr imary neurological dis- order and were confused because of t rauma history. Therefore, the patients were treated on the neurosurgical or orthopedic bases despite aorto-iliac occlusive disease. In 1960, Epstein focused attention on results of compression of the cauda equina and lumbosacral nerve roots in lumbar spondylosis 15. While exploring certain individuals he encountered unusual narrowing of the spinal canal associated with abnormally thickened yellow ligament, neural arches, and articular processes which were contributing to further stenosis of the canal. This suggested that spondylosis is progressive degenerative disease and cauda equina pseudoclaudication syndrome may occur somewhere in the process with other various changes 32. Also these alterations in many respects resembled those found during lami- nectomy in young achondroplastic dwarfs representing a type of congenital malformation 12. Interesting report was published in England in 1961 by Blau and Logue 3. These cases were clearly different from the former cases. In their cases, symptoms were relieved by standing still, compared with the former cases in which symptoms develope:l on standing or walking and relieved by sitting or lying down. Six patients out of 300 cases of lumbar disk protrusion showed intermittent claudication in the legs related to exercise of legs alone. Neurological findings at rest were almost absent. Because of this very typical intermittent claudication pattern, one of these patients had been treated for 6 years in vascular service as having a
Table 1. Intermittent claudication of cauda equina*
Distance producing Time in which Case Age History (yr) symptoms obtained relief
1 68 4 1/2-1 mile 1 min.
2 51 6 1 1/2 miles 2-3 min. reducing to few yards
3 55 4 50 yards seconds to 2 min. 4 49 2 variable "A short time"
800-100 yards
5 64 1/2 50-100 yards a few min.
6 54 6 1 mile 30 see.
* From Blau and Logue 3.
Volume 5 Number 3 Pseudodaudication 167
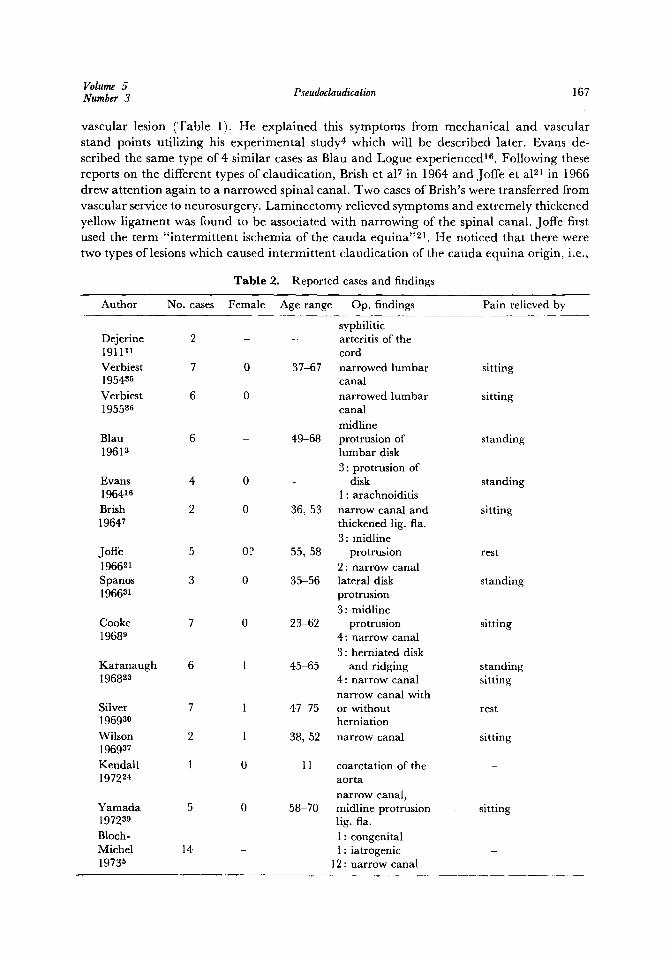
vascular lesion (Table 1). He explained this symptoms from mechanica l and vascular stand points uti l izing his exper imenta l study 4 which will be described later. Evans de- scribed the same type of 4 similar cases as Blau and Logue experienced 16. Following these reports on the different types of claudicat ion, Brish et a17 in 1964 and Joffe et a121 in 1966 drew at tent ion again to a nar rowed spinal canal. Two cases of Brish's were transferred from vascular service to neurosurgery. Laminec tomy relieved symptoms and extremely thickened yellow l igament was found to be associated with nar rowing of the spinal canal. Joffe first used the term " in te rmi t t en t ischemia of the cauda equina ''21. He noticed that there were two types of lesions which caused in te rmi t ten t c laudicat ion of the cauda equ ina origin, i.e.,
Table 2. Reported cases and findings
Author No. cases Female Age range Op. findings Pain relieved by
syphilitic Dejerine 2 - - arteritis of the - 191111 cord Verbiest 7 0 37-67 narrowed lumbar sitting 195435 canal Verbiest 6 0 narrowed lumbar sitting 1955 z6 canal
midline Blau 6 - 49-68 protrusion of standing 1961 z lumbar disk
3: protrusion of Evans 4 0 -- disk standing 196416 1 : arachnoiditis Brish 2 0 36, 53 narrow canal and sitting 19647 thickened lig. fla.
3 : midline Joffe 5 0? 55, 58 protrusion rest 196621 2 : narrow canal Spanos 3 0 35 56 lateral disk standing 196631 protrusion
3 : midline Cooke 7 0 23-62 protrusion sitting 19689 4: narrow canal
3: herniated disk Karanaugh 6 1 45-65 and ridging standing 196838 4: narrow canal sitting
narrow canal with Silver 7 1 47-75 or without rest 196930 herniation Wilson 2 1 38, 52 narrow canal sitting 1969a7
Kendall 1 0 11 coarctation of the - 197224 aorta
narrow canal, 0 58-70 midline protrusion sitting
lig. fla. 1 : congenital 1 : iatrogenic
12: narrow canal
Yamada 5 1972a9 Bloch- Michel 14 19735
168 Iwai Jap. J. Surg. Sept. 1975
1) central disk protrusion in the lumbar region, 2) stenosis of the lumbar canal or narrowing of the spinal canal. In the same year, Spanos and Andrew presented three cases with a different pathological lesion, which manifested progressive intermittent claudication in only one leg 31. These are assumed to be ruptured lumbar disk. Cooke and Lehmann 9 described 7 cases and classified them into two groups as Joffe did. In 1968 a new term "pseudoclaudication" syndrome was postulated by Karanaugh et al 2a of Mayo clinic group to avoid to be confused from separately named syndrome. Silver reported 7 cases of nar- rowed spinal canala0. Wilson reviewed all cases historically and pointed out the fact that two types of intermittent claudication of the cauda equina might exist ~7. The postural variety producing symptoms of compression from hyperextension of the lumbar spine and the ischemic variety resulting from impaired blood flow through constricted radicular arteries which based on the investigation of Blau and Logue, and Evans. More recently there are several reports about this syndrome and findings. Kendall presented 11 year-old boy developed intermittent claudication following an operation on the coarctation of the aorta 24. Yamada reported 5 cases from Japan ag. Block-Michel presented 14 cases with narrowed lumbar canal including one congenital stenosis and one iatrogenic case 5. Since 1911, at least 95 cases of cauda equina or neurogenic pseudoclaudication syndrome with variety of findings were published in the literature (Table 2).
ETIOLOGY
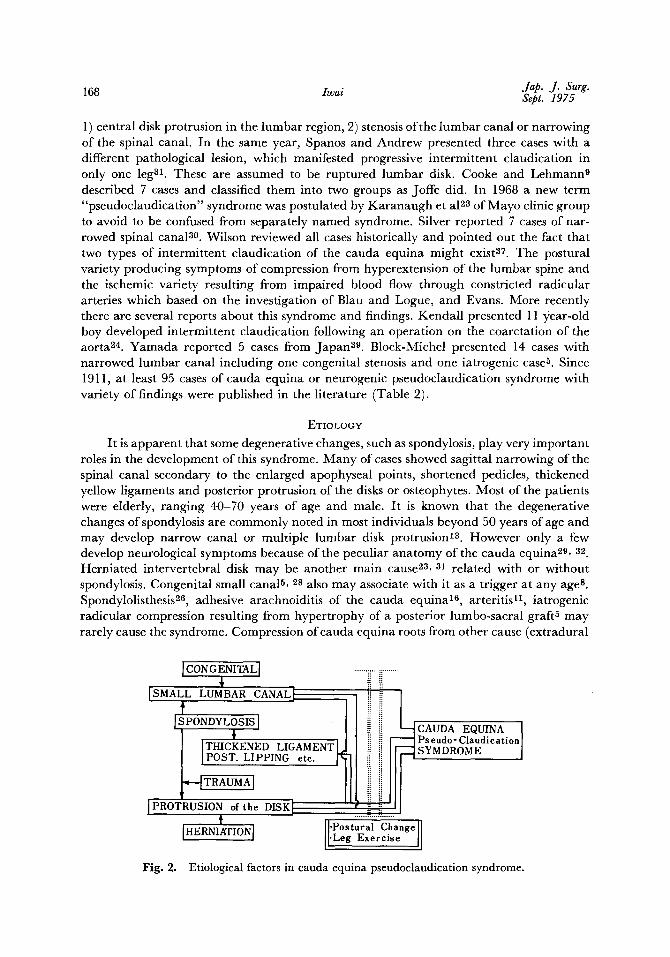
It is apparent that some degenerative changes, such as spondylosis, play very important roles in the development of this syndrome. Many of cases showed sagittal narrowing of the spinal canal secondary to the enlarged apophyseal points, shortened pedicles, thickened yellow ligaments and posterior protrusion of the disks or osteophytes. Most of the patients were elderly, ranging 40-70 years of age and male. I t is known that the degenerative changes ofspondylosis are commonly noted in most individuals beyond 50 years of age and may develop narrow canal or multiple lumbar disk protrusion 1~. However only a few develop neurological symptoms because of the peculiar anatomy of the cauda equina 29, 32 Herniated intervertebral disk may be another main cause 28, al related with or without spondylosis. Congenital small canalS, 28 also may associate with it as a trigger at any age s. Spondylolisthesis z6, adhesive arachnoiditis of the cauda equina 16, arteritis 11, iatrogenic radicular compression resulting from hypertrophy of a posterior lumbo-sacral graft 5 may rarely cause the syndrome. Compression of cauda equina roots from other cause (extradural
] CON G ENITAL] �89
[SMALL LUMBAR CANAL I
t ISPONDYLOSIS ]
THICKENED LIGAMENT L ]POST. LIPPING etc. Ix
..--qTRAUMAI IPROTRUSION of the DISK I
t I"ERNIATIONJ
....... ii ..............
H ---~ CAUDA EQUINA I
i ~ SYMDROME ]
...... .~.-;....?. ...... �9 Postural Change 1
JI-Le, Exorcise II
Fig. 2. Etiological factors in cauda equina pseudoclaudication syndrome.

Volume 5 Number 3 Pseudoclaudication 169
or intradural neoplasms) is a rare cause 20. Scoliosis, achondroplasia and, trauma may be related to the etiology in young age group patients 12, 32 (Fig. 9).
PATHOPHYSIOLOGY
Blau and Logue first described pathophysiological hypothesis. In their cases symptoms were relieved by standing still 3. Their patients differed from Verbiest's or Van Gelderen's in which the cause might be explained by the mechanical compression of the cauda equina nerve roots. They tried to account for the static mechanism to vascular and mechanical factors. Through an experimental study in the lumbar spinal cord of mice, they pre- sented a hypothesis that the vessels of the spinal nerve roots were particularly prominent and often widely dilated in exercised animal 4. Interference with venous return alone seemed unimportant because of the generous venous anastomoses in the spinal canal and the reversible venous flow around the nerve roots 17. Therefore when a person walks, there is a similar increase of blood flow to the cauda equina roots with concomitant increase in size and possibly a number of afferent and efferent vessels. I f firm constriction of nerve roots by the disk protrusion occurs and the increased dilation and increased supply in response to activity of the roots are disturbed by the compression, the symptoms of ischemic neuritis results. This possibility of intermittent nerve anoxia was further investigated by Evans 16. He created the compression-free or mechanical factor-free situation on the lumbar disk by bed rest. The results showed that claudication time correlated directly with oxygen tension of respired gas. Nevertheless mechanical or postural factors were not abandoned. Spanos believed with their lateral lumbar disk protrusion cases that when patients walked with weight bearing on the disk, because of its consistency, the disk gradually herniated further into the spinal canal. A critical point was reached when the overlying nerve root became stretched, then congestive edema or interference with the normal blood circulation would occur 31. In 1968 Cooke observed 7 patients and emphasized two factors of intermittent root dysfunction, namely hypoxia and postures 9. Karanaugh et al felt that cerebrospinal fluid dynamics might have an important bearing on the production of symptoms and postulated a hypothesis of compression of veins or venules brought about by increased pressure of cerebrospinal fluid 23. According to Davson 1~ veins have highly distensible wall which collapses completely when pressure of the fluid outside is only slightly greater than venous pressure. For this reason they thought even in a static situation such as prolonged standing or lying in certain positions, an increase in the pressure of the confined cerebrospinal fluid below the site of the block (in most cases, a very high grade obstruction occurrs in the subarachnoid space as a result of the impinging disk or bony ridge) could occur. Then an increase in the pressure of the cerebrospinal fluid could, in turn, collapse strategic venous return with resultant stagnant anoxia to certain nerve trunks. Silver et al proposed another possibility related to the nerve root pressure induced by lumbar disk protrusion affecting the autonomic nervous system pathways which would cause muscular ischemia secondary to vasoconstriction 3~ Wilson classified cauda equina pseudoclaudication syndrome patho- physiologically into two groups or varieties based on primary and secondary ischemia of the roots 37. Larger group in which symptoms appear during standing or continuous hyper- extension of the lumbar spine was termed as postural cauda equina claudication. Inter- estingly in this group symptoms may not be precipitated by activities such as riding a bicycle, playing tennis or swimming 3v. Smaller group, in which symptoms related to walking rather than to posture and believed to be caused by arterial insufficiency of roots, was termed "ischemic". This is based on an evidence that conducting peripheral neural tissue increases oxygen demand and sensory deficit at any level of the nervous system may be
170 Iwai Jap. J. Surg. Sept. 1975
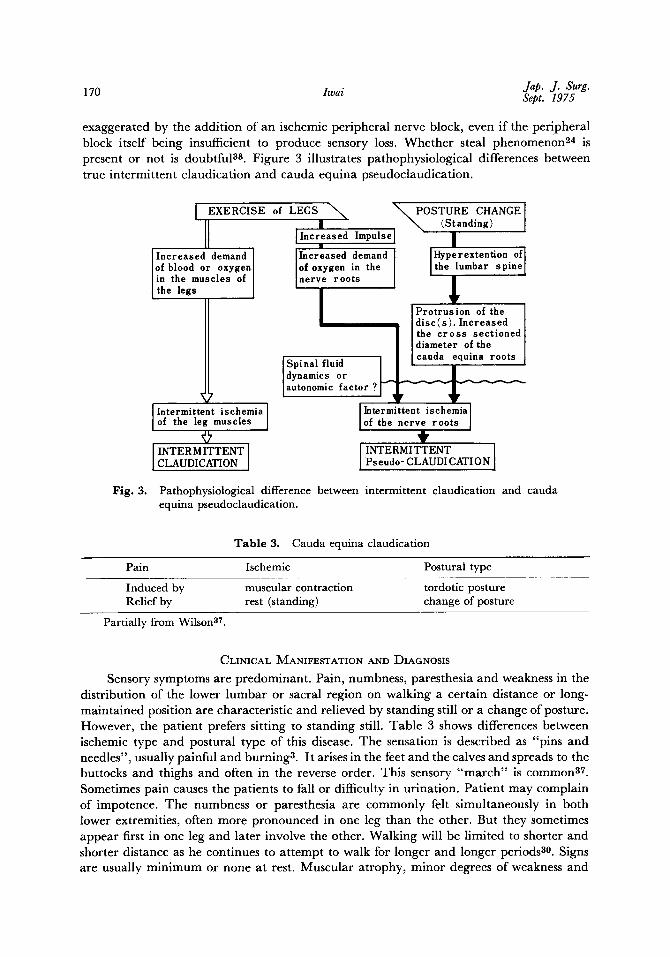
exaggerated by the addition of an ischemic peripheral nerve block, even if the peripheral block itself being insufficient to produce sensory loss. Whether steal phenomenon 24 is present or not is doubtful 3s. Figure 3 illustrates pathophysiological differences between true intermittent claudication and cauda equina pseudoclaudication.
Intermittent ischemia I of the leg muscles [ !
INTER M ITTENT CLAUDICATION [
[ EXERCISE of LEGS x", N ~ POSTURE CHANGE[ [I , ~ (Standing) [
[ Incr:ased Impulse[ I
Increased demand [ Increased demand [ [Hyperextention of of blood or oxygen[ of oxygen in the [ [the lumbar spine in the muscles of nerve roots / the legs
I ~ P r o t r u s i o n of the disc(s). Increased the cross sectioned diameter of the
Spinal fluid cauda equina roots dynamics or autonomic factor ?
Intermittent ischemia of the nerve roots
# INTERMITTENT Pseudo- CLAUDI CATION I
Fig. 3. Pathophysiological difference between intermittent claudication and cauda equina pseudoclaudication.
Table 3. Cauda equina claudication
Pain Ischemic Postural type
Induced by muscular contraction tordotic posture Relief by rest (standing) change of posture
Partially from Wilson zT.
CLINICAL MANIFESTATION AND DIAGNOSIS
Sensory symptoms are predominant. Pain, numbness, paresthesia and weakness in the distribution of the lower lumbar or sacral region on walking a certain distance or long- maintained position are characteristic and relieved by standing still or a change of posture. However, the patient prefers sitting to standing still. Table 3 shows differences between ischemic type and postural type of this disease. The sensation is described as "pins and needles", usually painful and burning 3. It arises in the feet and the calves and spreads to the buttocks and thighs and often in the reverse order. This sensory "march" is common 37. Sometimes pain causes the patients to fall or difficulty in urination. Patient may complain of impotence. The numbness or paresthesia are commonly felt simultaneously in both lower extremities, often more pronounced in one leg than the other. But they sometimes appear first in one leg and later involve the other. Walking will be limited to shorter and shorter distance as he continues to attempt to walk for longer and longer periods 30. Signs are usually minimum or none at rest. Muscular atrophy, minor degrees of weakness and
Volume 5 Number 3 Pseudoclaudication 171
reduced reflex (mostly Achilles tendon reflex) may occur more commonly. Straight leg raising test is normal or nearly so. Repetition of the neurological examination after maxi- mum walking may be more informative, because motor and sensory disturbances, absent at rest, may then become apparent a, 16 Reduction or disappearance of the deep tendon reflexes after exercise is very common in many reported cases.
Lumbar puncture shows normal or slight elevation of protein and jugular compression maneuvour may be abnormal. In all patients, myelography reveals complete or almost complete block in lumbar region. Lateral upright films are helpful. Small spinal canal may be seen. Final diagnosis is made only by myelography.
DIFFERENTIAL DIAGNOSIS
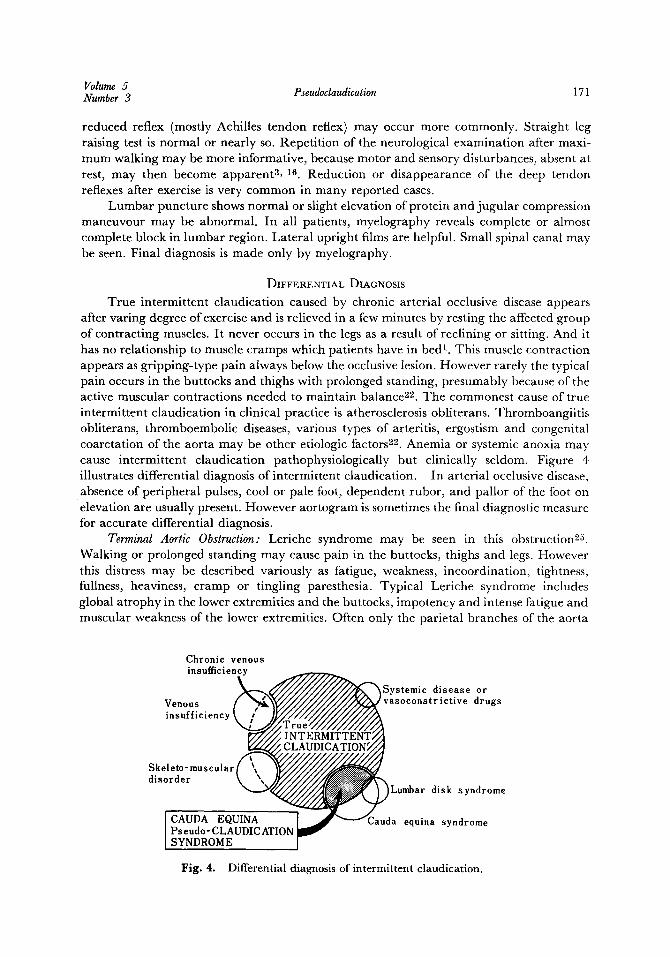
True intermittent claudication caused by chronic arterial occlusive disease appears after varing degree of exercise and is relieved in a few minutes by resting the affected group of contracting muscles. It never occurs in the legs as a result of reclining or sitting. And it has no relationship to muscle cramps which patients have in bed I. This muscle contraction appears as gripping-type pain always below the occlusive lesion. However rarely the typical pain occurs in the buttocks and thighs with prolonged standing, presumably because of the active muscular contractions needed to maintain balance 22. The commonest cause of truc intermittent claudication in clinical practice is atherosclerosis obliterans. Thromboangiitis obliterans, thromboembolic diseases, various types of arteritis, ergostism and congenital coarctation of the aorta may be other etiologic factors 22. Anemia or systemic anoxia may cause intermittent claudication pathophysiologically but clinically seldom. Figure 4 illustrates differential diagnosis of intermittent claudication. In arterial occlusive disease, absence of peripheral pulses, cool or pale foot, dependent rubor, and pallor of the foot on elevation are usually present. However aortogram is sometimes the final diagnostic measure for accurate differential diagnosis.
Terminal Aortic Obstruction: Leriche syndrome may be seen in this obstruction 25. Walking or prolonged standing may cause pain in the buttocks, thighs and legs. However this distress may be described variously as fatigue, weakness, incoordination, tightness, fullness, heaviness, cramp or tingling paresthesia. Typical Leriche syndrome includes global atrophy in the lower extremities and the buttocks, impotency and intense fatigue and muscular weakness of the lower extremities. Often only the parietal branches of the aorta
Chronic venous insufficiency
~Systemic disease or Venous / vasoconstrietive drugs insufficiency
Skeleto- muscular disorder
Lumbar disk syndrome
l CAUDA EQUINA Cauda equina syndrome ] Pseudo- CLAUDICATION / SYNDROME
Fig. 4. Differential diagnosis of intermittent claudication.

172 Iwai Jap. J. Surg. Sept. 1975
are obstructed and it m a y cause lumbar and hip pain that may be bilateral or unilateral and related to exercise is.
Total Iliac Obstruction: The patients usually have pain commenc ing in the lowbuttocks and extending into the thigh and then to the calf on the affected side. Collateral pulses may be present distally.
Partial Iliac Obstruction: A syndrome described by Gilfillan, Steinfeld and Leeds in 1953 will be present. Namely it included a systolic bruit over the involved artery and claudication pain starting in the calf and proceeding to the thigh and buttock secondarily. Patient with partial iliae occlusion also must be noted to lose his pedal pulses after and during exercise.
Chronic Venous Insu~ciency: Pigmentat ion or stasis ulcer in the lower leg and pain relieved by leg elevation are helpful signs and symptoms.
Musculo-Skeletal Disorders: T he presence of pressure pain and very slow recovery from pain are significant. Numbness or paresthesia is not present. Also plain X-ray is useful.
Table 4. Differential diagnosis between aorto-iliac occlusive disease and cauda equina pseudoclaudication syndrome
Finding Aorto-iliac occlusive disease Cauda equina pseudoclaudication
PAIN: location character
"march" relieved by induced by
Claudication distance Motor deficit Sensory deficit Deep tendon reflex Lasegue sign Lumbar puncture
Weakness, Muscle atrophy Pallor of foot on elevation Peripheral pulses Arterial bruit Impotence History of trauma Plain X-ray
Myelography Aortography Treatment
buttocks, hips, thighs & legs cramping, gripping, squeezing, dull or paresthesia absent standing still or may not walking or maybe prolonged standing fixed
rare maybe present normal, rarely reduced
normal normal
~equent
present
diminished or absent after exercise may be present may be present may be present may show vascular calcification normal diagnostic TEA or bypass graft in selected cases
buttocks, thighs & legs burning, paresthestic. maybe dull or cramping present standing or change of posture walking or standing
shorter and shorter
mild, variable mild, variable often reduced or absent
frequently normal may be difficult, demonstrate block, CSF protein elevated may be present
none
normal
none may be present often present abnormal lumbar spine (osteophytes, short pedicles) diagnostic normal laminectomy in most of cases
Modified by the author from Wilsona7 and Gilfillan is.
Volume 5 Pseudoclaudication 173 Number 3
Table 4 shows an outl ine of the m a i n diagnostic difference between aorto-iliac disease and cauda equina pseudoclaudicat ion syndrome.
TREATMENT AND PROGNOSIS
Whether it is ischemic or postural type of cauda equina pseudoclaudicat ion, wide laminec tomy and part ial facetectomy is the choice of t rea tment 37. Good result is expected in most cases. Conservative therapy is effective in selected cases 23.
WARNING
The cauda equina pseudoclaudicat ion syndrome is insidious like other degenerative diseases such as atherosclerosis. The existence or significance of a predisposing spinal abnormal i ty may not be recognized by general surgeons, neurosurgeons, orthopedic surgeons or anesthesiologists. Acute compression of cauda equina by artificially induced extention of the back while the pa t ient is under anesthesia may result in cauda equina palsy 14. A coexistence of chronic arterial occlusive disease and this syndrome may become more frequent in future. Accurate diagnostic measures and general unders tand ing of this syndrome will be necessary among neurosurgeons and vascular surgeons. Aortic reconstruc- tion will be required with more a t tent ion to the l u m b a r arteries in the selected cases. Final ly it would be emphasized that these problems must be approached by good combined efforts of the neurosurgeons, vascular surgeons, orthopedic surgeons and anesthesiologist.
ACKNOWLEDGEMENT
Thanks are due to Dr. E.J. Wylie for suggesting me to write this review and Dr. I. Yamaura for allowing me to study his patients. The assistance of Miss Haruko Ohno and Dr. R. Ha tano is gratefully acknowledged.
(Received for publication on June 12, 1975)
References
1. Allen, E. V., Barker, N. W., and Hines, E. A.: Peripheral vascular disease. Philadelphia, W. B. Saunders, 4th edition, 1972.
2. Bailey, P. and Csamajor, L.: Osteoarthritis of the spine as a cause of compression of the spinal cord and its roots. J. Nerv. ment. Dis. 38: 588-609, 1911.
3. Blau, J. N. and Logue, V. : Intermittent claudi- cation of the cauda equina--an unusual syndrome resulting from central protrusion of a lumbar intervertebral disc. Lancet 1: 1081 1086, 1961.
4. Blau, J. N. and Rushworth, G.: Observations on the blood vessels of the spinal cord and their responses to motor activity. Brain 81: 354-363, 1958.
5. Bloch-Michel, H., Cauchoix, J., Benoist, M. and Chassaing, P.: The radicular pains of the lower limbs of the intermittent claudica- tion type. Their connection with the narrow- ness or the diameter of the lumbar spinal canal. Revue. neurol. 129: 211-219, 1973.
6. Boullay, M. : Oblitdration des art~res fdmorales
(Mddicine vdt6rinaire). Arch. Grin. de M6d. 27: 425, 1831.
7. Brish, A., Lerner, M. A. and Braham, J.: Intermittent claudication from compression of cauda equina by a narrowed spinal canal. J. Neurosurg. 21." 207-211, 1964.
8. Clark, K.: Significance of the small lumbar spinal canal: Cauda equina compression syndromes due to spondylosis. Part 2 : Clini- cal and surgical significance. J. Neurosurg. 31 : 495~-98, 1969.
9. Cooke, T. D. V. and Lehman, P. O.: Inter- mittent claudication of neurogenic origin. Canadian J. Surg. 11: 151-159, 1968.
10. Davson, H.: Physiology of the cerebrospinal fluid. Boston, Little, Brown & Co., pp 342- 347, 1967.
11. Dejerine: La claudication intermittente de la moelle dpini~re. Presse Mddicale 19: 981- 984, 1911.
12. Duvoisin, R. C. and Yahr, M. D. : Compressive spinal cord and root syndromes in achondro-
174 Iwai Jap. J. Surg. Sept. 1975
plastic dwarfs. Neurology, Minneap. 12: 202-207, 1962.
13. Ehni, G.: Significance of the small lumbar spinal canal: Cauda equina compression syndromes due to spondylosis. Part 1: In- troduction. J. Neurosurg. 31 : 490-494, 1969.
14. Ehni, G.: Significance of the small lumbar spinal canal: Cauda equina compression syndromes due to spondylosis. Part 4: Acute compression artificially induced during oper- ation. J. Neurosurg. 31: 507-517, 1969.
15. Epstein, J. A.: Diagnosis and treatment of painful neurological disorders caused by spondylosis of the lumbar spine. J. Neurosurg 7:991 1001, 1960.
16. Evans,J. G. : Neurogenic intermittent claudica- tion. Brit. Med. J. 2: 985-987, 1964.
17. Gillilan, L. A. : The arterial blood supply of the human spinal cord. J. comp. Neurol. 110: 75-100, 1958.
18. Gilfillan, R. S., Jones, O. W. Jr., Roland, S. I. and Wylie, E. J . : Arterial occlusions simulating neurological disorders of the lower limbs. JAMA 154:1149-1152, 1954.
19. Goldthwait, J. E.: The lumbosacral articula- tion. An explanation of many cases of "Lum- bago", "Sciatica", and paraplegia. Bost. Med. Surg. J. 164: 365-372, 1911.
20. Jennett, W. B. : A study of 25 cases of compres- sion of the cauda equina by prolapsed in- tervertebral discs. J. Neurol. Neurosurg. Psychiat., 19:109 116, 1965.
21. Joffe, R., Appleby, A. and Arjona, V. : "Inter- mittent ischaemia" of the cauda equina due to stenosis of the lumbar canal. J. Neurol. Neurosurg. Psychiat. 29: 315-318, 1966.
22. Juergens, J. L.: Intermittent elaudication. Med. clin. N. Amer. 42-2: 981-989, 1958.
23. Karanaugh, G. J., Svien, H. J., Holman, C. B., and Johnson, R. M. : "Pseudoclaudica- tion" syndrome produced by compression of the cauda equina. JAMA 206: 2477-2481, 1968.
24. Kendall, B. E. and Andrew, J . : Neurogenic intermittent claudication associated with aortic steal from the anterior spinal artery complicating coarctation of the aorta. J. Neurosurg. 37:89 94, 1972.
25. Leriche, R.: Des Obliterations art6rielles hautes (Oblit6ration de la terminaison de l'aorte), comme cause des insuffisances circulatoires des membres int6rieurs. Bull. et
m6m. Soc. d. Chir. 49: 1404, 1925. 26. Moiel, R. and Ehnl, G. : Cauda equina com-
pression due to spondylolisthesis with intact neural arch. J. Neurosurg. 28" 262-265, 1968.
27. Richards, R. L.: Peripheral arterial disease. Edinburgh & London, E. and S. Livingstone, 1970.
28. Sarpyener, M. A.: Spina bifida aperta and congenital stricture of the spinal canal. J. Bone Joint Surg. 29: 817-821, 1947.
29. Shephard, R. H. : Diagnosis and prognosis of cauda equina syndrome produced by pro- trusion of lumbar disk. Brit. Med. J. No. 5164: 1434-1439, 1959.
30. Silver, R. A., Schuele, H. L., Stack, J. K., Conn, J. Jr . and Bergan, J. J. : Intermittent claudication of neuro-spinal origin. Arch. Surg. 98: 523-529, 1969.
31. Spanos, N. C., and Andrew, J . : Intermittent claudicatlon and lateral lumbar disc pro- trusions. J. Neurol. Neurosurg. Psychiat., 29: 273-277, 1966.
32. Teng, P. and Papatheodorou, C.: Lumbar Spondylosis with compression of cauda equina. Arch. Neurology. 8: 121-129, 1963.
33. Van Gelderen, Chr.: Ein Orthotisches (Lor- dotisches) Kaudasyndrom. Aeta Psychiatrica et Neurologica. 23: 57, 1948.
34. Verbiest, H.: Primary stenosis of lumbar vertebral canal in adults: new clinical pic- ture. Nederl. T. Geneesk. 94: 2414-2425, 1950.
35. Verbiest, H.: A radicular syndrome from developmental narrowing of the lumbar vertebral canal. J . Bone Joint Surg. 36B: 230-237, 1954.
36. Verbiest, H. : Further experience on the patho- logical influence of a developmental nar- rowing of the bony lumbar vertebral canal. J. Bone Joint Surg. 37B, 576-584, 1955.
37. Wilson, C. B. : Significance of the small lumbar spinal canal: Cauda equina compression syndromes due to spondylosis. Part 3: Intermittent claudication. J. Neurosurg. 31 : 499-506, 1969.
38. Wylie, E. J . : personal communication, 1974. 39. Yamada, H., Ohya, M., Okada, T. and Shio-
zawa, Z.: Intermittent cauda equina com- pression due to narrow spinal canal. J . Neurosurg. 37: 83-88, 1972.