Embed Size (px)
Citation preview

BioMed CentralCases Journal
ss
Open AcceCase ReportInfluence of immediate and permanent obturators on facial contours: a case seriesSüha Türkaslan*1, Timuçin Baykul2, M Asım Aydın3 and M Mustafa Özarslan1Address: 1Department of Prosthodontics, Faculty of Dentistry, Süleyman Demirel University, Isparta, Turkey, 2Department of Oral & Maxillofacial Surgery, Faculty of Dentistry, Süleyman Demirel University, Isparta, Turkey and 3Department of Plastic & Reconstructive Surgery, Faculty of Medicine, Süleyman Demirel University, Isparta, Turkey
Email: Süha Türkaslan* - [email protected]; Timuçin Baykul - [email protected]; M Asım Aydın - [email protected]; M Mustafa Özarslan - [email protected]
* Corresponding author
AbstractIntroduction: Rehabilitation of patients after surgical removal of carcinomas in facial skeleton isone of the most difficult therapies of the stomatognathic system. Significant deformation of tissues,dysfunctions of the stomatognathic system with concurrent biological imbalance of the oral cavityenvironment frequently affect the treatment to become arduous. Scars and contraction of the oralcrevice may cause serious psychological deficiencies that are another aspect of the treatmentschedule.
Case presentation: Three Turkish patients ages 46 (male), 61 (male) and 24 (female) whoexperienced similar operations were rehabilitated with maxillary obturators. The situations wasideal for patient no 1. Patient no 2 could not receive an immediate obturator and patient no 3rejected using permanent obturator. The paper describes the advantages of a surgical obturatorwhich is constructed before operation and inserted immediately following partial maxillectomy andexpresses long term complications when neglecting the use of definite obturator prosthesis, in thelight of three cases.
Conclusion: The primary objective of oral-maxillofacial and plastic surgeons and prosthodontistswhen treating tumors is to eliminate disease and to improve the quality of life including the facialcontours which influences the psychological condition of patient. Neglecting immediate obturatorconstruction may cause serious facial appearance problems due to soft tissue contracture. Whenpermanent obturator is rejected, serious contracture of soft tissues and facial disharmony isinevitable.
IntroductionProstodontic rehabilitation of maxillectomies is the pre-ferred treatment in most centers over autogenous tissuereconstructions [1-5]. It reveals satisfactory outcomes withrespect to speech, nutrition, and facial appearance when
the cooperation of the prostodontist begins before theoperation and the long term management of the patient ismaintained carefully [3,5-9]. When the patient is referredafter the operation, optimum results may not be obtained.Thus, if the patient is lost to follow-up and comes out after
Published: 3 January 2009
Cases Journal 2009, 2:6 doi:10.1186/1757-1626-2-6
Received: 2 December 2008Accepted: 3 January 2009
This article is available from: http://www.casesjournal.com/content/2/1/6
© 2009 Türkaslan et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Page 1 of 5(page number not for citation purposes)
Cases Journal 2009, 2:6 http://www.casesjournal.com/content/2/1/6
a long period without using prosthesis, facial disfigure-ment may be seen to be so severe that resumption of pros-thetic rehabilitation may become impossible [10-14]. Theaim of this paper is to describe and illustrate the advan-tages of a surgical obturator that is constructed beforeoperation and inserted immediately following partialmaxillectomy and to express the long term complicationsof neglected use of prosthesis in the light of three cases.
Case presentationThe following case reports illustrate the benefits of obtu-rator prostheses by emphasizing the advantages of theobturator that was constructed before operation andinserted immediately following maxillary surgery. Denialof using permanent obturator is also demonstrated.
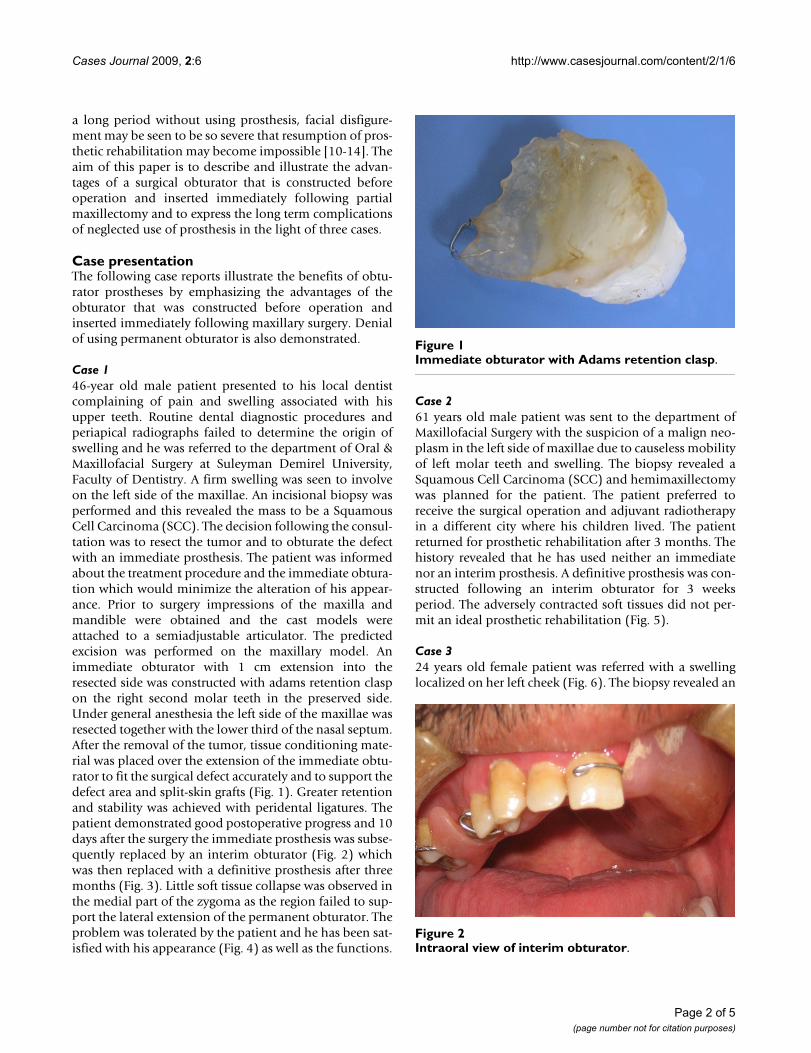
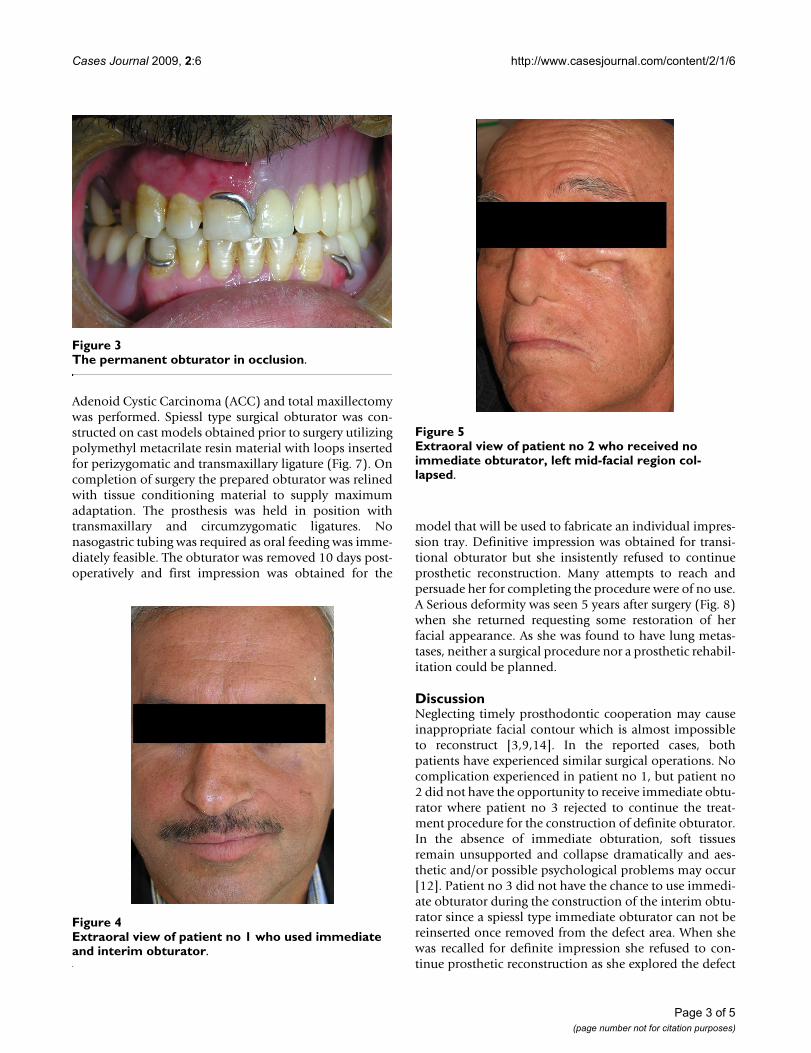
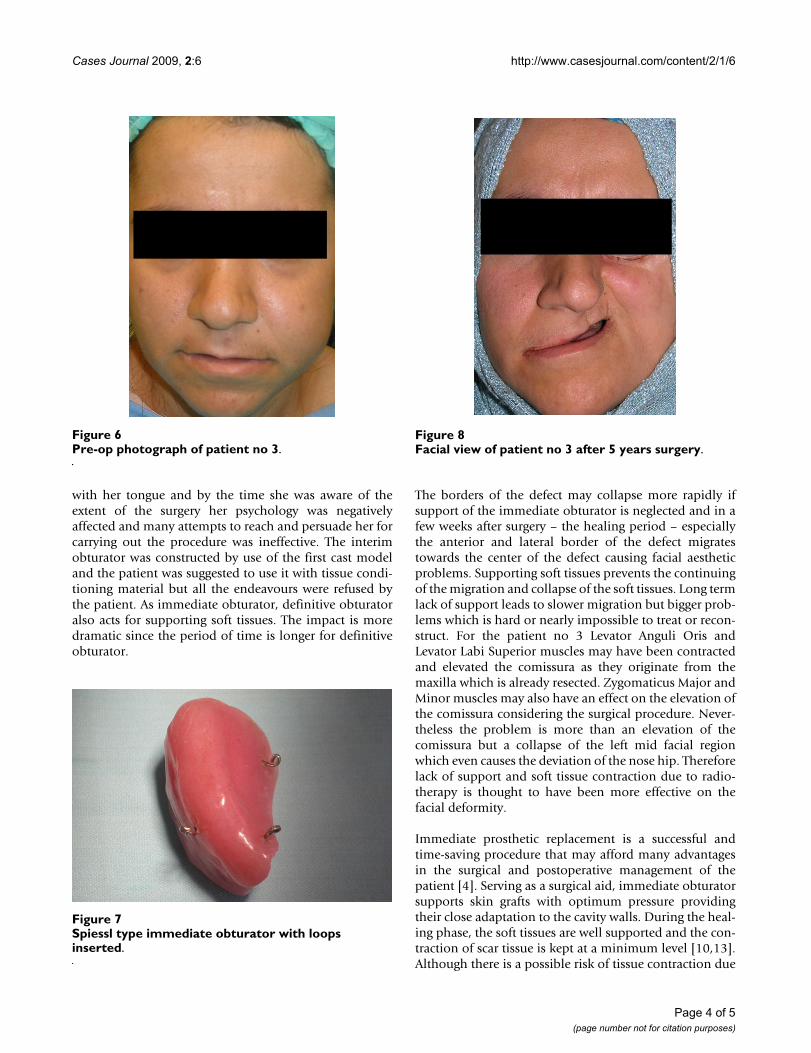
Case 146-year old male patient presented to his local dentistcomplaining of pain and swelling associated with hisupper teeth. Routine dental diagnostic procedures andperiapical radiographs failed to determine the origin ofswelling and he was referred to the department of Oral &Maxillofacial Surgery at Suleyman Demirel University,Faculty of Dentistry. A firm swelling was seen to involveon the left side of the maxillae. An incisional biopsy wasperformed and this revealed the mass to be a SquamousCell Carcinoma (SCC). The decision following the consul-tation was to resect the tumor and to obturate the defectwith an immediate prosthesis. The patient was informedabout the treatment procedure and the immediate obtura-tion which would minimize the alteration of his appear-ance. Prior to surgery impressions of the maxilla andmandible were obtained and the cast models wereattached to a semiadjustable articulator. The predictedexcision was performed on the maxillary model. Animmediate obturator with 1 cm extension into theresected side was constructed with adams retention claspon the right second molar teeth in the preserved side.Under general anesthesia the left side of the maxillae wasresected together with the lower third of the nasal septum.After the removal of the tumor, tissue conditioning mate-rial was placed over the extension of the immediate obtu-rator to fit the surgical defect accurately and to support thedefect area and split-skin grafts (Fig. 1). Greater retentionand stability was achieved with peridental ligatures. Thepatient demonstrated good postoperative progress and 10days after the surgery the immediate prosthesis was subse-quently replaced by an interim obturator (Fig. 2) whichwas then replaced with a definitive prosthesis after threemonths (Fig. 3). Little soft tissue collapse was observed inthe medial part of the zygoma as the region failed to sup-port the lateral extension of the permanent obturator. Theproblem was tolerated by the patient and he has been sat-isfied with his appearance (Fig. 4) as well as the functions.
Case 261 years old male patient was sent to the department ofMaxillofacial Surgery with the suspicion of a malign neo-plasm in the left side of maxillae due to causeless mobilityof left molar teeth and swelling. The biopsy revealed aSquamous Cell Carcinoma (SCC) and hemimaxillectomywas planned for the patient. The patient preferred toreceive the surgical operation and adjuvant radiotherapyin a different city where his children lived. The patientreturned for prosthetic rehabilitation after 3 months. Thehistory revealed that he has used neither an immediatenor an interim prosthesis. A definitive prosthesis was con-structed following an interim obturator for 3 weeksperiod. The adversely contracted soft tissues did not per-mit an ideal prosthetic rehabilitation (Fig. 5).
Case 324 years old female patient was referred with a swellinglocalized on her left cheek (Fig. 6). The biopsy revealed an
Immediate obturator with Adams retention claspFigure 1Immediate obturator with Adams retention clasp.
Intraoral view of interim obturatorFigure 2Intraoral view of interim obturator.
Page 2 of 5(page number not for citation purposes)
Cases Journal 2009, 2:6 http://www.casesjournal.com/content/2/1/6
Adenoid Cystic Carcinoma (ACC) and total maxillectomywas performed. Spiessl type surgical obturator was con-structed on cast models obtained prior to surgery utilizingpolymethyl metacrilate resin material with loops insertedfor perizygomatic and transmaxillary ligature (Fig. 7). Oncompletion of surgery the prepared obturator was relinedwith tissue conditioning material to supply maximumadaptation. The prosthesis was held in position withtransmaxillary and circumzygomatic ligatures. Nonasogastric tubing was required as oral feeding was imme-diately feasible. The obturator was removed 10 days post-operatively and first impression was obtained for the
model that will be used to fabricate an individual impres-sion tray. Definitive impression was obtained for transi-tional obturator but she insistently refused to continueprosthetic reconstruction. Many attempts to reach andpersuade her for completing the procedure were of no use.A Serious deformity was seen 5 years after surgery (Fig. 8)when she returned requesting some restoration of herfacial appearance. As she was found to have lung metas-tases, neither a surgical procedure nor a prosthetic rehabil-itation could be planned.
DiscussionNeglecting timely prosthodontic cooperation may causeinappropriate facial contour which is almost impossibleto reconstruct [3,9,14]. In the reported cases, bothpatients have experienced similar surgical operations. Nocomplication experienced in patient no 1, but patient no2 did not have the opportunity to receive immediate obtu-rator where patient no 3 rejected to continue the treat-ment procedure for the construction of definite obturator.In the absence of immediate obturation, soft tissuesremain unsupported and collapse dramatically and aes-thetic and/or possible psychological problems may occur[12]. Patient no 3 did not have the chance to use immedi-ate obturator during the construction of the interim obtu-rator since a spiessl type immediate obturator can not bereinserted once removed from the defect area. When shewas recalled for definite impression she refused to con-tinue prosthetic reconstruction as she explored the defect
The permanent obturator in occlusionFigure 3The permanent obturator in occlusion.
Extraoral view of patient no 1 who used immediate and interim obturatorFigure 4Extraoral view of patient no 1 who used immediate and interim obturator.
Extraoral view of patient no 2 who received no immediate obturator, left mid-facial region collapsedFigure 5Extraoral view of patient no 2 who received no immediate obturator, left mid-facial region col-lapsed.
Page 3 of 5(page number not for citation purposes)
Cases Journal 2009, 2:6 http://www.casesjournal.com/content/2/1/6
with her tongue and by the time she was aware of theextent of the surgery her psychology was negativelyaffected and many attempts to reach and persuade her forcarrying out the procedure was ineffective. The interimobturator was constructed by use of the first cast modeland the patient was suggested to use it with tissue condi-tioning material but all the endeavours were refused bythe patient. As immediate obturator, definitive obturatoralso acts for supporting soft tissues. The impact is moredramatic since the period of time is longer for definitiveobturator.
The borders of the defect may collapse more rapidly ifsupport of the immediate obturator is neglected and in afew weeks after surgery – the healing period – especiallythe anterior and lateral border of the defect migratestowards the center of the defect causing facial aestheticproblems. Supporting soft tissues prevents the continuingof the migration and collapse of the soft tissues. Long termlack of support leads to slower migration but bigger prob-lems which is hard or nearly impossible to treat or recon-struct. For the patient no 3 Levator Anguli Oris andLevator Labi Superior muscles may have been contractedand elevated the comissura as they originate from themaxilla which is already resected. Zygomaticus Major andMinor muscles may also have an effect on the elevation ofthe comissura considering the surgical procedure. Never-theless the problem is more than an elevation of thecomissura but a collapse of the left mid facial regionwhich even causes the deviation of the nose hip. Thereforelack of support and soft tissue contraction due to radio-therapy is thought to have been more effective on thefacial deformity.
Immediate prosthetic replacement is a successful andtime-saving procedure that may afford many advantagesin the surgical and postoperative management of thepatient [4]. Serving as a surgical aid, immediate obturatorsupports skin grafts with optimum pressure providingtheir close adaptation to the cavity walls. During the heal-ing phase, the soft tissues are well supported and the con-traction of scar tissue is kept at a minimum level [10,13].Although there is a possible risk of tissue contraction due
Pre-op photograph of patient no 3Figure 6Pre-op photograph of patient no 3.
Spiessl type immediate obturator with loops insertedFigure 7Spiessl type immediate obturator with loops inserted.
Facial view of patient no 3 after 5 years surgeryFigure 8Facial view of patient no 3 after 5 years surgery.
Page 4 of 5(page number not for citation purposes)

Cases Journal 2009, 2:6 http://www.casesjournal.com/content/2/1/6
Publish with BioMed Central and every scientist can read your work free of charge
"BioMed Central will be the most significant development for disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
to radiotherapy immediate obturators may resist reboundof non-supported soft tissues. The resection site is pro-tected from food debris, contaminants and trauma, whichmay delay healing or dislodge a skin graft. Consequentlyhealing process is provoked and accelerated. After theoperation, patients are able to swallow food more readilyand to resume a normal diet at an earlier stage[10] whichleads to shorter recovery period. The denture componentof the obturator allows mastication of soft foods initiallyand harder foods several days later [3]. Speech is mini-mally altered and in many instances remains nearlyunchanged [7,8]. Exploration of the defect by the tongueis prevented, and the patient remains unaware of thedimensions of the surgery. By maintaining facial contourand aesthetics, patients are psychologically betterequipped to face rehabilitation [12]. Experience in wear-ing an immediate obturator conditions the individual toaccept the subsequent prosthetic treatment with equanim-ity.
ConclusionThe use of immediate obturators is essential for the opti-mum rehabilitation of oral functions and cosmetics withprosthetics as well as the maintenance of definitive pros-thesis. Immediate obturators support soft tissues after sur-gery and minimize scar contracture and disfigurementthat may have a positive effect on the patients' psychol-ogy. Avoiding immediate obturator construction maycause serious facial appearance problems due to soft tissuecontracture. When wearing the permanent obturator isneglected, the dynamics of non-supported soft tissueschange towards serious contracture and facial dishar-mony.
ConsentWritten informed consent was obtained from the patientsfor publication of this case report and accompanyingimages. A copy of the written consent is available forreview by the Editor-in-Chief of this journal.
Competing interestsThe authors declare that they have no competing interests.
Authors' contributionsTB and MAA operated the patients no 1 & 3. TB also diag-nosed the patient no 2. ST and MMO constructed theprosthesis for both three patients and prepared draft man-uscript. All authors read and approved the final manu-script.
References1. Ackerman AJ: The prosthetic management of oral and facial
defects following cancer surgery. J Prosthet Dent 1955,5:413-438.
2. Zarb GA: The maxillary resection and its prosthetic replace-ment. J Prosthet Dent 1967, 18:268-281.
3. Heggie AA, MacFarlane WI, Warneke SC: Immediate prostheticreplacement following major maxillary surgery. Aust N Z JSurg 1980, 50:370-374.
4. Penn M, Grossmann Y, Shifman A: A preplanned surgical obtura-tor prosthesis for alternative resection lines in the anteriorregion. J Prosthet Dent 2003, 90:510-513.
5. Omondi BI, Guthua SW, Awange DO, Odhiambo WA: Maxillaryobturator prosthesis rehabilitation following maxillectomyfor ameloblastoma: case series of five patients. Int J Prosthodont2004, 17:464-468.
6. Beumer J, Curtis D, Firtell D: Restoration of acquired hard pal-ate defects: etiology, disability and rehabilitation. In Maxillofa-cial rehabilitation: prosthodontic and surgical considerations Edited by:Beumer J III, Curtis TA, Marunick MT. St. Louis: Medico Dental MediaIntl; 1996:225-284.
7. Arigbede AO, Dosumu OO, Shaba OP, Esan TA: Evaluation ofspeech in patients with partial surgically acquired defects:pre and post prosthetic obturation. J Contemp Dent Pract 2006,7:89-96.
8. Oki M, Iida T, Mukohyama H, Tomizuka K, Takato T, Taniguchi H:The vibratory characteristics of obturators with differentbulb height and form designs. J Oral Rehabil 2006, 33:43-51.
9. Park KT, Kwon HB: The evaluation of the use of a delayed sur-gical obturator in dentate maxillectomy patients by consid-ering days elapsed prior to commencement of postoperativeoral feding. J Prosthet Dent 2006, 96:449-453.
10. Lang BR, Bruce RA: Presurgical maxillectomy prosthesis. J Pros-thet Dent 1967, 17:613-619.
11. Desjardins RP: Early rehabilitative management of the maxil-lectomy patient. J Prosthet Dent 1977, 38:311-318.
12. Minsley GE, Warren DW, Hinton V: Physiologic responses tomaxillary resection and subsequent obturation. J Prosthet Dent1987, 57:338-344.
13. Huryn JM, Piro JD: The maxillary immediate surgical obturatorprosthesis. J Prosthet Dent 1989, 61:343-347.
14. Lapointe HJ, Lampe HB, Taylor SM: Comparison of maxillectomypatients with immediate versus delayed obturator prosthe-sis placement. J Otolaryngol 1996, 25:308-312.
Page 5 of 5(page number not for citation purposes)
![Immediate Obturator with Airway for Maxillary Resection ... · Palatal plate of the surgical obturator can easily be modified and used as an interim obturator [16-18]. Benefits of](https://img.dokumen.tips/doc/110x75/5f25b8b636c20c5f147362fe/immediate-obturator-with-airway-for-maxillary-resection-palatal-plate-of-the.jpg)




























