Embed Size (px)
DESCRIPTION
A case study on Acute Lymphocytic Leukemia (ALL)
Citation preview

Introduction of the Client
A 16 year old Malay boy, named Mohammad, presented to the emergency department of General Hospital Malacca on 07 January 2011 at 10:27 AM with fever, joint pain and loss of appetite. He was accompanied by his mother. His mother said that his fever was on and off for the last 2 months and with episode of high grade fever for 2 days in a week.
Based on his mother’s statement, Mohammad did not experience bleeding, any cough, upper respiratory tract and urinary tract infections symptoms and diarrhoea.
Physical Examination
On examination, Mohammad sitting blood pressure was 136/68 mmHg, his pulse rate was 112 bpm and body temperature was 38˚C.
Mohammad was alert, conscious, can speak in full sentences, pale, and not tachypneic. He has no palpable lymph node. Respiratory has clear and equal air entry, CVS showed Dual Rhythm No Murmur, abdomen soft, non-tender and a palpable spleen of about 4cm. and his CNS was grossly weak.
Diagnosis
Based on the clinical investigation and physical examination, Mohammed was diagnosed with Acute Lymphocytic/lymphoblastic Leukaemia (ALL).
Management Plan
Upon admission, the physician ordered IV Tazocin 4.5G TDS, IV infusion of 2 pint Dextrose Saline in 24 hours and FBC test for repeat.
Medical History
Two months ago Mohammad was admitted to Hospital Putra, Malacca. His complaint were tiredness (for 1 month), pale, fever and swelling on both hands. Based on the blood test results, his physician diagnosed him with acute lymphocytic/lymphoblastic leukaemia. Since birth he has no other health complaints except the current diagnosis.
Surgical History
No surgical history.
Family History
Mohammad’s father, a pensioner, told to have diabetes mellitus; his mother, a housewife, has hypertension while the rest of the family are healthy. The family claimed to have no history of malignancy.
Case Study on Acute Lymphocytic Leukemia1

Social History
Mohammad is currently staying with his parents and 1 sister. He is a form 5 student in one of the government school of Malacca. He loves to play football in school and play with his friends in the afternoon after class. He also loves to jog before playing any ballgames. He is the youngest among the 4 siblings in the family, 2 of them are married and are staying on their own.
Food and Drug Allergies
Mohammad has no known allergies.
Case Study on Acute Lymphocytic Leukemia2

Case Study on Acute Lymphocytic Leukemia3

ACUTE LYMPHOCYTIC LEUKEMIA (ALL)
Introduction of the Disease
Leukaemia (also known as “white blood”) is a group of chronic malignant disorders of white blood cells and white blood precursors. It is characterized by replacement of bone marrow by malignant immature white blood cells, abnormal immature circulating WBCs, and infiltration of these cells into the liver, spleen, and lymph nodes throughout the body (LeMone and Burke, 2008).
Physiology Review
Most blood cells are formed in the bone marrow, (the soft material in the center of most bones) called stem cells. Stem cells mature into different kinds of blood cells of which each kind has special functions:
a. White blood cells (also called WBCs or leukocytes), help the body fight infections and other diseases.
b. Red blood cells (also called RBCs or erythrocytes) carry oxygen from the lungs to the body’s tissues and take carbon dioxide from the tissues back to the lungs. The red blood cells give blood its colour.
c. Platelets (also called thrombocytes) help form blood clots that control bleeding.
New or immature blood cells are called blasts. Some blasts stay in the marrow to mature while some travel to other parts of the body to mature. When the blood cells grow old or get damaged, they die, and new cells will form again.
This picture shows how stem cells mature into 2 different types of white blood cells.
a. A myeloid stem cell matures into a myeloid blast, which further
differentiate into granulocytes, neutrophil, eosinophil and basophils.
Case Study on Acute Lymphocytic Leukemia4

b. A lymphoid stem cell matures into a lymphoid blast which further differentiate into lymphoid tissue such as B cells and T cells.
Leukemias are classified based on how quickly the disease develops and gets worse. It can be either chronic (which usually gets worse slowly) or acute (which usually gets worse quickly):
a. Chronic leukemia. It is characterized by an abnormal mature-appearing cell.
b. Acute leukemia. It is characterized by a rapid disease progression and immature or undifferentiated blast cells. They are aggressive tumors that reach a climax within few weeks or months.
The types of leukemia also can be grouped based on the type of white blood cell that is affected, namely lymphoid cells or myeloid cells:
a. Lymphocytic (or lymphoblastic) leukemias involve immature lymphocytes and their precursor cells in the bone marrow. It also penetrates the spleen, lymph nodes, CNS and other tissues. Acute lymphoblastic leukemia (ALL) is most common in children while chronic lymphoblastic leukemia (CLL) affects older adults.
b. Myeloid (also known as myelogenous, myelocytic or myeloblastic) leukemia. This involves the myeloid stem cells in the bone marrow, intervening with the maturation of all types of blood cells, including granulocytes, RBCs, and thrombocytes. This affects mostly on adult people. Acute myeloid leukemia (AML) commonly affects in children and young adults and is usually associated with toxins, genetic disorders and treatment of other cancers. Chronic myeloid leukemia (CML) on the other hand, affects primarily adults.
Pathophysiology
Case Study on Acute Lymphocytic Leukemia5

Bone marrow aspirate from a child with T-cell acute lymphoblastic leukemia. The marrow is replaced with lymphoblasts of various sizes.
Acute lymphocytic leukemia (ALL) is characterized by excessive accumulation of lymphoblasts (immature lymphocytes) in the bone marrow, lymph nodes, and spleen as well
as in the circulating blood and fails to function effectively as normal blood cells to maintain immunity. Lymphoblasts stop the normal bone marrow production of red blood cells, platelets and mature leucocytes resulting to thrombocytopenia, leukopenia, and anemia. Without treatment, the client may die of infection or haemorrhage.
In most cases, ALL result from altered expression of genes whose products contribute to the normal development of B cells and T cells. 80% cases of which results from malignancy transformation of B cells while 20% from T cells. It is most common in children, representing nearly one third of all paediatric cancer cases. The annual incidence is approximately 9-10 cases per 100,000 populations in childhood. The peak incidence occurs in children aged 2-5 years (Wikipedia). In adults, ALL is rarely seen until late middle age people where its incidence increases with aging.
Predisposing Factors
The exact cause of leukemia is not clear. However, few have been associated with an increased risk of developing the disease, to wit:
Radiation: People exposed to very high levels of radiation are much more likely than others to get acute myeloid leukemia, chronic myeloid leukemia, or acute lymphocytic leukemia.
Atomic bomb explosion (World War II): people, especially children, who survive during atomic bomb explosions, are at increased risk of leukemia.
Radiation therapy: medical treatment for cancer and other conditions.
Case Study on Acute Lymphocytic Leukemia6
Bone marrow aspirate from a child with B-precursor acute lymphoblastic leukemia. The marrow is replaced primarily with small, immature lymphoblasts.

Diagnostic x-rays: Exposure to much lower levels of radiation e.g., dental x-rays and other diagnostic x-rays ( CT scans). However, research study is still on going to confirm the link of x-rays and leukemia.
Chemotherapy: Cancer patients treated with certain types of cancer-fighting drugs sometimes later get acute myeloid leukemia or acute lymphocytic leukemia e.g., alkylating agents or topoisomerase inhibitors is linked with a small chance of later developing acute leukemia.
Down Syndrome and Certain Other Inherited Disease increase the risk of acute leukemia.
Clinical Manifestations
Leukemias, like other blood cells, travel through the body where it influences the health and function of all organs and systems. Symptoms may vary from one person to another, depending on the number of leukemic cells and where these cells collect in the body. But generally, manifestation of leukemia results from anemia, infection and bleeding. These include pallor, fatigue, tachycardia, malaise, lethargy, and dyspnoea on exertion.
Infection may cause fever, night sweats, oral ulcerations, and frequent or recurrent respiratory, urinary, integumentary or other infections.
Increased bleeding is due to thrombocytopenia.
Other manifestations results from leukemic cell infiltrations, increased metabolism and increased leukocytes destruction.
Case Study on Acute Lymphocytic Leukemia7

Infiltration of the liver, spleen, lymph nodes and bone marrow causes pain and tissue swelling in the involved areas.
Meningeal infiltration causes increased intracranial pressure that leads to headache, altered level of consciousness, cranial nerve impairment, nausea and vomiting.
Infiltration of the kidney may affect renal function, with decreased urine output and increased blood urea nitrogen and creatinine.
Increased metabolism causes heat intolerance, weight loss, dyspnoea on exertion, and tachycardia.
Destruction of large numbers of WBCs releases substantial amounts of uric acid into the circulation; uric acid crystals may obstruct renal tubules, causing renal insufficiency.
Table 2. General Signs and Symptoms of ALL
POSSIBLE PRESENTED BY THE PATIENT
Fever Fever
Loss of appetite Loss of appetite
Joint/Bone pain Joint/Bone pain
Weakness Weakness
Spleen enlargement (splenomegaly) Spleen enlargement (splenomegaly)
Hepatomegaly Hepatomegaly
Infection (sepsis) Sepsis
Dyspnoea on Exertion
Bleeding
Anemia Anemia
Headache
Vomiting
Confusion
Visual disturbance
Seizure
Lymphadenopathy
Elevated WBCs Elevated WBCs
Of the signs and symptoms listed above, Mohammad’s only showed fever, loss of appetite, bone pain, weakness, sepsis, anemia, elevated WBCs and spleen and liver enlargement of about 4 cm and 5 cm, respectively.
Clinical Investigations
The following clinical investigations are ordered when patient is suspected of leukemia:
Case Study on Acute Lymphocytic Leukemia8

Physical exam: Checks for swollen lymph nodes, spleen, or liver.
Blood tests: Complete blood count to check the number of white blood cells, red blood cells, and platelets. Leukemia causes a very high level of white blood cells. It may also cause low levels of platelets and haemoglobin, which is found inside red blood cells.
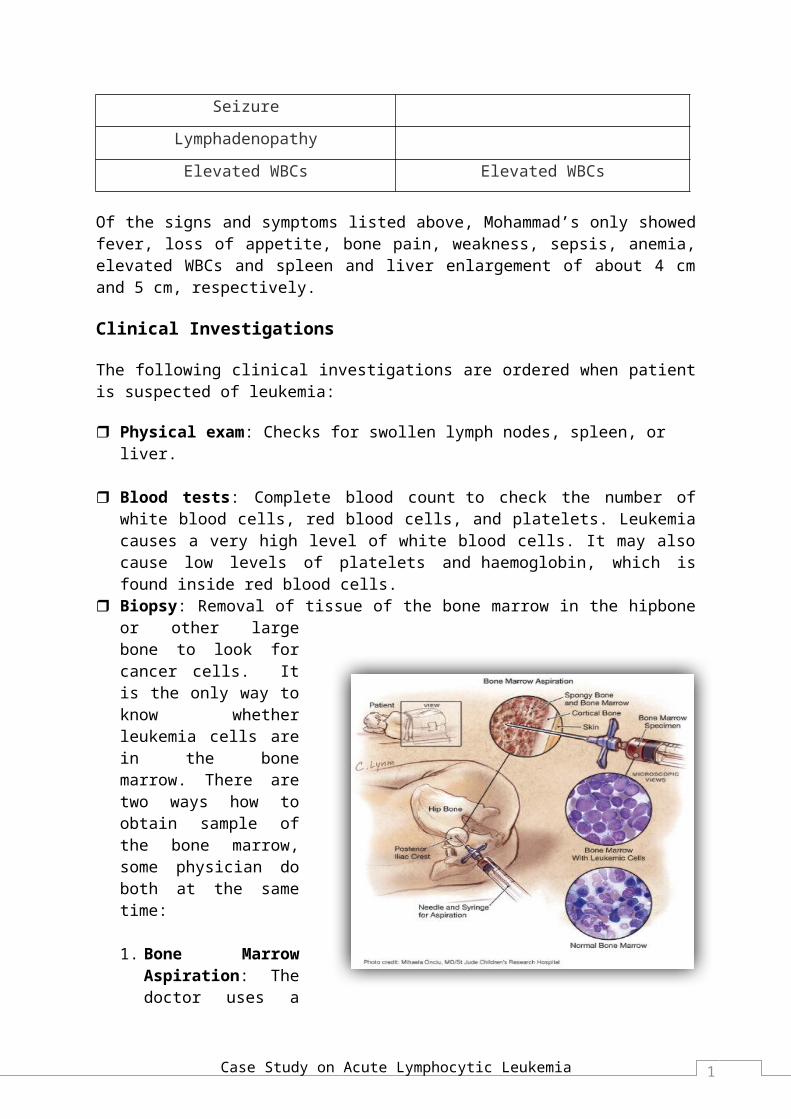
Biopsy: Removal of tissue of the bone marrow in the hipbone or other large bone to look for cancer cells. It is the only way to know whether leukemia cells are in the bone marrow. There are two ways how to obtain sample of the bone marrow, some physician do both at the same time:
1. Bone Marrow Aspiration: The doctor uses a thick, hollow needle to remove samples of bone marrow.
2. Bone Marrow Biopsy. The doctor uses a very thick, hollow needle to remove a small piece of bone and bone marrow.
Lumbar Puncture: A procedure used to collect cerebrospinal fluid from the spinal column. A long, thin needle is inserted into the lower back below the level of spinal cord and fluid is aspirated. If the treatment is for CNS, after aspiration of fluid, chemotherapy is injected into the spinal canal. This procedure is done from time to time to check if leukemic cells are being killed and to give more doses of chemotherapy. Sometimes both chemo and radiation therapies are used.
Chest x-ray: It shows swollen lymph nodes or other organs and bones inside the chest.
For Mohammad, the clinical investigation were purely blood test because he himself and his mother were not keen on bone marrow aspiration, where his doctor recommended to do for further investigation of his case.
Case Study on Acute Lymphocytic Leukemia9
Treatment
Patients with acute lymphocytic leukemia have several treatment options, e.g., chemotherapy, radiation therapy, watchful waiting, targeted therapy, biological therapy, and stem cell transplant. If your spleen is enlarged, your doctor may suggest removal. Sometimes a combination of these treatments is used.
Chemotherapy. This is the treatment choice of most types of leukemia, with a goal of eradicating leukemic cells and producing remission. Children with this disease are likely to be cured and a number of adult patients have high remissions.
Generally, chemotherapy is divided into 2 phases: induction phase therapy and post-remission therapy.
a. Induction Phase. During this phase drugs doses are high to eradicate leukemic cells from the bone marrow. A combination of drugs is used such as daunorubin (cerubidine, an antitumor antibiotic) with vincristine (oncovin, a plant alkaloid) with prednisone with asparaginase (elspar). These high doses of drug often damage the stem cells and interfere with the production of normal blood cells but circulating mature blood cells are not affected because they are no longer dividing. The degree of bone marrow suppression is influenced by the number of factor e.g., age, nutritional status; current chronic diseases (impaired liver or renal function, drug and drug dose and prior treatment.Colony-stimulating factors (CSFs), also called hematopoietic growth factors, and often are administer to rescue the bone marrow following the induction of chemotherapy. CSFs are cytokines that regulate the growth and differentiation of blood cells.
b. Post-remission Therapy. Once remission is achieved, post remission chemotherapy is continued to eradicate any additional leukemic cells, prevent relapse, and prolong survival. A single chemotherapy agent, combination therapy or bone marrow transplant may be used for post remission treatment (LeMone & Burke, 2008).
Radiation Therapy (also called radiotherapy) uses high-energy rays to kill leukemia cells. Radiotherapy damages cellular DNA. Though the leukemic cells continue to function, it cannot divide and multiply e.g., cells in bone marrow and cancer cells divides rapidly and respond quickly to radiation therapy. Radiotherapy is also aimed at the spleen, the brain, or other parts of the body where leukemia cells have collected.
Bone Marrow Transplant (BMT). This is often used in conjunction with chemotherapy or radiation. There are 2 categories:
1. Allogenic BMT. Uses the bone marrow of a healthy donor (usually from a sibling/unrelated closed matched antigen. The donor’s bone marrow is aspirated and is infused through a central venous line into the recipient.
2. Autologous BMT (or bone marrow rescue). Uses the client own bone marrow to restore the bone marrow function after chemotherapy or radiation. During the period of disease remission, about 1L of bone marrow is aspirated from the
Case Study on Acute Lymphocytic Leukemia10
patient. It is then stored and frozen for use after treatment of chemotherapy or radiation, with the aim of destroying the immune system and malignant cells and to prepare space in the bone marrow for new cells. The filtered bone marrow is thawed and infused intravenously through central line and slowly become part of the client’s bone marrow, neutrophil count increases, and normal haematopoiesis takes place.
Allogeneic Stem Cell Transplant. Is a replacement of the recipients blood cell lines (WBCs, RBCs, and platelets) with cells derived from the donor stem cells. This is an alternative to bone marrow transplant. The recipient and the donor tissue must be closely matched prior to harvesting and necessary procedure and treatment are conducted prior to harvesting to prevent the risk of infection and other complications.
Biologic Therapy. Interferon and interleukin (cytokines) may be used to treat leukemias. They modify the body’s response to cancer cells, moderate immune function and inhibit abnormal cell proliferation and growth.
Upon admission of the client, he was given Paracetamol for his fever, IV Tezocin 4.5g tds for his antibiotic and IV infusion of 2 pints normal saline in 24 hours. He was also given a series of blood transfusion due to low haemoglobin count; however, any of the above treatment options were not given to the patient.
Table 3. Schedule of Blood Transfusion
Date Time Amount Transfused (ml) Reaction
07.1.2011 7:30 pm 350 No08.1.2011 7:40 pm 350 No10.1.2011 7:20 pm 345 No11.1.2011 7:00 pm 331 No
Table 4. Medication
Name Indications Side Effects
IV Tazocin 4.5mg (TDS)
Treatment of systemic and local bacterial infection in susceptible organisms. Lower the respiratory tract infection.
Diarrhoea, rashes, nausea, vomiting, increased sweating, weakness, dry mouth, muscle pain.
T. Paracetamol 1g (PRN)
Analgesic. Relief of pain and fever in adult and children.
Vomiting, nausea, abdominal pain, anuria, liver injury, oedema
Case Study on Acute Lymphocytic Leukemia11

The physician of Mohammed order treatment of chemotherapy and bone marrow aspiration, but the patient and his parents refused for the said treatments even after the physician’s explanations about his illness, its complications e.g., bleeding, infection, coma and death, if remain untreated and poor prognosis if treatment is delayed. The patient’s mother only preferred symptomatic treatment and follow up.
Possible Complications
Complications of leukemia and its therapy may differ from one patient to another. The following are the possible complications:
Tumor Lysis Syndrome: Rapid destruction of large numbers of malignant cells leads to alteration in electrolytes (hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia).
Sepsis: Due to low immunity
Renal Failure: Decreased urine output and increased blood urea nitrogen and creatinine.
Bleeding (subarachnoid, renal haemorrhage): Due to thrombocytopenia (low platelet count) leads to bruising, petechiae, bleeding gums, and bleeding within specific organs and tissues.
Neuropathy: Infiltration of leukemic cell in the CNS Seizure (also called convulsion): Due to increased intracranial pressure. Seizure is a
single event abnormal electrical discharge in the brain resulting in an abrupt and temporary altered state of cerebral function
Disseminated Intravascular Coagulation (DIC): A disruption of haemostasis characteristic by widespread intravascular clotting and bleeding
Leukostasis: Blood vessel walls are infiltrated and weakened, with high risk of rupture and bleeding, including intracranial haemorrhage
Until Mohammad was discharge, no complications have been reported.
Case Study on Acute Lymphocytic Leukemia12

Case Study on Acute Lymphocytic Leukemia13

Case Study on Acute Lymphocytic Leukemia14

Case Study on Acute Lymphocytic Leukemia15

Discharge Plan
Mohammed was discharge on 12 January 2011. He was alert, conscious but the skin was a bit pale. His blood pressure was 134/90 mmHg, pulse of 114 bpm, respiratory rate of 20 breath per minute and sPO2 of 100%. He was afebrile and no more complaint of bone pain and his blood test showed still on the low side. Upon his discharge, his physician and staff nurses advised him and his mother on how to keep him healthy as possible, how to prevent himself from getting injury, infection, and what to do if signs and symptoms of illness will come back again.
A. Follow-up Care
He was advised to come to leukemia clinic in 1 month time for blood test. He was advised for a regular check-up, necessary to help ensure that any changes in his health are noted and treated if needed. If any health problems between check-ups are encountered, contact his doctor immediately or come to the hospital.
Check-up may include a careful physical examination, blood tests, cytogenetic, x-rays, bone marrow aspiration, or spinal tap, only upon consent is given.
B. Self Help Guide At Home
Diet: Eat a variety of healthy foods from all the food groups e.g., breads, vegetables, fruits, milk and milk products, and protein (beans, eggs, poultry, meat and fish). Eating healthy foods may help you feel better and have more energy. You may need
Case Study on Acute Lymphocytic Leukemia16

to make diet changes depending on your tolerance. Eat small-frequent meal and snacks rather than 1 big meal which will only suppress the appetite.
Drink Fluids: Drink about about 2-3 liters of liquid each day or prescribed by doctor. Choose healthy like water, juices, and milk rather than carbonated drinks. If you are used to drinking liquids that contain caffeine, such as coffee, these can also be counted in your daily liquid amount.
Avoid Constipation: Try to keep from getting constipation or diarrhoea. These can irritate the rectum which can cause infection. Do not try to push the stool out if it is too hard. Walking is the best way to keep your bowels moving. Eat food high in fiber e.g. cereals, beans, and whole grain breads. Use fiber medicine or a stool softener as prescribed by doctors to soften stools and easy excretion.
Rest: Balance activity to the amount of energy you have. Nap a couple of times during the day. Going to bed early and getting up late may also help.
Exercise: Exercise keeps you healthy. Decrease activities if blood cell count is low based on the result of blood test. Ask your doctor to help you plan the best exercise program for you. Start exercising when your doctor says it is OK. It is best to start slowly and do more as you get stronger.
Avoid Things That Can Cause Cuts Or Bruises: Do not play contact sports since it may bleed or bruise easily.
C. Preventing Infection
Hand washing. Wash hands after using the bathroom and before eating with correct hand washing technique.
Shower daily. Keep yourself clean daily to prevent accumulation of microorganisms on your skin.
Use a deodorant spray instead of antiperspirant. Antiperspirants block sweat glands which can cause an infection.
Brush teeth two to three times a day. Use soft-bristle toothbrush and gently brush teeth to avoid bleeding and infection. See your dentist for regular check-ups to detect and treat dental infection and diseases.
Do not water and take care plants and flowers. Microorganisms are present in plant dirts and flower vase water.
Perineum care. Clean perineum area properly each time you pass urine and bowel.
Stay away from colds or flu. Stay away from large groups of people this will decrease chances of getting sick e.g. colds and flu.
Get vaccinated. Get shots of vaccination to keep from getting flu and pneumonia.
D. Avoid Bruises and Bleeding
Case Study on Acute Lymphocytic Leukemia17

Beware of bumps and cuts. Do not play contact sports such as football or soccer.
Beware of high altitudes. Do not do any activity that may cause chest pain or trouble breathing.
Beware of slippery slippers and shoes. Wear non-skid slippers or shoes when are out of bed and when walking outside especially slippery and wet floors and grounds. This will keep you away from slipping or falling.
Beware of hard-bristled tooth brush. Use soft-bristled brush to help prevent gum bleeding. Do not floss teeth while platelet count is low. Do not use tooth picks, it may prick your gums.
Do not blow your nose hard. It may damage of the mucous membrane increasing the risk of bleeding.
Use nail clippers or a nail file. Do not use scissors to trim your nails. Use nail file to smoothened the nails and trim the sides.
Avoid straining during bowel movement. Ask the doctor for stool softeners to prevent constipation. Walking helps to keep bowels moving.
Beware of Aspirin. Do not take medicine containing aspirin. Aspirin is for thinning of the blood increasing the risk of bleeding.
Put pressure on the bleeding area. Ice packs cool the area and decrease blood flow. Put the ice in a plastic bag and cover with towel and place over at the injured area.
E. Seek care immediately if the following is experienced:
Chest pain.
Trouble breathing.
Fever for the last 2 weeks
Signs of minor bleeding, such as petechiae, ecchymosis, conjunctival haemorrhage, nose bleed, bleeding gums, bleeding at puncture sites.
Be alert for signs of serious bleeding, such as headache with change in responsiveness, blurred vision, haemoptysis (coughing op of blood), hematemesis (vomiting of blood), melena, hypotension, tachycardia, dizziness.
Case Study on Acute Lymphocytic Leukemia18

Case Study on Acute Lymphocytic Leukemia19

Case Study on Acute Lymphocytic Leukemia20

Case Study on Acute Lymphocytic Leukemia21

Case Study on Acute Lymphocytic Leukemia22

Bibliography
Cancer. (2008, February 22). Retrieved January 15, 2011, from The Patrick Demsey Center for Cancer Hope and Healing: http://dempseycenteratcmmc.com/cancers/views/CDR257989
Leukemia. (2009, June 24). Retrieved January 15, 2011, from MedicineNet.com: http://www.medicinenet.com/leukemia/article.htm
Acute Lymphocytic Leukemia. (2010, February 9). Retrieved January 16, 2011, from The Leukemia and Lymphoma Society: http://www.leukemia-lymphoma.org/all_page?item_id=7049
Leukemia. (2011, January 6). Retrieved January 15, 2011, from Wikipedia The Free Encyclopedia: http://en.wikipedia.org/wiki/Leukemia#acute lymphoblastic
Burke, P. L. (2008). Medical Surgical Nursing (6th ed.). New Jersey, USA: Pearson Education International.
Lhynnelli. (2009, April 5). Leukemia Case Study. Retrieved January 16, 2011, from Nursing Crib.com: http://nursingcrib.com/case-study/leukemia-case-study/
Noriko Satake, M. (2010, April 6). Acute Lymphoblastic Leukemia. Retrieved January 15, 2011, from WebMD: http://emedicine.medscape.com/article/990113-overview
Case Study on Acute Lymphocytic Leukemia23

Case Study on Acute Lymphocytic Leukemia24