ContentsIDENTITY2PHYSICAL EXAMINATION (December 1th
2014)6General Status6Antropometry Status8Head to Toe
Examination9Neurological Examination10Meningeal Sign10Motoric
Examination10Autonom Examination11Laboratory Investigation11FOLLOW
UP13LITERATURE
REVIEW18DEFINITION19EPIDEMIOLOGY19PATOFISIOLOGY20CLINICAL
MANIFESTATIONS21DIAGNOSIS22TREATMENT23PREVENTION24PROGNOSIS26REFERENCES27
IDENTITY
Patient Name : FMBirth Date:November 1 th 2004 Age: 11 years
oldGender: MaleAddress: street Panca Warga 2 No 005/2, East
JakartaNationality: IndonesiaReligion: Islam Date of admission:
December 04th 2014.Date of examination: December 04th 2014- Januari
22th 2014
FatherMother
NameMr. IMrs. E
Age43 years old40 years old
JobGuruh gramediaHousewife
NationalityJavaneseJavanese
ReligionIslamIslam
EducationSenior High SchoolSenior High School
Earning/monthApproximately Rp3.000.000,--
Addressstreet Panca Warga 2 No 005/2, East Jakarta
ANAMNESISThe anamnesis was taken on December 04th 2014, by
alloanamnesis (from patients mother).
Chief complain : Massive headache eight days before admission to
the hospital.Additional complains : Fever, Urinating and right leg
starting to lose sensation, shacking and numb, abdominal pain.
History Of Present IlnessA 11 years old came to Raden Said
Sukanto Police Center Hospital with his mother patients complained
of dizziness was heavy on his head back, the patient feels better
when lying down and when walking or sitting head feels heavier, and
feels better when both eyes closed. Since 8 days before msuk
hospital patients also experience fever, fever up and down and
increased late in the afternoon and midnight, when the house
temperature is not measured. Already given paracetamol fever just
down momentarily but increased to 6 days before admission. Patients
treated in hospital depok expectations. During the treatment the
patient felt no improvement. 4 days before admission the patient
urinate more than 10x colored clear day. 3 days before admission
paien complained find it difficult to urinate. 12 hours before
admission the patient complained of right leg can not be moved,
trembling and tingling. Patients present with a referral from
hospital depok expectations.
History Of Past IllnessPharyngitis/Tonsilitis-
Bronchitis-
Pneumonia-
Morbilli-
Pertussis-
Varicella-
Diphteria-
Malaria-
Polio-
Enteritis-
Bacillary Dysentry-
Amoeba Dysentry-
Diarrhea-
Thypoid-
Worms-
Surgery-
Brain Concussion-
Fracture-
Drug Reaction-
Birth HistoryMothers Pregnancy HistoryThe mother routinely
checked her pregnancy to the midwife and Rs. Ibu dan anak. She
denied any problem noted during her pregnancy. She took vitamins
routinely given.
Childs Birth History Labor : RS. Ibu dan anak Birth attendants:
midwife Mode of delivery: sc Gestation: 40 weeks Infant state:
healthy Birth weight : 3100 grams Body length: 50 cm According to
the mother, the baby started to cry and the baby's skin is red, no
congenital defects were reported
Development History First dentition: 6 months Psychomotor
development Head Up: 1 month old Smile: 1 month old Laughing: 1- 2
month old Slant: 2,5 month old Speech Initation: 5 month old Prone
Position: 5 month old Food Self: 5 6 month old Sitting: 6 month old
Crawling: 8 month old Standing: *not able to until present time*
Walking: *not able to until present time*
Mental Status:Normal Conclusion: Growth and development status
is still in the normal limits and was appropriate according to the
patients age
History of Eating Breast Milk : Exclusively 6 month.. Formula
milk : Bebelac since 1 month ago Baby biscuits : Biscuits regal
Fruit and vegetables : Banana, Papaya Solid foods and side dishes :
White ricee, Carrots, PotatoesImmunization
HistoryImmunizationFrequencyTime
BCG1 time1 month old
Hepatitis B3 times0, 1, 6 months old
DPT3 times2, 4, 6 months old
Polio4 times0, 2, 4, 6 months old
Morbilli--
Family History Patients both parents were married when they were
21 years old and 19 years old, and this is their first marriage.
There are not any significant illnesses or chronic illnesses in the
family declared.
History of her brothersNoChildbirthGenderAgeAge DiedSumption
Died
1.Spontan pervaginam, gestation atermBoy
6 years old--
2.Spontan pervaginam, gestation atermGirl
4 years old--
3.Spontan pervaginam, gestation atermGirl10 month--
The patient is the third child of three brothers. Born died : (
- ) Child dies : ( - ) Miscarriage : ( - )
History of Disease in Other Family Members / Around the
HouseThere is no one living around their home known for having the
same condition as the patient.
Sosial and Economic History The patient lived at the house with
size 10 m x 8 m together with father and mother. There are 1 door
at the front side, 1 toilet near the kitchen and 3 rooms, in which
1 room is the bedroom of three of them and 1 room is for guest.
There are 4 windows inside the house. The windows are ocassionaly
opened during the day. Hygiene: The patient changes his clothes
everyday with clean clothes. Bed sheets changed every two
weeks.PHYSICAL EXAMINATION (December 1th 2014)General Status
General condition: mild ill Awareness: Compos Mentis Pulse: 105
x/min, regular, full, strong. Breathing rate: 26x/min Temperature:
38,7oC (per axilla)Antropometry Status Weight: 9 kilogram Height:
69 cm
Nutritional Status based NCHS (National Center for Health
Statistics) year 2000:WFA (Weight for Age): 9/8,9 x 100 % = 101 % (
good nutrition)HFA (Height for Age): 69/71 x 100 % = 97 % (good
nutrition)WFH (Weight for Height): 9/8 x 100 % = 112 %
(normal)Conclusion: The patient has good nutritional status.
Head to Toe Examination
HeadNormocephaly, hair (black, normal distributon, not easily
removed ) sign of trauma (-), large fontanelle closed. EyesIcteric
sclera -/-, pale conjunctiva -/-, hyperaemia conjunctiva -/- ,
lacrimation -/-, sunken eyes -/-, pupils 3mm/3mm isokor, Direct and
indirect light response ++/++ EarsNormal shape, no wound, no
bleeding ,secretion or serumen NoseNormal shape, midline septum,
secretion +/+ Mouth Lips: dry Teeth: no caries Mucous: moist
Tongue: Not dirty Tonsils: T1/T1, No hyperemia Pharynx: No
hyperemia NeckLymph node enlargement (-), scrofuloderma (-)
Thorax:i. Inspection: symmetric when breathing , no retraction,
ictus cordis is not visibleii. Palpation: mass (-), tactile
fremitus +/+iii. Percussion: sonor on both lungsiv. Auscultation:1.
Cor: regular S1-S2, murmur (-), gallop (-)2. Pulmo: vesicular +/+,
Wheezing -/- , Rhonchy -/- Abdomen:i. Inspection: Convex,
epigastric retraction (-), there is no a widening of the veins, no
spider nevi.ii. Palpation: supple, liver and spleen not palpable,
fluid wave (-), abdominal mass (-)iii. Percussion: The entire field
of tympanic abdomen, shifting dullness (-)iv. Auscultation: normal
bowel sound, bruit (-) Vertebra: There does not appear scoliosis,
kyphosis, and lordosis, do not look any mass along the line of the
vertebral Ekstremities: warm, capillary refill time < 2 second,
edema(-) Skin: Good turgor. Neurological ExaminationMeningeal
Sign
Motoric ExaminationPower Hand Feet5 5 5 5/ 5 5 5 55 5 5 5/ 5 5 5
5
Tonus Hand FeetNormotonus / NormotonusNormotonus /
Normotonus
Trophy Hand FeetNormotrophy / NormotrophyNormotrophy /
Normotrophy
Physiologic Reflex Upper extrimities Biceps Triceps
Lower extrimities Patella Achilles
+ / ++ / +
+ / ++ / +
Pathologic Reflex Upper extrimities Hoffman Trommer
Lower extrimities Babinsky Chaddock Oppenheim Gordon
Schaeffer
- / +- / +
- / +- / +- / +- / +- / +
Clonus Patella Achilles- / +- / +
Autonom Examination Defecation Urination SweatingNormal ( 1
times daily, normal consistency )Normal ( 4-5 times daily
)Normal
Laboratory InvestigationHematology December 1th 2014
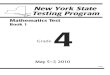
Thorax Photo (December 3th 2014)Right hilar roughInfiltrate (+)
at suprahilar dextra and sinistra.Cor, Sinus, Diaphragma is on a
normal state.Bone and Tissue are on normal limits.Conclusion: Susp.
TB.DD/ Bronchopneumonia
WORKING DIAGNOSISMyelitis TransversaDD/ - Guillain barre -
Chikungunya
MANAGEMENT IVFD KAEN 3B, micro drip, 14 dpm 1000cc / 24 Hours.
Inj. Cefotaxime 2x500 mg IV Paracetamol syrup 3x1 cth Ambroxol
syrup 3x1 cth
PROGNOSIS Quo ad vitam: dubia ad bonam Quo ad functionam: dubia
ad bonam Quo ad sanactionam: dubia ad bonam
LITERATURE REVIEWDEFINITIONTransverse myelitis (MT) is an acute
inflammatory process affecting a focal area of the spinal cord with
the clinical characteristics of the development of acute or
subacute of signs and symptoms of neurological dysfunction in motor
nerves, sensory and autonomic nerves and tracts in the medulla
spinalis2. Disturbances in the spinal cord is usually involve
spinothalamic tract, pyramidal tract, posterior columns, and
funikulus anterior3.In 1948, a neurological dr.Suchett-Kaye of
England, acute transverse myelitis terminology introduced in its
report on a case of transverse myelitis complications after
pneumonia. Transverse describe the clinical presence of a band-like
horizontal area of altered sensation in the neck area or piston.
Since then, the syndrome of progressive paralysis due to
inflammation in the spinal cord known as transverse myelitis.
Inflammation means that there is activation of the immune system
that existed at the lesion area and potentially cause
kerusakan2.ETIOLOGYEtiology MT is a combination of several factors.
However, in some cases, the clinical syndrome is the result of
damage MT nerve tissue caused by an infectious agent or by the
immune system, or both. In some other cases, MT caused by direct
microbial infection in the CNS. MT 30-60% of patients reported
suffering from an infection in 3-8 weeks earlier and serological
evidence of acute infection by rubella, measles, infectious
mononucleosis, influenza, enteroviruses, mycoplasma or hepatitis A,
B, and C. The other pathogen that herpesviruses (CMV, VZV, HSV1,
HSV2, HHV6, EBV), HTLV-1, HIV-1 that directly infects the spinal
cord and cause clinical symptoms MT. Borrelia burgdorferi (Lyme
neuroborreliosis) and Treponema pallidum (syphilis) were also
associated with direct CNS infection and MT1.MT has been associated
with systemic autoimmune diseases such as LES. Some patients
reported having focal spinal vasculitis associated with symptoms
that aktif1 LES.PATHOPHYSIOLOGYAcute transverse myelitis
post-vaccinationEvaluation of spinal cord autopsy showed severe
axonal loss with mild demyelination and infiltration of mononuclear
cells, especially T lymphocytes in the nerve roots and spinal
ganglion. In the spinal cord there is infiltration of lymphocytes
in the perivascular and parenchymal in gray matter, especially in
the anterior horns. Some studies conclude vaccination can induce
autoimmune process that develops into MT5.
MTA parainfectiousAs many as 30-60% of cases of idiopathic
transverse myelitis, there is the presence of respiratory
complaints, gastrointestinal, or systemic disease earlier. The word
"parainfectious" has been used for neurological injury caused by
direct microbial infection and injury caused by infection, direct
microbial infection with immune-mediated damage, or infection are
asymptomatic and followed by a systemic response that induces
neuronal damage. Some of the herpes virus has been associated with
myelitis, and may be the cause of the infection directly to nerve
cells in the spinal cord. Other agents, such as Listeria
monocytogenes brought into the axon to the nerve in the spinal
cord. By using some ways, an agent can achieve access to rich
location of the immune system, avoiding the immune system that are
on other organs. Such a mechanism may explain the inflammation is
limited to a focus area in the spinal cord that can be seen in
patients with MT5.
molecular mimicryMolecular mimicry as a mechanism to explain the
nervous system inflammatory nice sting implemented in cases of GBS.
Campilobakter jejuni infection proven to be an important cause that
precedes the occurrence of GBS. Human neural tissue contains
several subtypes of ganglioside moieties such as GM1, GM2, and GQ1b
in the cell wall. Typical components of human ganglioside, sialic
acid, also found on the surface antigens of C. jejuni
lipopolysaccharide in the outer sheath. Ganglioside antibodies
which react with C. jejuni was found in the serum of patients with
GBS, and has been demonstrated to bind to peripheral nerves,
complement binding, and damaging nerve transmission. Molecular
mimicry in the MTA can also occur due to the formation of
autoantibodies in response to infection that occurs
before.Microbial superantigen-mediated inflammationAnother
relationship between a history of previous infection with the MTA
that the fulminant activation of lymphocytes by microbial
superantigens. Microbial superantigens a peptide that has a unique
capacity to stimulate the immune system, and contribute to
autoimmune disease that varies. Superantigen that has been studied
is Staphylococcal enterotoxin A to I, toxin-1 toxic shock syndrome,
and exotoxin piogen streptococci. Superantigens activate T
lymphocytes with a unique pathway compared with conventional
antigens. Moreover, unlike conventional antigens, superantigens can
activate T lymphocytes in the absence of co-stimulant molecules.
With the existence of this ssperbedaan, superantigens can activate
between 2-20% of circulating lymphocytes compared with conventional
antigens. Moreover, superantigens often cause expansion followed by
deletion of T lymphocyte clones which causes the formation of
"holes" on T lymphocytes for a while after aktivasi5.Stimulation of
a large number of lymphocytes may trigger autoimmune disease by
activating autoreactive T cell clones. In humans, many reports
expansion Vb selected group of patients with autoimmune disease,
which indicates previous exposure to superantigens. Autoreactive T
cells activated by superantigens entering and being retained in the
network of networks with repeated exposure to the autoantigen. In
the central nervous system, which is isolated from Staphylococcal
superantigen-induced paralysis in mice experiments. In humans,
patients with acute disseminated ensefalomyelitis and necrotizing
myelopathy piogen streptococci were found to have
superantigen-induced T cell activation against myelin5 basic
protein.
Humoral abnormalitiesOne of the above process can lead to
abnormalities in the function of the humoral system, with reduced
ability to distinguish between "self" and "non-cell". The formation
of abnormal antibodies can activate other components of the immune
system or attract additional cellular elements to the spinal cord.
Circulating antibodies may form immune complexes and deposited in
an area in the medulla spinalis5.CLINICAL MANIFESTATIONTransverse
myelitis may arise stand alone or together with other diseases.
Acute transverse myelitis said when signs and symptoms develop
within hours to a few days, while the sub-acute clinical symptoms
develops over 1-2 weeks. Transverse myelitis symptoms evolve
rapidly from a few hours to several weeks. Approximately 45% of
patients experience worsening maximally within 24 jam2.Diagnostic
in this patient is clinically characterized by the development of
signs and symptoms of neurological dysfunction in motor nerves,
sensory and autonomic nerves and tracts in the spinal cord either
acute or subacute. Inflammation in the spinal cord pathways
break-this pathway and lead to the presence of the common symptoms
of myelitis transversalis2.Weakness is described as a rapidly
progressive paraparesis lasting, starting from the feet and in
addition can also be followed involvement hand. The weakness may be
the first recorded with signs of pyramidal tract involvement
picture that progresses slowly in the second week after the OS
sakit2.The involvement of the sensory level can be found in nearly
all cases. Pain can arise on the back, extremities or abdomen.
Paresthesia is the most common early signs of transverse myelitis
in adults and not in children. Reduced sensation below the level of
spinal cord involvement in the majority of patients, as well as
pain and temperature.Autonomic symptoms varies consists of an
increase in urinary urgency, urinary incontinence and Alvi
(difficulty or unable to urinate), incomplete emptying of the
stomach or constipation. Also often found as a result of the
involvement of sensory and autonomic nervous system of sexual
dysfunction. More than 80% of patients received clinical signs at
the most severe level within 10 days after onset of symptoms,
although the deterioration of neurological function varied and
lasting progressive, usually takes place in the 4-21 day
2.DIAGNOSISThe diagnostic criteria for acute transverse myelitis
Idiopathic can be seen in Table 2.1. Diagnosis MTA must meet all
the inclusion criteria and none of the exclusion criteria are met.
Diagnosis MTA associated with other diseases must meet all the
inclusion criteria and patients also had clinical manifestations of
the disease are included in the criteria ekslusi6.Table 2.1.
Diagnostic Criteria transverse myelitisinclusion criteria1)
Development of sensory, or autonomic dysfunction motors
attributable to the spinal cord2) Bilateral signs or symptoms
(Although not necessarily symmetric)3) Clearly-defined sensory
level4) Exclusion of extra-axial compressive etiology by
neuroimaging (MRI or myelography; CT of the spine is not
adequate)5) Inflammation within the spinal cord demonstrated by CSF
pleocytosis or elevated IgG index or gadolinium enhancement. If
none of the inflammatory criteria is met at symptom onset, repeat
MRI and LP evaluation between 2 and 7 days after symptom onset
meets criteria6) Progression to nadir between 4 h and 21 days after
the onset of symptoms (if patient awakens with symptoms, symptoms
must Become more pronounced from the point of awakening)exclusion
criteria1) History of previous radiation to the spine within the
past 10 years2) Clear arterial distribution clinical deficit
consistent with thrombosis of the anterior spinal artery3) Abnormal
flow voids on the surface of the spinal cord consistent with AVM4)
serological or clinical evidence of connective tissue disease
(sarcoidosis, Behcet's disease, Sjogren's syndrome, SLE, mixed
connective tissue disorder, etc.) a5) CNS manifestations of
syphilis, Lyme disease, HIV, HTLV-1, mycoplasma, other viral
infection (eg HSV-1, HSV-2, VZV, EBV, CMV, HHV-6, enteroviruses)
a(a) Brain MRI abnormalities suggestive of MSA(b) History of
clinically apparent optic neuritisaAVM, arteriovenous malformation;
CMV, cytomegalovirus; CNS, central nervous system; CSF,
cerebrospinal fluid; CT, computed tomography; EBV, Epstein Barr
virus; HHV, human herpesvirus; HSV, herpes simplex virus; HTLV,
human T cell leukemia virus; LP, lumbar puncture; MRI, magnetic
resonance imaging; MS, multiple sclerosis; SLE, systemic lupus
erythematosus. ADO not exclude disease-associated acute transverse
myelitis.(Quoted from: Transverse myelitis Consortium Working
Group. Proposed diagnostic criteria and nosology of acute
transverse myelitis. Neurology 2002; 59: 499-5TREATMENT No
consensus guidelines Mainstays include: corticosteroids: no
randomized trials plasmapheresis: moderate to severe cases, or
those who do not respond to steroids after 3-5 days Pulse dose IV
cyclophosphamide CSF filtration therapy: spinal fluid is filtered
for inflammatory factors (not available in US) For severe,
refractory cases: 2 year course of azothioprine, methotrexate,
mycophenolate, or oral cyclophosphamide
PREVENTIONimmunotherapies initialsThe goal of therapy during the
acute phase of myelitis is to inhibit progression and initiating
resolution inflamed spinal lesions that can accelerate clinical
improvement. Corticosteroids are the first-line therapy.
Approximately 50-70% of patients experienced a partial or complete
repair. High-dose intravenous regimen (1000 mg methylprednisolone
every day, usually for 3-5 days) given to the patient. Oral regimen
can be used in cases of mild episodes myelitis patients who do not
require hospitalization. Undesirable effects on corticosteroid
therapy are gastrointestinal symptoms, insomnia, headache, anxiety,
hypertension, manic, hyperglycemia, and impaired elektrolit4.With
plasma exchange therapy beneficial in patients who do not respond
to corticosteroids. Hypotension, electrolyte disturbances,
coagulopathy, thrombocytopenia, thrombosis associated with catheter
placement, and infection as a complication of action
ini4.Plasmapharesis useful in patients who still have residual
sensorimotor function when the first attack, but the patients who
lost sensorimotor function improved only when treated with
cyclophosphamide and plasmapharesis. In patients with
demyelination, or long-acting immunomodulatory therapy showed a
reduction in the risk of attack imunosupressan berulang4.
Respiration and Oropharyngeal SupportTransverse myelitis can
cause respiratory failure if the upper cervical spinal cord and
brain stem has been involved. Therefore, regular examination of the
respiratory function and oropharynx are needed during the course of
the disease. Dyspnea, use respiratory muscles, or a weak cough
require further examination of lung function and capacity of forced
respiration. Intubation with mechanical ventilation is
required.abnormalities TonusSevere myelitis cause hypotonia in the
acute phase (spinal shock), but it is usually followed by increased
resistance to movement (spasticity tone), together with involuntary
muscle spasms (spasticity wicked). Spasticity is an adaptive
response, but if excessive, painful or intrusive, requiring
treatment with physiotherapy or drugs. The study controlled trials
examining that baclofen, Tizanidine, and benzodiazepines as a
therapy for patients with spasticity due to brain disorders and
spinalis4 cord.
painfulPain is a frequent manifestation appeared during and
after the attack myelitis and can be caused by direct injury to the
nerves (neuropathic pain), orthopedic factor (pain due to a change
in position or bursitis), spasticity, or a combination of these
factors. Neuropathic pain responds well to anticonvulsant agents,
drugs anti-depressants (tricyclic antidepressants and selective
reuptake inhibitors of serotonin and norepinephrine), NSAIDS, and
narkotik4.
malaiseLimited movement, medications, pain, and other factors
contribute to excessive malaise after myelitis attacks. Data from
randomized controlled trials demonstrated the efficacy of
amantadine for the treatment of malaise due to multiple sclerosis,
and in one study of modafinil may be the treatment of choice.
Stimulants such as methylphenidate Dextroamphetamine or been used
for the treatment of severe and refractory malaise occurring after
the episode myelitis, but the benefits of these agents for the
treatment of patients with myelitis has not been studied in
randomized, controlled trials4.
Bowel dysfunction and GenitourinaryCatheter is usually required
during the acute phase of transverse myelitis due to urinary
retention. After the acute phase, detrusor hyperreflexia usually
appear with the characteristics of frequent urination frequency,
incontinence, and perception of bladder spasm. These symptoms are
usually reduced by administration of anticholinergics (oxybutinin
and tolterodine). Ultrasound to check the remaining volume of urine
after micturition useful to rule out urinary retention, but studies
may be needed to assess urodinamis urinary dysfunction. Drugs that
inhibit 1-adrenergic receptors may help urinary sphincter
relaxation and discharge of urine in patients with sphincter
hyperactivity, but some patients require intermittent
catheterization to empty the bladder kemih4.In acute and chronic
phases of transverse myelitis, bowel dysfunction characterized by
constipation and impaction risk, difficulty emptying the bowel, and
in some cases of incontinence are usually caused by interference
programming to reduce constipation and bowel control defekasi4
time.Sexual dysfunction is a frequent consequence of transverse
myelitis. Manifestations are reduced genital sensation, pain, and
reduced ability to orgasm, or anorgasmia4.
consulting psychiatristMood and anxiety disorders often become
long-term complications in patients with transverse myelitis and
can affect other symptoms, such as pain and sexual dysfunction.
Pharmacotherapy is often prescribed, as monotherapy or combined
with consultation with psikolog4.
PROGNOSISRecovery must begin within six months, and most
patients showed recovery of function neurologinya in 8 weeks.
Recovery may occur rapidly during 3-6 weeks after onset and may
continue even can take place at a slower pace until 2 years. In
these patients treatment progress seen in 2 weeks terapi2.
REFERENCES
1. Kerr, D, 2001. Current Therapy in Neurologic Disease:
Transverse myelitis. 6th ed. [Accessed 20 November 2011]2. Tapiheru
LA, Sinurat PPO, Rintawan K. 2007. Case report: transverse
myelitis. Magazine Medical Nusantara 2007; 40; E235 [Accessed 20
November 2011]3. Al Deeb SM, Yaqub BA, Bruyn GW, Biary NM. 1997.
Acute transverse myelitis: A Localized Form of Postinfectious
encephalomyelitis. Brain 1997; 120; 1115-1122 [Accessed 20 November
2011]4. Frohman EM, DM Wingerchuk. 2010. Transverse myelitis. The
New England Journal of Medicine 2010; 363: 564-72. [Accessed 20
November 2011]5. Kerr DA, Ayetey H. 2002. Immunopathogenesis of
acute transverse myelitis. Current Opinion in Neurology 2002, 15:
339 347 [Accessed 20 November 2011]6. Transverse myelitis
Consortium Working Group. 2002. Proposed Diagnostic Criteria and
Nosology of Acute Transverse myelitis. Neurology 2002; 59; 499-505.
[Accessed 20 November 2011]7. Jacob A, Weinshenker BG. 2008. An
Approach to the Diagnosis of Acute Transverse myelitis. Semin Liver
Dis 2008; 1; 105-120. [Accessed 20 November 2011]Google Translate
for Business:Translator ToolkitWebsite TranslatorGlobal Market
Finder
15