Embed Size (px)
Citation preview
Feature Article_860 1..8
Career in mental health still an unlikely careerchoice for nursing graduates: A replicatedlongitudinal study
John Stevens, Graeme Browne and Iain GrahamSouthern Cross University, Lismore, New South Wales, Australia
ABSTRACT: The lack of qualified mental health nurses is at critical level with the problem likelyto worsen as the aging mental health nursing workforce retires. This study investigates the careerpreferences of undergraduate nursing students by comparing preferences at the start, middle, and endof the Bachelor of Nursing program. The comparison of the cohorts gave an indication of the changein preferences over the intervening years. It replicates research completed in 1992, 1997, and 2001,and develops a profile of nursing career preferences and the rationale underpinning those preferencesin a cohort of students (n = 150) who began their Bachelor of Nursing studies in 2007 and completedin 2009. The main findings included that, like the previous studies, mental health nursing is one ofthe least desirable career choices for most nurses at the start of their course and remains so as theyapproach graduation. The reasons change but the outcome remains the same. The current system ofusing the Bachelor of Nursing award to produce mental health nurses in Australia does not encouragenurses to consider a career in mental health nursing. Which begs the question: where will mentalhealth nurses in the future come from?
KEY WORDS: mental health nursing, recruitment, student nurses career preferences.
Internationally, in developed countries, there is a short-age of nurses. This shortage will worsen as the currentworkforce ages (Graham & Duffield 2010; Nadler-Moodie & Loucks 2011). For mental health nursing, thecurrent and worsening shortage is more serious; mentalhealth nurses as a group are older than the generalnursing population (Ng et al. 2010; Pickens & Fargotstein2006; Whitehead et al. 2007).
The published work has shown consistently thatundergraduate nurses are less likely to choose a career inmental health nursing (Björkman 2008; Charleston &Happell 2006; Halter 2008; Happell & Gough 2007;
Hayman-White & Happell 2005; Ross & Goldner 2009;Stevens & Crouch 1995; Stevens & Dulhunty 1992; 1997;Ward et al. 2003). At least part of the reason is that, inundergraduate nursing programs in Australia, studentsare encouraged to go into medical–surgical nursing aftertheir studies, in order to consolidate their experience(Baker et al. 2010; Nadler-Moodie & Loucks 2011).
Despite the reality of mental health nursing practice,the care of people with mental illness is consideredroutine and mundane in comparison with the excitementinvolved in the manipulation of technology in surgical andcritical care areas of practice (Happell 2001; Ross &Goldner 2009; Stevens & Crouch 1995; Stevens & Dul-hunty 1992; 1997). The studies reported by Stevens andDulhunty (1992; 1997) and Happell (2001) indicated thatnot only had nursing education failed to rectify this situ-ation but it had indeed assisted, through the process ofprofessional socialization, in exacerbating it.
Correspondence: John Stevens, Southern Cross University, PO Box157, Lismore, NSW 2480, Australia. Email: [email protected]
John Stevens, RN, PhD.Graeme Browne, RN, PhD.Iain Graham, RN, PhD.Accepted June 2012.
bs_bs_banner
International Journal of Mental Health Nursing (2012) ••, ••–•• doi: 10.1111/j.1447-0349.2012.00860.x
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

THE STUDY
In the light of the worsening shortage of qualified nursesin mental health care, this study asks the question that,given the intervening years, has the developing bodyof knowledge, strategies, and efforts to improve recruit-ment to mental health nursing from current Bachelorof Nursing programs encouraged students to considermental health as a career option?
This longitudinal study replicates the Australianresearch by Stevens and Dulhunty (1992; 1997) andHappell (2001) that explored the career choices ofstudent nurses (and the reasons for those choices) withregard to mental health nursing. The career choices ofstudent nurses are examined from a cohort who begantheir studies in 2007.
AIM
The research aim was to develop a profile of nursingcareer preferences and rationale underpinning choicesin a cohort of students who began their Bachelor ofNursing studies in 2007 and completed in 2009. It wasexpected that comparing preferences at the start, middle,and end of the Bachelor of Nursing program wouldimprove understanding of the impact of that program onstudents’ career choices.
ETHICS
Ethics approval was obtained from Southern Cross Uni-versity’s Ethics Committee. Students were advised ver-bally and in writing that participation was voluntary andthat they could withdraw at any point without prejudice.Students were encouraged to identify themselves eitherby name or code of their choice on the questionnairesso that their responses could be matched over three datacollection points. They were advised that once the ques-tionnaires were matched the data would be de-identified.They were informed that the return of a completed orpartially completed questionnaire would be considered asan indication of informed consent.
DESIGN
This study used a repeated measures design. Data werecollected at three time points over 3 years of an under-graduate nursing program and used a non-probabilitysample of undergraduate Bachelor of Nursing studentsin the state of New South Wales (NSW), Australia. Thedata collection commenced in February 2007 and was
completed at the end of 2009 when this cohort of stu-dents neared completion of their undergraduate nursingstudies.
DATA COLLECTION AND ANALYSIS
This study used a questionnaire developed by Stevens andCrouch (1995). Students were asked to rank career pref-erences from 10 choices, where 1 was the most popularcareer destination and 10 the least. This instrument hasbeen used to investigate nursing students’ attitudes instudies by Stevens and Dulhunty (1992; 1997) and latermodified and used by Happell (2001).
Data from the questionnaires were analyzed usingthe Statistical Package for the Social Sciences ver. 19(SPSS, Chicago, IL, USA). The rankings between thethree time points were then tested for statistical signifi-cance using non-parametric statistics, particularly theWilcoxon rank sum test.
The questionnaire had a section that asked students toqualify their rankings by providing reasons for the mostand least popular choices, as well as the ranking of threeother specific areas: working with older people, mentalhealth, and intensive care nursing. Data were also col-lected on reasons for entering nursing, previous lifeand work experiences, as well as the number of days thatstudents could recall having spent on practicum in theranked areas.
The responses to these open-ended questions wereanalyzed by the author for major themes using contentanalysis (Graneheim & Lundman 2004). Where appropri-ate, the themes were coded to match the equivalentthemes developed from the earlier studies.
An audit of the qualitative component of 30 randomlychosen questionnaires was undertaken by a second expe-rienced researcher. The process was aimed at improvingthe consistency of the analysis of the open-ended ques-tions that were used to have students explain their rankingchoices. The audit found that of the 30 questionnaires, 30were coded the same by the auditor and the author.
PARTICIPANTS
Six campuses within NSW were approached to participatein the study, and eventually three agreed to be involved.
The first stage of the study was undertaken within thefirst week of the first semester of the Bachelor of Nursingprogram at each site. With the cooperation of faculties, thequestionnaire was administered in lecture time in order toencourage a high return rate. Based on expected enrol-ment numbers at each location, 300 survey questionnaires
2 J. STEVENS ET AL.
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.
were distributed and 203 (68%) were returned completed.The second stage of the study was undertaken at the endof the third semester or midway point of the programs.Based on remaining enrolment numbers, 250 survey ques-tionnaires were distributed and 189 (76%) were retuned.The third stage of the study was undertaken in the lastweek of lectures in the final semester. Two hundredsurveys were distributed and 160 (80%) were returned.After the 3 years, 150 of the questionnaires were matchedat the three time points; these were used in the analysis forthis study.
RESULTS
As can be seen in Table 1, there were 150 participantswhose questionnaires could be matched at each adminis-tration over the 3 years. Of these, 124 (82.6%) werewomen and 26 (17.3 %) were men, which is an approxi-mately 50% greater proportion of men than shown in thenational registered nurse work force figures which areapproximately 90% women and 10% men (AustralianInstitute of Health and Welfare 2009). The age of partici-pants in the first stage of the study ranged 17–64 years andhad a mean of 26 and a mode of 18 years. The first stageresponses indicated that 93 (62%) participants had noprevious experience working in health, 36 (24%) had beenor were currently assistants in nursing, and three (2%) hadbeen enrolled nurses. A further nine (6%) had experiencein healthcare in other roles such as wards-people andcleaners. Of those who were assistants in nursing, all hadbeen or were currently working in residential aged care,and of these 10 noted they had over 10 years experience.
Table 2 shows the rank order of career preferencesfor the three stages of the study. Those career preferencesmarked with an asterisk indicate that following analysisby Wilcoxon rank sum test there was statistically signifi-cant movement of preference over the three stages(P < 0.01).
Table 2 shows that working in mental health andcommunity health nursing were ranked eighth and ninth,respectively, in the first stage of the questionnaire, andseventh and eighth in the second and third stages. TheWilcoxon rank sum test showed that movement over thethree stages was not statistically significant (P = 0.345 and0.2, respectively).
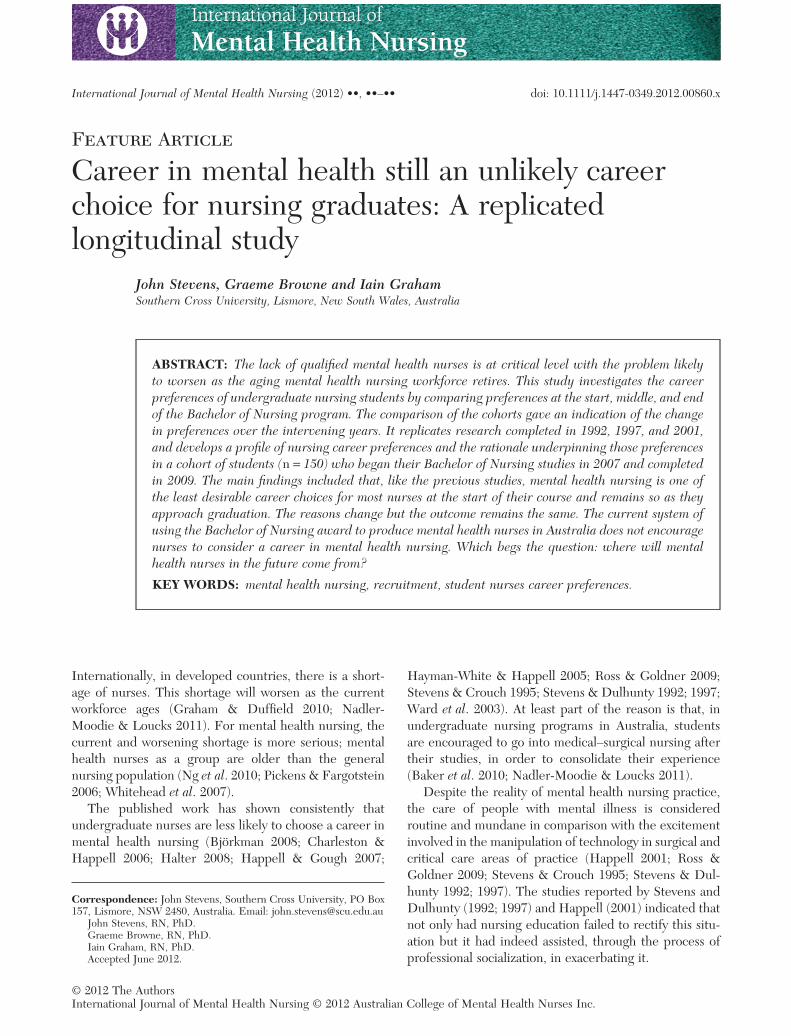
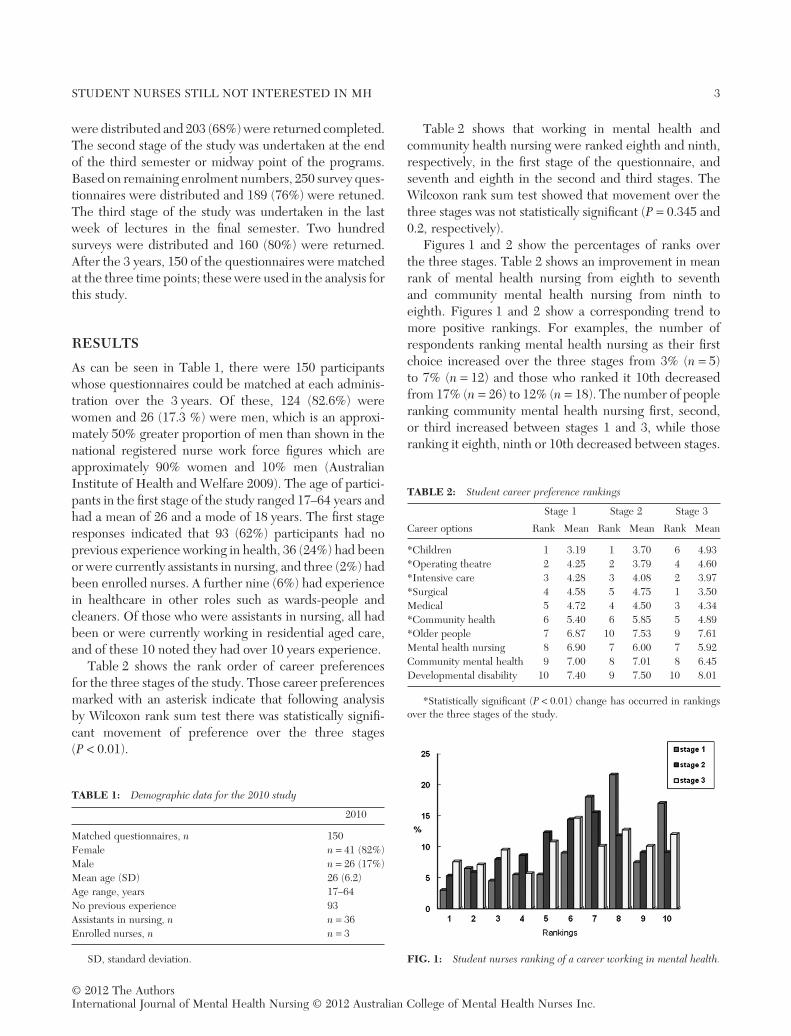
Figures 1 and 2 show the percentages of ranks overthe three stages. Table 2 shows an improvement in meanrank of mental health nursing from eighth to seventhand community mental health nursing from ninth toeighth. Figures 1 and 2 show a corresponding trend tomore positive rankings. For examples, the number ofrespondents ranking mental health nursing as their firstchoice increased over the three stages from 3% (n = 5)to 7% (n = 12) and those who ranked it 10th decreasedfrom 17% (n = 26) to 12% (n = 18). The number of peopleranking community mental health nursing first, second,or third increased between stages 1 and 3, while thoseranking it eighth, ninth or 10th decreased between stages.
TABLE 1: Demographic data for the 2010 study
2010
Matched questionnaires, n 150Female n = 41 (82%)Male n = 26 (17%)Mean age (SD) 26 (6.2)Age range, years 17–64No previous experience 93Assistants in nursing, n n = 36Enrolled nurses, n n = 3
SD, standard deviation.
TABLE 2: Student career preference rankings
Career options
Stage 1 Stage 2 Stage 3
Rank Mean Rank Mean Rank Mean
*Children 1 3.19 1 3.70 6 4.93*Operating theatre 2 4.25 2 3.79 4 4.60*Intensive care 3 4.28 3 4.08 2 3.97*Surgical 4 4.58 5 4.75 1 3.50Medical 5 4.72 4 4.50 3 4.34*Community health 6 5.40 6 5.85 5 4.89*Older people 7 6.87 10 7.53 9 7.61Mental health nursing 8 6.90 7 6.00 7 5.92Community mental health 9 7.00 8 7.01 8 6.45Developmental disability 10 7.40 9 7.50 10 8.01
*Statistically significant (P < 0.01) change has occurred in rankingsover the three stages of the study.
FIG. 1: Student nurses ranking of a career working in mental health.
STUDENT NURSES STILL NOT INTERESTED IN MH 3
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.
EXPERIENCE AND CHOICE
Table 3 shows the number of days students calculatedthat they had spent in each of the ranked areas. Pearson’scorrelations were conducted on the number of days spenton practicum and the ranking changes over the threestages. Table 3 shows that the more time spent on practi-cum in community mental health significantly correlated(r = 0.240) with an increase in preference for it as careerdestination, even though the average length of experi-ences was a relatively short duration of 4.8 days.
There are also correlations for time spent and rankingchanges for working with older people, and in operatingtheatres and community health. In the case of workingwith older people, there was a large significant correlation(r = 0.825) with number of days spent on practicumand a decrease in the preference of working with olderpeople as a career destination. In the case of operatingtheatres (r = 0.305) and community nursing (r = 0.240),
the correlations indicated that more time on practicumled to more favourable rankings. There was no correlationbetween days spent on practicum and mental healthnursing (r = 0.025).
REASONS FOR RANKING MENTALHEALTH NURSING
Responses were divided into positive and negativereasons for choices and then coded into the five categories(Tables 4,5) used in previous iterations of this survey.
The majority of reasons provided for ranking of themental health career options were negative. There wasa total of 50 positive reasons compared to 292 negativereasons received over the three stages of the question-naire (there were also 53 responses that were consideredneutral or non-specific and 45 questionnaires with noresponses to these items).
Positive responses were quite general and mostlynon-specific over the three stages. They provided littleinsight into reasons for choice and included commentslike: ‘I just think I would like it’ (stage 1), ‘because I feelI could be good at it’ (stage 1), ‘I can make a differencehere’ (stage 2), and ‘I loved the team I was with’ (stage 3).For community nursing, comments included: ‘I don’treally know what it is but sounds cool’ (stage 1), ‘the
FIG. 2: Student nurses ranking of a career working in communitymental health.
TABLE 3: Correlation between practicum days and rankings overthree stages in the 2010 study
Days onpracticum, n
Correlation,r
Paediatrics 2.6 0.023Operating theatres 4.7 0.305Intensive care 3.2 0.000Surgical 10.8 0.049General medical 13.2 0.000Community health 6.3 0.240Working with older people 15.7 0.825Mental health nursing 10.0 0.049Community mental health 4.8 0.240Developmental disability 0.3 0.005
TABLE 4: Positive responses to choices for a career in mental healthnursing
Total positive responsesStage 1 Stage 2 Stage 3n = 10 n = 20 n = 20
A. Negative view of clients 20% 20% 20%B. Negative view of the institutions
and type of work found there30% 25% 25%
C. Negative effect on self-esteem 30% 25% 25%D. Negative effect on career pathway 20% 30% 20%E. Negative experience specific to
the course0% 0% 10%
TABLE 5: Negative responses to choices for a career in Mental HealthNursing
Total negative responses n =Stage 1 Stage 2 Stage 3n = 93 n = 105 n = 94
A. Negative view of clients 32% 21% 13%B. Negative view of the institutions and
type of work found there21% 29% 18%
C. Negative effect on self esteem 21% 10% 7%D. Negative effect on career pathway 25% 30% 54%E. negative experience specific to
the course0% 12% 7%
4 J. STEVENS ET AL.
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.
relaxed atmosphere’, ‘more one on one time for holisticcare’ (stage 3), and ‘I’d be out and about’ (stage 3).
Most negative comments were focused on the clientelein stage 1; they made comments on the nature of thepeople they would be working with like: ‘you would not beable to turn your back on them’, ‘the uncertainty of psy-chiatric patients makes them terrifying’, ‘you can’t tell thestaff from the patients’, ‘it would depress me’, ‘I am notpersonally suited to this area’, ‘it’s not an exciting careerarea’, and ‘I think I would go as crazy as they are’.
By stage 3, negative responses were in the clear major-ity and focused on mental health nursing as a careeroption and still some negativity about the people theywould be working with. Comments included: ‘this isnot where I can make my mark’, ‘no career prospectshere’, ‘how would I ever get the skills to become a CNC(clinical nurse consultant) here?’, ‘the staff at (namewithheld) were unreceptive . . . they really turned me offgoing there’, ‘psych drained me so emotionally that after afew days I’d had it’, ‘I am not emotionally strong enoughto work there’, ‘despite all the education I still get thecreeps and feel depressed about being there’, ‘I am nolonger afraid of the mentally ill [sic] but I would preferpatients who are going to get better’, ‘I like to see peoplego home and know they are cured, that does not appear tohappen in psych’, and ‘I can’t stand crazy people’.
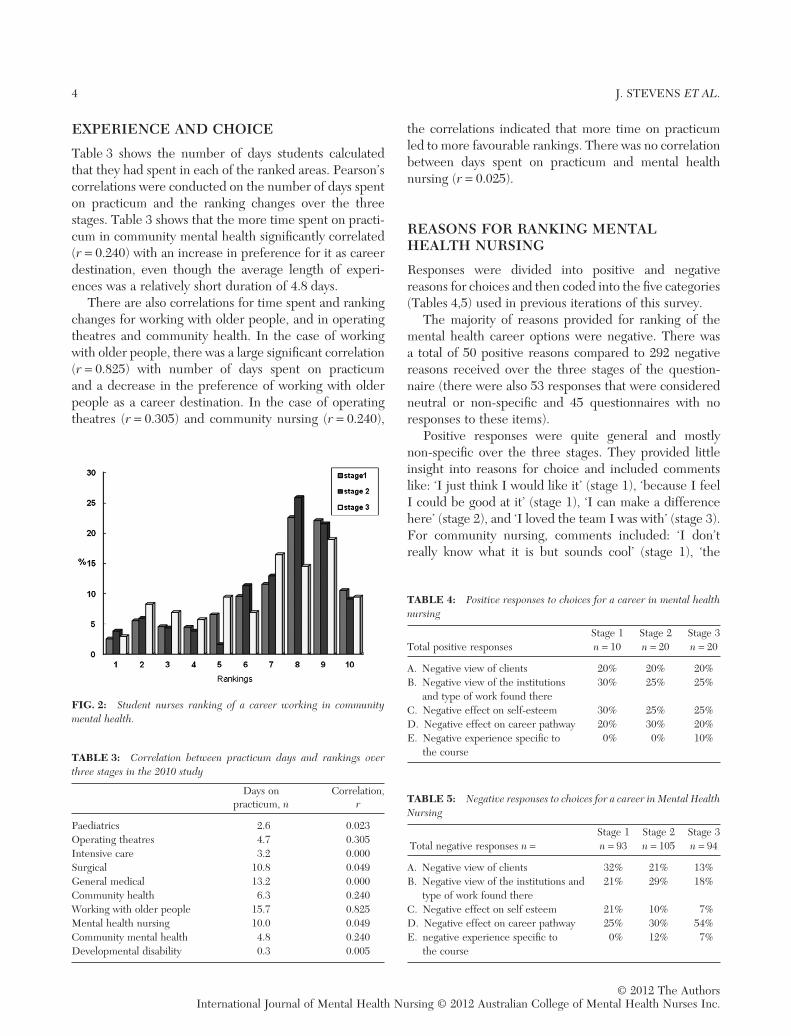
To better understand the reasons for students careerchoices, the findings related to choices of the morepopular career options are reported (Figure 3).
The most common reason for intensive care beingranked highly in the third stage was because the graduatesreported that it was a great place to develop skills andgain the experiences needed to have a successful nursingcareer (n = 69, 46%). Some typical responses were: ‘this iswhere the action is’, ‘if I can learn the skills needed hereI can do anything, work anywhere’, and ‘I feel I can builda long lasting meaningful career here’.
REASONS FOR RANKING SURGICALNURSING AND OTHERS
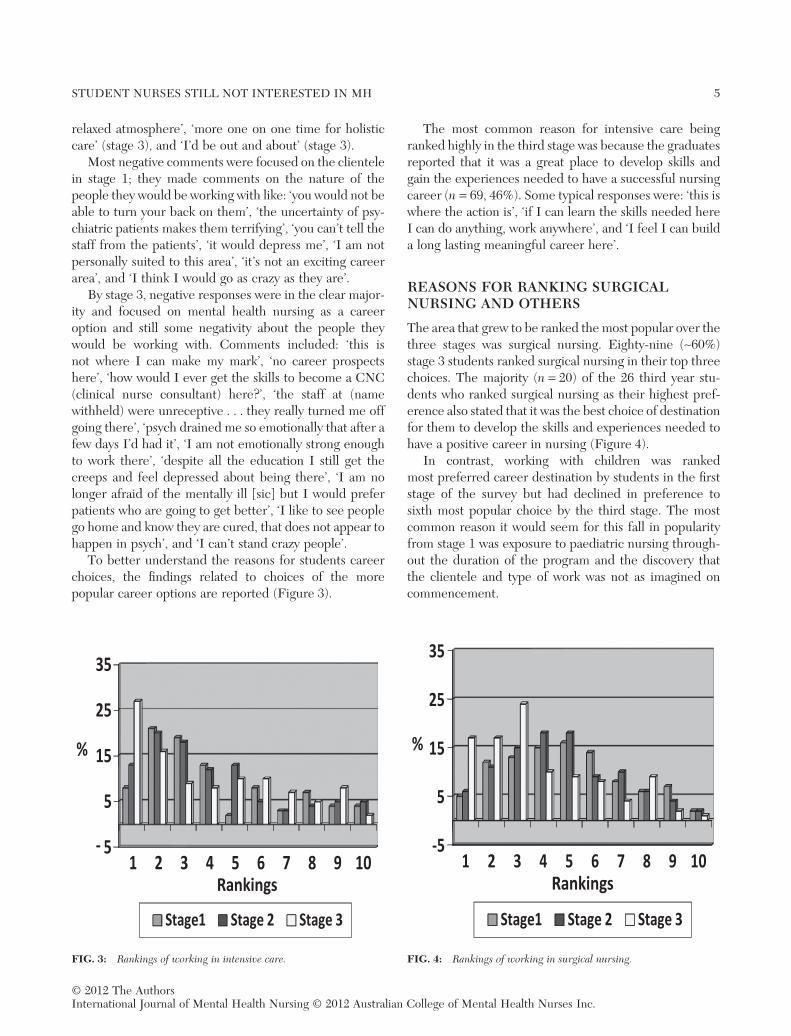
The area that grew to be ranked the most popular over thethree stages was surgical nursing. Eighty-nine (~60%)stage 3 students ranked surgical nursing in their top threechoices. The majority (n = 20) of the 26 third year stu-dents who ranked surgical nursing as their highest pref-erence also stated that it was the best choice of destinationfor them to develop the skills and experiences needed tohave a positive career in nursing (Figure 4).
In contrast, working with children was rankedmost preferred career destination by students in the firststage of the survey but had declined in preference tosixth most popular choice by the third stage. The mostcommon reason it would seem for this fall in popularityfrom stage 1 was exposure to paediatric nursing through-out the duration of the program and the discovery thatthe clientele and type of work was not as imagined oncommencement.
FIG. 3: Rankings of working in intensive care. FIG. 4: Rankings of working in surgical nursing.
STUDENT NURSES STILL NOT INTERESTED IN MH 5
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.
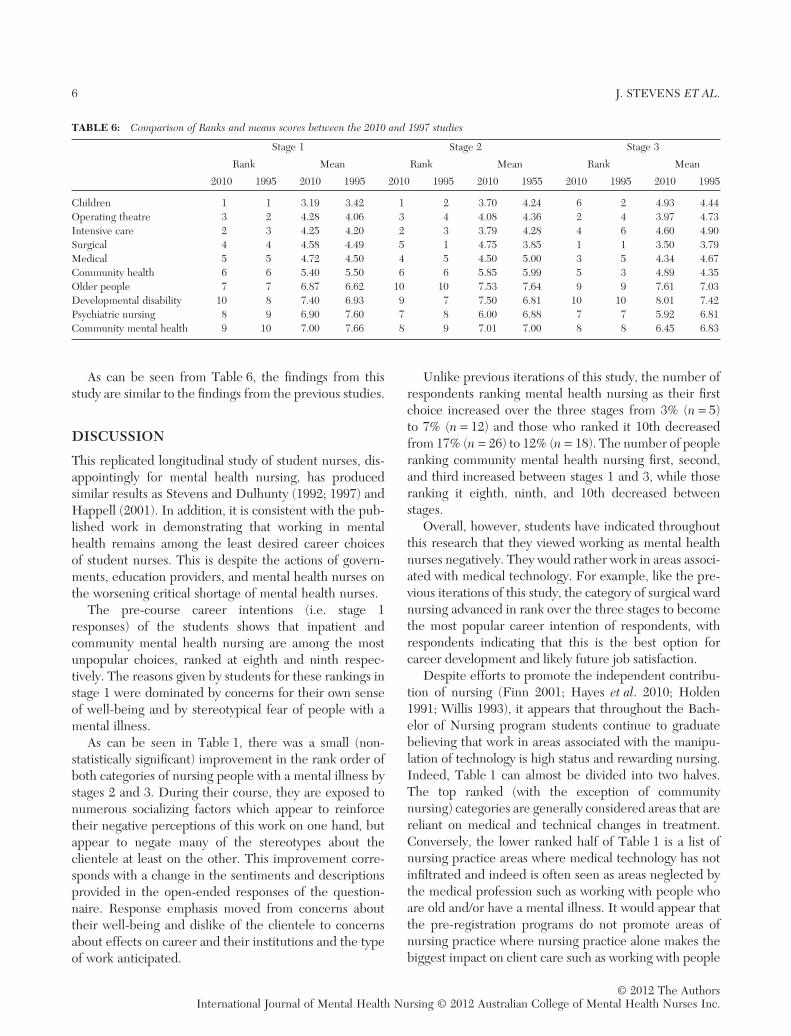
As can be seen from Table 6, the findings from thisstudy are similar to the findings from the previous studies.
DISCUSSION
This replicated longitudinal study of student nurses, dis-appointingly for mental health nursing, has producedsimilar results as Stevens and Dulhunty (1992; 1997) andHappell (2001). In addition, it is consistent with the pub-lished work in demonstrating that working in mentalhealth remains among the least desired career choicesof student nurses. This is despite the actions of govern-ments, education providers, and mental health nurses onthe worsening critical shortage of mental health nurses.
The pre-course career intentions (i.e. stage 1responses) of the students shows that inpatient andcommunity mental health nursing are among the mostunpopular choices, ranked at eighth and ninth respec-tively. The reasons given by students for these rankings instage 1 were dominated by concerns for their own senseof well-being and by stereotypical fear of people with amental illness.
As can be seen in Table 1, there was a small (non-statistically significant) improvement in the rank order ofboth categories of nursing people with a mental illness bystages 2 and 3. During their course, they are exposed tonumerous socializing factors which appear to reinforcetheir negative perceptions of this work on one hand, butappear to negate many of the stereotypes about theclientele at least on the other. This improvement corre-sponds with a change in the sentiments and descriptionsprovided in the open-ended responses of the question-naire. Response emphasis moved from concerns abouttheir well-being and dislike of the clientele to concernsabout effects on career and their institutions and the typeof work anticipated.
Unlike previous iterations of this study, the number ofrespondents ranking mental health nursing as their firstchoice increased over the three stages from 3% (n = 5)to 7% (n = 12) and those who ranked it 10th decreasedfrom 17% (n = 26) to 12% (n = 18). The number of peopleranking community mental health nursing first, second,and third increased between stages 1 and 3, while thoseranking it eighth, ninth, and 10th decreased betweenstages.
Overall, however, students have indicated throughoutthis research that they viewed working as mental healthnurses negatively. They would rather work in areas associ-ated with medical technology. For example, like the pre-vious iterations of this study, the category of surgical wardnursing advanced in rank over the three stages to becomethe most popular career intention of respondents, withrespondents indicating that this is the best option forcareer development and likely future job satisfaction.
Despite efforts to promote the independent contribu-tion of nursing (Finn 2001; Hayes et al. 2010; Holden1991; Willis 1993), it appears that throughout the Bach-elor of Nursing program students continue to graduatebelieving that work in areas associated with the manipu-lation of technology is high status and rewarding nursing.Indeed, Table 1 can almost be divided into two halves.The top ranked (with the exception of communitynursing) categories are generally considered areas that arereliant on medical and technical changes in treatment.Conversely, the lower ranked half of Table 1 is a list ofnursing practice areas where medical technology has notinfiltrated and indeed is often seen as areas neglected bythe medical profession such as working with people whoare old and/or have a mental illness. It would appear thatthe pre-registration programs do not promote areas ofnursing practice where nursing practice alone makes thebiggest impact on client care such as working with people
TABLE 6: Comparison of Ranks and means scores between the 2010 and 1997 studies
Stage 1 Stage 2 Stage 3
Rank Mean Rank Mean Rank Mean
2010 1995 2010 1995 2010 1995 2010 1955 2010 1995 2010 1995
Children 1 1 3.19 3.42 1 2 3.70 4.24 6 2 4.93 4.44Operating theatre 3 2 4.28 4.06 3 4 4.08 4.36 2 4 3.97 4.73Intensive care 2 3 4.25 4.20 2 3 3.79 4.28 4 6 4.60 4.90Surgical 4 4 4.58 4.49 5 1 4.75 3.85 1 1 3.50 3.79Medical 5 5 4.72 4.50 4 5 4.50 5.00 3 5 4.34 4.67Community health 6 6 5.40 5.50 6 6 5.85 5.99 5 3 4.89 4.35Older people 7 7 6.87 6.62 10 10 7.53 7.64 9 9 7.61 7.03Developmental disability 10 8 7.40 6.93 9 7 7.50 6.81 10 10 8.01 7.42Psychiatric nursing 8 9 6.90 7.60 7 8 6.00 6.88 7 7 5.92 6.81Community mental health 9 10 7.00 7.66 8 9 7.01 7.00 8 8 6.45 6.83
6 J. STEVENS ET AL.
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.

with a mental illness. This is of concern for the futureof the nursing profession in general and mental healthnursing in particular.
There is an irony in students believing that theircareers will be better served by choosing a ‘high-tech’destination, an area which is the most resourced and leastlikely to contribute to the health of the community (WorldHealth Organisation 1986, World Health Organisation,1990). The areas considered ‘high-tech’ are already domi-nated by medicine. As these are often the areas for themedical treatment of illness, the practice of nurses inthese areas is limited and more often than not led bymedical professionals and least likely to value the contri-bution of nursing.
On the other hand, the more consumer focused areassuch as mental health rely heavily on the skills and prac-tice of nurses. As noted in the published work and gov-ernment reports above, there will be an increasing needfor competent nurses in this environment in light of theinevitable global movement of decreasing affordabilityand therefore reliance on traditional tertiary settings,especially in dealing with chronic disease managementand illness prevention.
LIMITATIONS
The findings from this study used data from 150 question-naires out of a possible 300. This study could have beenimproved if more demographic data were collected fromthe participants. This could have given an indication ifthose variables impacted on decisions and perhaps anindication of the differences between the participantswho chose to be involved and those who did not completethe data collection. The decision not to collect specificdemographic data was made in an effort to maintainboth confidentiality and the students’ confidence in thatconfidentiality.
IMPLICATION FOR PRACTICE
The direct implication of the published work and thesedata is that they suggest that the continuation of mentalhealth care as an area of nursing practice is under very realthreat. Clearly, nursing bachelors degree programs fail toencourage nurses to consider, positively, the prospect of acareer in mental health nursing. Therefore, with the intro-duction of the nursing professional degree the profession,as a whole, should be deeply concerned for the future aswell as for the continuation of quality care for people livingwith a mental illness. This area of practice will be led byother less qualified occupational groups unless much more
thought and resources than currently allocated areprovided to making a career in mental health more appeal-ing to nursing graduates. This study suggests that an alter-nate pathway to registration for those wanting a career inmental health nursing needs to be reconsidered.
Further holistic person-centred care is the business ofall nurses. If the mental health aspects of care are under-valued in comparison to bio-medical aspects, nurses arenot being properly prepared for their role.
REFERENCESAustralian Institute of Health and Welfare (Australia)
(2009). Health and Community Services Labour Force,2006. Canberra: Australian Institute of Health and Welfare.
Baker, J., Playle, J., Nelson, P. & Lovell, K. (2010). An evaluationof the impact of the recommendations of the Chief NursingOfficer’s (England) Review of Mental Health Nursing inMental Health Trusts and Universities in England: Findingsfrom stage one, an e-survey. Journal of Clinical Nursing, 19,2590–2600.
Björkman, T. T. M. (2008). Attitudes towards people withmental illness: A cross-sectional study among nursing staff inpsychiatric and somatic care. Scandinavian Journal of CaringSciences, 22, 170–177.
Charleston, R. & Happell, B. (2006). Recognising and reconcil-ing differences: Mental health nurses and nursing students’perceptions of the preceptorship relationship. The Austra-lian Journal Of Advanced Nursing, 24, 38–43.
Finn, C. P. (2001). Autonomy: An important componentfor nurses’ job satisfaction. International Journal of NursingStudies, 38, 349–357.
Graham, E. M. & Duffield, C. (2010). An ageing nursing work-force. Australian Health Review, 34, 44–48.
Graneheim, U. H. & Lundman, B. (2004). Qualitative contentanalysis in nursing research: Concepts, procedures and mea-sures to achieve trustworthiness. Nurse Education Today, 24,105–112.
Halter, M. J. (2008). Perceived characteristics of psychiatricnurses: Stigma by association. Archives of PsychiatricNursing, 22, 20–26.
Happell, B. (2001). Comprehensive nursing education in Victo-ria: Rhetoric or reality? Journal of Psychiatric and MentalHealth Nursing, 8, 507–516.
Happell, B. & Gough, K. (2007). Undergraduate nursingstudents’ attitudes toward mental health nursing: Determin-ing the influencing factors. Contemporary Nurse, 25,72–81.
Hayes, B., Bonner, A. & Pryor, J. (2010). Factors contributing tonurse job satisfaction in the acute hospital setting: A reviewof recent literature. Journal of Nursing Management, 18,804–814.
Hayman-White, K. & Happell, B. (2005). Nursing students’attitudes toward mental health nursing and consumers:
STUDENT NURSES STILL NOT INTERESTED IN MH 7
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.
Psychometric properties of a self-report scale. Archives ofPsychiatric Nursing, 19, 184–193.
Holden, R. J. (1991). Responsibility and autonomous nursingpractice. Journal of Advanced Nursing, 16, 398–403.
Nadler-Moodie, M. & Loucks, J. (2011). The implementation ofa new-graduate nurse residency training program directlyinto psychiatric-mental health nursing. Archives of Psychiat-ric Nursing, 25, 479–484.
Ng, S., Kessler, L., Srivastava, R. et al. (2010). Growing practicespecialists in mental health: Addressing stigma and recruit-ment with a nursing residency program. Nursing Leadership(Toronto, Ont.), 23 Spec No 2010, 101–112.
Pickens, J. M. & Fargotstein, B. P. (2006). Preceptorship: Ashared journey between practice & education. Journal ofPsychosocial Nursing & Mental Health Services, 44, 31.
Ross, C. A. & Goldner, E. M. (2009). Stigma, negative attitudesand discrimination towards mental illness within the nursingprofession: A review of the literature. Journal of Psychiatricand Mental Health Nursing, 16, 558–567.
Stevens, J. & Crouch, M. (1995). Who cares about care innursing education? International Journal of Nursing Studies,32, 233–242.
Stevens, J. & Dulhunty, G. (1992). New South Wales nursingstudents’ attitudes towards a career in mental health. Aus-tralian Journal of Mental Health Nursing, 2, 59–64.
Stevens, J. A. & Dulhunty, G. (1997). A career with mentallyill people: An unlikely destination for graduates of pre-registration nursing programs. The Australian ElectronicJournal of Nursing Education, 3, 128–138.
Ward, C., Bosco, A. & Styles, I. (2003). Student nurses’ perceivedgoals and future career pathways within nursing: Are theyrealistic? Australian Journal of Advanced Nursing, 20, 37–42.
Whitehead, E., Mason, T. & Ellis, J. (2007). The future ofnursing: Career choices in potential student nurses. BritishJournal of Nursing (BJN), 16, 491–496.
Willis, E. (1993). Nurses and independent fee-for-service prac-tice: A critical view. Contemporary Nurse, 2, 135–142.
World Health Organisation (1986). The Ottawa Charterfor Health Promotion. First International Conference onHealth Promotion, Ottawa 21 November 1986. Ottawa: WorldHealth Organisation.
World Health Organisation (1990). Report of a World HealthOrganization (WHO) meeting on consumer involvement inmental health services. (No. 0147-5622).
8 J. STEVENS ET AL.
© 2012 The AuthorsInternational Journal of Mental Health Nursing © 2012 Australian College of Mental Health Nurses Inc.





























