Embed Size (px)
Citation preview
ICU BEDSIDE TECHNOLOGY 07494704/00 $15.00 + .OO
CARDIOPULMONARY AND CEREBRAL RESUSCITATION
James E. Manning, MD, and Laurence M. Katz, MD
Over the past four decades, closed-chest cardiopulmonary resuscita- tion (CPR) and advanced cardiac life support (ACLS) interventions have saved many lives, but overall survival after cardiac arrest remains quite low, with survival rates of less than 5% reported in most studies?, l5 The poor survival rates can be attributed to one or more of the following factors: (1) use of aggressive resuscitative measures in patients with end- stage disease processes for whom even optimal resuscitative efforts are unlikely to prove successful, (2) delays in initiation of effective therapies within the critical therapeutic window, and (3) ineffective or suboptimal therapeutic interventions. The first factor is complex and involves clini- cal judgment, advanced directives, medicolegal concerns, and societal expectations that are beyond the scope of this article. The second factor is primarily a problem for out-of-hospital victims and for nonmonitored in-hospital patients. The third factor is an ongoing challenge for the resuscitation research community.
Resuscitative interventions can be classified as electrical therapy, artificial ventilation, artificial perfusion, or pharmacologic therapies. Al- though advances continue to be made in the areas of electrical therapy and artificial ventilation, presently available interventions are highly effective if they can be initiated in a timely manner. Thus, electrical therapy and artificial ventilation are usually not the limiting factors in a resuscitation. Pharmacologic agents given during cardiac arrest are primarily directed toward reversing the adverse effects of tissue hypo- perfusion. The principal therapeutic effect of vasoconstrictor agents,
From the Departments of Emergency Medicine OEM, LMK), Surgery OEM) and Anesthesi- ology (JEM), University of North Carolina School of Medicine, Chapel Hill, North Car- olina
CRITICAL CARE CLINICS
VOLUME 16 NUMBER 4 OCTOBER 2000 659
660 MANNlNG & KATZ
traditionally epinephrine, is to restore peripheral arterial resistance to improve blood flow generated by closed-chest CPR.29, 38 The contribu- tions of adrenergic agents and other drugs to improving survival from cardiac arrest have not been clearly demonstrated.
Artificial perfusion is the principal weak link in the resuscitation armamentarium. Closed-chest CPR has been shown to generate blood flow equivalent to about 25% to 33% of normal cardiac output under optimal condition^.^, l3 If there is any time delay before the initiation of CPR, as commonly occurs, the progressive loss of peripheral arterial resistance substantially decreases the blood flow generated by CPR, even if performed well te~hnically.~~ Thus, one of the greatest challenges in the development of better resuscitative interventions is to develop more effective methods of artificial perfusion support that can be initiated within the criticial time window allowing for return of spontaneous circulation (ROSC) with good neurologic recovery. Therefore, interven- tions to improve vital organ perfusion during cardiac arrest are the major focus of this article.
Although significant underlying disease is prevalent in the general population of patients suffering cardiac arrest, this is especially true for patients in the intensive care unit setting. Myocardial dysfunction, pulmonary disease, metabolic disturbances, and sepsis only serve to complicate the task of the intensivist who is attempting to resuscitate patients in cardiac arrest. The monitoring sophistication of the ICU provides for early recognition of lethal dysrhythmias or other acute cardiovascular decompensation events. Also, patients in the ICU fre- quently have monitoring parameters available that can be used to guide the resuscitation. These parameters include arterial pressure, central venous pressure, central venous oximetry, and end-tidal carbon dioxide. This article discusses how these parameters can be used to optimize CPR techniques and to assess the effect of pharmacologic agents admin- istered.
MONITORING AND ASSESSMENT DURING RESUSCITATION
Interventions in the ACLS treatment algorithms are guided by the electrocardiogram (ECG) rhythm present. Unfortunately, the ECG offers very limited information regarding vital organ perfusion and does not allow for effective mechanical adjustments in closed-chest CPR or titra- tion of drug therapy to allow optimal resuscitation outcome. Capnome- try and hernodynamic monitoring, commonly used in the critical care setting, provide useful information about organ perfusion and can be used to adjust therapeutic interventions on an individual basis.
Arterial Pressure Monitoring. The presence of an arterial line in a patient who is experiencing cardiac arrest can provide valuable informa- tion about the effectiveness of CPR and a means of obtaining serial blood gas values. The peak arterial pressure generated by the chest
CARDIOPULMONARY AND CEREBRAL RESUSCITATION 661
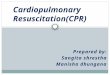
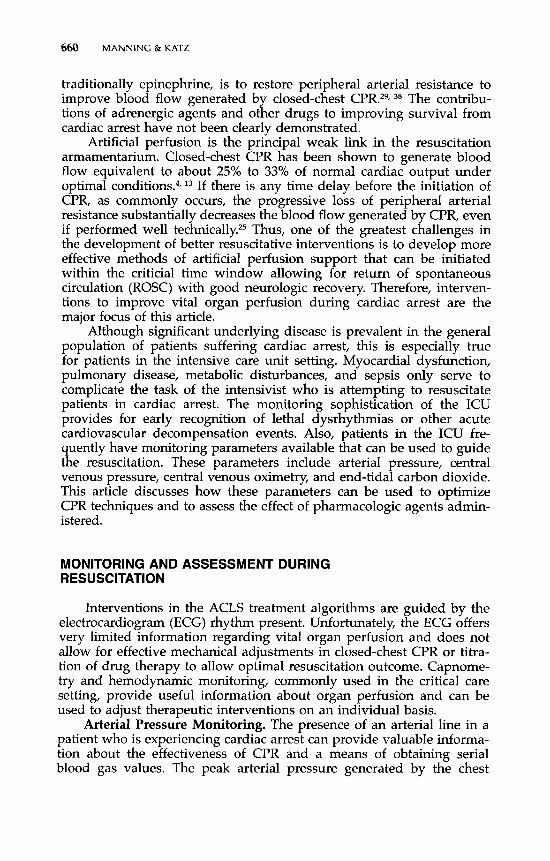
compressions is not the most important factor, because the central ve- nous pressure during chest compression is nearly equivalent to the arterial pressure, yielding little or no pressure gradient to generate blood flow. The most useful arterial pressure information during closed-chest CPR is the pressure during the relaxation phase of chest compressions, also called the CPR-diastolic arterial pressure (Fig. 1). Depending on the systemic arterial resistance, the CPR-diastolic arterial pressure can be greater than the central venous pressure, providing a gradient to drive tissue perfusion. Thus, the CPR-diastolic arterial pressure is the principal factor determining perfusion of the heart during resuscitation. Without knowing the central venous pressure, the minimum arterial pressure required for ROSC cannot be defined; however, laboratory studies have shown that a CPR-diastolic arterial pressure of greater than 30 mm Hg is usually needed to achieve ROSC.4O, By observing the arterial pres- sure, the force and rate of CPR compressions can be adjusted with the objective being to generate the highest possible CPR-diastolic arterial pressure. The frequency and dosage of administration of vasoconstrictor agents also can be guided by the arterial pressure response. If the arterial catheter is in the aorta, such as a cardiac arrest in the cardiac catheterization laboratory, the vasoconstrictor agent could be adminis- tered in small frequent doses directly into the arterial system. Laboratory investigation has shown intraaortic epinephrine administration to be more effective than central venous epinephrine admini~tration.3~ Arterial pressure monitoring also allows for detecting early signs of ROSC be-
' j . .
. . :
. . . . . j . . . . . .
. . . . . . . .
. . . . . .
. . . . . . .
&
. . . j 4
. . . . . . .
. _ . . I g
n/w 1 le:!
. . . . . . .
. . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . .
. . . . . . . . . .
. . . . . . . . . . . . . : . . . . : . . . . . . . . . . . . . . . -.
~ . . . . . .
. . . . . . .
. . : . .
. . . : . . .
Figure 1. Central arterial pressure tracing in a patient during closed-chest manual CPR. The arterial pressure during chest compressions (CPR-systole) is about 130 mm Hg. The arterial pressure during the relaxation phase of chest compression (CPR-diastole) averages about 20 mm Hg. This CPR-diastolic arterial pressure is the principal determinant of myocardial perfusion during closed-chest CPR. Adjustments in force and rate of CPR and in vasoconstrictor therapy should be made to maximize the CPR-diastolic arterial pressure.
662 MANNING & KATZ
cause intrinsic arterial pressure fluctuations often are seen before palpa- ble pulses become detectable.
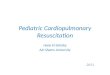
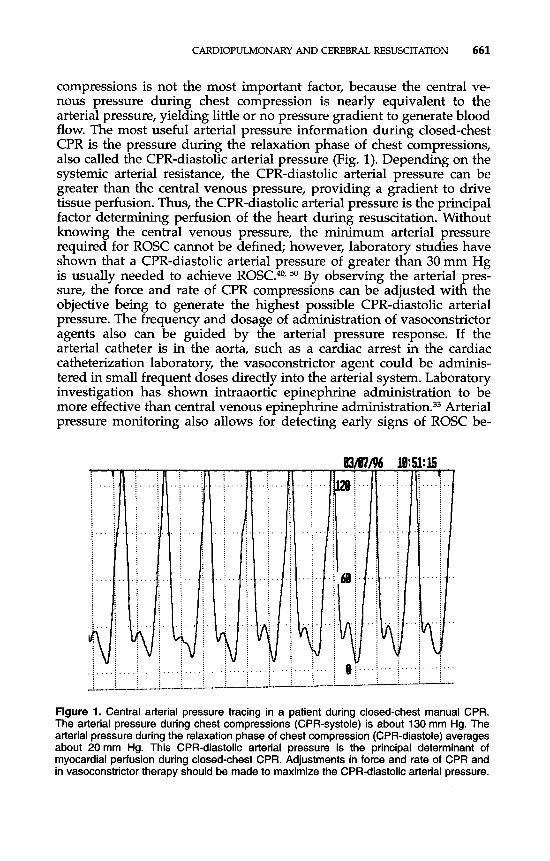
Coronary Perfusion Pressure Monitoring. The presence of both arterial and central venous catheters allows for quick calculation of the arterial-to-venous pressure gradient during CPR. Myocardial perfusion during closed-chest CPR is directly related to this coronary perfusion pressure (CPP) gradient, which is defined as the aortic pressure minus the right atrial pressure during the CPR-diastolic phase3" 41 (Fig. 2). The CPP gradient is principally determined by the arterial pressure gener- ated by closed-chest CPR, which is in turn primarily affected by CPR technique and peripheral arterial vasomotor tone. Laboratory and clini- cal data have both shown that a minimum CPP gradient of 15 mm Hg is generally required to achieve ROSC.", 51 The higher the CPP gradient, the greater the prospects of ROSC. Not unexpectedly, clinical studies have shown that CPP gradients generated by standard CPR in humans are usually less than this minimum.
If invasive pressure catheters are present, they should be used to guide the resuscitation. If such catheters are not in place, the insertion of such catheters is at the judgment of the intensivist. The authors have inserted central arterial and venous catheters by way of the femoral blood vessels in the emergency department and in the prehospital setting to guide resu~citation.~~ The time required to insert these lines has
!pqLE . . . . . . . . . . . . . . . 1: . . [ . . . . . . . . . . . . . . . . . . . . . . . . . . . . .I\; . . . : . . . j . . . . . . . . 1'1; ; 1. I. .y:\ . .
. . . . . . . . . . . . . . 1 ; j i 1; ; ; : . . . . . . . . . . . . . . .
Figure 2. Central arterial and venous pressure tracings in a patient during closed-chest manual CPR allow for estimation of CPP. The pressure scale on the tracing has been adjusted to focus on the relaxation phase of chest compression (CPR-diastole). CPP is equal to the central arterial pressure minus the central venous pressure during CPR- diastole. Adjustments in the force and rate of CPR and in vasoconstrictor therapy should be made to maximize the CPP. A CPP of at least 15 mm Hg is generally required to achieve return of spontaneous circulation. In this example, the CPP is approximately 30 mm Hg, and the patient was successfully resuscitated.
CARDIOPULMONARY AND CEREBRAL RESUSCITATION 663
generally been less than 5 minutes. Thus, if resuscitative efforts in a patient in the critical care unit setting are likely to be sustained for more than 5 to 10 minutes, the intensivist might consider the insertion of a femoral arterial catheter and possibly a femoral venous catheter to help guide therapy.
End-Tidal Carbon Dioxide. Capnometry has become a widely avail- able and standard tool for the assessment of endotracheal tube place- ment and monitoring of ventilation. Although cardiac arrest is a clinical scenario in which the accuracy of capnometry is suboptimal for these purposes, the use of capnometry during cardiac arrest nonetheless offers valuable information. Assuming that carbon dioxide production and pulmonary diffusion do not remarkably change during cardiac arrest, end-tidal carbon dioxide (ETCO,) correlates with pulmonary perfusion as long as minute ventilation is held constant. Pulmonary blood flow correlates with systemic blood flow, so ETCO, reflects vital organ perfu- sion during CPR.17, l8 This information makes semiquantitative colorimet- ric and quantitative digital capnometers useful monitoring devices dur- ing resuscitation. If during resuscitation ETCO, is undetectable or very low, either the endotracheal tube is not in the tracheobronchial tree or there is essentially no blood flow being generated by CPR. If endotra- cheal tube placement can be confirmed by other methods, the ETCO, readings indicate that adjustments in CPR must be made to improve perfusion.
Laboratory studies have demonstrated a correlation between ETCO, and CPP during closed-chest CPR.6, Thus, ETCO, can serve as a noninva- sive indicator of the effectiveness of CPR and can be used to adjust CPR technique to allow optimal vital organ perfusion. In one clinical study, 90% of patients with an initial ETCO, of 2 15mm Hg had ROSC, whereas patients with an ETCO, of < 15 mm Hg almost never achieved ROSC.9 ETCO, readings do not always correlate precisely with CPP, and the relationship between the two can be affected by pharmacologic agents. Adrenergic agents have been shown to decrease ETCO, despite improvements in CPP.37 Bicarbonate administration will increase the ETCO, transiently during CPR without changing organ perfusion. De- spite these limitations, ETCO, is the most accurate noninvasive indicator of CPR effectiveness currently available. With minute ventilation held relatively constant, adjustments in CPR technique can be made to max- imize the ETCO, and chance of ROSC.
Central Venous Oxygen Saturation Monitoring. Central venous oxygen saturation has been shown to be useful in assessing tissue oxygenation during resuscitation. Low central venous oxygen saturation indicates severe oxygen delivery/ consumption imbalance with high oxy- gen extraction ratios and poor resuscitation success, whereas higher central venous oxygen saturations are associated with lower oxygen extraction ratios and a higher rate of ROSC. In one clinical study of patients in cardiac arrest a central venous oxygen saturation of less than 30% resulted in a 0% ROSC rate, whereas a value greater than 72% resulted in a 100% ROSC Thus, resuscitative interventions can be
664 MANNING & KATZ
adjusted to maximize the central venous oxygen saturation if this param- eter is available, such as in patients with an oximetric pulmonary artery catheter in place.
Median Frequency of Ventricular Fibrillation. It has long been recognized that the coarseness of the ventricular fibrillation (VF) wave- form has a rough correlation with defibrillation success. However, quan- tifying this observation in a way that could potentially be used to make therapeutic decisions during resuscitation has been relatively recent. The use of mathematical formulas to rapidly analyze the power spectrum of the VF waveform has yielded a quantitative parameter, the median frequency, that has been found to correlate with the duration of cardiac arrest and the prospects for successful defibrillation:, l4 As the duration of VF increases the median frequency of the VF waveform decreases; however, resuscitative measures that improve myocardial perfusion re- sult in increase in median frequency. It further appears that the median frequency can be used to predict the likelihood of successful defibrilla- tion. Thus, median frequency could allow for adjustments in CPR, medi- cations, and the timing of defibrillation attempts. Monitor-defibrillator devices of the future will likely incorporate the technology needed to measure median frequency of the VF waveform.
NONINVASIVE ARTIFICIAL PERFUSION TECHNIQUES
Research has sought to find more effective methods for performing closed-chest CPR in the hopes of improving resuscitation outcome. These methods are generally based on the two prevailing theories for the mechanism of blood flow during chest compression. The cardiac pump theory proposes that compression of the heart is the principal reason for blood flow during CPR. The thoracic pump theory proposes that pressurization of the entire thorax, not just the heart, is responsible for blood flow. Most likely, both mechanisms are involved in promoting perfusion during CPR and the relative contribution of each probably varies on an individual basis. Because of this individual variation, the decision to try any of these alternative techniques is arbitrary unless some method of assessing perfusion is used to determine which alterna- tive technique is most effective.
High-Impulse CPR. Laboratory investigations using faster chest compression rates (100 min-' and 150 min-') showed increased cardiac output compared with a compression rate of 60mi1--'.~~ The impact force required to perform these rapid CPR compression rates led to the term high-impulse CPR. Proponents argued that the observed improve- ments supported the cardiac pump mechanism of blood flow. Although this method influenced the present recommendations for the rate of CPR chest compressions (increased from 60 min-' to 80 min-' to 100 -'), survival studies have not been done to clarify the effect of higher compression rates.
Active Compression-Decompression CPR. Standard CPR involves
CARDIOPULMONARY AND CEREBRAL RESUSCITATION 665
a forceful or active chest compression phase with elastic recoil of the chest wall during the relaxation phase (passive decompression). Active compression-decompression (ACD-CPR) involves both active compres- sion and active decompression of the thorax using a device that consists of a circular suction cup with a handle and force guage that is applied to the midsternal chest.” Laboratory evidence has shown that ACD-CPR can decrease the venous system pressure to a greater extent than the arterial pressures during the active decompression phase, resulting in improved venous return and increased CPR-diastolic CPP gradient. Some early clinical reports showed improvement in ROSC and survival, but a large randomized clinical trial in in-hospital and out-of-hospital cardiac arrest patients showed no improvement in survival with use of the ACD-CPR device compared with standard CPR? Thus, the clinical benefit of ACD-CPR remains unclear. As with all alternative CPR tech- niques, ACD-CPR can be an option if an ACD-CPR device is available and standard CPR has been unsuccessful.
Interposed Abdominal Compression CPR. The use of abdominal compressions in CPR evolved from the hypothesis that venous return might be improved and from laboratory observations that compression of the abdomen during cardiac arrest resulted in aortic pressure fluctua- tions similar to those seen with CPR chest compressions. This led to interposed abdominal compression CPR (IAC-CPR) in the hopes of increasing both the CPR-diastolic arterial pressure and central venous return from the abdomen. IAC-CPR involves one person performing CPR chest compressions while another person performs abdominal com- pressions during the relaxation phase of chest compressions. Although laboratory investigations have not yielded consistent findings, some studies have demonstrated increased coronary perfusion pressure and cardiac output. Results of clinical studies of IAC-CPR have not been consistent, but some studies have reported significant improvements in ROSC and survival to hospital Although there are not suffi- cient data to recommend IAC-CPR over standard CPR with chest com- pression alone, the use of IAC-CPR is a reasonable alternative to try if standard CPR is ineffective, especially if there is some means of assessing perfusion such as with hemodynamic monitoring or capnometry.
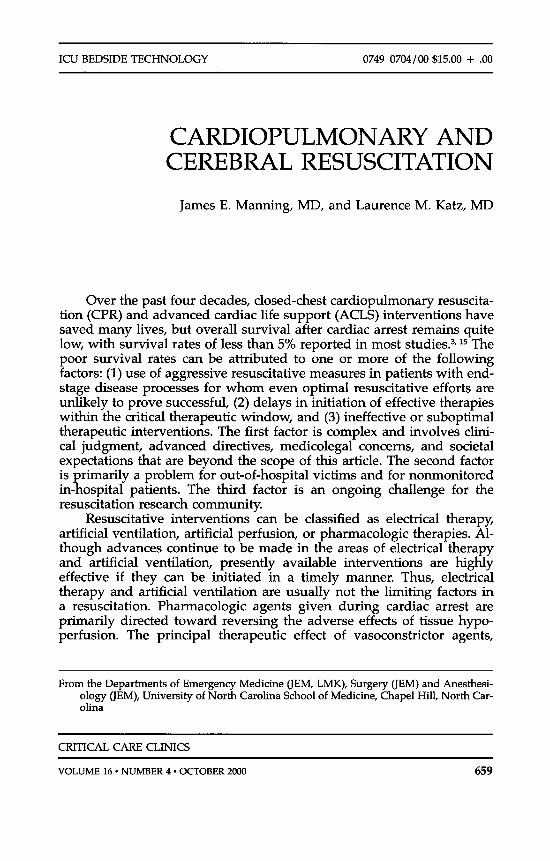
Phased Chest and Abdominal Compression-Decompression. Re- cently, a device called the Lifestick resuscitator (Datascope Corporation, Fairfield, NJ) that combines the concepts of IAC-CPR and ACD-CPR has been des~r ibed .~~ The device has adhesive chest and abdominal pads that are connected to an adjustable rigid frame with a handle at each end (Fig. 3). The chest and abdomen are compressed in an alternating pattern by a single operator in a seesaw manner. Laboratory study has shown improved CPP, ROSC, and &hour survival with this phased chest and abdominal compression-decompression technique. Clinical studies are needed to assess this new device further.
Circumferential Thoracic-Vest CPR. Based on the thoracic pump theory of CPR blood flow previously noted, the idea emerged of com- pressing the entire chest over a broad area rather than simply by sternal
666 MANNING & KATZ
B
A
Figure 3. Representative analog record of a control animal and a Lifestick-treated animal after 5 min of untreated VF. CPP, aortic pressure (AP) and PETCO, are shown at 3 min after start of compression. Arrow labeled A indicates onset of chest compression and abdominal decompression. Arrow labeled B indicates onset of chest decompres- sion and abdominal compression. (From Tang W, Weil MH, Schock RB, et al: Phased chest and abdominal compression-decompression: A new option for cardiopulmonary resuscita- tion. Circulation 951 335-1 340, 1997; with permission.)
depression. This idea led to the concept of a vest CPR device to create optimal intrathoracic pressure fluctuations by pressurizing the thorax from all directions (Fig. 4). Halperin and colleague^'^ reported improve- ments in CPP and ROSC using a circumferential thoracic vest CPR device in humans who had failed to respond to initial standard CPR.19 Of 34 patients randomized in their study 8 of 17 patients (47%) in the vest CPR group had ROSC compared with 3 of 17 patients (18%) who continued to receive standard manual CPR. If further clinical studies show improved ROSC and survival, circumferential thoracic vest CPR devices may become available.
INVASIVE ARTIFICIAL PERFUSION METHODS
Invasive artifical perfusion to treat cardiac arrest is not a recent idea. Before the landmark description of ”closed chest cardiac massage”

CARDIOPULMONARY AND CEREBRAL RESUSCITATION 667
Vest CPR
compression
Manual CPR
comDression
Figure 4. A comparison of the thoracic-vest system for cardiopulmonary resuscitation (Vest CPR) with standard manual CPR. The vest contains a bladder that is inflated and deflated by the pneumatic system. Defibrillation can be accomplished during chest compression through the flat defibrillator electrodes (dashed circle) under the vest. The ECG can be recorded through the same electrodes. The lower panels show transverse sections of the midthorax during vest CPR and manual CPR. The thoracic size during chest relaxation is shown by the solid lines. The arrows indicate force applied to the thorax during chest compression. With vest inflation, there is a relatively uniform decrease in the dimensions of the thorax. With manual CPR, the sternum is displaced during compression (arrow) and the lateral thorax can bulge, thereby increasing thoracic volume and reducing the intratho- racic pressure generated during compression. (From Halperin HR, Tsitlik JE, Gelfand M, et al: A preliminary study of cardiopulmonary resuscitation by circumferential compression of the chest with use of a pneumatic vest. N Engl J Med 329:762-768, 1993; with permission.)
668 MANNING & KATZ
in 1960, the method for treating cardiac arrest was thoracotomy and “open chest cardiac massage.’’21 However, this technique had relatively limited use during the first half of this century. Over the past 20 years, invasive technologies have been developed or adapted for use in resusci- tation. Although less practical because of the equipment, technical skill, and time-critical availability required, the vital organ perfusion gener- ated by invasive perfusion techniques has been shown to be superior to standard closed-chest CPR in laboratory investigations. Most of these interventions also allow for continued perfusion support during the post-resuscitation phase. Invasive perfusion techniques, like all invasive procedures, have potential complications but the risks in the setting of cardiac arrest are outweighed by the potential benefits. Despite the practical challenges involved, invasive perfusion methods may offer the greatest hope for substantially improving survival from cardiac arrest.
Cardiopulmonary Bypass Support and Extracorporeal Membrane Oxygenation. Advances in technology have led to the development of portable cardiopulmonary bypass support (CPBS) and extracorporeal membrane oxygen (ECMO) devices that have been used for systemic perfusion in the resuscitation of cardiac arrest 6o Laboratory studies have demonstrated improved ROSC and neurologic recovery with CPBS compared with standard ACLS intervention^.^^ Several clini- cal reports have described the use of femorofemoral CPBS and ECMO in the treatment of cardiac arrest with variable results. Phillips and colleagues@ reported percutaneous CPBS in 21 patients with cardiac arrest who had undergone an average of 30 minutes of CPR before CPBS; all but one of the 21 patients achieved ROSC.@ Of the 17 patients with nontraumatic cardiac arrest, six (35%) survived to hospital dis- charge. Reichman and colleagues46 reported successful CPBS in 36 of 38 patients with cardiac arrest in whom standard care had failed. ROSC was achieved in 34 of 36 patients with six (17%) having long-term survival. Shawl and c011eagues~~ reported seven cardiac arrest patients in whom standard ACLS had failed and who underwent CPBS in a cardiac catheterization laboratory an average of 21 minutes after onset of cardiac Six of the seven patients regained consciousness and four (57%) had long-term survival. Data published from the Extracorpo- real Life Support Organization ECMO registry reported the use of ECMO for the treatment of 386 patients in cardiac arrest with a survival rate of 27%.* Overall, the long-term survival for victims of cardiac arrest undergoing CPBS or ECMO is higher than for most of the reported literature with standard ACLS. The very high success rate for achieving ROSC with CPBS and ECMO suggests that patients with correctable pathophysiological conditions are given an optimal chance to survive if perfusion support can be initiated rapidly. A major advantage of CPBS and ECMO over standard ACLS is the ability to provide continued systemic perfusion during the post-resuscitation phase when intrinsic cardiac function is usually inadequate and the risk of recurrent cardiac arrest is high. The ability to gradually withdraw perfusion support facilitates cardiovascular stability. The major challenge is the time re-
CARDIOPULMONARY AND CEREBRAL RESUSCITATION 669
quired to get the equipment and skilled personnel needed to the patient and to perform the procedures. Even under good conditions, the time required to perform vascular access and initiate perfusion support is about 10 to 15 minutes. Survival in the studies first noted has been predominantly in patients with cardiac arrest times less than about 30 minutes. Thus, to be effective in the cardiac resuscitation, a highly coordinated system must be in place to allow for rapid implementation.
Ventricular Assist Devices. Left ventricular assist devices (LVAD) have the potential for being used acutely in the setting of cardiac arrest. An example of a VAD that has been reported to treat cardiac arrest is the Hemopump5* (Fig. 5). This catheter-based temporary ventricular assist device consists of an axial flow pump component at the distal end of the catheter powered by an external motor by way of a flexible drive cable that runs the length of the catheter. The distal tip of the axial flow pump component is advanced from a femoral artery into the left ventri- cle. When in operation, forward blood flow is generated by blood enter- ing the axial flow pump component in the left ventricle and exiting in
Figure 5. The Hemopump positioned in the left ventricle. (From Schroder T, Hering JP, Uhlig P, et al: Efficiency of the left ventricle assist device Hemopump in cardiac fibrillation. Br J Anaesth 68536, 1992; with permission.)
670 MANNING & KATZ
the aortic arch. Laboratory investigation in a cardiac arrest model has demonstrated sustained mean arterial pressures of approximately 60 mm Hg and cardiac output averaged 2.3 L / min.52 The major difficulty with the use of this device in the setting of cardiac arrest is the ability to accurately and rapidly insert the catheter from a femoral artery to the left ventricle.
Aortic Balloon Catheter Perfusion Techniques. There is a growing interest in the use of thoracic aortic balloon occlusion catheters to pro- vide vital organ perfusion during cardiac arrest. Although the use of intra-aortic balloon pump (IABP) catheters is an established clinical intervention for the treatment of left ventricular dysfunction, the value of standard IABP therapy is limited in cardiac arrest. Laboratory studies have shown that IABP can increase CPP during closed-chest CPR, but the effect is not dramatic.16 The use of thoracic aortic balloon catheters to occlude the aorta and allow for infusion of resuscitation solutions selectively to the heart and brain has yielded promising results in labora- tory models of cardiac arrest.
The use of an ascending aortic arch balloon occlusion catheter to allow for intermittent isolated perfusion of the coronary arteries has been described by Tang et al.57 Laboratory studies using this technique have shown marked increases in coronary perfusion with intermittent balloon occlusion alone. Fluid infusion resulted in further increases in coronary artery perfusion that promoted ROSC. Despite the remarkable coronary perfusion generated by this technique, rapid insertion of the catheter to the ascending aortic arch during cardiac arrest poses a sig- nificant challenge because of the limited margin of error. Some imaging technology would almost certainly be required to confirm proper place- ment of the catheter tip before initiation of therapy. The time delays associated with this imaging may prove unacceptable.
The use of a descending aortic arch balloon occlusion catheter for the purpose of selectively perfusing the heart and brain also has been described. The technique, termed selective aortic arch perfusion (SAAP) by Manning and c011eagues~~ and selective aortic perfusion and oxygen- ation (SAPO) by Paradis and was developed specifically for the treatment of cardiac arrest. The catheter is inserted into a femoral artery and advanced into the thoracic aorta between the left subclavian artery and the diaphragm (Fig. 6). This flexibility in balloon placement should allow for appropriate insertion without the need for imaging. With the balloon inflated, the coronary and cerebral circulations are relatively isolated for perfusion with an oxygenated resuscitation fluid, such as a hemoglobin solution or fluorocarbon emulsion.31, 43 The resusci- tation fluid might contain pharmacologic agents to enhance ROSC and limit reperfusion injury. The ability to administer agents to combat reperfusion injury at the moment of or just before reperfusion may prove to be a significant advantage. The balloon is deflated once ROSC has occurred. The limitation of this technique is related to intravascular volume loading, which can lead to pulmonary congestion. The approach anticipated by the authors is that if ROSC is not achieved with infusion
CARDIOPULMONARY AND CEREBRAL RESUSCITATION 671
\‘
Figure 6. Positoning of the selective aortic arch perfusion balloon occlusion catheter at the end of the descending aortic arch through a femoral artery. Placement of the balloon at this level restricts flow to aortic arch vessels, including coronary arteries. (From Manning JE, Murphy CA, Hertz CM, et al: Selective aortic arch perfusion during cardiac arrest: A new resuscitation technique. Ann Emerg Med 21 :1058-1065, 1992; with permission.)
of the resuscitation fluid, simultaneous femoral venous catheterization could allow for limited cardiopulmonary bypass until ROSC and partial perfusion support during the post-resuscitation phase.
Direct Mechanical Ventricular Assistance. The direct mechanical ventricular assistance (DMVA) apparatus, developed by Anstadt, uses a cup-shaped device that fits around the ventricles and is held in place by a vacuum at the apex of the heart (Fig. 7). Cyclic positive and negative pressures are transmitted to a flexible diaphragm on the inner surface of the cup resulting in compression and reexpansion of the ventricles, respectively. Unlike open-chest manual cardiac compression of the heart,
672 MANNING & KATZ
Figure 7. DMVA drive system and cup. Note the device actuates the ventricular myocardium into systolic (right) and diastolic (left) configurations. (From Anstadt MP, Anstadt GL, Lowe JE: Direct mechanical ventricular actuation: A review. Resuscitation 21 :7-23, 1991 ; with permission.)
the negative pressure applied to the ventricles by the DMVA device actively enhances ventricular filling for the next compression phase. Several laboratory studies have investigated DMVA in cardiac arrest models. DMVA has been shown to generate higher arterial pressures and greater cardiac output than open-chest manual cardiac compression. This device has seen only very limited clinical use thus far. DMVA is highly effective but the need for a thoracotomy makes this technology less attractive than some of the other less invasive techniques. However, one potentially important advantage of DMVA is that it can provide perfusion support for an extended time period without the need for anticoagulation.
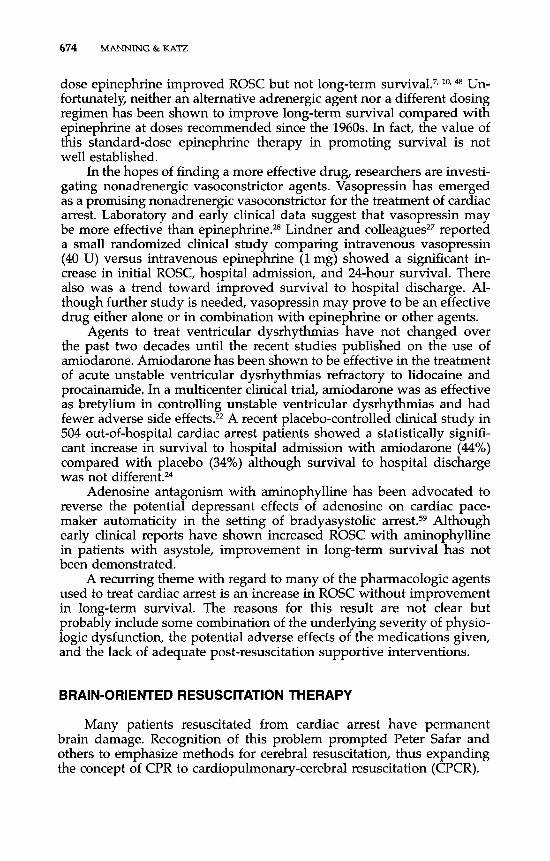
Minimally Invasive Direct Cardiac Massage. Buckman and col- leagues8 have reported a relatively simple device for the rapid initiation of internal cardiac compression without the need for the large lateral thoracotomy required for open-chest manual cardiac massage. The de- vice used is a padded plate connected to a handle that is inserted through an intercostal incision at the anterolateral left chest at the level of the lower sternum (Fig. 8). In a swine model of cardiac arrest, this technique generated CPP and cardiac output similar to those produced by manual open-chest cardiac massage. The device that is presently being studied could potentially be inserted by way of a small (2 to 3 cm) intercostal incision. The advantages of this technique are that the device is relatively simple and can be inserted very quickly.
CARDIOPULMONARY AND CEREBRAL RESUSCITATION 673
Figure 8. The heart-contracting baseplate and a portion of the stem of the cardiac compres- sive device are inserted into the thorax through a small, parasternal incision. The manually operated handle remains outside the chest. The baseplate is positioned directly on the cardiac ventricles, lying within an intact pericardium. Manual decompression of the device compresses the heart and produces an artificial systole. (From Buckman RF Jr, Badellino MM, Mauro LH, et al: Direct cardiac massage without major thoracotomy: Feasibility and systemic blood flow. Resuscitation 29:237-248, 1995; with permission.)
ASPECTS OF PHARMACOLOGIC THERAPY
Adrenergic agents, antidysrhythmic agents, and agents to treat aci- dosis constitute the principal pharmacologic therapies for cardiac arrest promulgated by ACLS guidelines over the past 30 years. Recent research has looked at other potential agents, such as adenosine antagonists, magnesium, nonadrenergic vasoconstrictors, and alternative agents for reversing metabolic acidosis. Probably the most important pharmaco- logic frontier for future resuscitation research is in limiting and reversing cellular, especially neuronal, damage associated with ischemia and reper- fusion.
The adrenergic agent epinephrine has been the principal resuscita- tion drug for all types of cardiac arrest. The primary beneficial effect of adrenergic agents in cardiac resuscitation has been shown to be alpha- adrenergic receptor-mediated vasoconstriction.29~ 38, Increases in the peripheral arterial resistance result in increased aortic pressure and, thus, increased coronary perfusion pressure generated by closed-chest CPR. Thus, epinephrine is given to improve artificial vital organ perfusion. Its beta-adrenergic cardiac effects have not been shown to be important during cardiac arrest. There has been an enormous amount of research on adrenergic therapy in an effort to find the optimal agent and most effective dosage to treat cardiac arrest. Clinical trials showed that high-
674 MANNING & KATZ
dose epinephrine improved ROSC but not long-term s~rvival.~, *Or 48 Un- fortunately, neither an alternative adrenergic agent nor a different dosing regimen has been shown to improve long-term survival compared with epinephrine at doses recommended since the 1960s. In fact, the value of this standard-dose epinephrine therapy in promoting survival is not well established.
In the hopes of finding a more effective drug, researchers are investi- gating nonadrenergic vasoconstrictor agents. Vasopressin has emerged as a promising nonadrenergic vasoconstrictor for the treatment of cardiac arrest. Laboratory and early clinical data suggest that vasopressin may be more effective than epinephrine.28 Lindner and reported a small randomized clinical study comparing intravenous vasopressin (40 U) versus intravenous epinephrine (1 mg) showed a significant in- crease in initial ROSC, hospital admission, and 24-hour survival. There also was a trend toward improved survival to hospital discharge. Al- though further study is needed, vasopressin may prove to be an effective drug either alone or in combination with epinephrine or other agents.
Agents to treat ventricular dysrhythmias have not changed over the past two decades until the recent studies published on the use of amiodarone. Amiodarone has been shown to be effective in the treatment of acute unstable ventricular dysrhythmias refractory to lidocaine and procainamide. In a multicenter clinical trial, amiodarone was as effective as bretylium in controlling unstable ventricular dysrhythmias and had fewer adverse side effects.22 A recent placebo-controlled clinical study in 504 out-of-hospital cardiac arrest patients showed a statistically signifi- cant increase in survival to hospital admission with amiodarone (44%) compared with placebo (34%) although survival to hospital discharge was not different."
Adenosine antagonism with aminophylline has been advocated to reverse the potential depressant effects of adenosine on cardiac pace- maker automaticity in the setting of bradyasystolic Although early clinical reports have shown increased ROSC with aminophylline in patients with asystole, improvement in long-term survival has not been demonstrated.
A recurring theme with regard to many of the pharmacologic agents used to treat cardiac arrest is an increase in ROSC without improvement in long-term survival. The reasons for this result are not clear but probably include some combination of the underlying severity of physio- logic dysfunction, the potential adverse effects of the medications given, and the lack of adequate post-resuscitation supportive interventions.
BRAIN-ORIENTED RESUSCITATION THERAPY
Many patients resuscitated from cardiac arrest have permanent brain damage. Recognition of this problem prompted Peter Safar and others to emphasize methods for cerebral resuscitation, thus expanding the concept of CPR to cardiopulmonary-cerebral resuscitation (CPCR).
CARDIOPULMONARY AND CEREBRAL RESUSCmATION 675
Disruption of blood flow to the brain for even a few minutes sets in motion a cascade of cellular derangements resulting in continued brain damage after the heart is restarted. These cascades appear to be triggered in part by energy depletion during cardiac arrest and circula- tion of oxygenated, acidotic blood during reperfusion. Reperfusion, al- though vital for reestablishing energy metabolism and cell viability, results in generation of free radicals, release of excitatory amino acids, and many other derangements at the cellular level. These abnormalities are collectively referred to as the reperfusion disease.39 There is a wide gap in the understanding of the relative importance and interactions of these pathways and how they cause the brain to die. This deficit of knowledge has severely hampered development of a robust brain ther- apy to treat cardiac arrest. Recent research suggests that cardiac arrest also may cause disruptions of brain function at the molecular level, resulting in erroneous expression of genes that program cells in the brain (and other organs) to commit suicide, a process known as a p ~ p t o s i s . ~ ~
There is evidence of ongoing brain damage for 48 to 72 hours after reperfusion from cardiac arrest. This phenomenon, referred to as delayed neuronal death, raises hope that resuscitative therapies (therapies begun after the cerebral insult begins) may be effective in attenuating brain damage caused by cardiac arrest.45 The limitation of most therapies currently being developed to reduce brain damage after cardiac arrest is that they affect a single pathway of the reperfusion syndrome. This strategy is scientifically more pure than combination therapy, but has not identified a magic bullet that can reverse all the cellular and molecular derangements that occur during cardiac arrest and reperfusion. Reperfu- sion injury is a multifactorial disease, so therapy directed at management of the most prominent mechanisms that lead to brain damage must be developed.
Mild (33°C to 35°C) resuscitative brain hypothermia currently holds the greatest promise for the treatment of brain damage associated with cardiac arrest because it attenuates most, if not all of the mechanisms of reperfusion injury. Nearly all preclinical trials of induced mild hypother- mia after cardiac arrest have shown some benefit in improving neuro- logic outcome. Small clinical trials suggest that cooling of the head early after resuscitation from cardiac arrest can improve neurologic outcome5; however, the full clinical potential of hypothermia has not been realized, because methods currently available to induce mild brain hypothermia are rather slow to achieve the therapeutic brain temperature. It appears that hypothermia must be induced rapidly and for prolonged periods to have its greatest impact on neurologic outcome.1z, 23 Methods to comfort- ably and safely maintain prolonged mild hypothermia in awake individ- uals require further development.
Combination therapies with blood flow promotion, toxin scaven- gers, hemodilution with a blood substitute, and hypothermia hold prom- ise in reducing brain damage after cardiac arrest.26, 35, % The challenge will be in developing practical methods to apply these therapies within the therapeutic window after resuscitation from cardiac arrest.
676 MANNING & KATZ
As resuscitation research progresses, it will raise new and challeng- ing ethical issues. The greatest challenges will be in determining who should receive the new technology and how it should be allocated. Hopefully advancements in the understanding of the pathophysiology of brain death from cardiac arrest will also identify clinical markers that can be used to determine who can benefit from the advancements in resuscitation therapies.
SUMMARY
The future of cardiopulmonary resuscitation lies in new technolo- gies for monitoring and generating vital organ perfusion during cardiac arrest and the post-resuscitation phase and in pharmacologic agents that will enhance ROSC and reverse ischemia-reperfusion injury. ROSC is the first step toward survival, so interventions that improve ROSC deserve further investigation. Long-term survival with good neurologic recovery is the critical endpoint. Interventions recommended for clinical practice must therefore demonstrate improved long-term survival. The resources required to provide many of the interventions discussed in this article, principally invasive perfusion technologies, cannot be justified unless there is clear benefit. The allocation of such resources to provide inten- sive resuscitation and post-resuscitation support will need to be ad- dressed from medical and societal viewpoints.
References
1. Anstadt ME Anstadt GL, Lowe JE: Direct mechanical ventricular actuation: A review. Resuscitation 21:7, 1991
2. Bartlett RH: Extracorporeal life support registry report 1995. American Society for Artificial Internal Organs Journal 43:107,1997
3. Becker LB, Ostrander ME Barrett J, et al: Outcome of CPR in a large metropolitan area: Where are the survivors. AM Emerg Med 20:355, 1991
4. Bellamy RF, DeGuzman LR, Pedersen DC: Coronary blood flow during cardiopulmo- nary resuscitation in swine. Circulation 69:174, 1984
5. Bernard S, Jones B, Home M: Clinical trial of induced hypothermia in comatose survivors of out-of-hospital cardiac arrest. Ann Emerg Med 30:146, 1997
6. Brown CG, Griffith R, Van Lighten F, et al: Median frequency: A new parameter for predicting defibrillation success rate. Ann Emerg Med 20:787, 1991
7. Brown CG, Martin DR, Pepe PE, et al: A comparison of standard-dose and high- dose epinephrine in cardiac arrest outside the hospital: The Multicenter High-dose Epinephrine Study Group. N Engl J Med 327:1051-1055, 1992
8. Buckman RF Jr, Badellino MM, Mauro LH, et al: Direct cardiac massage without major thoracotomy: Feasibility and systemic blood flow. Resuscitation 29:237, 1995
9. Callaham ML, Barton C W Prediction of outcome of cardiopulmonary resuscitation from end-tidal carbon dioxide concentration. Crit Care Med 18:358, 1990
10. Callaham M, Madsen CD, Barton CW, et al: A randomized clinical trial of high-dose epinephrine and norepinephrine vs. standard-dose epinephrine in prehospital cardiac arrest. JAMA 268:2667-2672, 1992
11. Cohen TJ, Tucker KJ, Lurie KG, et al: Active compression-decompression: A new method of cardiopulmonary resuscitation. JAMA 2672916, 1992
CARDIOPULMONARY AND CEREBRAL RESUSCITATION 677
12. Colboume F, Corbett D: Delayed postischemic hypothermia: A six-month survival study using behavioral and histological assessment of neuroprotection. J Neurosci 15:7250, 1995
13. Ditchey RV, Winkler JV, Rhoads C A Relative lack of coronary blood flow during closed-chest resuscitation in dogs. Circulation 66:297, 1982
14. Dzwonczyk R, Brown CG, Werman H A The median frequency of the ECG during ventricular fibrillation: Its use in an alogorithm for estimating the duration of cardiac arrest. IEEE Trans Biomed Eng 37640, 1990
15. Eisenberg MS, Honvood BT, Cummins RO, et a1 Cardiac arrest and resuscitation: A tale of 29 cities. Ann Emerg Med 19:179, 1990
16. Emerman CL, Pinchak AC, Hagen JF, et al: Hemodynamic effects of the intra-aortic balloon pump during experimental cardiac arrest. Am J Emerg Med 7378, 1989
17. Falk JL, Rackow EC, Weil MH: End-tidal carbon dioxide concentration during cardio- pulmonary resuscitation. N Engl J Med 318:607, 1988
18. Garnett AR, Omato JP, Gonzalez ER, et al: End-tidal carbon dioxide monitoring during cardiopulmonary resuscitation. JAMA 257512, 1987
19. Halperin HR, Tsitlik JE, Gelfand M, et al: A preliminary study of cardiopulmonary resuscitation by circumferential compression of the chest with use of a pneumatic vest. N Engl J Med 329:762, 1993
20. Kogure T, Kogure K Molecular and biochemical events within the brain subjected to cerebral ischemia (targets for therapeutic intervention). Clin Neurosci 4:179, 1997
21. Kowenhoven WB, Jude JR, Knickerbocker GG: Closed chest cardiac massage. JAMA 173:94, 1960
22. Kowey PR, Levine JH, Herre JM, et al, for the Intravenous Amiodarone Multicenter Investigators Group: Randomized, double-blinded comparison of intravenous amio- darone and bretylium in the treatment of patients with recurrent hemodynamically destabilizing ventricular tachycardia and fibrillation. Circulation 923255, 1995
23. Kuboyama K, Safar P, Radovsky A, et al: Delay in cooling negates the beneficial effect of mild resuscitative cerebral hypothermia after cardiac arrest in dogs: A prospective randomized study. Crit Care Med 21:1348, 1993
24. Kudenchuk PJ, Cobb LA, Copass MK, et al: Amiodarone for resuscitation after out-of- hospital cardiac arrest due to ventricular fibrillation. N Engl J Med 341:871, 1999
25. Lee SK, Vaagenes P, Safar P, et al: Effect of cardiac arrest time on cortical cerebral blood flow during subsequent standard external cardiopulmonary resuscitation in rabbits. Resuscitation 17105, 1989
26. Leonov Y, Sterz F, Safar P, et al: Hypertension with hemodilution prevents multifocal cerebral hypoperfusion after cardiac arrest in dogs. Stroke 23:45, 1992
27. Lindner KH, Dirks 8, Strohmenger HU, et al: Randomised comparison of epinephrine and vasopressin in patients with out-of-hospital ventricular fibrillation. Lancet 349:535, 1997
28. Lindner KH, Prengel AW, Pfenninger EG, et al: Vasopressin improves vital organ blood flow during closed-chest CPR in pigs. Circulation 91:215, 1995
29. Livesay JJ, Follette DM, Fey KH, et al: Optimizing myocardial supply/demand balance with alpha-adrenergic drugs during cardiopulmonary resuscitation. J Thorac Cardio- vasc Surg 76:244, 1978
30. Maier GW, Tyson GS, Olsen CO, et al: The physiology of external cardiac massage: High-impulse cardiopulmonary resuscitation. Circulation 70236, 1984
31. Manning JE, Batson DN, Payne FB, et al: Selective aortic arch perfusion during cardiac arrest: Enhanced resuscitation using oxygenated perflubron emulsion with and without aortic arch epinephrine. Ann Emerg Med 29:580, 1997
32. Manning JE, Mears GW, McCoy MC et al: Pre-hospital hemodynamic monitoring to guide cardiopulmonary resuscitation: Preliminaryc experience of a physician response system. Acad Emerg Med 2442, 1995
33. Manning JE, Murphy CA, Batson DN, et al: Aortic arch versus central venous epineph- rine during CPR. Ann Emerg Med 22703, 1993
34. Manning JE, Murphy CA, Hertz CM, et al: Selective aortic arch perfusion during cardiac arrest: A new resuscitation technique. Ann Emerg Med 21:1058-1065, 1992
678 MANNING & KATZ
35. Marion D, Leonov Y, Ginsberg M, et al: Resuscitative hypothermia. Crit Care Med 24(2 Suppl):S81, 1996
36. Martin GB, Carden DL, Nowak RM, et al: Aortic and right atrial pressures during standard and simultaneous compression and ventilation CPR in human beings. AM Emerg Med 15:125, 1986
37. Martin GB, Gentile N, Paradis NA, et al: Effect of epinephrine on end-tidal carbon dioxide monitoring during CPR. Ann Emerg Med 19:396, 1990
38. Michael JR, Guerci AD, Koehler RC, et al: Mechanisms by which epinephrine augments cerebral and myocardial perfusion during cardiopulmonary resuscitation in dogs. Circulation 69:822, 1984
39. Negovsky VA: Postresuscitation disease. Crit Care Med 16:942, 1988 40. Niemann JT, Criley JM, Rosborough JP, et al: Predictive indices of successful cardiac
resuscitation after prolonged arrest and experimental cardiopulmonary resuscitation. Ann Emerg Med 14:521, 1985
41. Niemann JT, Rosborough JP, Ung S, et al: Coronary perfusion pressure during experi- mental cardiopulmonary resuscitation. Ann Emerg Med 11:127, 1982
42. Paradis NA, Martin GB, Rivers EP, et al: Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary resuscitation. JAMA 263:1106,1990
43. Paradis NA, Rose MI, Gawryl MS Selective aortic perfusion and oxygenation: An effective adjunct to external chest compression-based cardiopulmonary resuscitation. J Am Coll Cardiol23:497-504, 1994
44. Phillips SJ, Zeff RH, Kongtahworn C, et al: Percutaneous cardiopulmonary bypass: Application and indication for use. Ann Thorac Surg 47121, 1989
45. Pulsinelli W, Brierley B, Plum F Temporal profile of neuronal damage in a model of transient forebrain ischemia. Ann Neurol 11:491, 1982
46. Reichman RT, Joy0 CI, Dembitsky WP, et al: Improved patient survival after cardiac arrest using a cardiopulmonary support system. Ann Thorac Surg 49:101, 1990
47. Rivers EP, Martin GB, Smithline H, et al: The clinical implications of continuous central venous oxygen saturation during human CPR. Ann Emerg Med 21:1094, 1992
48. Sack JB, Kesselbrenner MB: Hemodynamics, survival benefits, and complications of interposed abdominal compression during cardiopulmonary resuscitation. Acad Emerg Med 1:490, 1994
49. Safar P, Abramson NS, Angelos M, et al: Emergency cardiopulmonary bypass for resuscitation from prolonged cardiac arrest. Am J Emerg Med 8:55, 1990
50. Sanders AB, Ewy GA, Taft TV Prognostic and therapeutic importance of the aortic diastolic pressure in resuscitation from cardiac arrest. Crit Care Med 12:871, 1984
51. Sanders AB, Ogle M, Ewy GA: Coronary perfusion pressure during cardiopulmonary resuscitation. Am J Emerg Med 3:11, 1985
52. Schroder T, Hering JP, Uhlig P, et al: Efficiency of the left ventricle assist device Hemopump in cardiac fibrillation. Br J Anaesth 68:536, 1992
53. Shawl FA, Domanski MJ, Wish MH, et al: Emergency cardiopulmonary bypass support in patients with cardiac arrest in the catheterization laboratory. Catheter Cardiovasc Diag 19:8, 1990
54. Sterz F, Leonov Y, Safar P, et al: Hypertension with or without hemodilution after cardiac arrest in dogs. Stroke 21:1178, 1990
55. Stiell IG, Hebert PC, Weitzman BN, et al: High-dose epinephrine in adult cardiac arrest. N Engl J Med 3271045, 1992
56. Stiell IG, Hebert PC, Wells GA, et al: The Ontario trial of active compression-decom- pression cardiopulmonary resuscitation for in-hospital and prehospital cardiac arrest. JAMA 275:1417, 1996
57. Tang W, Weil MH, Noc M, et al: Augmented efficacy of external CPR by intermittent occlusion of the ascending aorta. Circulation 88:1916, 1993
58. Tang W, Weil MH, Schock RB, et al: Phased chest and abdominal compression- decompression: A new option for cardiopulmonary resuscitation. Circulation 95:1335, 1997
59. Viskin S, Belhassen B, Roth A, et al: Aminophylline for bradyasystolic cardiac arrest refractory to atropine and epinephrine. Ann Intern Med 118:279, 1993

CARDIOPULMONARY AND CEREBRAL RESUSCITATION 679
60. Von Segesser LK. Cardiopulmonary support and extracorporeal membrane oxygen-
61. Yakaitis RW, Otto CW, Blitt CD: Relative importance of alpha and beta adrenergic
62. Weil MH, Bisera J, Trevino RR, et al: Cardiac output and end-tidal carbon dioxide.
ation for cardiac assist. Ann Thorac Surg 68:672, 1999
receptors during resuscitation. Crit Care Med 7293-296, 1979
Crit Care Med 13907, 1985
Address reprint requests to James E. Manning, MD
Department of Emergency Medicine Campus Box 7594
Neurosciences Hospital, Ground Floor University of North Carolina School of Medicine
Chapel Hill, NC 27599-7594
e-mail: [email protected]