Embed Size (px)
Citation preview
Cardiac RehabilitationCardiac Rehabilitation
Paula O’NeillPaula O’NeillCHD Nurse SpecialistCHD Nurse Specialist
Hammersmith/Charing Cross HospitalsHammersmith/Charing Cross Hospitals
2424thth September 2008 September 2008
Learning ObjectivesLearning Objectives
Components of cardiac rehabilitationComponents of cardiac rehabilitation
What is cardiac rehabilitation?What is cardiac rehabilitation?
Structure of cardiac rehabilitationStructure of cardiac rehabilitation
Ways of delivering cardiac Ways of delivering cardiac rehabilitationrehabilitation
The future of cardiac rehabilitationThe future of cardiac rehabilitation

Definition of Definition of Cardiac RehabilitationCardiac Rehabilitation
““The sum of activities required to ensure The sum of activities required to ensure
patients the best possible physical, patients the best possible physical,
mental and social conditions so that mental and social conditions so that
they may resume and maintain as they may resume and maintain as
normal a place as possible in the normal a place as possible in the
community”.community”.World Health OrganisationWorld Health Organisation
The EvidenceThe Evidence
Comprehensive help with lifestyle Comprehensive help with lifestyle modification modification
involving education and involving education and psychological input aspsychological input as
well as exercise training can reduce well as exercise training can reduce mortality bymortality by
20-25% over 3 years.20-25% over 3 years.Oldridge et al 1988; O’Connor et al 1989Oldridge et al 1988; O’Connor et al 1989
Target GroupsTarget Groups
CoronaryCoronary heart disease (CHD) heart disease (CHD)– Exertional angina .Exertional angina .– ACS (unstable angina or NSTEMI or ACS (unstable angina or NSTEMI or
STEMI) following medical/surgical STEMI) following medical/surgical management.management.
– RevascularisationRevascularisation– Stable heart failure and cardiomyopathyStable heart failure and cardiomyopathy
Those at high risk of developing CVD: totalThose at high risk of developing CVD: totalCVD risk > 20% over 10 years or diabetes CVD risk > 20% over 10 years or diabetes mellitus.mellitus.

Who should be involved?Who should be involved?
Patient
PharmacistNurse
ConsultantGP
PhysiotherapyPhysiotherapy
Dietician
Exercise instructor
Smoking cessation advisor
Social Services
Psychologist
District Nurses
Practice nurses
Health Visitor
Secondary care

Components of CR.Components of CR.
Lifestyle:Lifestyle:– Diet and weight managementDiet and weight management– Smoking cessationSmoking cessation– Physical activity and exercisePhysical activity and exercise
– Secondary preventionSecondary prevention– EducationEducation
Psychosocial carePsychosocial care Long-term management strategyLong-term management strategy

Physical ActivityPhysical Activity
Assess and risk stratifyAssess and risk stratify Develop individual exercise planDevelop individual exercise plan Teach FITT principleTeach FITT principle Regain/develop physical fitnessRegain/develop physical fitness Regain confidence in physical Regain confidence in physical
activityactivity Develop long-term activity planDevelop long-term activity plan Self monitoringSelf monitoring
Secondary PreventionSecondary Prevention
Cholesterol managementCholesterol management
BP managementBP management
Blood sugar managementBlood sugar management
Cardio-protective drug therapyCardio-protective drug therapy

EducationEducation
CHD as a diseaseCHD as a disease
Treatment including medicationTreatment including medication
Recovery processRecovery process
CHD risk factorsCHD risk factors
Symptom managementSymptom management
Living with CHDLiving with CHD
Psychosocial CarePsychosocial Care
Reduce fear and anxietyReduce fear and anxiety
Assist with adjustmentAssist with adjustment
Promote positive attitudePromote positive attitude
Facilitate behaviour changeFacilitate behaviour change
Identify need for further supportIdentify need for further support
Structure of Structure of Cardiac RehabilitationCardiac Rehabilitation
Phase 1:Phase 1: In-patient (1In-patient (1stst contact) contact)
Phase 2:Phase 2: Immediate post dischargeImmediate post discharge
Phase 3:Phase 3: 2-4 weeks post discharge2-4 weeks post discharge
Phase 4:Phase 4: Long-term, on-goingLong-term, on-going
Phase 1Phase 1
Understanding of conditionUnderstanding of condition Information & educationInformation & education Risk factor assessmentRisk factor assessment Personalised health planPersonalised health plan Psychological assessment/supportPsychological assessment/support ReferralReferral Drug therapyDrug therapy
Phase 2Phase 2
Home visits.Home visits.
Telephone Telephone support.support.
ClinicsClinics
Phase 3Phase 3
Reassess health & risk factors first.Reassess health & risk factors first.
Health EducationHealth Education
ExerciseExercise
RelaxationRelaxation
Phase 4Phase 4
Maintenance of exercise/activityMaintenance of exercise/activity
On-going lifestyle supportOn-going lifestyle support
Challenges for the Pt and FamilyChallenges for the Pt and Family
Challenges for the Pt and Family
•Frightening, life threatening event (MI, major surgery)
•A chronic illness, reduced life expectancy, symptoms
•Altered identity - an invalid, walking time bomb
•Fears for family and partner being left alone
•Threat to employment and financial status
•Medication side effects (lethargy, impotence)
•Being treated differently by other people
•Neurological impairement (esp. cardiac arrest pats.)
•Making lifestyle changes, smoking, diet, activity

Delivering CRDelivering CR
Can be done individually or in a groupCan be done individually or in a group
Venue:Venue: HomeHome
CommunityCommunity
ClinicsClinics
Menu: Mixing up of all 4 phases too Menu: Mixing up of all 4 phases too provide an individualised package of provide an individualised package of care.care.
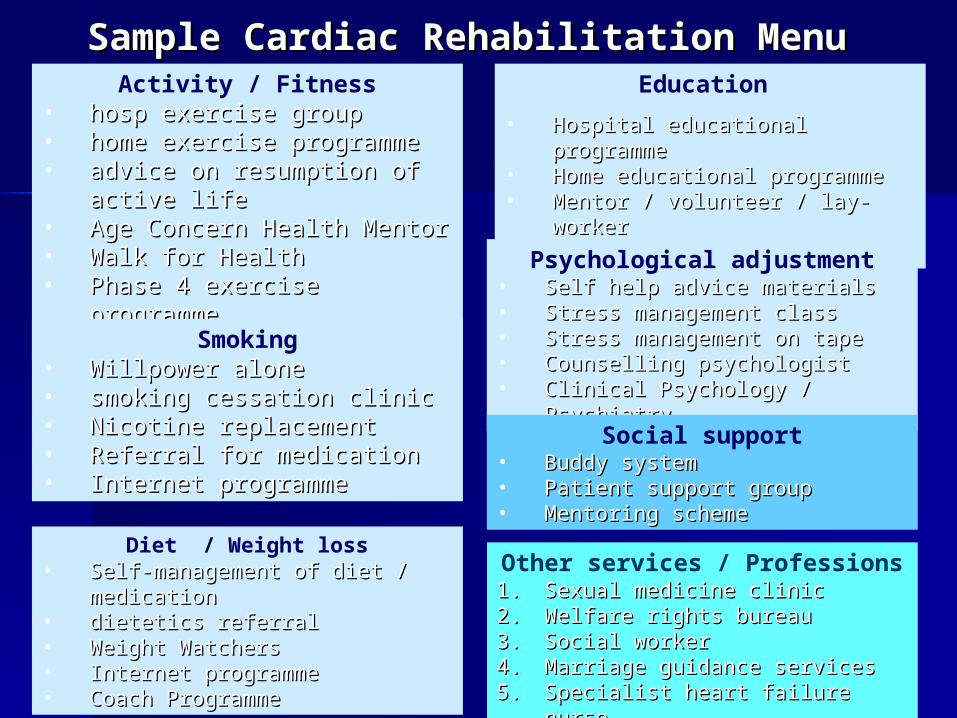
Other services / Professions1.1. Sexual medicine clinicSexual medicine clinic2.2. Welfare rights bureauWelfare rights bureau3.3. Social workerSocial worker4.4. Marriage guidance servicesMarriage guidance services5.5. Specialist heart failure nurseSpecialist heart failure nurse
Sample Cardiac Rehabilitation MenuSample Cardiac Rehabilitation MenuActivity / Fitness
• hosp exercise grouphosp exercise group• home exercise programmehome exercise programme• advice on resumption of active lifeadvice on resumption of active life• Age Concern Health MentorAge Concern Health Mentor• Walk for HealthWalk for Health• Phase 4 exercise programmePhase 4 exercise programme• Tai Chi classesTai Chi classes
Smoking• Willpower aloneWillpower alone• smoking cessation clinicsmoking cessation clinic• Nicotine replacementNicotine replacement• Referral for medicationReferral for medication• Internet programmeInternet programme
Diet / Weight loss• Self-management of diet / medicationSelf-management of diet / medication• dietetics referral dietetics referral • Weight WatchersWeight Watchers• Internet programmeInternet programme• Coach ProgrammeCoach Programme
Education
• Hospital educational programmeHospital educational programme• Home educational programmeHome educational programme• Mentor / volunteer / lay-workerMentor / volunteer / lay-worker• InternetInternet
Psychological adjustment• Self help advice materialsSelf help advice materials• Stress management classStress management class• Stress management on tapeStress management on tape• Counselling psychologistCounselling psychologist• Clinical Psychology / PsychiatryClinical Psychology / Psychiatry
Social support• Buddy systemBuddy system• Patient support groupPatient support group• Mentoring schemeMentoring scheme
Angina PlanAngina Plan
WHAT?WHAT?
Self help Self help packagepackage
A CBT A CBT programmeprogramme
WHO?WHO?
Recent anginaRecent angina
1 year since 1 year since diagnosisdiagnosis
www.anginaplan.org.uk
Using the Angina PlanUsing the Angina Plan
Advice tape & information sheetAdvice tape & information sheet
30 minute appointment30 minute appointment
4 phone calls over 3 months (5-10 4 phone calls over 3 months (5-10 mins)mins)
Pro & Cons of the Angina PlanPro & Cons of the Angina Plan
RestrictionsRestrictions
Must be literateMust be literate Must be motivatedMust be motivated CostCost Time commitmentTime commitment
Advantages (RCT)Advantages (RCT)
Less medicationLess medication Less GP/hospital visitsLess GP/hospital visits anxiety/depressionanxiety/depression MI treated quicklyMI treated quickly incidence of CHDincidence of CHDLewin R et al (2002) A Randomised controlled Lewin R et al (2002) A Randomised controlled
trial of a selftrial of a self
management plan for patients with newly management plan for patients with newly diagnosed angina.diagnosed angina.
British Journal of General Practice 52: 476, 194-British Journal of General Practice 52: 476, 194-201201

The Heart Manual The Heart Manual (1)(1)
6 week, home based post MI 6 week, home based post MI rehab programme rehab programme
A work book, diaries, record A work book, diaries, record sheets and information sheets and information
2 audio tapes, advice for 2 audio tapes, advice for family, a stress family, a stress management course on management course on tapetape
A specially trained A specially trained ‘Facilitator’‘Facilitator’

The Heart Manual The Heart Manual (2)(2)
Exercise programme – walkingExercise programme – walking
Secondary prevention – written adviceSecondary prevention – written advice
Cognitive behavioural techniquesCognitive behavioural techniquesChange patients Change patients beliefs and attributions beliefs and attributions
(cardiac (cardiac misconceptions) misconceptions) Self help for psychological problemsSelf help for psychological problemsRelaxation and stress managementRelaxation and stress management
Initial face-to-face session, then phone calls or Initial face-to-face session, then phone calls or home/clinic visits at week 1, 4, 6 after discharge.home/clinic visits at week 1, 4, 6 after discharge.
Multi-centred RCT of HM vs. Hospital based. Equal gain on all measures including 2 Met gain in fitness, HM
fewer readmissions. Andrew Coats, Jenny Bell
Initial RCT - less anxiety & depression: better quality of life: fewer readmissions to hospital: less contact with
GP. Lewin B, Lancet, 1992.
The Heart Manual: Evidence BaseThe Heart Manual: Evidence Base
Recommended by - WHO: BHF: Department of Health: Scottish Office

CHD NSFCHD NSF•By 2009 85% of MI and revasc patients will be offered cardiac rehabilitation
•After that all except unstable angina patients should receive CR.

The RealityThe Reality
25-30% of 25-30% of patientspatients
getting cardiacgetting cardiac
rehab in 2006-rehab in 2006-7.7.

ProblemsProblems
InequalitiesInequalities – women, poor, ethnic minorities, – women, poor, ethnic minorities, depressed, smokers, elderly, all believed to be depressed, smokers, elderly, all believed to be under-represented, postcode lotteryunder-represented, postcode lottery
Failure to invite all indicated in NSFFailure to invite all indicated in NSF – angina, – angina, heart failure, ICD, arrhythmiaheart failure, ICD, arrhythmia
DropoutDropout – varies widely from programme to – varies widely from programme to programmeprogramme
StaffingStaffing – from single-handed, part-time, – from single-handed, part-time, coordinator for 600 patients to a full multi-coordinator for 600 patients to a full multi-disciplinary team. Only 50% of programmes have disciplinary team. Only 50% of programmes have an identifiable budget.an identifiable budget.

Cost of Cardiac RehabilitationCost of Cardiac Rehabilitation
The average cost per patient in 2006-7 The average cost per patient in 2006-7 was £413 was £413
Single day in a CCU costs £1,400 Single day in a CCU costs £1,400
Angioplasty (does not reduce mortality) Angioplasty (does not reduce mortality) costs £3,000 costs £3,000
Bypass surgery costs £8,000. Bypass surgery costs £8,000.
Remember the Evidence!Remember the Evidence!
Comprehensive help with lifestyle modification Comprehensive help with lifestyle modification
involving education and psychological input asinvolving education and psychological input as
well as exercise training can reduce mortality well as exercise training can reduce mortality byby
20-25% over 3 years.20-25% over 3 years.
Oldridge et al 1988; Oldridge et al 1988; O’Connor et al 1989O’Connor et al 1989

Cardiac Rehabilitation Cardiac Rehabilitation Saves Lives!Saves Lives!
No treatment in cardiac disease has stronger No treatment in cardiac disease has stronger scientific evidence or a significantly greater impact scientific evidence or a significantly greater impact on survival.on survival.
The scientific evidence has been reviewed by many The scientific evidence has been reviewed by many scientific and expert bodies over the last 30 years. scientific and expert bodies over the last 30 years. Every review has come to the same conclusion that Every review has come to the same conclusion that cardiac rehabilitation is an essential treatment.cardiac rehabilitation is an essential treatment.
CR is only form of chronic disease management CR is only form of chronic disease management with an evidence base. with an evidence base.
The SolutionsThe Solutions
NACRNACR National CampaignNational Campaign NICE GuidelinesNICE Guidelines CR QoFCR QoF TariffsTariffs CDM AgendaCDM Agenda





























