Embed Size (px)
Citation preview

Journal of Equine Veterinary Science 33 (2013) 590-596
Journal of Equine Veterinary Science
journal homepage: www.j -evs.com
Original Research
Cardiac Arrhythmias in Standardbreds During and After RacingdPossibleAssociation Between Heart Size, Valvular Regurgitations,and Arrhythmias
Rikke Buhl DVM, PhD a, Ellen Ekkelund Petersen DVMa, Maria Lindholm DVMa,Lars Bak DVMa, Katarina Nostell DVM, PhD a,b
aDepartment of Large Animal Sciences, Large Animal Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Taastrup, DenmarkbDepartment of Clinical Sciences, Faculty of Veterinary Sciences, Swedish University of Agricultural Sciences, Uppsala, Sweden
a r t i c l e i n f o
Article history:Received 30 May 2012Received in revised form2 September 2012Accepted 19 September 2012Available online 13 November 2012
Keywords:HorseExerciseECGArrhythmiasEchocardiographyTroponin I
Corresponding author at: Rikke Buhl, DVM, PhD, DAnimal Sciences, Large Animal Medicine, Faculty of HSciences, University of Copenhagen, Agrovej 5,Denmark.
E-mail address: [email protected] (R. Buhl).
0737-0806/$ - see front matter � 2013 Elsevier Inc. Ahttp://dx.doi.org/10.1016/j.jevs.2012.09.009
a b s t r a c t
Cardiac arrhythmias during racing and in recovery period are limited in description, as isthe relationship between left ventricular size, valvular regurgitations, and arrhythmias.Therefore, the aim of this study was (i) to study development of supraventricular andventricular premature complexes (SVPCs and VPCs) during and after racing in trotters;(ii) to assess the associations between myocardial hypertrophy, valvular regurgitations,and arrhythmias during and after racing; and (iii) to estimate correlation between cardiacarrhythmias and the myocardial biomarker (cardiac troponin I [cTnI]). Clinically normaltrotters (N ¼ 26) were examined using echocardiography and electrocardiography. Leftventricular muscle mass relative to bodyweight (g/kg) was calculated, and valvularregurgitations were registered. ECG recordings were obtained at rest, during racing, andin recovery period. Blood samples were taken on three occasions: at rest, once just afterracing (15-60 minutes), and once between 12 and 14 hours after racing. During racing,50.0% of horses had one or more SVPCs, whereas 3.9% had one or more VPCs. Within therecovery period, 46.2% of horses showed one or more SVPCs, whereas 19.2% had VPCs.There was no significant association between occurrence of arrhythmias and heart size orpresence of valvular regurgitations. All horses had plasma cTnI concentrations of <0.022mg/L. In conclusion, a high number of horses showed SVPCs during racing and in therecovery period. Also, a moderate number of horses developed VPCs after racing. Thehigh number of arrhythmias was not related to heart size or increased cTnI and isprobably physiologically normal in origin.
� 2013 Elsevier Inc. All rights reserved.
1. Introduction Previously it has been suggested that arrhythmias
Cardiac arrhythmias play an important role amongcardiovascular causes of poor performance in horses [1],but research on the prevalence and significance of thesearrhythmias is limited [2-6], although a study in a largepopulation of trotters was published recently [7].
epartment of Largeealth and Medical
DK-2630 Taastrup,
ll rights reserved.
occurring during maximal intense exercise or immediatelyafter are of clinical importance and are a potential cause ofreduced performance [2]. Other researchers have arguedthat single and isolated arrhythmias can be seen in horseswithout clinical signs of disease or history of heart disease,but that frequent occurrence of supraventricular orventricular premature complexes (SVPCs and VPCs) duringand immediately after exercise is considered abnormal[8,9]. An electrocardiographic (ECG) study in clinical healthyThoroughbred racehorses showed that arrhythmias occurfrequently during training [3]. These authors, therefore,question whether arrhythmias during and immediately

R. Buhl et al. / Journal of Equine Veterinary Science 33 (2013) 590-596 591
after exercise always should be regarded as pathologic anda cause of poor performance. A recently published Cana-dian study showed that 27.8% of trotters developedventricular arrhythmias in the early recovery period afterracing, but the researchers did not observe arrhythmiaswhile the horses were actively racing [7].
It is well described in both equine and human athletesthat exercise-induced hypertrophy of both left and rightventricles occurda physiological phenomenon known as“Athlete’s heart” [10-15]. Exercise-induced cardiac hyper-trophy is characterized by a decreased afterload, which is incontrast to the hypertensive heart, characterized byincreased afterload. Therefore, the Athlete’s heart isconsidered more benign than the hypertensive heart.However, exercise-induced hypertrophy may also, like inthe hypertensive heart, result in ECG abnormalities withboth supra- and ventricular arrhythmias. Therefore, a morethorough knowledge and understanding of cardiac elec-trophysiology in athletes is essential to differentiate path-ological- from physiological-induced arrhythmias. Studiesin humans showed that exercise-induced cardiac hyper-trophy can be associated with various pathological condi-tions suchas cardiac arrhythmias andheartmuscle ischemia[16], which may substantially increase the risk of athletesdying during or after exercise [17-19]. The term “CardiacSudden Death” is used to describe a situation where other-wise healthy athletes suddenly die due to cardiovasculardisease [14,17,18,20,21]. At present, it is unknown whetherexercise-induced cardiac hypertrophy increases the risk ofdeveloping ventricular arrhythmias in the equine athlete.
Apart from cardiac hypertrophy, increased prevalence ofvalvular regurgitation is observed in equine athletes, prob-ably as a result of increased cardiac size [22,23]. Whetherthese mild regurgitations in athletes predispose for devel-opment of arrhythmias is unknown, but it can be speculatedthat mitral and tricuspid regurgitation may predispose forsupraventricular arrhythmias or atrial fibrillation [24-26].
Enlargement of cardiac muscle may lead to exercise-induced ischemia during intensive training [16,20].Ischemia results in cell death and fibrosis of the myocar-dium, which can trigger severe arrhythmias [20]. Cardiactroponin I (cTnI) is a polypeptide found specifically inmyocardium. Serum and plasma concentrations of thisprotein act as a diagnostic and prognostic indicator of heartdiseases in humans, dogs, and horses [27-30]. In somehorses, cTnI increases after exercise [31,32], but the asso-ciation between cTnI and exercise-induced arrhythmiashas never been investigated in horses.
The aim of this study was (i) to study development ofSVPCs and VPCs during racing and in the recovery period inclinically normal trotters; (ii) to assess the associationbetween myocardial hypertrophy, valvular regurgitations,and arrhythmias; and (iii) to examine whether horsesdeveloping arrhythmias have sign of myocardial damage,indicated by increased plasma cTnI concentrations.
2. Materials and Methods
2.1. Horses
Initially, 44 Standardbreds were included in the study.The horses were selected by two Swedish trainers.
Inclusion criteria were that the horses should be consid-ered clinically healthy, in racing condition, and ready forracing. Of these horses, 14 were excluded because theywere not racing within the study period (6 weeks), andfour horses were excluded owing to poor ECG qualitywhile racing. The quality of ECG was considered accept-able if distinct R waves were detected during the record-ings. Twenty-six horses with complete ECG andechocardiographic data were included in the study. Allhorses had cTnI measured 24 hours before racing, once 15-60 minutes after racing, and once 12-14 hours after racing.The horses were between 3 and 7 years of age (42.3%stallions, 38.5% geldings, and 19.2% mares). The mean bodyweight was estimated to be 510 � 34 kg. Registration oftraining amount was not attempted. The trainer gaveinformed consent for the study, and the study wasapproved by The Ethical Committee for Animal Experi-ment, Uppsala, Sweden (C216/8).
2.2. Methods
The horses underwent a clinical examination withspecific focus on the cardiovascular system. Bodytemperature, heart rate (HR), and respiratory rate wereregistered, and cardiac and pulmonary auscultation wascarried out. Horses were included with a normal clinicalexamination and with cardiac murmurs �grade III out ofVI and no pathological arrhythmias during auscultation orresting ECG. The bodyweight was estimated by measuringchest girth.
2.2.1. EchocardiographyHeart size was measured by standard two-dimensional
and M-mode echocardiography as previously described[13]. Three nonconsecutive cardiac cycles (three frames)were measured, and an average was calculated for eachindividual measure. Measurements of left ventricularinternal diameter (LVID), interventricular septal thickness(IVS), and left ventricular free wall thickness (LVFW) wereobtained in both diastole (d) and systole (s). Left ventricularmuscle mass (LV mass ¼ 1.04 � [{LVIDd þ LVFWd þ IVSd}3
� LVIDd3] � 13.6) [33], relative to estimated body weight(LVmass [g/kg]), was calculated.
The tricuspid (TRI), pulmonary (PUL), mitral (MIT) andaortic (AO) valves were all examined by color flowDoppler echocardiography with a 1.5-MHz phased-arraysector transducer with harmonic imaging (Vivid 3, GEHealthcare, Brøndby, Denmark). Based on the area ofregurgitation in comparison with the approximated size ofthe atrium for the mitral and tricuspid regurgitation, fourgroups were defined as previous described [22]. Group 1:“very small jet” (>0%-10% of the area of the atrium),Group 2: “small jet” (>10%-30%), Group 3: “medium jet”(>30%-50%), and Group 4: “large jet” (>50%). For theaortic and pulmonary regurgitation, maximal diameter ofthe regurgitant blood flow just below the aortic/pulmo-nary valves was measured [22].
The echocardiographic variables were obtained andanalyzed in a blinded manner by an experienced operatorunaware of the identity of the horse and the electrocar-diographic findings.

R. Buhl et al. / Journal of Equine Veterinary Science 33 (2013) 590-596592
2.2.2. ECG RecordingResting ECG was recorded in the stall. The electrodes
were placed as follows in the saddle girth area: the green(positive) electrode was placed 5 cm left from the sternum.The red electrode (negative) was placed on the left side ofthe thorax, approximately 20 cm below the top of thethorax. The black electrode (neutral) was placed betweenthe red and green electrodes. Finally, the yellow (positive/negative) electrode was placed on the right side of thorax,approximately 20 cm below the top of the thorax. Wireswere connected to the electrodes and linked up to thetelemetric ECG unit (Krutech Televet 100 Veterinary Tele-metric ECG system, Kruuse A/S, Denmark). Resting ECGwasrecorded for 10minutes, and datawere saved on an SD cardthat was later inserted into a computer for analysis.
When recording ECG during racing, electrodes wereplaced as described previously. Adhesive foam tape (SnöggA/S, Kristiansand, Norway) was used as an extra safety tosecure the electrodes. All electrodes were placed so theycould be tightly fixated by an elastic girth. ECG recordingswere obtained during and until 15 minutes after racing(Fig. 1).
2.2.3. ECG AnalysesThe ECG recordings were analyzed in a blinded manner
by observer unaware of the identity of the horse or thefindings on the echocardiography.
The analyses were performed using the ECG softwareprogram (Krutech Televet 100 Veterinary Telemetric ECGsystem, Kruuse A/S, Denmark), detecting deviations in R-Rintervals at a 20% level for resting ECG and 10% level forexercise and postexercise ECGs. In addition, all ECGs werevisually inspected. Only those ECG recordings wereincluded where R-R intervals were easy recognizable andECG recording was complete from race start until15 minutes after racing. ECG recordings were analyzed forarrhythmias at rest, during exercise, and after exercise.
The following arrhythmias were registered [5]:
� Sinoatrial (SA) block: absence of P waves for a durationof twice the previous P-P interval.
Fig. 1. Placement of electrodes. (A) Placement of electrodes (arrows) on the left sidand the telemetric sender is fixed to the girth (arrow).
� Second-degree Atrio-ventricular (AV) block: P wavenot associated with any following QRS complex anddouble length of R-R interval.
� SVPC: R-R interval decreased more than 20% (duringrest) or 10% (during exercise or in the immediaterecovery period) in distance from the previous R-Rinterval and no change in configuration of the QRScomplex.
� VPC: R-R interval decreased more than 20% (duringrest) or 10% (during exercise or in the immediaterecovery period) in distance from the previous R-Rinterval and configuration of QRS complex was ofobviously higher amplitude, longer duration, andabnormal morphology than the previous sinus QRScomplex.
2.2.4. Blood SamplesPeripheral blood samples were obtained by jugular
venipuncture approximately 24 hours before racing. Forpractical reasons, blood samplings were only performed ontwo occasions after racing, once just after racing (15-60minutes) and once between 12 and 14 hours after racing.Samples were collected in 10-mL lithium heparin tubes (BDvacutainer LH, Belliver Industrial Estate, Plymonth, UK). Allblood samples were centrifuged (906 g for 10minutes), andthe plasma was separated and frozen at �80�C within 15minutes after sampling.
Plasma concentrations of cTnI were measured with anenzyme immunoassay (Architect CI8200, Abbot Laborato-ries, Diagnostic Division, Abbott Park, IL) with an analyticalsensitivity of <0.0022 mg/L. The troponin amino-acidsequence is highly conserved across species, and humanassays can therefore be used for equine samples [27,28].
2.2.5. Statistical MethodsEchocardiographic images were analyzed by three
repeated-measures from three different images, both forcalculation of LV mass and for tricuspid, pulmonary, mitral,and aortic valve regurgitation. Mean values of LV mass,pulmonary, and aortic regurgitation as well as the median
e of thorax covered by foam tape. (B) The girth is placed over the electrodes,

Table 1Number of horses (N,%) developing SVPCs and/or VPCs during racing andin the recovery period (0-2 minutes and 3-15 minutes after racing)
SVPC VPC
N (%) N (%)
Racing 13 (50.0) 1 (3.8)0-2 minutes after racing 12 (46.2) 5 (19.2)3-15 minutes after racing 2 (7.7) 1 (3.8)
SVPC, supraventricular premature complexes; VPC, ventricular prematurecomplexes.
R. Buhl et al. / Journal of Equine Veterinary Science 33 (2013) 590-596 593
value of tricuspid and mitral were calculated. For furtherstatistical analysis, the valvular regurgitation was classifiedas present or absent, with regurgitation being presentwhenever the mean (for pulmonary and aortic) or median(for tricuspid and mitral) regurgitation was above zero.
Numbers of arrhythmias were calculated for eachexamination for each horse at rest, during racing, and0-2 minutes and 3-15 minutes in the recovery period afterracing.
Association between presence of valvular regurgitation(TRI, PUL, MIT, AO) and arrhythmias during and after racing(SVPCs or VPCs) as well as association between heart sizeand the presence of arrhythmias during and after racing(SVPCs or VPCs) were examined by Spearman correlationcoefficient using GraphPad Prismversion 5.04 forWindows(GraphPad Software, San Diego, CA). A 5% significance levelwas used.
3. Results
3.1. Clinical Examination
Clinical examinations of all horses fell within the inclu-sion criteria of the study and were unremarkable, withnormal resting HR (range: 26-44 bpm), rectal temperature,and cardiac and pulmonary auscultation. Cardiac rhythmwas normal, with three horses having second-degree AVblock and two horses having sinoatrial block. In sevenhorses, a systolic murmur with a point of maximum inten-sity (PMI) over tricuspid valvewasheard (twohorses grade I,three horses grade II, and two horses grade III). Four horseshad a diastolic murmur auscultated with a PMI over aorticvalve (grade I).
3.2. Echocardiography
All 26 horses underwent echocardiographic examina-tion, and no abnormal enlargement of the size of leftventricle or abnormal contractility of the left ventricle wasobserved. The LV mass was estimated to 4000 g � 618 g(mean � SD), and LV mass relative to body weight wascalculated to 7.89 g/kg � 1.33 g/kg. Three horses had novalvular regurgitation diagnosed by echocardiography. Theremaining horses had one or more valvular regurgitations:9 (34.6%) mitral valve regurgitation, 16 (61.5%) tricuspidvalve regurgitation, 10 (38.5%) aortic valve regurgitation,and 7 (26.9%) pulmonary valve regurgitation. All mitral andtricuspid valvular regurgitations were classified as “verysmall jet” according to previously described classificationcriteria. For aortic and pulmonary regurgitation, themaximal diameter of the regurgitant blood flow just belowthe aortic/pulmonary valves was <1.0 cm for all horses.
3.3. Electrocardiography
The average maximum HR during racing was229 � 10 bpm (mean � SD). Two minutes after racing,average HR was 133 � 18 bpm, which was further reducedto 93 � 11 bpm 15 minutes after racing.
The distribution of horses developing arrhythmiasduring and after racing is shown in Table 1, with themajority of SVPCs developing during racing and within the
first 2 minutes in the recovery period after racing. Thefrequency of SVPCs during racing and in the recoveryperiod was �18 SVPCs/horse, with mean � SD of 4 � 4.Eight horses had paired SVPCs. Only one horse developedVPC during racing; five horses showed VPC within0-2 minutes after racing; and one horse had one VPC3-15 minutes after racing. The VPCs occurred in singleepisodes, except in one horse, where paired VPCs wereobserved during the first 2 minutes of recovery after racing.The distribution of SVPCs and VPCs for individual horses isshown in Table 2, and examples of individual ECG record-ings are shown in Figure 2.
There was no significant association between heart size(LVmass [g/kg]) and presence of SVPCs or VPCs duringracing or in the recovery period (P> .05). Also, therewas nosignificant association between the presence of any type ofvalvular regurgitation and the presence of either SVPCs orVPCs during racing or in the recovery period (P > .05).
3.4. Blood Samples
cTnI was for all blood samples below the detection limitof the assay (<0.022 mg/L) at rest and both at 15-60minutesand 12-14 hours after the race, and therefore, no furtherstatistical analyses were performed.
4. Discussion
To our knowledge, this is the first study that evaluatedthe association between cardiac arrhythmias during racingand in the recovery period to the size of the heart,the prevalence of valvular regurgitation, and cTnIconcentrations.
Only one recently published study has examined horseselectrocardiographically during racing conditions [7]. Allprevious studies have examined horses during training orduring treadmill exercise [2-6]. In contrast to the latterstudies, the current study showed a high number of horsesdeveloping SVPCs both during and in the recovery periodimmediately after racing [2-4]. This discrepancy in resultsmay be explained by the lack of consistency in the defini-tion of arrhythmia between studies. We accepteda maximal deviation in R-R intervals of 10% during exercise,as we have used it previously [5,6]. If higher maximaldeviation in R-R intervals was allowed, it would lead toa decrease in the number of SVPCs detected. As no defini-tion of deviation in R-R intervals was described in theprevious studies, we were not able to explain thedisagreement between our study and earlier studies.Furthermore, cardiovascular stress may differ dependingon the workload (training situation vs. racing), where

Table 2Total number of SVPCs and VPCs during racing and in the recovery period (0-2 and 3-15 minutes after racing) for each of the 26 horses completing the study
Caserecord no.
Age Sex SVPCduring race
SVPC recovery0-2 minutes
SVPC recovery3-15 minutes
VPC duringrace
VPC recovery0-2 minutes
VPC recovery3-15 minutes
2 6 S 0 0 0 0 0 04 3 S 2 1 1 0 0 05 7 S 7 (1 pair) 0 0 0 0 06 6 M 0 0 0 0 0 08 6 G 3 1 0 0 0 19 3 M 3 0 0 0 0 012 4 S 0 0 0 0 0 014 4 M 0 0 0 0 0 016 6 G 2 3 (1 pair) 1 0 1 017 5 G 0 0 0 0 0 018 3 G 7 (1 pair) 6 0 0 0 021 3 S 0 4 (1 pair) 0 0 5 (1 pair) 022 5 S 3 1 0 0 0 025 3 S 2 5 0 0 0 029 5 G 0 5 (1 pair) 0 0 1 030 6 S 0 0 0 0 0 031 3 S 4 0 0 0 0 033 6 G 2 2 0 0 1 034 3 G 0 0 0 0 0 036 4 M 0 0 0 1 1 037 6 G 0 4 (1 pair) 0 0 0 038 6 G 0 2 (1 pair) 0 0 0 041 4 G 16 (1 pair) 2 0 0 0 042 4 M 1 0 0 0 0 043 5 S 0 0 0 0 0 044 3 S 1 0 0 0 0 0
G, gelding; M, mare; S, stallion; SVPC, supraventricular premature complexes; VPC, ventricular premature complexes.If double SVPCs were found, this is specified in parentheses.
R. Buhl et al. / Journal of Equine Veterinary Science 33 (2013) 590-596594
racing conditions are generally accepted to be more phys-ical demanding in comparison with training situations. Asthe only study that previously has been performed duringracing conditions [7] did not examine the prevalence ofSVPCs, we cannot compare these two studies.
The number of horses with VPCs in the current studywas lower than in previous studies [2,4] but was inagreement with that reported by Physick-Sheard andMcGurrin [7], who found that 27.8% of the horses devel-oped ventricular arrhythmias immediately after racing.Interestingly we primary observed single VPCs in contrastto Physick-Sheard and McGurrin [7] who observed morecomplex ventricular arrhythmias. The disparity betweenthe results of previous studies [2,4] and our study mayagain be explained by different training regimens and lackof consistency of arrhythmias’ assessment. Furthermore,horses examined in the previous studies [2,4] were allpoorly performing horses, which probably explains thehigher prevalence of VPCs. This supports the opinion ofequine cardiologists that SVPCs generally are to be regar-ded as physiological and VPCs as pathological [8,9,34]. It iswell-known that horses exhibit high vagal tone, and it isbelieved that fluctuations on autonomic tone are related toarrhythmias [7,9]. In an earlier study, it was observed thatthe autonomic control was reduced during high exerciseintensity [35], which supports that arrhythmias primarilyoccur when HR changes, probably influenced by the para-sympathetic nervous system. This is supported by results ofa previous study, where one-third of the arrhythmic eventsoccurred simultaneously with a sudden reduction in HR,suggesting autonomic instability and increase in vagal toneas a contributing factor [7]. Association with physical effort
and potential stressful circumstances may also influencearrhythmia development. Physick-Sheard andMcGurrin [7]found that circumstances imposing unusual demandappeared to predispose on subsequent arrhythmias devel-oping after exercise. This was observed in horses parked atthe half mile or trotters breaking in the stretch. Therefore,these authors suggest that both physiological as well aspsychological stress may influence on development ofventricular arrhythmias. As we did not register specificevents during racing, we were not able to confirm theirinterpretations.
In the present study, single SVPC and VPC and pairedSVPCs and VPCs were observed. Coupled prematurecomplexes are regarded to be of higher clinical significancethan single premature complexes [8,9,34]. The data of thepresent study cannot support this, but other studiesdemonstrated a higher risk of subsequent development ofatrial or ventricular fibrillation in horses with frequentlyoccurring SVPCs or VPCs [36,37].
The presence of aortic, pulmonary, mitral, and tricuspidvalve regurgitation detected by color flow Doppler echo-cardiography in the present study is similar to that reportedboth for human and equine athletes [22,23,38-40]. Valvularregurgitations found in this study were classified as smalland regarded as physiological in agreement with others[22,23]. No significant association between valvular regur-gitation and the presence of arrhythmias was found, whichindicates that minor valvular regurgitations do not influ-ence on the regularity of electrical conduction of the heart.These data add further weight to the hypothesis that thehigh prevalence of valvular regurgitation in all athleticspecies is physiological in origin. Therefore, they generally
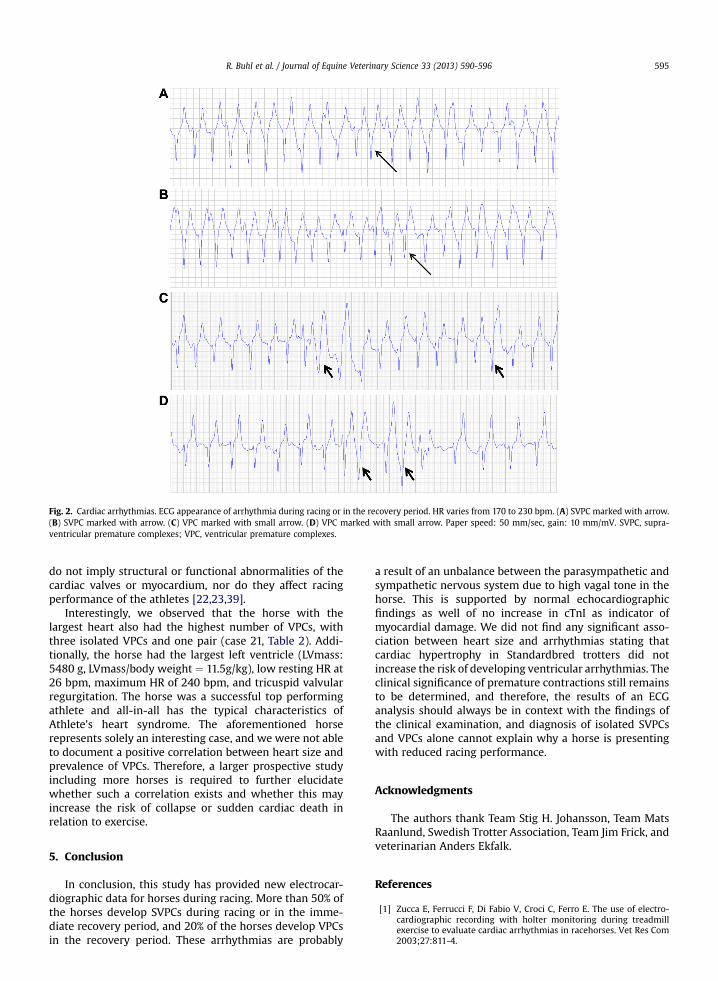
Fig. 2. Cardiac arrhythmias. ECG appearance of arrhythmia during racing or in the recovery period. HR varies from 170 to 230 bpm. (A) SVPC marked with arrow.(B) SVPC marked with arrow. (C) VPC marked with small arrow. (D) VPC marked with small arrow. Paper speed: 50 mm/sec, gain: 10 mm/mV. SVPC, supra-ventricular premature complexes; VPC, ventricular premature complexes.
R. Buhl et al. / Journal of Equine Veterinary Science 33 (2013) 590-596 595
do not imply structural or functional abnormalities of thecardiac valves or myocardium, nor do they affect racingperformance of the athletes [22,23,39].
Interestingly, we observed that the horse with thelargest heart also had the highest number of VPCs, withthree isolated VPCs and one pair (case 21, Table 2). Addi-tionally, the horse had the largest left ventricle (LVmass:5480 g, LVmass/body weight ¼ 11.5g/kg), low resting HR at26 bpm, maximum HR of 240 bpm, and tricuspid valvularregurgitation. The horse was a successful top performingathlete and all-in-all has the typical characteristics ofAthlete’s heart syndrome. The aforementioned horserepresents solely an interesting case, and we were not ableto document a positive correlation between heart size andprevalence of VPCs. Therefore, a larger prospective studyincluding more horses is required to further elucidatewhether such a correlation exists and whether this mayincrease the risk of collapse or sudden cardiac death inrelation to exercise.
5. Conclusion
In conclusion, this study has provided new electrocar-diographic data for horses during racing. More than 50% ofthe horses develop SVPCs during racing or in the imme-diate recovery period, and 20% of the horses develop VPCsin the recovery period. These arrhythmias are probably
a result of an unbalance between the parasympathetic andsympathetic nervous system due to high vagal tone in thehorse. This is supported by normal echocardiographicfindings as well of no increase in cTnI as indicator ofmyocardial damage. We did not find any significant asso-ciation between heart size and arrhythmias stating thatcardiac hypertrophy in Standardbred trotters did notincrease the risk of developing ventricular arrhythmias. Theclinical significance of premature contractions still remainsto be determined, and therefore, the results of an ECGanalysis should always be in context with the findings ofthe clinical examination, and diagnosis of isolated SVPCsand VPCs alone cannot explain why a horse is presentingwith reduced racing performance.
Acknowledgments
The authors thank Team Stig H. Johansson, Team MatsRaanlund, Swedish Trotter Association, Team Jim Frick, andveterinarian Anders Ekfalk.
References
[1] Zucca E, Ferrucci F, Di Fabio V, Croci C, Ferro E. The use of electro-cardiographic recording with holter monitoring during treadmillexercise to evaluate cardiac arrhythmias in racehorses. Vet Res Com2003;27:811-4.

R. Buhl et al. / Journal of Equine Veterinary Science 33 (2013) 590-596596
[2] Martin BB, Reef VB, Parente EJ, Sage AD. Causes of poor performanceof horses during training, racing, or showing: 348 cases (1992-1996). J Am Vet Med Assoc 2000;216:554-8.
[3] Ryan N, Marr CM, McGladdery AJ. Survey of cardiac arrhythmiasduring submaximal and maximal exercise in thoroughbred race-horses. Equine vet J 2005;37:265-8.
[4] Jose-Cunilleras E, Young LE, Newton JR, Marlin DJ. Cardiacarrhythmia during and after treadmill exercise in poorly performingThoroughbred racehorses. Equine vet J Suppl 2006;36:163-70.
[5] Buhl R, Meldgaard C, Barbesgaard L. Cardiac arrhythmias in clinicallyhealthy show jumping horses. Equine Vet J Suppl 2010;42:196-201.
[6] Barbesgaard L, Buhl R, Meldgaard C. Prevalence of exercise-associated arrhythmias in normal performing dressage horses.Equine Vet J Suppl 2010;42:202-7.
[7] Physick-Sheard PW, McGurrin MK. Ventricular arrhythmias duringrace recovery in Standardbred racehorses and associations withautonomic activity. J Vet Intern Med 2010;24:1158-66.
[8] Miller MS, Bonagura JD. Atrial arrhythmias. J Equine Vet Sci1985;5:300-4.
[9] Durando M. Exercise and stress testing. In: Marr CM, Bowen M,editors. Cardiology of the horse. Second Ed. St. Louis, MO: SaundersElsevier; 2010. p. 139-49.
[10] Bryan G, Ward A, Rippe JM. Athletic heart syndrome. Clin SportsMed 1992;11:259-72.
[11] Fagard RH. Athlete’s heart: a meta-analysis of the echocardiographicexperience. Int J Sports Med Suppl 1996;3:140-4.
[12] Young L. Cardiac responses to training in 2-year-old Thoroughbreds:an echocardiographic study. Equine Vet J Suppl 1999;30:195-8.
[13] Buhl R, Ersbøll AK, Eriksen L, Koch J. Changes over time in echo-cardiographic measurements in young Standardbred racehorsesundergoing training and racing and association with racing perfor-mance. J Am Vet Med Assoc 2005;226:1881-7.
[14] Maron BJ, Pelliccia A. The heart of trained athletes. Cardiac remod-elling and the risks of sports, including sudden death. Circulation2006;114:1633-44.
[15] Buhl R, Ersbøll AK. Echocardiographic evaluation of changes in leftventricular size and valvular regurgitation associated with physicaltraining during and after maturity in Standardbred trotters. J Am VetMed Assoc 2012;240:205-12.
[16] Maron BJ, Chaitman BR, Ackerman MJ. Recommendations forphysical activity and recreational sports participation for youngathletes with genetic cardiovascular diseases. Circulation2004;109:2807-16.
[17] Maron BJ, Roberts WC, McAlliater HA, Rosing DR, Epstein SE. Suddendeath in young athletes. Circulation 1980;62:218-29.
[18] Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G. Trendsin sudden cardiovascular death in young competitive athletes afterimplementation of a preparticipation screening program. J Am MedAssoc 2006;296:1593-601.
[19] Wang W, Manson JE, Hu FB. Physical exertion, exercise and suddencardiac death in woman. J Am Med Assoc 2006;295:1399-403.
[20] Ehses W, Niklaus K, Brockmann M, Angenendt W, Saborowski F.Fatal arrhythmia in a juvenile athlete due to myocardial hypertrophyand infarction. Int J Sports Med 2000;21:536-9.
[21] Fagard R. General cardiology. Athlete’s heart. Heart 2003;89:1455-61.[22] Buhl R, Ersbøll AK, Eriksen L, Koch J. Use of color Doppler echocar-
diography to assess the development of valvular regurgitation inStandardbred trotters. J Am Vet Med Assoc 2005;227:1630-5.
[23] Young LE, Rogers K, Wood JL. Heart murmurs and valvular regur-gitation in Thoroughbred racehorses: epidemiology and associationwith athletic performance. J Vet Intern Med 2008;22:418-26.
[24] Miller PJ, Holmes JR. Observations on seven cases of mitral insuffi-ciency in the horse. Equine Vet J 1985;17:181-90.
[25] Shaftoe S, McGuirk SM. Valvular insufficiency in a horse with atrialfibrillation. Compend Contin Educ Pract Vet 1985;9:203-8.
[26] Reef VB, Bain FT, Spencer PA. Severe mitral regurgitation in horses:clinical, echocardiographic and pathological findings. Equine Vet J1998;30:18-27.
[27] Adams JE, Bodor GJ, Davila-Roman VG, Delmez JA, Apple FS,Ladenson JH, et al. Cardiac troponin I. A marker with specifity forcardiac injury. Circulation 1998;88:101-6.
[28] Ricchiuti V, Sharkey SW, Murakami MW, Voss EM, Apple FS. CTnIand T alterations in dog hearts with myocardial infarction: corre-lation with infarct size. Am J Clin Pathol 1998;110:241-7.
[29] Gehlen H, Rohn K, Deegen E, Stadler P. Analysis of laboratory valuesin horses with cardiac disease. Diagnostic value of different cardiacbiomarkers. Pferdeheilkunde 2006;22:532-41.
[30] Schwartzwald CC, Hardy J, Bucellato M. High cTnI serum concen-tration in a horse with multiform ventricular tachycardia andmyocardial necrosis. J Vet Intern Med 2003;17:364-8.
[31] Durando MM, Reef VB, Kline K, Birks EK. Acute effects of shortduration maximal exercise on cTnI in healthy horses. Equine andComparative Exercise Physiology 2006;3:217-23.
[32] Nostell K, Häggström J. Resting concentration of cTnI in fit horsesand effect of racing. J Vet Cardiol 2008;10:105-9.
[33] Devereux RB, Reichek N. Echocardiographic estimation of ventric-ular mass in man: anatomic validation of the method. Circulation1977;55:613-8.
[34] Bonagura JD, Miller MS. Junctional and ventricular arrhythmias.J Equine Vet Sci 1985;5:347-50.
[35] Cottin F, Medigue C, Lopes P, Petit E, Papelier Y, Billat V. Effect ofexercise intensity and repetition on heart rate variability duringtraining in elite trotting horse. Int J Sports Med 2005;26:859-67.
[36] Hiraga A, Kubo K. Two cases of paroxysmal atrial fibrillation duringexercise in horses. Equine Vet Educ 1999;11:6-10.
[37] Kiryu K, Machida N, Kashida Y, Yoshihara T, Amada A, Yamamoto T.Pathologic and electrocardiographic findings in sudden cardiacdeath in racehorses. J Vet Med Sci 1999;61:921-8.
[38] Pollak SJ, McMillan SA, Knopff WD. Cardiac evaluation of womendistance runners by echocardiographic color Doppler flow mapping.J Am Coll Cardiol 1988;11:89-93.
[39] Douglas PS, Berman GO, O’Toole ML, Hiller WD, Reichek N. Preva-lence of multivalvular regurgitation in athletes. Am J Cardiol1989;64:209-12.
[40] Macchi C, Catini C, Catini CR. A comparison between the heart ofyoung athletes and of young healthy sedentary subjects;a morphometric and morpho-functional study by echo-colordoppler method. Ital J Anat Embryol 2001;106:221-31.