Embed Size (px)
Citation preview

http://rsh.sagepub.com/for the Promotion of Health
The Journal of the Royal Society
http://rsh.sagepub.com/content/104/5/161The online version of this article can be found at:
DOI: 10.1177/146642408410400501
1984 104: 161The Journal of the Royal Society for the Promotion of HealthVal Box
Cancer: Myths and Misconceptions
Published by:
http://www.sagepublications.com
On behalf of:
Royal Society for Public Health
can be found at:The Journal of the Royal Society for the Promotion of HealthAdditional services and information for
http://rsh.sagepub.com/cgi/alertsEmail Alerts:
http://rsh.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://rsh.sagepub.com/content/104/5/161.refs.htmlCitations:
What is This?
- Oct 1, 1984Version of Record >>
at The University of Edinburgh on November 17, 2014rsh.sagepub.comDownloaded from at The University of Edinburgh on November 17, 2014rsh.sagepub.comDownloaded from

161
The Journal of .
The Royal Society ofHealth
VOLUME 104 No 5 OCTOBER 1984
Cancer: Myths and Misconceptions*VAL BOX, M.SC., DIP.DIET, DIP.ED. FRSH., Cancer Education Adviser, S. W. Thames Regional Cancer Organisation, Royal Marsden Hospital,Sutton
INTRODUCTIONTHE FIRST paragraph of an American textbook ofCancer Nursing will be quoted, as it provides an approp-riate introduction to the psychosocial impact of cancer.
&dquo;Cancer is a word that elicits an immediate emotionalresponse, a response that seems to have no relationshipto rational thinking, depth of knowledge of the indi-vidual, or the individual’s role in society. The sameresponse seems to occur in physiciens, nurses, collegeprofessors, researchers, politicians, and unskilledlabourers alike. It occurs in patients, families, friends ofthose who have cancer, people who think they may have
’ cancer, or people who take the view that cancer is some-thing that will happen to other people. In all of thesegroups, the feelings and mental images stirred up by themention or thought of the word cancer seem to be practi-cally identical&dquo;’.
’
So far this description has only stated that attitudes tocancer are universal. However the writer would be sur-
prised if the majority of readers had not imagined this tobe a pessimistic description.
This article will attempt to document the public’sknowledge in relation to cancer.. However when asked aquestion very few people will admit to not knowing theanswer. It is the author’s contention that wrong answers
may provide useful information in relation to therespondent’s attitude to a subject. Therefore knowledgeof and attitudes to cancer will be considered together.Health professionals’ attitudes will then be comparedwith those of the public. The expected effects in relationto such issues as reporting ’suspicious symptoms’ earlywhen the chance of cure would be greater and com-
* Paper presented at a meeting of The Royal Society of Health March1 st 1984.
pliance to health behaviour such as screening will also beconsidered.
Based on discussion of cancer knowledge andattitudes, the aims and objectives of cancer educationwill then be suggested and how these could be
implemented. ,
PUBLIC OPINON SURVEYSTHERE HAVE BEEN four large public opinion studies inthe U.K. carried out between 1953 and 1974, andinformation from these will be quoted together withadditional evidence from smaller studies where approp-riate.( 1 ) Manchester Study
In 1953 Paterson and Aitken-Swan conducted aninterview study in the Manchester area 2. A follow-upstudy was carried out by the same authors in 1957 on twodifferent populations within the region, one of whomhad been exposed to a cancer public education cam-paign3. Approximately 1200 women chosen ’systemati-cally’ from the electoral role were interviewed in each ofthe three groups. Women were chosen as they werebelieved to delay longer in consulting a doctor whensymptoms which could suggest cancer occurred.(2) Lancaster StudyThe second large ’public opinion’ study was carried
out by Briggs and Wakefield in Lancaster in 1966, againon women over 21 years of age’. As in the previous studya follow-up was carried out by Knopf 7 years later after apublic education campaign’, but this also includedwomen between 18-21 years.(3) Merseyside StudyA parallel study was conducted by Hobbs in Mersey-
side, 1966, to the one carried out in Lancaster6. How-
at The University of Edinburgh on November 17, 2014rsh.sagepub.comDownloaded from

162
ever the results are not exactly comparable as a certainamount of public education had already been carried outin Merseyside. Apart from those on Merseyside beingless positive about preventive measures, there is little toreport which is different from the other studies.(4) S.E. Wales StudyThe fourth study was carried out by Williams et al in
1972~ and is interesting as 203 men were interviewed aswell as 801 women. Differences in beliefs between thetwo sexes are noted, and in particular more men thanwomen -
(a) are optimistic in relation to cancer treatment(b) give definite answers instead of ’don’t knows’(c) provide correct answers.
THE PUBLIC’S KNOWLEDGE IN RELATION TOCANCERGeneral Cancer Knowledge:Some of the answers supplied by the public when
interviewed in the studies previously described are
documented in Table 1. It is interesting to note commonmisconceptions, but also pleasing to see evidence thatknowledge has improved over time.
a) Which disease kills most peopleIn 1980 there were 130,566 deaths from cancer in the
U.K., which accounted for 22% of all deathsg. Howeverdeaths from I.H.D. diease were 154,371, accounting for27% of deaths, and if figures are taken for ’circulatory’disease deaths these were 290,395, approximately halfof all deaths. The incidence of cancer is high, and it isnow quoted that 1 in 3 people develop cancer duringtheir life-time9. However, cure seems to be overlookedand to many a diagnosis of cancer implies impendingdeath. Data in Table 1 suggests that a large proportion ofthe population believe cancer to be the chief cause ofdeath and if anything the belief was increasing.
b) Early treatment increases the chance of cureSeveral studies have shown that with increasing delay
in reporting symptoms and receiving treatment, thepatient’s prognosis has become poorer. It is thereforereassuring to find that belief in early treatment hasimproved and by 1973 was 88%. However when lookingat the same studies there seems an overlap of views aswhen for example in 1973, 88% believed in curabilitywith early treatment there were also 22% who suggestedthat cancer is never completely curable. One feels thatalthough some people have correct information, whichthey can quote, their attitude may deny this knowledge.
c) Do you know someone who has been cured of cancer ?If approximately 33% of the population have cancer
at some time and yet only 20% of the population diefrom it, it could be suggested as a crude figure that 1 in 3are ’cured’ of their cancer or it is successfully controlledso that they do not die from it.Hoever in 1953 only 30% of the population knew
someone who had been cured and 45 % by 1966. It couldbe suggested that those with cured cancer may neverhave been told their diagnosis and therefore could nottell of their cure. Cancer has often been described as ataboo subject, one which we do not talk of and thereforecures are not advertised. Journalists appear happier topublicise ’The death of another cancer victim’ than thestory of an individual who is cured or coping successfullywith their disease.Early Warning Signs:
.
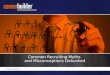
Questions and answers in relation to the ’early warningsigns’ of cancer are to be found in Table 2 and Figure 1.
It would appear that there has always been a highawareness of a lump in the breast being possibly cancer.Indeed one would be surprised if any woman did notknow of the possibility and one wonders if those who donot mention it are engaging in some type of denial.The knowledge that bleeding ten years after the
menopause is likely to be cancer still does not appear to(be realised by even the majority of women. Also it couldibe said that bleeding after the menopause is more likelythan a lump in the breast, of being cancer. One in ninebreast lumps are benign although in older women thechance of malignancy is higher. Cancer of both the cervixand uterus increase in the lower social classes, but unfor-tunately knowledge of their symptoms decreases as doescompliance with the cervical smear test.Other reasons given in 1973 for bleeding after the
menopause are listed in Figure 1. One finds that ’asusual’ the pill is blamed. There is some suggestion thatnot looking after oneself or perhaps being run down as acause. It has also beeen suggested’° that there is a beliefparticularly in social classes IV and V that it is normal toexpect poorer health as one gets older and this symptomin that case would probably not be reported.The last two suggestions are unfortunate, as although
it is now generally accepted that the incidence of cervicalcancer increases with the number of sexual partners, amoral judgement appears to have been made againstthose developing this type of cancer. This can produceseveral problems ranging from the belief that only prom-iscuous women need cervical smears, to being unwilling (to go for confirmation of the diagnosis of this type ofcancer for the fear of societal rejection.
Table 1.
Public Opinion in Relation to Cancer(% indicating a particular answer or attitude)
at The University of Edinburgh on November 17, 2014rsh.sagepub.comDownloaded from

163
Table 2.
Figure 1.
Other reasons given for bleeding 10 years after menopause
What Causes Cancer?:The most common spontaneous answers to interviewersquestions in relation to cancer causative factors are
smoking; and knocks, bumps and falls. Smoking wasmentioned by 18% of those interviewed in Lancaster in1966 rising to 20% in Lancaster in 1974, but this still isvery low. There was more agreement in the wrong belifin knocks, bumps and falls, 25% in 1953, 38% in 1969and 32% in 1974. This is often in relation to breastcancer. However it is also mentioned in relation to sportsinjuries and cancer of a limb bone. Other answers in1973 included highly seasoned food, pneumonia, pesti-cides and stress. The author would hazard a guess that ifthe public were asked in 1984 stress would be mentionedvery often. The difference between stress as a possiblepromoter more than a causative factor also appears to belittle understood. Table 3 summarises the percentage ofrespondents who agreed with a particular statement inrelation to cancer causation made by the interviewer in
, particular studies.- Belief in smoking is shown more clearly here andparticularly in men. Again there are moral overtonessuggested, as about a third of respondents agreed with’bad living’ as a cause. ’Bad living’ on probing meanssexual intercourse outside marriage but also treatingfamily members badly!
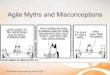
Physical cleanliness is also thought to be causative byabout a quarter of respondents. May be this is due toemphasis on hygiene in early health education. The onlyevidence to confirm this is a correlation between poordental hygiene and cancers of the mouth and one studysuggesting increased cervical cancer in the wives of menwho are employed in dirty jobs&dquo;. Figure 2 shows cervixstandardised mortality ratios for wives of men in particu-lar occupations. Very few people now appear to believethat cancer is catching but approximately a third believeit to be hereditary. However many of the public believethat if something is hereditary that if your father ormother had it then you are also bound to develop it.Inheritance of a higher potential than average does notseem to be understood and that one still needs to beexposed to a carcinogen such as cigarette smoke.
Figure 2.
Cervical Cancer - Standardised Mortality Ratios
Table 3.
% Agreeing with Interviewer Suggesting Cancer Causative factors
How can cancer be prevented?:When asked for spontaneous answers in relation tocancer prevention not many are quoted. The realisationthat having a cervical smear can be considered a first stepin cancer prevention has increased from 8% in 1966 to33% by 1973. Several answers made in 1973, the originsof which are debatable, will be quoted: don’t eat burntfood; stop tumbling; don’t think too much about it; keepblood in good condition; don’t eat tinned food.
THE PUBLIC’S MOST COMMON QUESTIONSIN 1977-80 several U.K. organisations with a remit forCancer Education under the auspices of the CancerEducation Co-ordinating Group of the U.K. kept a
record of the questions that were asked by the publicafter cancer talks. The information was collated and a
at The University of Edinburgh on November 17, 2014rsh.sagepub.comDownloaded from

164
report produced by Davison’2. These questions are
summarised in Table 4.
Table 4
Public’s Most Common Questions in Relation to Cancer 1979-80
’
As can be seen in almost 60% of the talks someoneasked whether cancer is inherited - suggesting personalvulnerability felt by individuals. Many of the audienceswere all female and therefore it may not be surprisingthat there ’ are several questions relating to cervicalsmears. However it may be useful for health profession-als to note that education and publicity in relation tocervical smears does not appear to be adequate.Almost half of the audiences asked whether cancer is
on the increase. Cancer is now given increasing publicity,although often undesirable in format or content, andtherefore it would seem reasonable that the public wouldthink it to be on the increase. However it must beremembered that the general public do not realise thatsome increase could be accounted for by an ageing pou-lation and much increase in relation to smoking. How-ever it is useful to remember that standardised mortalityratios for cancer by period of birth have decreased stead-ily since 1900 for men although not until 1930 forwomen&dquo;.
Other questions asked are quite predictable from theprevious discussion.
PROFESSIONAL BELIEFS ABOUT CANCERAre the public’s negative feelings about cancer just areflection of professional attitudes?It has been suggested that as health professionals andparticularly doctors are opinion leaders in relation tohealth, it would seem reasonable to consider whether thebeliefs and opinions of lay people have been influencedby those of health professionals. There has been no largeopinion poll conducted of doctors in relation to cancer,which is probably as researchers would assume theseprofessionals to be well informed. However there was astudy of attitudes of health professionals to the curabilityof cancer carried out by Davison in 1963&dquo;. Medicalstudents, general practitioners and nurses were asked toquote % five year survival after diagnosis of early stagecancer. The results are shown in Table 5.More medical students provided correct answers than
practising doctors or nurses. It could be suggested thatmedical students have more recently been provided withthe facts. As doctors underestimate survival for breatcancer by 25%, and cervical cancer by 37%, it could besuggested that this pessimistic attitude may affect thepatient adversely and they may be more hestitant inapproaching their general practitioner with vague symp-toms. The doctor may also, for example, not activelyencourage his patients to have regular cervical smears. If
the diagnosed patient is not likely to find an optimisticattitude from the doctor caring for him/her, this may beexpected to affect their ability to cope with the diagnosis.Indeed Beuhler1s reports that hope is promoted incancer patients when there is a generalised feeling ofhope amongst staff. A study by Klagsburn~6 correlates apositive ward climate with cancer patients’ increased willto live.
Table 5.
Comparison of health professionals’ attitudes to curability of BreastCancer
One wonders why some health professionals are
overly pessimistic about the curability of cancer. How-ever one begins to get an answer to this question, if oneconsiders the difference in attitude to curability whichhas been recorded amongst different health profession-als. For example Deeley&dquo; reports an overly optimisticview in skin specialists where cure is high and an overlypessimistic one in specialists dealing with stomachcancer. The particular curability of one particular sitemay become considered generalisable to all cancers. Thepessimism of community nurses has been explained bytheir daily contact with patients in a terminal stage of thedisease&dquo;. They may also have several patients at any onetime with fungating breast cancers, as the incidence isrelatively high. The author would also suggest that thecommunity nurse, who is usually female, will often iden-tify with a breast cancer patient, increasing the emo-tional impact of the situation providing over-
representation in attitude development.Compliance with recommended health practicesa) The health professional as a model:Gilmer and Hassels18 found that the American workingnurse had poorer health practices in relation to the pre-vention of cancer (abstaining from smoking) and check-ing for early warning signs (examining her breasts regu-larly) and fear cancer more than unemployed nurses.When members of the public, particularly those whosmoke are questioned about their belief in the relation-ship between smoking and lung cancer, those who do notaccept the causal association to be proven often quotethat if it was so, doctors and nurses would not smoke,which however they have observed them doing. A par-ticular example of such public scepticism can be illus-trated by quoting the answer of a West Indian respon-dent in a study conducted by Calnan and Johnson’9.
’Interviewer: Do you know of any causes of cancer?Respondent: They say smoking ...Interviewer: Would that be a special sort of cancer
that is caused?
at The University of Edinburgh on November 17, 2014rsh.sagepub.comDownloaded from

165
Respondent: Well I don’t know but the first time thatI hear about this complaint I was in theWest Indies - Jamaica - and a ladydie with it in our home and she neversmoke. And then a next lady die with itagain and she never smoke- but - youwent to doctor and doctor say ’Youmustn’t smoke’ and they still smoke,the doctors smoke. I know a doctor upat the hospital there - he tell a patientnot to smoke and he smoke - so I can’tsee it true.’
Fortunately smoking rates in doctors and nurses aredropping. A recent survey carried out in a cancer hospi-tal by Chilvers et al2° reported that 16% of doctors stillsmoke and 26% nurses (excluding nursing ausiliaries).These rates are below the national average which in1983 was reported for England and Wales as 33%women and 38% men21, but it is still surprising that justover a quarter of health professionals who can see theresults of this behaviour in the patients on their wardsstill smoke.The respondent’s answer may suggest another com-
mon misconception that all cancers are thought by some~of the public to be associated with smoking. Whichwould more easily explain their sceptism when nonsmokers also develop cancer.
b) Is the reason for non-compliance with health recom-mended practices due to the differeing health valuesof doctor and lay public?:
’
There appear to be different values placed on particularhealth practices not only between professionals and thelay public but between these groups in different coun-tries. In studies carried out in the U.S. the proportion ofpeople going regularly for check-ups increased from26% to 36% between 196622 and 19782&dquo;. Also themajority of people interviewed in 1978 had a positiveattitude towards check-ups, considering them to beworthwhile, necessary, thorough and effective.
In the U.K. General Practitioners usually do notencourage their patients to attend for regular check-ups.Indeed in a study carried out by Bluck24 in S.E. Wales in1975, General Practitioners were asked how they wouldrespond to a request for a general health check-up. Themajority of respondents suggested that the patient
Bwould have a ’psychological reason’ for asking for this.In an interview study conducted by the author&dquo; whenpatients were asked what services they would like theirhealth centre to offer, many of the 50-60 year oldssuggested they would like blood pressure checks, whichhad been refused. This request was interesting as the’real purpose’ of the study was to find out why patientshad not complied with a Haemoccult screening prog-ramme offered by their general practitioners. The per-ceived value of particular screening modalities differedbetween doctor and patient.The Haemoccult study compared compliance in rela-
tion to being offered the Haemoccult test, whichinvolved the patient in taking a small portion of theirfaeces and spreading this on a reagent impregnated cardon three consecutive days and returning this to theirhealth centre. 44% returned the kit in one practice and37% in another. 64 individuals were interviewed fromthe former practice to ascertain reasons for non-compliance. However as 24 individuals denied receivingthe kit and 5 said they had returned it only 35 could befully questioned. However the reliability of information
collected from the other 35 could well be questioned.Reasons for non-compliance are given in Table 6.
30% of respondents appeared to have no screeningorientation, many believing that their doctor should notbe troubled unless they had definite symptoms or couldno longer function adequately. A lack of a positive con-ception ot health is shown in this instance. A quarter ofrespondents expressed an opinion that they would rathernot know that they had cancer. These would be thecategory of person who may usually ’cope’ with prob-lems by denying their existence. They may also notbelieve cancer to be curable and therefore there seemedlittle value in early diagnosis and longer to live with thisknowledge? 9% expressed dissatisfaction in previousencounters with health professionals or hospitals and didnot wish to repeat these unpleasant experiences. 40% ofrespondents said they had not had enough time to com-ply with the test. In this case it could be suggested thatthe costs (in time and invonvenience) did not seem towarrant their perceived value of the particular test.
Table 6.
Haemoccult: Reasons for Non-Compliance
c) Patients dissatisfied with information given by theirdoctors are defaulting from their doctor’s instruc-tions :
It was the contention of Korsch et a126 that if doctors donot satisfy their patients’ desires for information in theirconsultations then the latter are less likely to conformwith medical prescribed behaviour. With a disease suchas cancer that has been described as stigmatised and ataboo subject&dquo; it is even more likely that doctors will beless likely to be completely open in the answers theyprovide. The work of McIntosh2K is useful to illustratethe extent of the subterfuge which may be used whendealing with the person with cancer and their relatives.McIntosh spent six months observing communication ina cancer ward of a large Scottish hospital.Whether to tell the cancer patient his diagnosis
appeared to be a major issue in McIntosh’s study, as theauthor would suggest it still is in many hospitals now.McIntosh reported that 94% of dermatologists informedtheir patients of their diagnosis, whereas only 12°/0 of theradiologists did. The deciding factor seemed to be theexpected curability of the cancer. If the cancer was emi-nently curable then the diagnosis was disclosed. How-ever euphemisms were often used instead of the word’cancer’. ’Suspicious cells’, ’turning cancerous’ and
‘malignant’ are a few examples. It would therefore notbe surprising to find that many patients who supposedly
at The University of Edinburgh on November 17, 2014rsh.sagepub.comDownloaded from

166
had been told, were still ignorant that they had a cancer.Why did most doctors not tell their patients? Was it
that the doctors shared the negative image of cancer heldby many of the public? Many doctors appear to assumethat the patient does not wish to be told. However, astudy conducted by Reynolds29 in 1981 suggested that90% of hospital patients interviewed, and these were notcancer patients, said they would want to know theirdiagnosis and 85 % their prognosis if they had cancer.interestingly a study carried out by Renneker andCutler3° as long ago as 1952 suggested that 100% ofbreast cancer patients actually knew their diagnosis,although many had not been explicitly told. It has beensuggested that the lack of trust that the ’aware patient’develops towards health professionals when they con-tinue to be evasive has a marked adverse affect on their
psychological well-being.
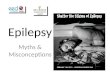
AIMS AND OBJECTIVES OF CANCER EDUCATION:HAVING CONSIDERED some of the public’s myths andmisconceptions in relation to cancer, and consideredtheir attitudes and how this may affect their vehaviour, itwould seem appropriate now to list the aims and objec-tives of cancer education and briefly consider how thesecould be implemented.
Figure 3
The aims of cancer education are suggested in Figure3. They are grouped such that some aims are in relationto providing accurate knowledge, whereas othersaddress themselves to producing more positive attitudes,which may hopefully produce behaviour expected toeither prevent cancer or minimise the treatment
required, while maximising the chance of cure in thosewho develop this disease.The aims and objectives of cancer education may
appear admirable,. but who is to put them into opera-tion ? The G.P. is considered to be in a powerful positionto health educate’° and the person-to-person approachto be more effective then the large group method. How-ever the author feels that the role of the nurse as cancereducator cannot be overstressed. Most of the publicknow a nurse, as they tend to belong to all social strataand every neighbourhood. Many people have less hesita-tion in asking their questions of nurses than doctors asthe latter are often thought to be too busy. If realisticattitudes are to be engendered then education will needto begin early. Cancer education therefore must also beprovided for school children. It is reassuring, althoughmay be surprising, to find that a survey carried out byCharlton3’ suggested that teachers held more optimisticattitudes and their information was more likely to becorrect than many health professionals. It was interest-ing that only 25 % of the children thought cancer to be
the main cause of death, and surprising that 60%believed road accidents to be the main killer. Indeedduring adolescence accidents are the main killer. Thismay provide a valuable evaluation of a recent RoadSafety Campaign!The person diagnosed with cancer may find that
friends and even family may begin to react differently tothem. There may be less touching and less eye contact.Conversations may be held standing at greater distancesfrom those with cancer 32, and jokes are no longer told.Persons with cancer are often gradually left out of thesocial circles in which they normally operate.Help in coming to terms with cancer can often usefully
be provided by those who have experienced and success-fully come to terms themselves. Although there aremany different cancers and aetiology and treatment willdiffer markedly, those with cancer may well have experi-enced very similar fears in relation to their disease andsimilar societal reactions. The author feels that experien-tial information and emotional support that can be pro-vided by those who have gone through a similar experi-ence, is of almost unquestionable value. So that thosewho have experienced cancer themselves or as relativesor close friends can also be called upon as cancereducators. It is the hope of the author that both profes-sional and experiential expertise can be successfully har- 4nessed to optimise the cancer experience for all of thosewho have already, or will in the future develop thishighly prevalent disease.
REFERENCES1 BURNS, N. Nursing and cancer, 1982. W. B. Saunders, Philadelphia.2 PATERSON, R. and AITKEN-SWAN, J., 1954. ’Public opinion on
cancer— a survey among women in the Manchester area’. Lancet ii,857.3 PATERSON, R. and AITKEN-SWAN, J., 1958. ’Public opinion on
cancer: changes following five years of cancer education. Lancet ii,791.
4 BRIGGS, J. E. and WAKEFIELD, J., 1967. Public opinion on cancer: asurvey of knowledge and attitudes among women in Lancaster.Dept. of Social Research, Christie Hospital and Holt Radium Insti-tute, Manchester.5 KNOPF, A., 1974. Changes in opinion after 7 years of public educa-
tion in Lancaster. Manchester Regional Committee on Cancer.6 HOBBS, P.,1967. Public opinion on cancer— a survey of knowledgeand attitudes among women on Merseyside. Merseyside CancerEducation Committee, Liverpool.
7 WILLIAMS, E. M., CRUICKSHANK, A. and WALKER, W., 1972. Publicopinion on cancer in South East Wales. Tenovus Cancer Informa-tion Centre, Cardiff.
8 H.M.S.O., 1983. Mortality statistics: cause England and Wales1981.
9 H.M.S.O., 1983. Cancer statistics: registrations England and Wales 1978.
10 DINGWALL, R., 1976. Aspects of illness. Martin Robertson, Lon-don.11 O.P.C.S., 1981. Cancer statistics: incidence, survival and mortabil-
ity in England and Wales. H.M.S.O., London.12 DAVISON, R. L., 1983. ’Questions about cancer: a study of the
public’s demand for information in six centres of the U.K. and theRepublic of Ireland’. J.Inst.HealthEduc., 21 (a). 5-16.13 OSMOND, C., GARDENER, M. J., ACHESON, E. D., 1982. ’Analysis of
trends in cancer mortality in England and Wales during 1951-80,separating changes associated with period of birth and period ofdeath’. B.M.J.: 284, 1005-8.14 DAVISON, R. L. 1965. ’Opinions of nurses on cancer, its treatment
and curability: a survey among nurses in Public Health Service. B. J.SOC. Prev. Med.: 19, 24-29.15 BEUHLER, J., 1975. ’What contributes to hope in the cancer
patient?’. Am.J.Nursing: 75, 453-60.16 KLAGSBRUN, S., 1970. ’Cancer emotions and nurses’.
Am.J.Psychiatry: 126, 1247-1244.17 DEELEY, T., 1979. Attitudes to cancer. Camelot Press, London.18 GILMER, R. and HASSELS, A., 1969. ’Nurses practises and attitudes
towares cancer’. Am.J.Nursing: 64, 84-5. 19 CALNAN, M. W. and JOHNSON, B. M., 1983. ’Understanding non-
compliance with cancer education campaigns’. Public educationabout cancer, U.I.C.C. Technical Report Series No.76.
continued on page 170
at The University of Edinburgh on November 17, 2014rsh.sagepub.comDownloaded from