Embed Size (px)
Citation preview
Calcium and Parathyroid Disorders
Hussain Mahmud, MDClinical Assistant Professor of MedicineDivision of Endocrinology, Diabetes, and Metabolism
University of Pittsburgh
Butler Memorial HospitalNovember 11, 2017
Disclosures
None
Outline
• Physiology of calcium, parathyroid hormone and vitamin D
• Hypercalcemia
• Primary hyperparathyroidism
• Hypocalcemia
PHYSIOLOGYAKA HOW THINGS WORK…
Physiologic Roles of Calcium
• Maintains electrochemical gradient across cell membranes
• Excitation contraction coupling in cardiac and other muscles
• Coagulation, synaptic transmission
• Hormone release and intracellular messenger:– Calcium acts as a second messenger
– Transforms extracellular signals into intracellular responses
Physiologic Roles of Calcium
Extracellular (ionized) calcium is tightly regulated
• Hypercalcemia => raises potential across cell making it difficult to excite
• Hypocalcemia => reduced membrane potential making cell hyperexcitable
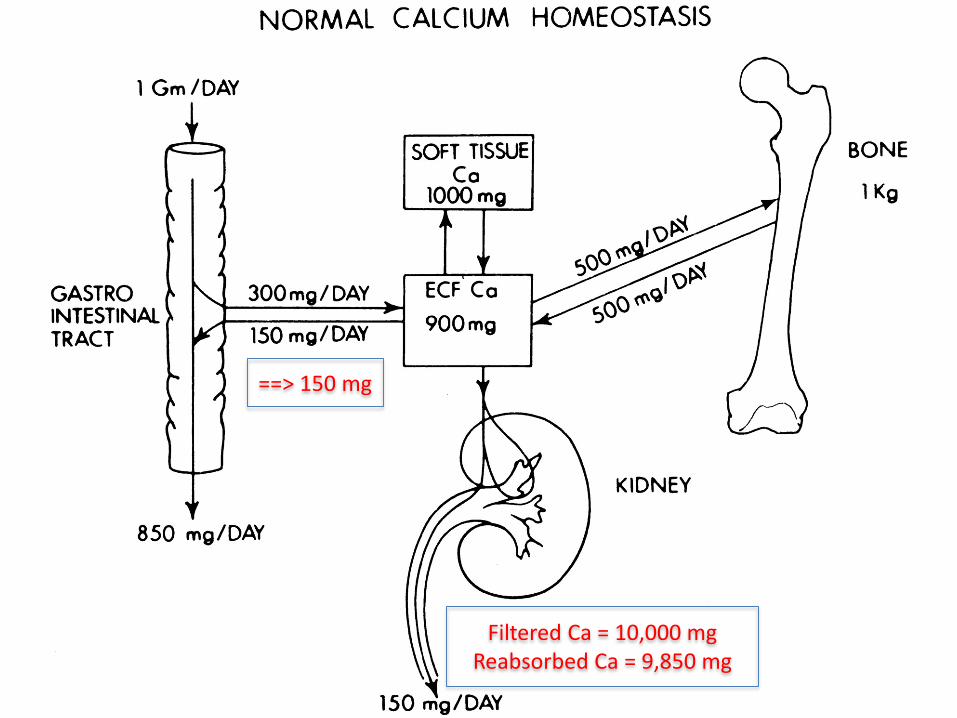
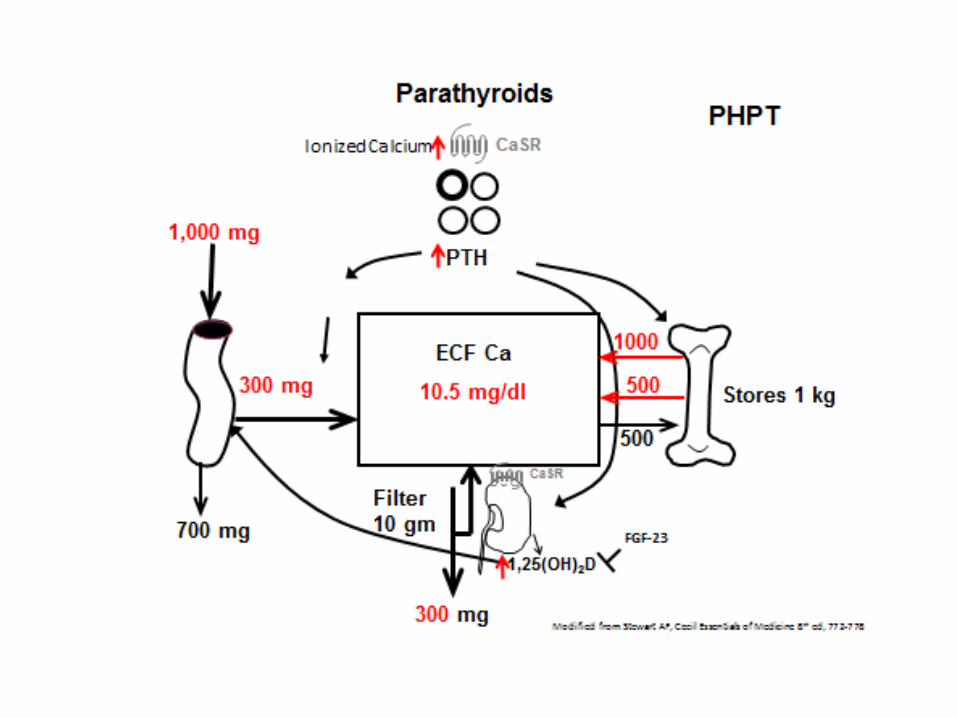
==> 150 mg
Filtered Ca = 10,000 mgReabsorbed Ca = 9,850 mg

NIH Office of Dietary Supplements Fact Sheet
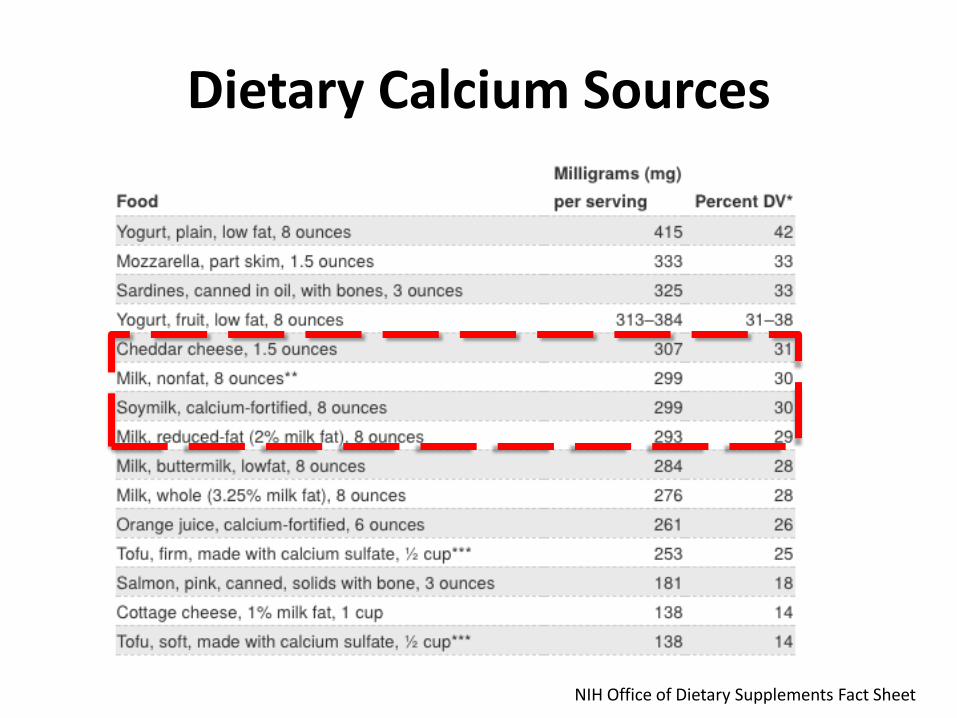
Dietary Calcium Sources
NIH Office of Dietary Supplements Fact Sheet
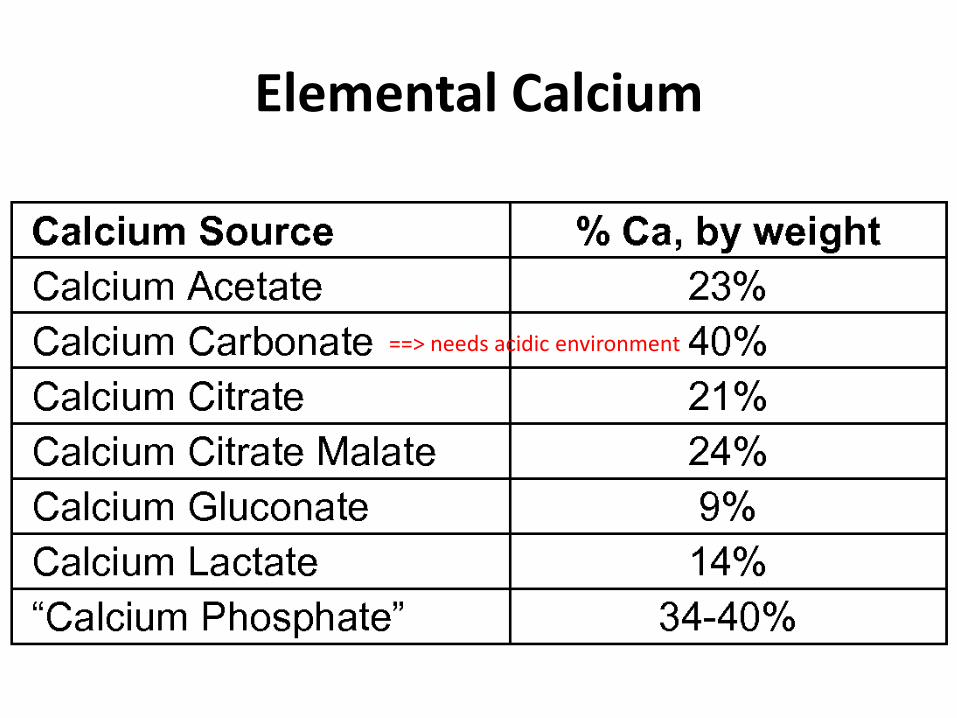
Elemental Calcium
==> needs acidic environment
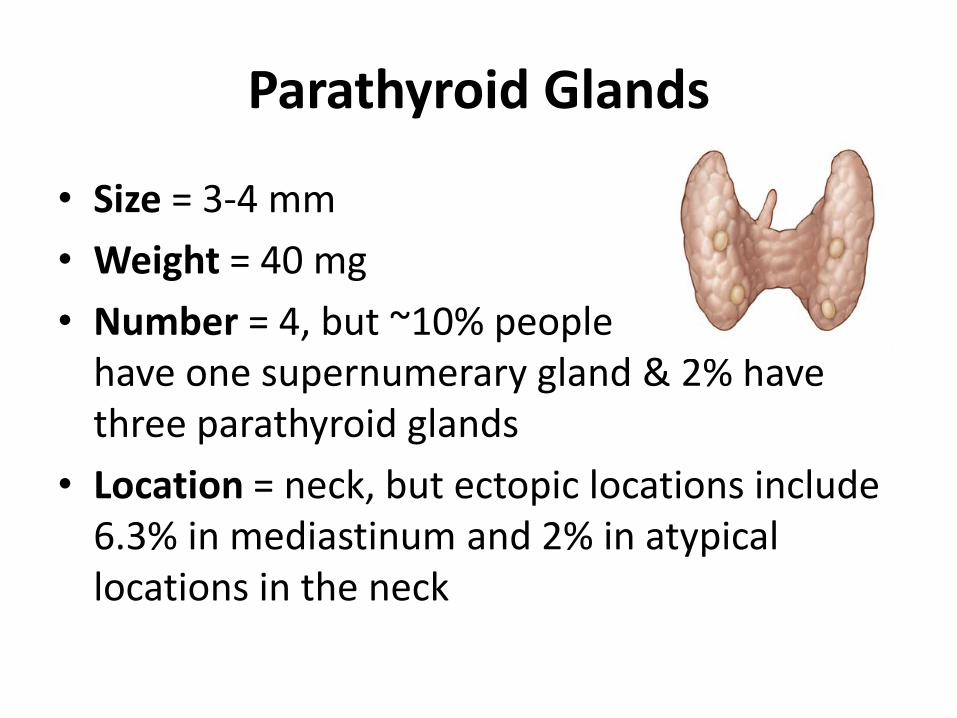
Parathyroid Glands
• Size = 3-4 mm
• Weight = 40 mg
• Number = 4, but ~10% people have one supernumerary gland & 2% have three parathyroid glands
• Location = neck, but ectopic locations include 6.3% in mediastinum and 2% in atypical locations in the neck
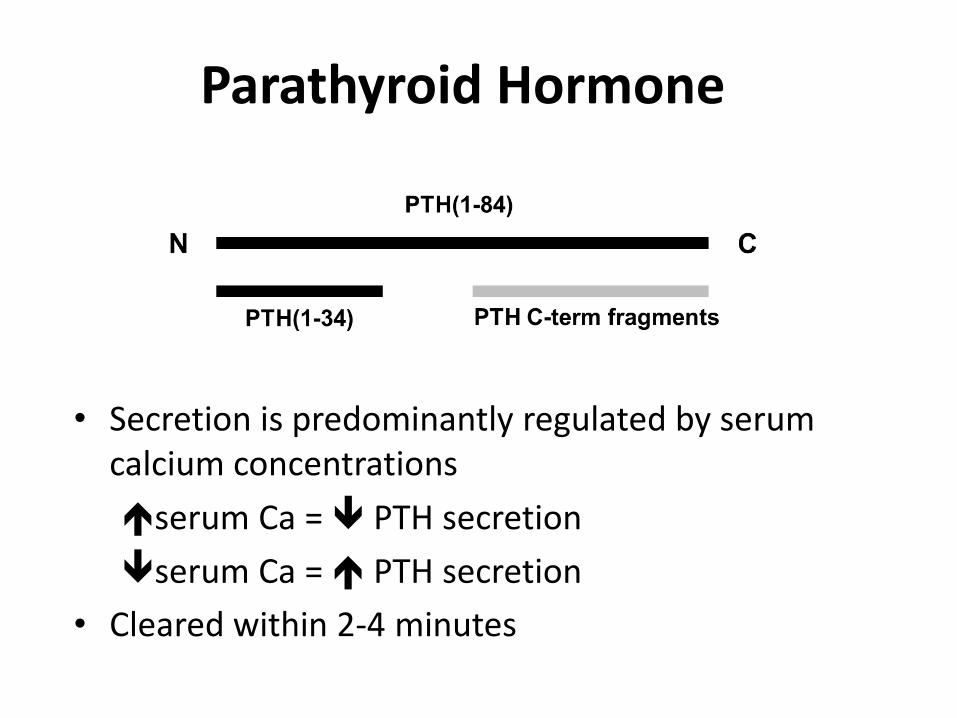
Parathyroid Hormone
• Secretion is predominantly regulated by serum calcium concentrations
serum Ca = PTH secretion
serum Ca = PTH secretion
• Cleared within 2-4 minutes

Parathyroid Hormone Regulation
• Calcium sensing receptor (CaSr) – cell surface receptor that senses extracellular calcium
– found in parathyroid glands and kidney
• Binding of Ca to CaSR inhibits PTH secretion and level of PTH mRNA
• Familial Hypocalciuric Hypercalcemia (FHH):inactivating mutation of the CaSR – higher set point for calcium sensing

Kidney: Stimulate 1,25(OH)2D production
Stimulate Calcium Reabsorption
Block Phosphate Reabsorption
Bone: Activate Osteoclastic Resorption (acute)
Activate Osteoblastic Bone Formation
(subacute, chronic)
Intestine:Activate Calcium Transport (indirect via
1,25(OH)2D)
Actions of PTH
Modified from Stewart AF, Cecil Essentials of Medicine 8th ed, 772-778
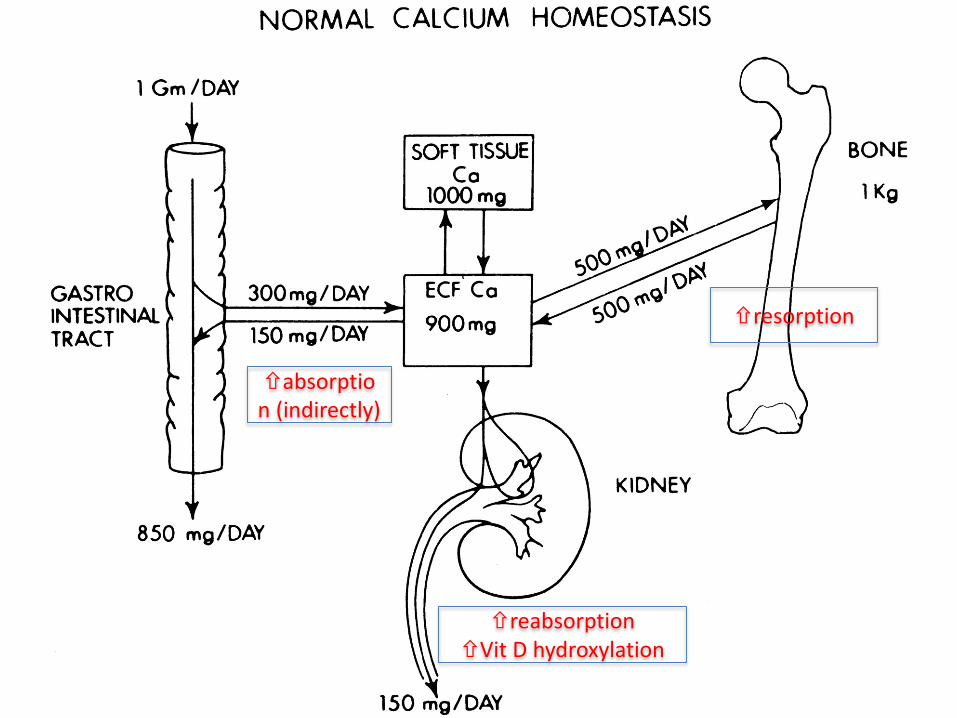
absorption (indirectly)
resorption
reabsorptionVit D hydroxylation
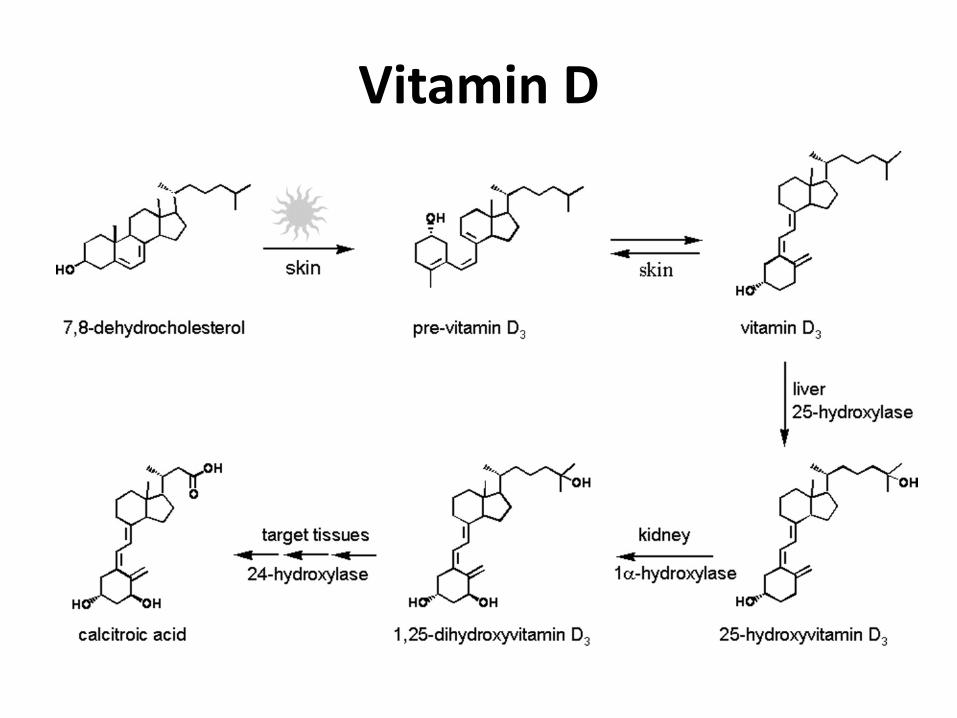
Vitamin D
• Wide range of other biologic actions: inhibits cellular proliferation and angiogenesis, stimulates insulin production, inhibits renin production, stimulates macrophages
• 25 (OH) D major circulating formbest indicator of vitamin D status
1,000 X > concentration than 1,25 (OH)2D
• Deficiency: children => rickets, adults => Osteomalacia
Vitamin D
Vitamin D Supplementation
• Vitamin D2 (ergocalciferol) => plant source
• Vitamin D3 (cholecalciferol) => animal source
• Recent data that D3 is more effective at raising serum vitamin D levels compared to D2
How Much Vitamin D Do We Need?
Depends on who you ask
• IOM – provides guidance for dietary standards in the general public, used by government to set dietary regulations
• Endocrine Society Practice guidelines –intended for use by clinicians who have patients who are at risk for deficiency
• Goal: Serum 25 Vitamin D > 30 ng/ml

Hyperparathyroidism
HYPERCALCEMIAAKA ‘DOC I’M TIRED ALL THE TIME’
Hypercalcemia
• Corrected total or ionized calcium > 2 SD above normal mean (10.2-10.5 mg/dl or 1.13-1.29 mM)
• No formal grading criteria for severity:
<12.0 mg/dl => mild
12-14 mg/dl => moderate
> 14.0 mg/dl => severe
• Serum Calcium:40-50 % ionized (active)40-45% bound to albumin10 % bound to citrate
• Total calcium varies with alterations in binding proteins, specifically albumin
• Corrected calcium should be used for decision making
Corrected Total Ca+ = Measured Ca+ mg/dl + 0.8 ( 4.0 – measured albumin)
Hypercalcemia
Manifestations of Hypercalcemia
Signs and symptoms depend on severity and rapidity of onset
• electrical gradient across a cell
• depolarization potential
• response to chemical or neural stimulus
• Neurologic:– Fatigue => obtunded => coma– Influenced by rate of onset, age, baseline MS– Seizures (cerebral vasoconstriction)
• Renal:– Polyuria => thirst and dehydration
• Calcium directly inhibits H2O reabsorption due to osmotic diuresis• Calcium inhibits ADH effect on distal nephron = nephrogenic DI
– Nephrocalcinosis = deposition of Ca-Phos salts in renal interstitium
– Hypercalciuria => nephrolithiasis– Renal insufficiency or failure over time
Manifestations of Hypercalcemia
• Cardiovascular:– Shortened QTc interval: deposition of Ca-Phos in
cardiac conduction system
– Arteriolar vasoconstriction
• Musculo-skeletal:– Skeletal muscle weakness: contractility
• Gastrointestinal:– Constipation, nausea, vomiting, ileus (due to smooth
muscle hypoactivity)
– Pancreatitis: calcium deposits within pancreas
Manifestations of Hypercalcemia
Check PTH
PTH
Primary Hyperparathyroidism
Tertiary Hyperparathyroidism
Parathyroid Carcinoma
FHH
PTH
Everything Else
Differential Diagnosis of Hypercalcemia
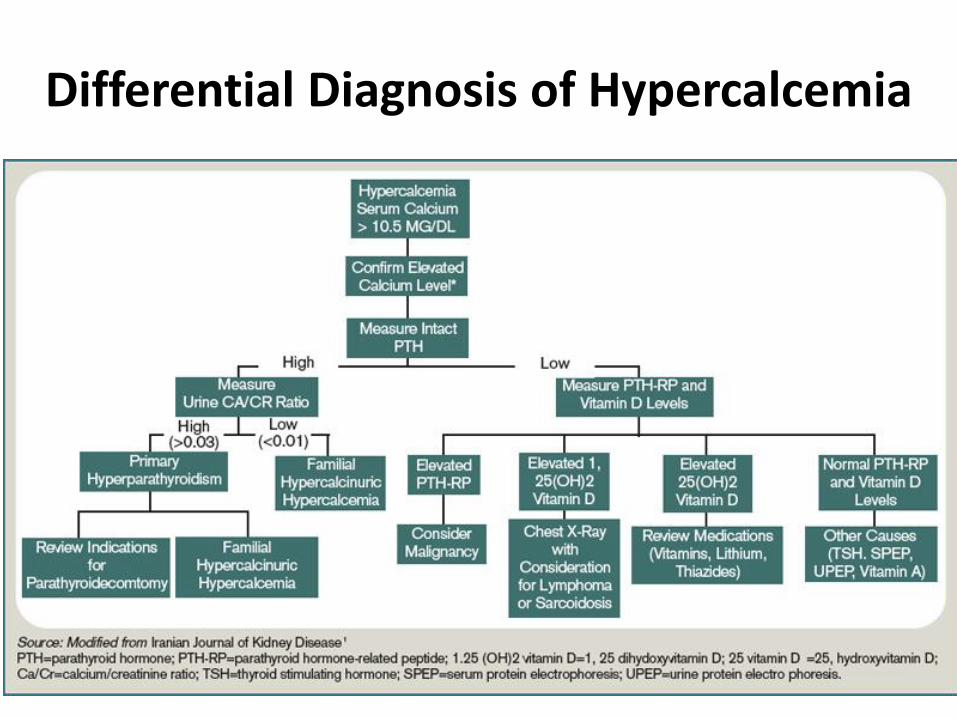
Differential Diagnosis of Hypercalcemia
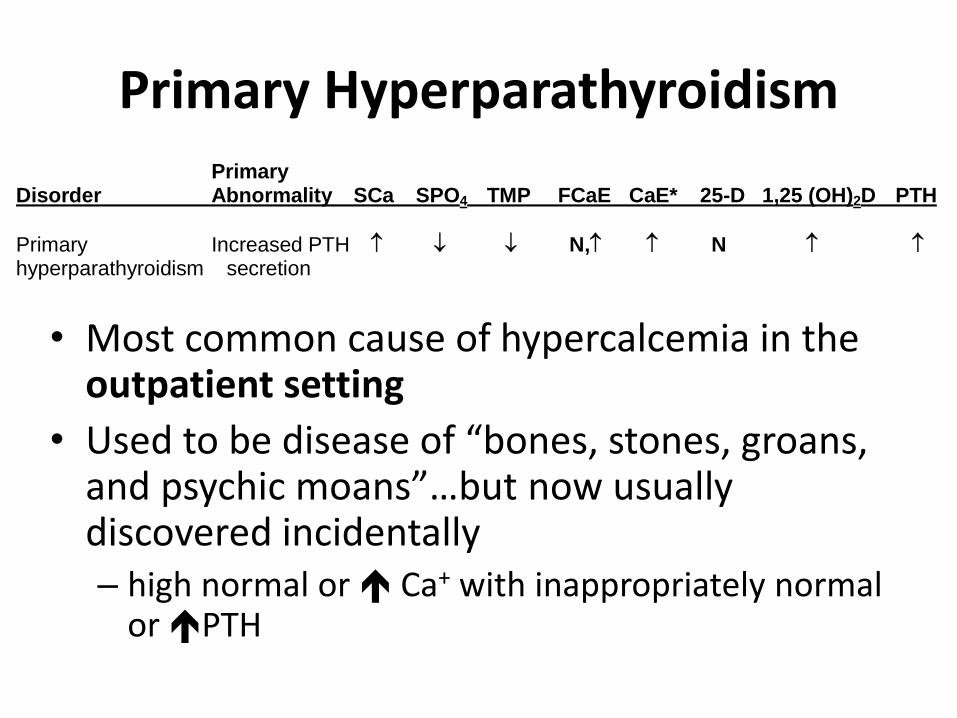
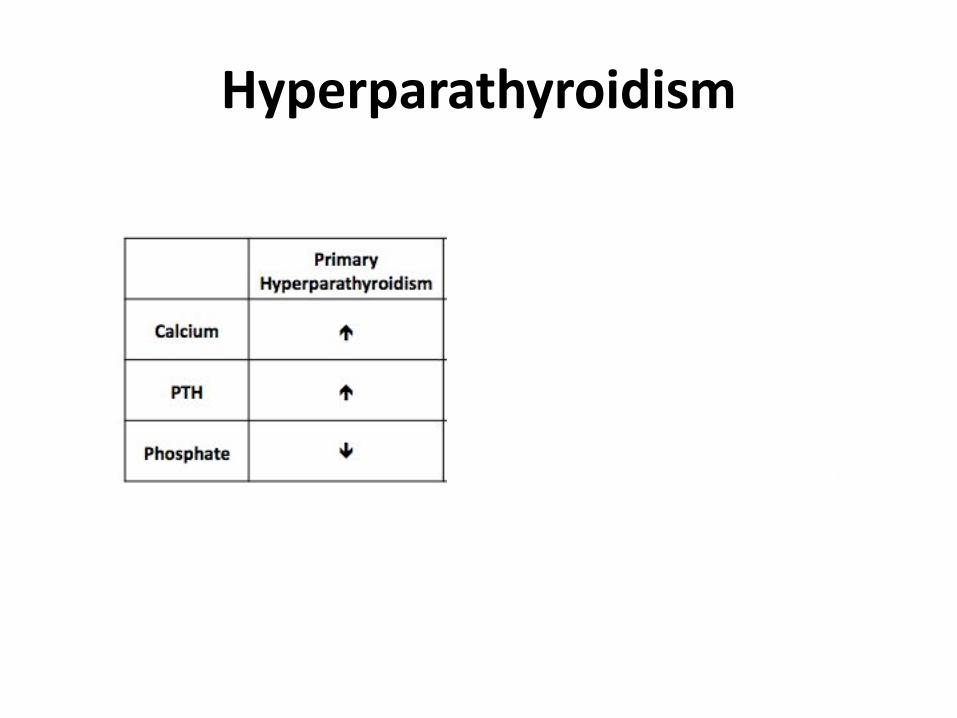
Primary Hyperparathyroidism Primary Disorder Abnormality SCa SPO4 TMP FCaE CaE* 25-D 1,25 (OH)2D PTH
Primary Increased PTH N, N hyperparathyroidism secretion
• Most common cause of hypercalcemia in the outpatient setting
• Used to be disease of “bones, stones, groans, and psychic moans”…but now usually discovered incidentally– high normal or Ca+ with inappropriately normal
or PTH
• Caused by over secretion of PTH by parathyroid gland – loss of normal feedback of PTH by serum calcium– 85% benign solitary parathyroid adenoma
– 15% hyperplasia of two or more parathyroid glands• Consider hereditary endocrine disorders: MEN I and
MEN II
– Rare parathyroid carcinoma (1.25 cases per 10 million)
Primary Hyperparathyroidism
• Most patients are asymptomatic with mild elevated Ca+ = 10.2-10.8 mg/dl
• Symptoms => same as Ca, bone pain
• Evaluation:– Serum calcium, albumin, phosphorous, creatinine,
PTH, 25 OH vitamin D (correct if low)
– 24 urine calcium and creatinine
– DXA scan (with forearm BMD)
• Imaging: Order sestamibi scan (+/- SPECT) only after diagnosis is confirmed biochemically
Primary Hyperparathyroidism
• Definitive treatment is surgical
• Refer to an experienced surgeon!
• Who is a surgical candidate?
– Any symptomatic patient
– Asymptomatic patients with any of the following:
• Age <50
• Serum total calcium ≥1.0 mg/dl above ULN
• T-score ≤ -2.5 SD at any site or vertebral fracture
• Cr clearance < 60cc/min, Ur Ca >400 mg/d and high biochemical stone risk, presence of nephrolithiasis or nephrocalcinosis
Primary Hyperparathyroidism: Management
Bilezikian JP, JCEM 2014.
• Antiresorptives (bisphosphonates) for low bone density
• Calcimimetic (cinacalcet) symptomatic or severe hypercalcemia in non-surgical candidate
• Yearly monitoring for those with mild disease– S Calcium, albumin, phosphorous , PTH, 25 OH Vit D
– Urine calcium and creatinine if indicated
– BMD every 1-2 years (include distal radius)
Primary Hyperparathyroidism: Medical Management

Check PTH
PTH
Primary Hyperparathyroidism
Tertiary Hyperparathyroidism
Parathyroid Carcinoma
PTH
Everything Else
Differential Diagnosis of Hypercalcemia
• Familial Hypocalciuric Hypercalcemia• Malignancy associated hypercalcemia• Granulomatous disorders (lymphoma, sarcoidosis)
• Endocrine disorders (hyperthyroidism, Addison’s, Pheochromocytoma)
• Milk alkali syndrome • Immobilization (among adolescents, Paget’s)
• Acute Renal Failure• TPN/hyperproteinemia• End Stage Liver Disease• Medications
Non-PTH Mediated Hypercalcemia
Malignancy Associated Hypercalcemia
• Most common cause of hypercalcemia in inpatient setting
• Common cause of death among cancer patients: – severe hypercalcemia leads to coma and renal failure– Breast, lung, renal, ovarian, hematologic
• Secretion of Parathyroid hormone-related protein (PTHrP) causing humoral hypercalcemia of malignancy
• Skeletal metastases – cytokine mediated osteoclasticbone destruction
• Lymphomas can make 1,25 (OH)2 Vitamin D• Rare tumors make ectopic PTH
Malignancy Associated Hypercalcemia:Treatment
• Treat underlying malignancy
• Acute management:
– Vigorous intravenous hydration
– Loop diuretics only to prevent CHF
– Calcitonin
• Often responds acutely to meds that block bone resorption
– IV Bisphosphonates: Zoledronate or Pamidronate
Sarcoidosis
• Granulomatous disease: giant granuloma cells multiple organs
• Prototype of hypercalcemia associated with granulomatous diseases
• Occurs in 10% of sarcoid patients
• 1,25 (OH)2 D production by macrophages and giant cells => intestinal hyperabsorption of calcium
• Lesser extent – renal calcium absorption and osteoclastic bone resorption
• Treatment: Glucocorticoids
Medications
• Hypervitaminosis A
• Hypervitaminosis D
• Thiazide diuretics
• Lithium
• Estrogens, androgens
• Tamoxifen

HYPOCALCEMIAAKA ‘DOC I’M TINGLING ALL OVER’
Hypocalcemia
• Corrected total or ionized calcium < 2 SD below normal mean (<8.5 mg/dl = <1.16 mM)
• As with hypercalcemia, total calcium needs to be corrected for albumin when assessing hypocalcemia
• Evaluation includes measurement of:
– Serum calcium, albumin
– Serum ionized Ca, Mg, Phos, PTH, and 25 OH Vit D
Manifestations of Hypocalcemia
Signs and symptoms depend on severity and rapidity of onset
• electrical gradient across a cell
• depolarization potential
• response to chemical or neural stimulus => hyperexcitability
• Neurologic:
– Fatigue, seizures, perioral numbness, tingling
– Basal ganglia and intra-cerebral calcifications
• Cardio-vascular:
– Prolonged QTc interval, arrhythmias
– CHF
– Cardiomyopathy
Manifestations of Hypocalcemia
• Musculo-skeletal:– Muscle twitches, cramps, tetany
– Chvostek’s sign => twitching of facial muscle
– Trousseau’s sign => spasms of forearm with BP cuff > systolic
• Gastrointestinal:– Cramping
• Other:– Bronchospasm
– Cataracts
Manifestations of Hypocalcemia

Differential Diagnosis of Hypocalcemia
• Hypoparathyroidism• Psuedohypoparathyroidism• Vitamin D Disorders• Hypoalbuminemia• Magnesium disorders• Rapid Bone formation• Hyperphosphatemia• Medications• Pancreatitis
Hypoparathyroidism
• Rare, results from no or little PTH
– low ionized calcium with low PTH
– Phos often elevated early in disease
– Low 1,25 (OH)2 vitamin D
• Result is hypocalcemia that is often symptomatic at onset
• Etiology
– Surgical
– Idiopathic/Autoimmune
– Infiltrative diseases – Wilson’s, hemochromatosis
– Congenital
Hypoparathyroidism: Treatment
• One of the few endocrine disorders that has previously not been treated with replacement hormone
• 2 main components of therapy:
– Calcium supplementation (~2 gm a day)
– 1,25 (OH)2 vitamin D (rocaltrol, calcitriol)
• Important to monitor serum and urine calcium closely to avoid calcium-phosphate precipitation
• Recombinant PTH 1-84 recently (2015) approved for treatment of long-standing severe hypoparathyroidism
Severe Hypocalcemia Among Inpatients
Treat with IV calcium if:Symptomatic (carpopedal spasm, tetany, seizures)QT prolongationAcute hypocalcemia, corrected Ca <7.5 mg/dL• Administer IV calcium gluconate (mix 1 amp with 50
mL D5 to avoid hypotension and bradycardia)• Start calcium gluconate infusion (11 amps in 890mL NS
= 1 mg/mL elemental Ca) 50 mL/hr• Start oral calcium carbonate 2 gm TID• Start calcitriol 0.25 mcg BID• Treat hypomagnesemia and monitor Ca closely
QUESTIONS?
Have you tried Googling that?