Embed Size (px)
Citation preview
Brief Cogni+ve Assessment Tool (BCAT®) Training Program Presented by Dr. William Mansbach CEO & Founder, Mansbach Health Tools, LLC [email protected] www.thebcat.com
1
Proficiency in the cogniBve assessment of persons who have a subjecBve or objecBve memory or cogniBve complaint is criBcally important to effecBve diagnosis, treatment, educaBon, and support. The primary goal of this program is to equip you with the knowledge and skills necessary to be proficient in administering, scoring, and interpreBng the BCAT.
Cer+fied BCAT Trainer
INTRODUCTION TO BCAT 2
Program Objec+ves
Be able to administer, score, and interpret the BCAT Be able to apply BCAT scores to clinical care Understand the strengths and limitaBons of cogniBve screening tools Understand basic neuro-‐cogniBve structure-‐funcBon concepts
3 INTRODUCTION TO BCAT
Course Outline
The basics of primary neuro-‐cogniBve domains in everyday living The uBlity of cogniBve screening tools Commonly used cogniBve screening tools The BCAT and BCAT System of tests
4 INTRODUCTION TO BCAT
Neuro-‐Cogni+ve Domains
5
The basics of primary neuro-‐cogni+ve domains in everyday living
Structure-‐funcBon Neurons Basic brain structures
NEURO-‐COGNITIVE DOMAINS 6
Basic Brain Structures
Whole Brain
7 NEURO-‐COGNITIVE DOMAINS
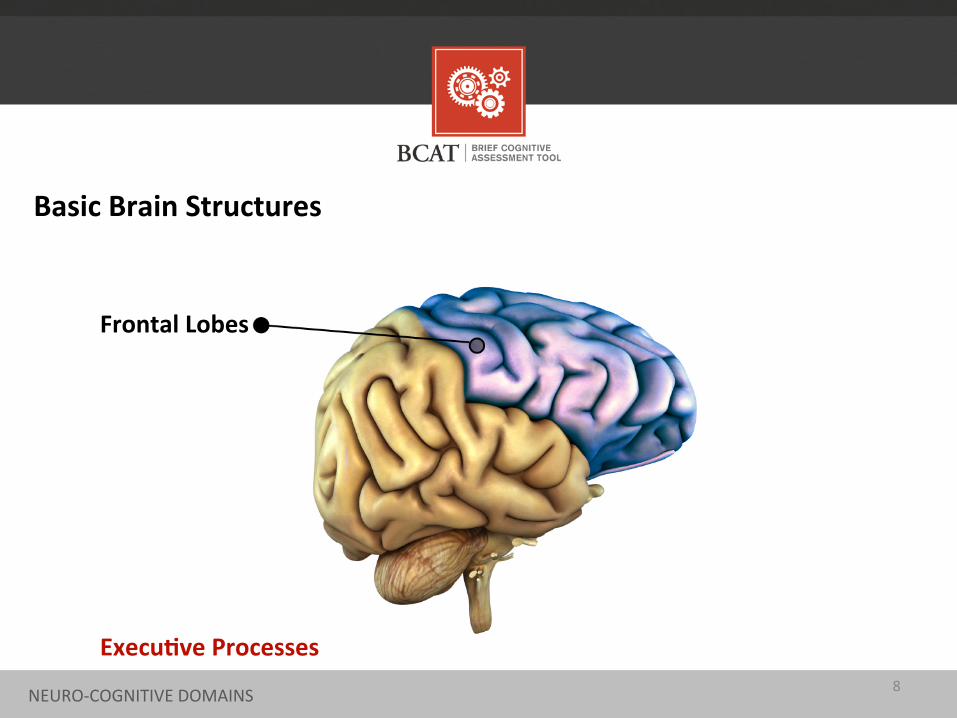
Basic Brain Structures
Frontal Lobes
Execu+ve Processes 8 NEURO-‐COGNITIVE DOMAINS
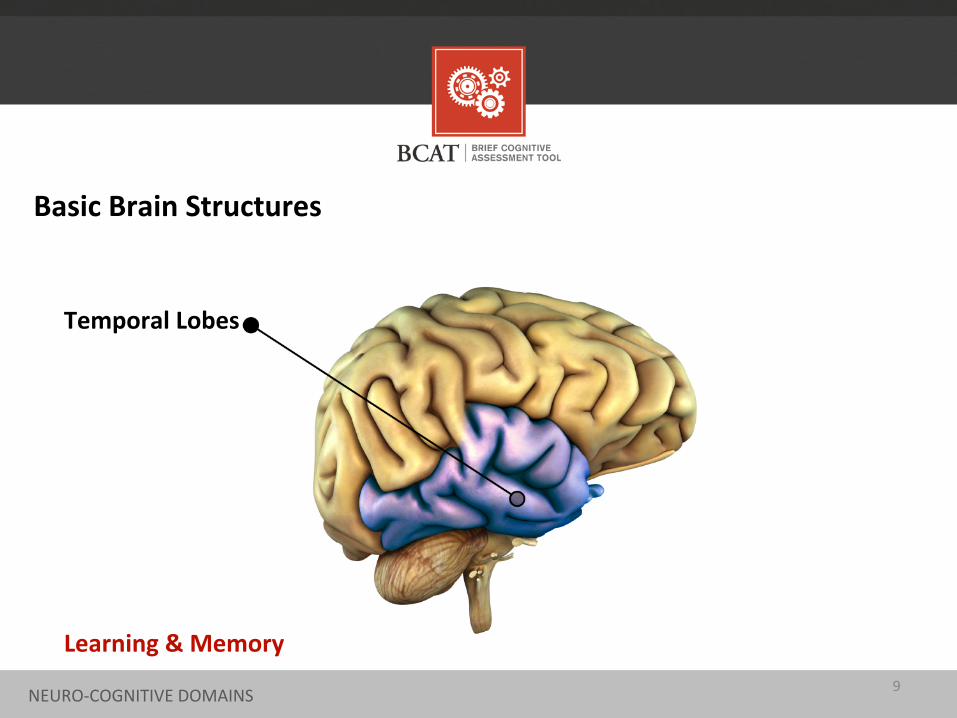
Basic Brain Structures
Temporal Lobes
Learning & Memory 9 NEURO-‐COGNITIVE DOMAINS
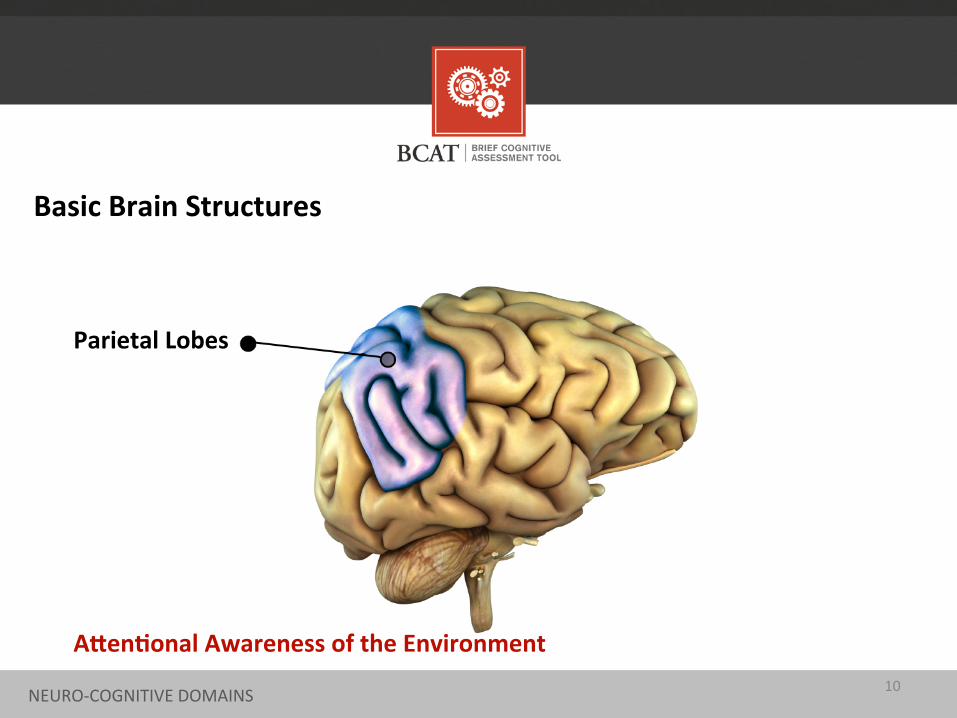
Basic Brain Structures
Parietal Lobes
AMen+onal Awareness of the Environment 10 NEURO-‐COGNITIVE DOMAINS
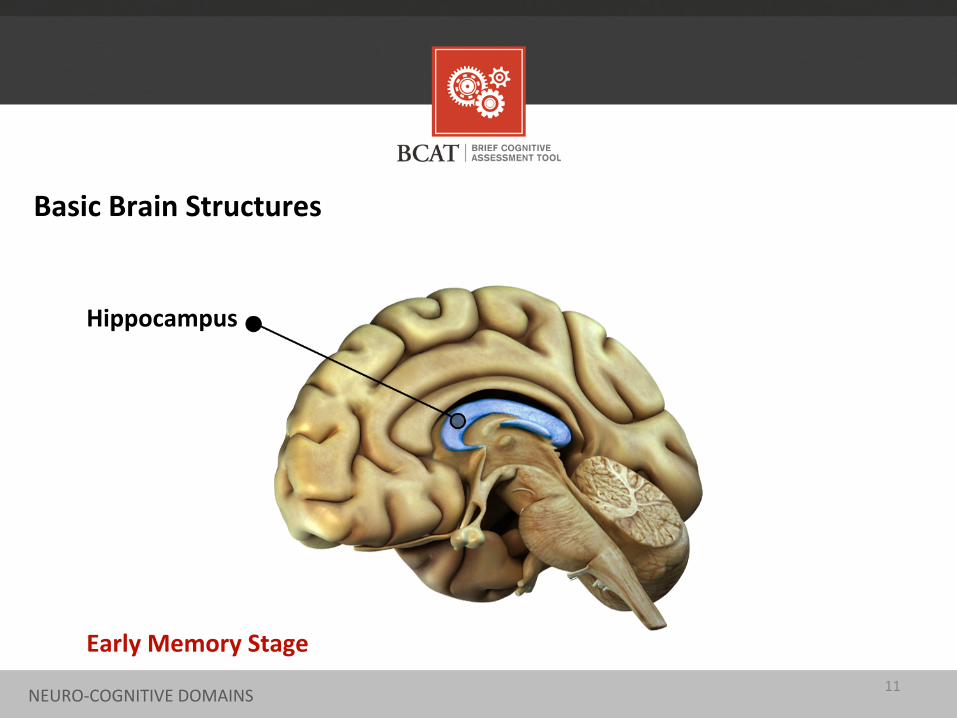
Basic Brain Structures
Hippocampus
Early Memory Stage 11 NEURO-‐COGNITIVE DOMAINS
Contextual memory The case of story recall
ExecuBve funcBons The case for execuBve controls
A_enBonal capacity The case for a_enBon as “the oil”
The Three Central Cogni+ve Domains (The Cogni+ve Task Manager)
12 NEURO-‐COGNITIVE DOMAINS
U+lity of Cogni+ve Screening Tools
13
We have an aging society with associated problems. As people live longer, the incidence/prevalence of demenBa rates increase. Over 5 million people have Alzheimer’s disease (AD), anBcipated to be 13 million by 2050. Numbers are vastly greater if you include other demenBas and people with Mild CogniBve Impairment (MCI).
UTILITY OF COGNITIVE SCREENING TOOLS
The u+lity of cogni+ve screening tools
14
U.S. PrevenBve Services Task Force Statement RouBne screening versus screening when there is a subjecBve or objecBve memory complaint Age as risk factor and screening for people over 80 The special case of MCI and demenBa conversion (10-‐15% annually)
When to use screening tools
15 UTILITY OF COGNITIVE SCREENING TOOLS
• Aide in diagnosis • Early recogniBon enhances efficacy of treatments • Improve disease management and planning • IdenBfy funcBonal issues • Manage expectaBons of paBents, families, providers, staff • Time and cost effecBve • Lowers paBent resistance and encourages compliance
Uses of screening tools
16 UTILITY OF COGNITIVE SCREENING TOOLS
What should a good cogni+ve screening tool be able to do?
• Administered by professionals and techs • Completed in less than 15 minutes
(someBmes five minutes) • Able to differenBate between MCI and demenBa • Broadly assess memory skills • Broadly assess execuBve skills • Assess a_enBonal skills • Predict ADLs & IADLs
17 UTILITY OF COGNITIVE SCREENING TOOLS
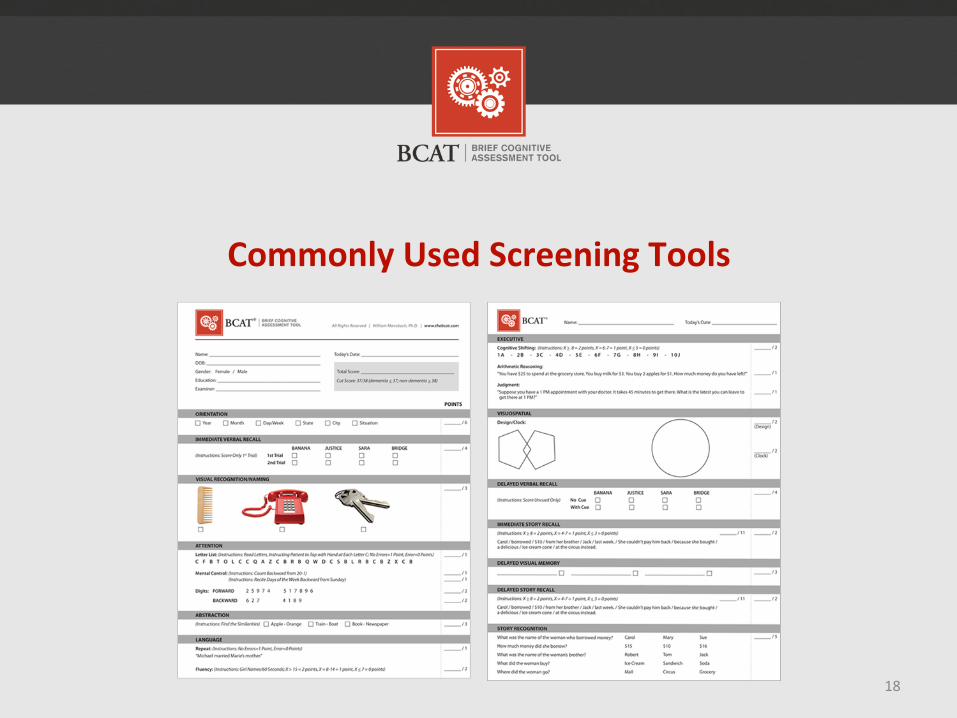
Commonly Used Screening Tools
18
Mini-‐Mental State ExaminaBon (MMSE) Short Test of Mental Status (STMS) Montreal CogniBve Assessment (MoCA) Saint Louis University Mental Status ExaminaBon (SLUMS) Brief CogniBve Assessment Tool (BCAT) & BCAT-‐SF
COMMONLY USED SCREENING TOOLS
Commonly used cogni+ve screening tools
19
• The first major screening instrument • SensiBve for moderate to severe demenBa • Less sensiBve for MCI and mild demenBa • EducaBon bias (overesBmates for those with
li_le educaBon) • Weak on memory and execuBve funcBons • Floor effect
MMSE (Folstein, Folstein, & McHugh, 1975)
20 COMMONLY USED SCREENING TOOLS
• Verbal features are more complex than MMSE • RelaBvely poor sensiBvity to MCI
STMS (Kokmen et al., 1987)
21 COMMONLY USED SCREENING TOOLS
• SensiBve to cogniBve spectrum • Designed primarily for frontline providers • RelaBvely weak on memory • No story recall component • Stronger on execuBve funcBons, but no complex
reasoning item
MoCA (Nasreddine et al., 2005)
22 COMMONLY USED SCREENING TOOLS
• SensiBve to cogniBve spectrum • Designed primarily for frontline providers • Has a story recall, but no free recall or delayed
recall • Has complex reasoning, but no cogniBve
set-‐shiming
SLUMS (Tariq et al., 2006)
23 COMMONLY USED SCREENING TOOLS
• Four studies, starBng in 2005 • 21 items, 50 maximum points • 10-‐15 minutes in administraBon • Has a MCI versus demenBa “cut” score (37/38) • Has score ranges for cogniBve categories • Has three cogniBve “clusters” • Predicts ADL & IADL • Website-‐based scoring program
BCAT (Mansbach, MacDougall, & Rosenzweig 2012)
24 COMMONLY USED SCREENING TOOLS
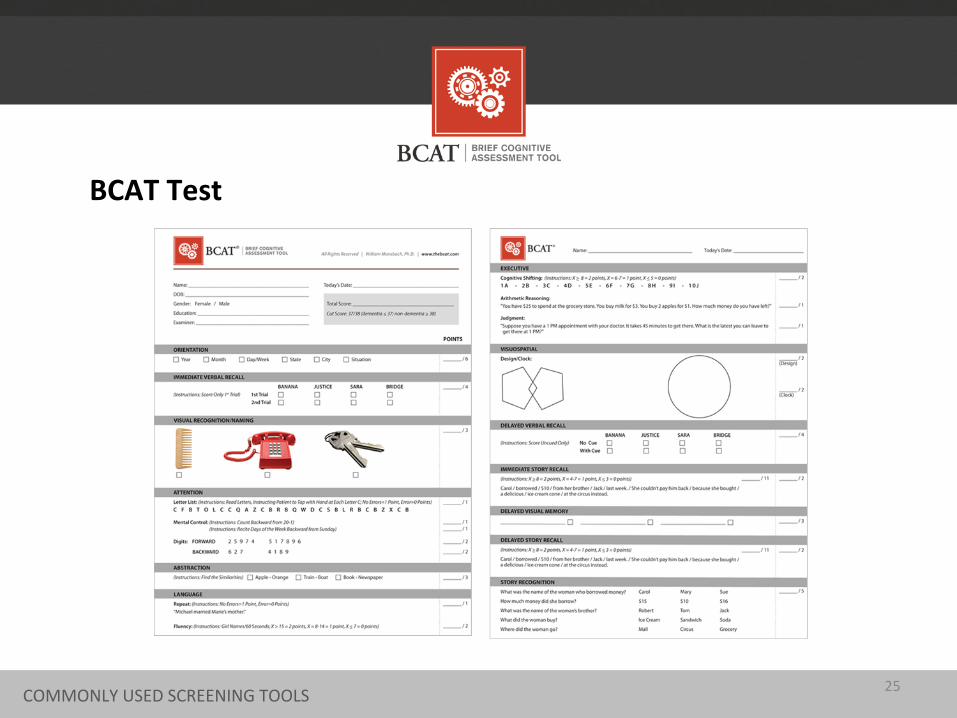
BCAT Test
25 COMMONLY USED SCREENING TOOLS
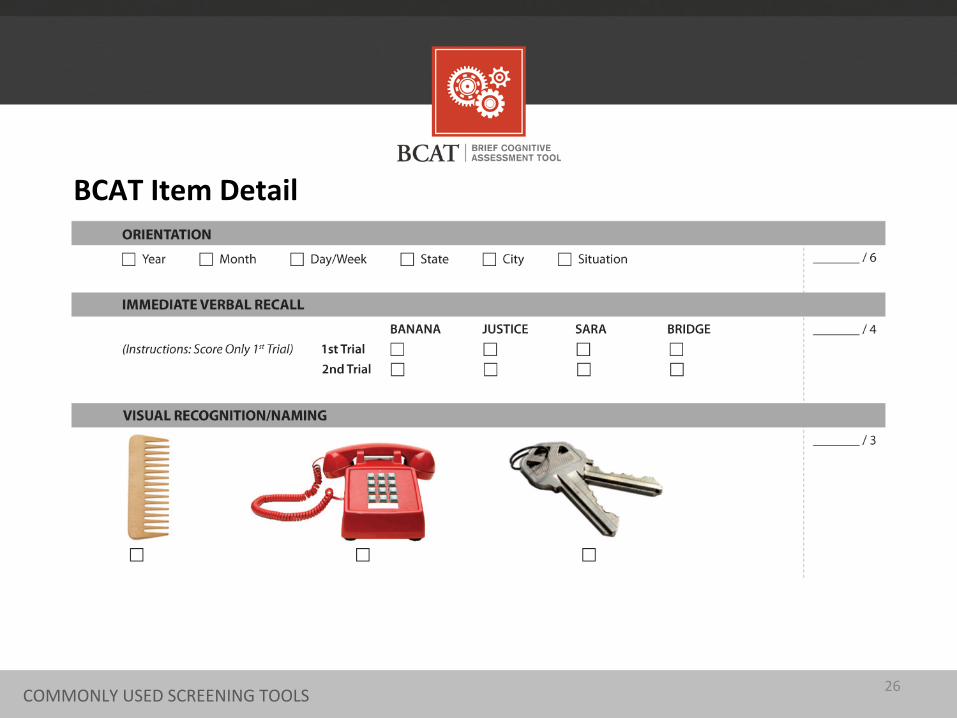
BCAT Item Detail
26 COMMONLY USED SCREENING TOOLS
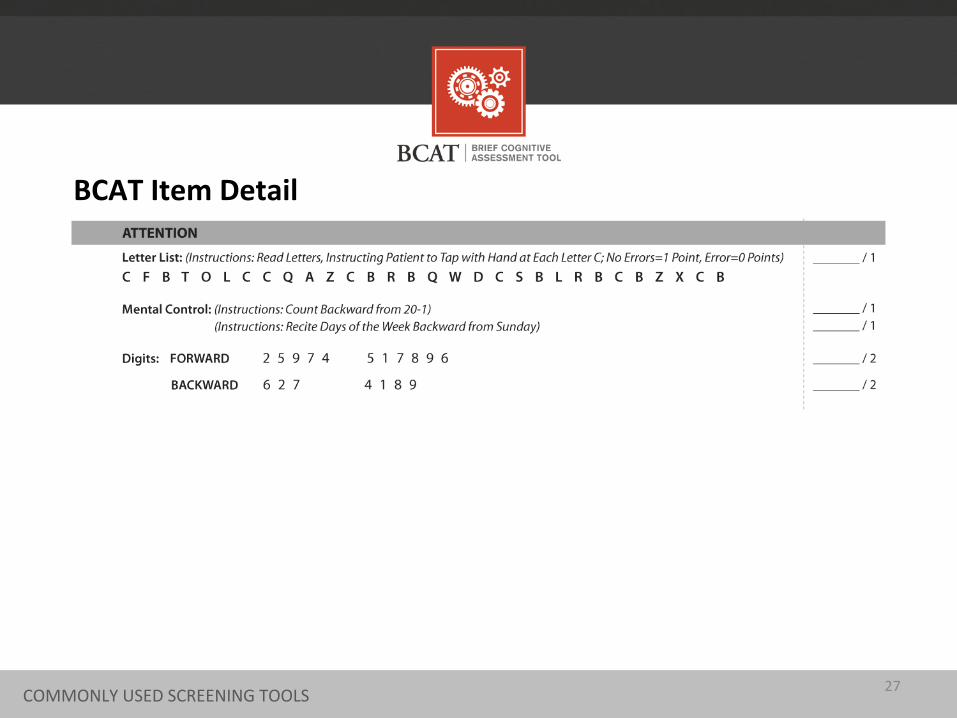
BCAT Item Detail
27 COMMONLY USED SCREENING TOOLS
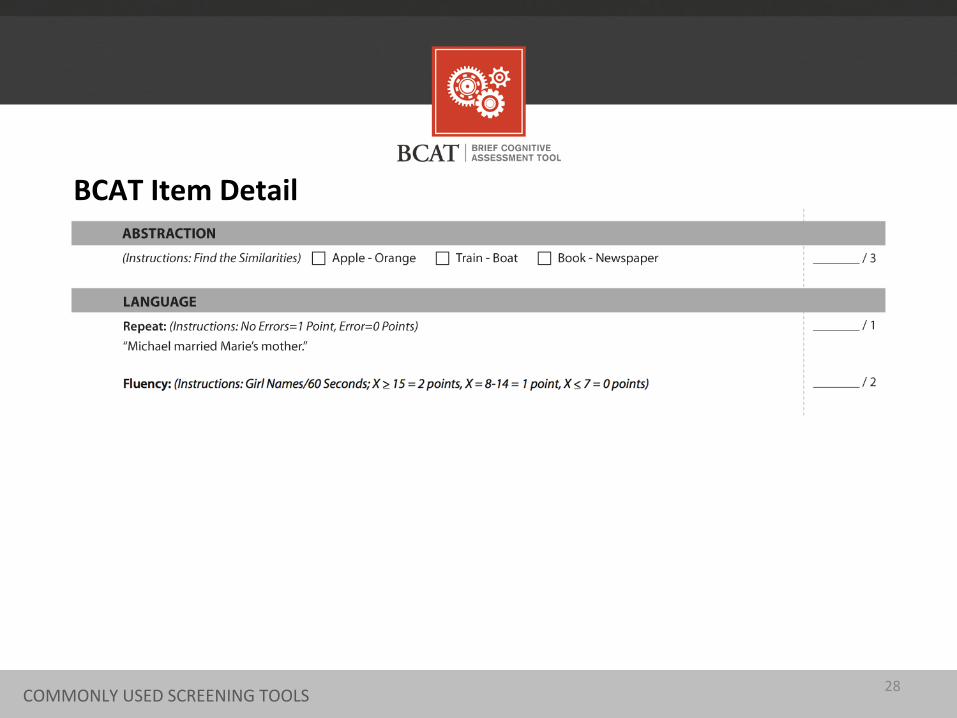
BCAT Item Detail
28 COMMONLY USED SCREENING TOOLS 28 COMMONLY USED SCREENING TOOLS
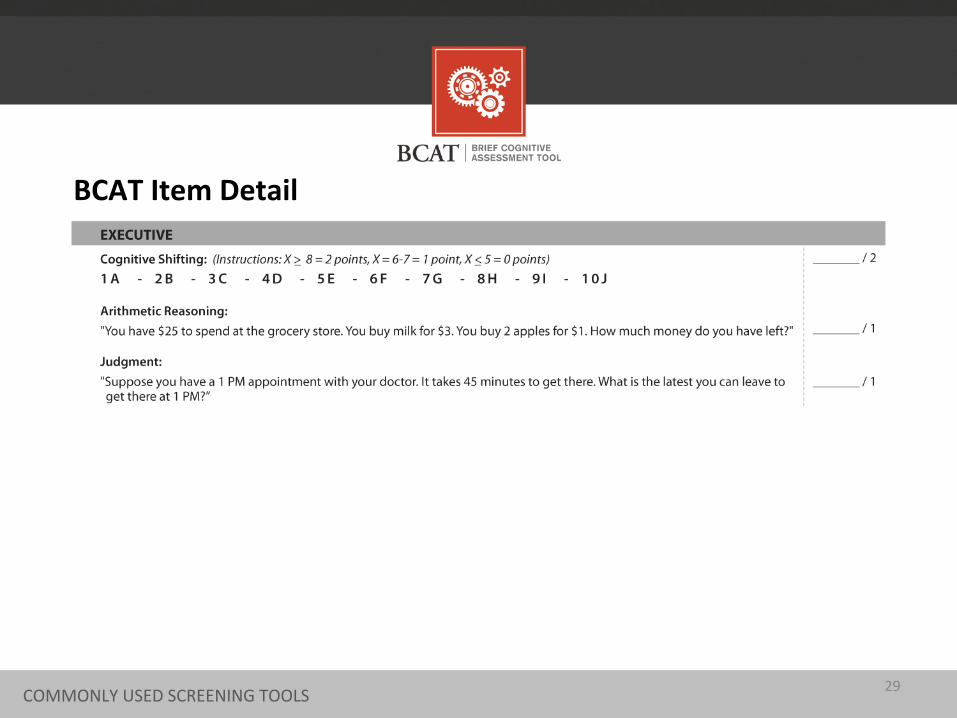
BCAT Item Detail
29 COMMONLY USED SCREENING TOOLS
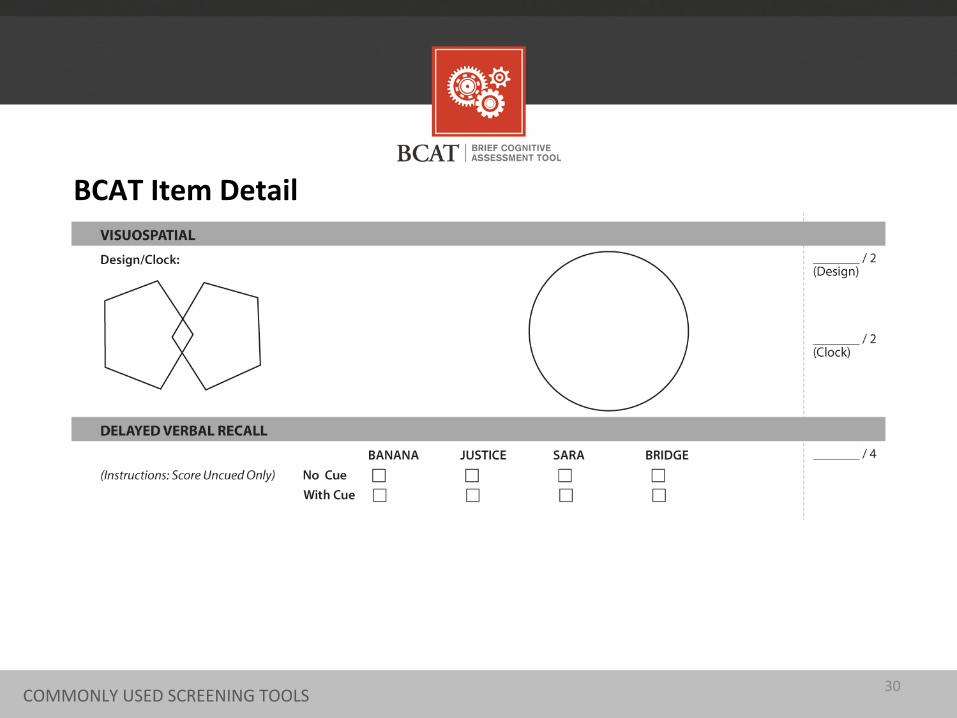
BCAT Item Detail
30 COMMONLY USED SCREENING TOOLS
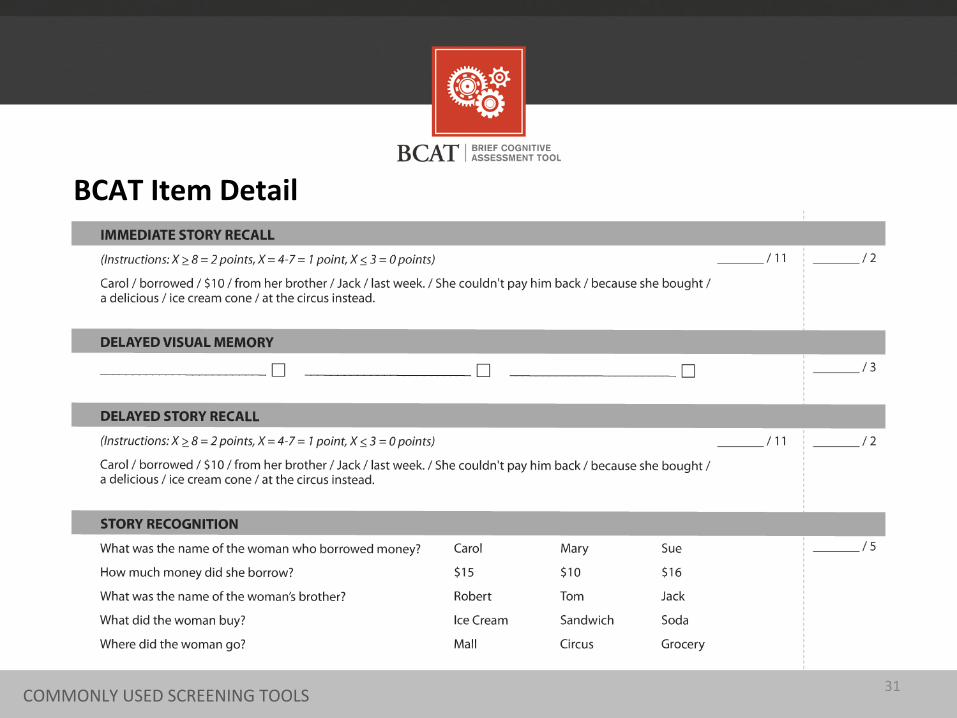
BCAT Item Detail
31 COMMONLY USED SCREENING TOOLS
BCAT Scoring Program
32
Computer-‐assisted scoring Total score & Factor scores Clinical consideraBons Report that can be printed and/or emailed
BCAT SCORING PROGRAM
BCAT Scoring & Interpre+ng
33
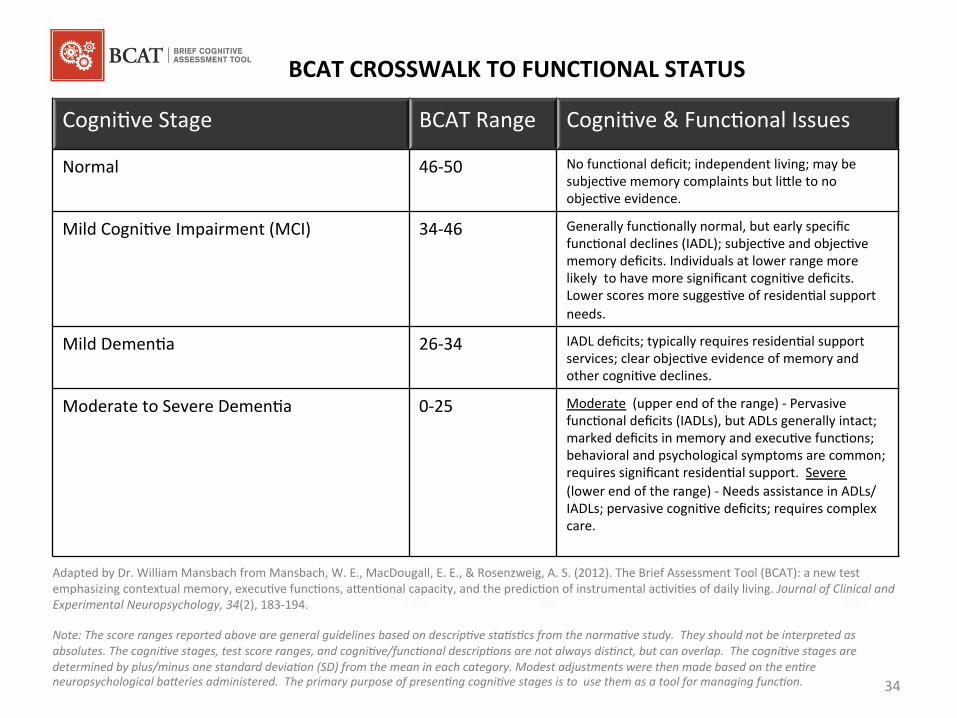
BCAT CROSSWALK TO FUNCTIONAL STATUS
CogniBve Stage BCAT Range CogniBve & FuncBonal Issues
Normal 46-‐50 No funcBonal deficit; independent living; may be subjecBve memory complaints but li_le to no objecBve evidence.
Mild CogniBve Impairment (MCI)
34-‐46 Generally funcBonally normal, but early specific funcBonal declines (IADL); subjecBve and objecBve memory deficits. Individuals at lower range more likely to have more significant cogniBve deficits. Lower scores more suggesBve of residenBal support needs.
Mild DemenBa
26-‐34 IADL deficits; typically requires residenBal support services; clear objecBve evidence of memory and other cogniBve declines.
Moderate to Severe DemenBa
0-‐25 Moderate (upper end of the range) -‐ Pervasive funcBonal deficits (IADLs), but ADLs generally intact; marked deficits in memory and execuBve funcBons; behavioral and psychological symptoms are common; requires significant residenBal support. Severe (lower end of the range) -‐ Needs assistance in ADLs/IADLs; pervasive cogniBve deficits; requires complex care.
Adapted by Dr. William Mansbach from Mansbach, W. E., MacDougall, E. E., & Rosenzweig, A. S. (2012). The Brief Assessment Tool (BCAT): a new test emphasizing contextual memory, execuBve funcBons, a_enBonal capacity, and the predicBon of instrumental acBviBes of daily living. Journal of Clinical and Experimental Neuropsychology, 34(2), 183-‐194. Note: The score ranges reported above are general guidelines based on descripCve staCsCcs from the normaCve study. They should not be interpreted as absolutes. The cogniCve stages, test score ranges, and cogniCve/funcConal descripCons are not always disCnct, but can overlap. The cogniCve stages are determined by plus/minus one standard deviaCon (SD) from the mean in each category. Modest adjustments were then made based on the enCre neuropsychological baLeries administered. The primary purpose of presenCng cogniCve stages is to use them as a tool for managing funcCon. 34
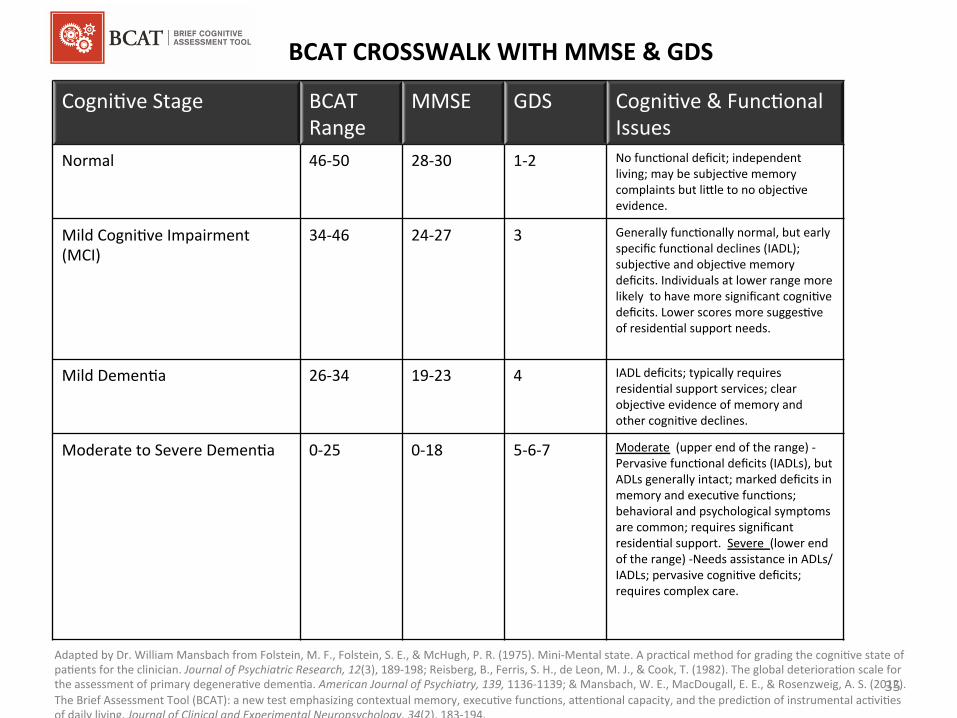
BCAT CROSSWALK WITH MMSE & GDS
CogniBve Stage BCAT Range
MMSE GDS CogniBve & FuncBonal Issues
Normal 46-‐50 28-‐30 1-‐2
No funcBonal deficit; independent living; may be subjecBve memory complaints but li_le to no objecBve evidence.
Mild CogniBve Impairment (MCI)
34-‐46 24-‐27 3
Generally funcBonally normal, but early specific funcBonal declines (IADL); subjecBve and objecBve memory deficits. Individuals at lower range more likely to have more significant cogniBve deficits. Lower scores more suggesBve of residenBal support needs.
Mild DemenBa
26-‐34 19-‐23
4
IADL deficits; typically requires residenBal support services; clear objecBve evidence of memory and other cogniBve declines.
Moderate to Severe DemenBa
0-‐25 0-‐18
5-‐6-‐7
Moderate (upper end of the range) -‐ Pervasive funcBonal deficits (IADLs), but ADLs generally intact; marked deficits in memory and execuBve funcBons; behavioral and psychological symptoms are common; requires significant residenBal support. Severe (lower end of the range) -‐Needs assistance in ADLs/IADLs; pervasive cogniBve deficits; requires complex care.
Adapted by Dr. William Mansbach from Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). Mini-‐Mental state. A pracBcal method for grading the cogniBve state of paBents for the clinician. Journal of Psychiatric Research, 12(3), 189-‐198; Reisberg, B., Ferris, S. H., de Leon, M. J., & Cook, T. (1982). The global deterioraBon scale for the assessment of primary degeneraBve demenBa. American Journal of Psychiatry, 139, 1136-‐1139; & Mansbach, W. E., MacDougall, E. E., & Rosenzweig, A. S. (2012). The Brief Assessment Tool (BCAT): a new test emphasizing contextual memory, execuBve funcBons, a_enBonal capacity, and the predicBon of instrumental acBviBes of daily living. Journal of Clinical and Experimental Neuropsychology, 34(2), 183-‐194. Note: The score ranges reported above are general guidelines based on descripCve staCsCcs from the normaCve study. They should not be interpreted as absolutes. The cogniCve stages, test score ranges, and cogniCve/funcConal descripCons are not always disCnct, but can overlap. The cogniCve stages are determined by plus/minus one standard deviaCon (SD) from the mean in each category. Modest adjustments were then made based on the enCre neuropsychological baLeries administered. The primary purpose of presenCng cogniCve stages is to use them as a tool for managing funcCon.
35
PracBcal recommendaBons Rehab focus Value of cogniBve exercises as determined by BCAT scores Brain fitness
It’s all about func+on
36 BCAT SCORING PROGRAM

For more informaBon about the BCAT Test System, visit www.TheBCAT.com.
37
UBlize the automated online BCAT test. Access the most current clinical research, news, and treatments about memory loss. Take advantage of conBnuing educaBon courses for healthcare professionals. Receive weekly emails with links to the Mind & Memory Blog and the latest arBcles for healthcare professionals.
It’s FREE to Register
Go to www.thebcat.com/register.php and register today!
38
BCAT Training Program Presented by Dr. William Mansbach CEO & Founder, Mansbach Health Tools, LLC [email protected] www.thebcat.com For more informaCon about becoming a BCAT Trainer, contact us at: [email protected]
39





























