Embed Size (px)
Citation preview
British Journal of Plastic Surgery (1982) 25, 452451 0 1982 The Trustees of British Association of Plastic Surgeons
0007-1226/82/0376-0452 $02.00
Breast reconstruction with a lower abdominal myocutaneous flap
ENRIQUE A. GANDOLFO
Plastic Surgery Service, Municipal. Cancer Hospital, Buenos Aires, Argentina
Summary-A new technique for breast reconstruction is presented using a lower abdominal myocutaneous flap based on one of the rectus abdominis muscles and the superior epigastric artery.
The sacrifice of the latissimus dorsi -muscle, the of them resulted in distal necrosis because of distress caused by ugly scars and the com- circulatory failure due to torsion of the pedicle. plications arising from existing procedures In seven cases a greater amount of tissue was spurred us to investigate another method of needed. In every case a large abdominal scar breast reconstruction. remained.
A technique is presented in which most of the tissue discarded in a conventional dermolipec- tomy is used as a myocutaneous flap of the lower abdominal wall. This large flap can be trans- ported by mobilisation of one of the rectus abdominis muscles with its superior epigastric artery. This procedure provides a myocutaneous flap which carries so much tissue that a pros- thesis is unnecessary. At the same time it leaves a far more acceptable aesthetic scar.
Nowadays breast reconstruction with myocuta- neous flaps based on the latissimus dorsi muscle (Bostwick et al., 1978) is a significant advance since it can be performed in one stage, with or without a prosthesis. We have used latissimus dorsi myocutaneous flaps in nine patients. In two cases with radionecrosis following mastectomy the flaps underwent necrosis of their distal portion with muscular atrophy.
Several authors (Pennisi, 1979; Schwartz, 1979) have written on breast reconstruction and studied factors such as timing, the patient’s wishes, age, tumour, histology and axillary lymph node in- volvement. In breast reconstruction where skin cover is adequate in amount and quality the insertion of a silicone prosthesis is usually sufli- cient. In radical mastectomy, however, skin cover is often poor and repair must include the intro- duction of cutaneous or myocutaneous tissues.
The most widely used techniques are based on thoraco-abdominal or abdominal cutaneous flaps (Gillies and Millard, 1957; Millard, 1976; Webster, 1937) but general surgeons often shun their use as their tailoring requires several stages and often produces ugly scars. If the cutaneous flaps are thin the defect can be compensated for by adding a prosthesis (Brown et al., 1975; Davies et al., 1977).
We have performed 12 breast reconstructions with simple vertical abdominal cutaneous flaps with an epigastric pedicle (Fernandez, 1968); five
Because of these problems, we sought for a better substitute for the “missing” breast. We investigated the blood supply in ten patients with horizontal dermolipectomies in W (Regnault, 1975) and the possibility of using one rectus abdominis muscle as the supporting pedicle for a lower abdominal myocutaneous flap. If the perforating vessels of both rectus abdominis muscles are preserved it is possible to maintain a good blood supply to the horizontal block of skin and subcutaneous usually discarded in a lower abdominal dermolipectomy. Division of the perforating vessels of one rectus abdominis muscle, however, provides a good blood supply to four-fifths of the flap with some venous stasis in the remaining fifth. We can, therefore, design with reasonable safety a large myocutaneous flap consisting of four-fifths of the tissue usually discarded in a dermolipectomy based on the perforating vessels of one rectus abdominis muscle, with its arteries and veins (perforating, inferior epigastric, superior epigastric and inter- nal mammary).
452
BREAST RECONSTRUCTION WITH A LOWER ABDOMINAL MYOCUTANEOUS FLAP 453
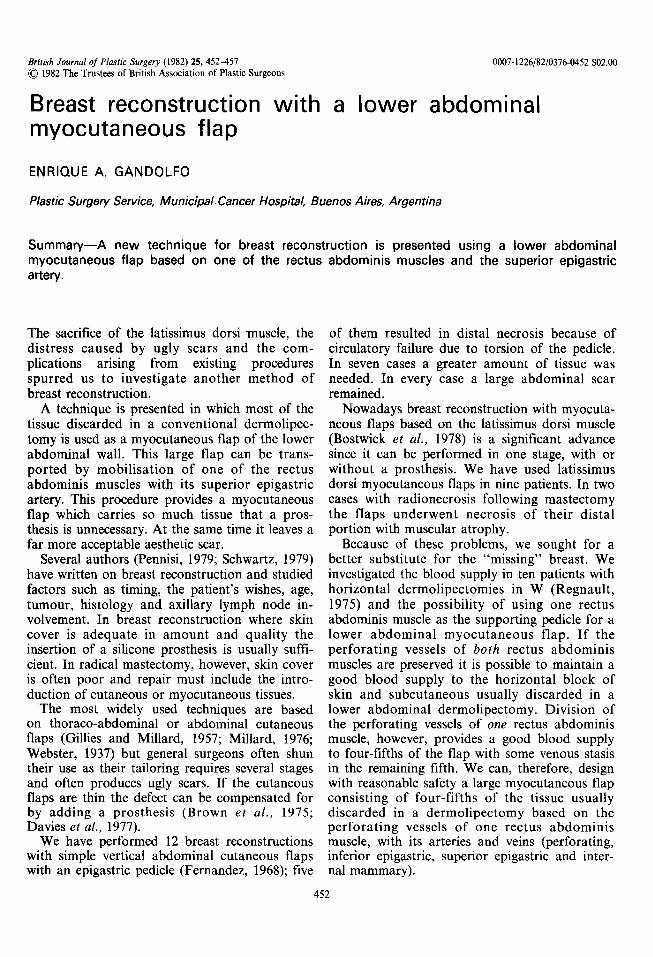
Fig. 1A. A radical mastectomy right side. The markings of a horizontal dermolipectomy in ‘w” have been drawn on the lower abdominal wall. B. Diagrammatic representation of a lower abdominal myocutaneous flap based on the right rectus muscle.
Procedure
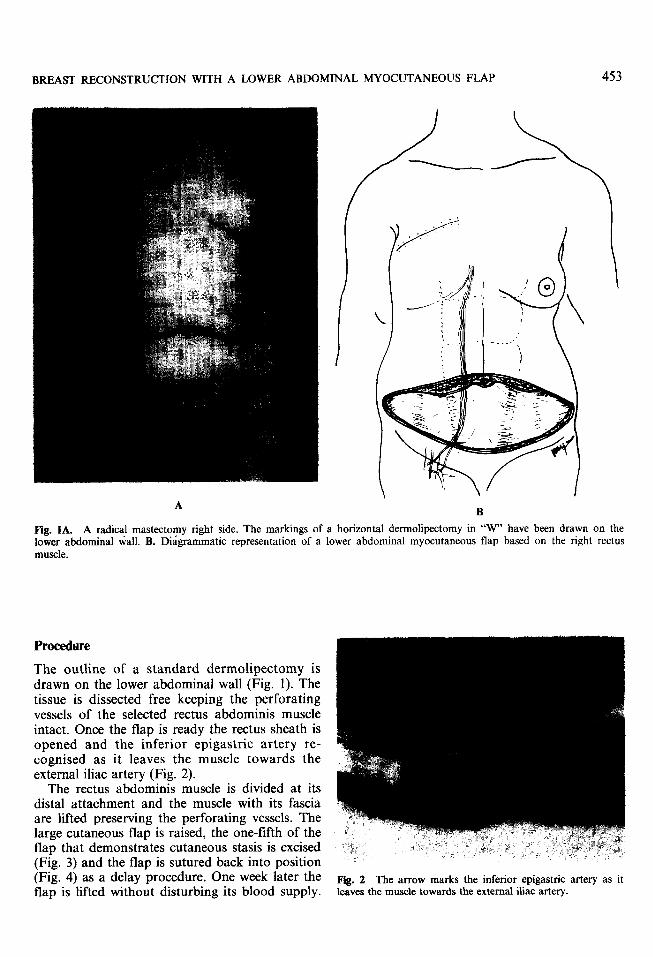
The outline of a standard dermolipectomy is drawn on the lower abdominal wall (Fig. 1). The tissue is dissected free keeping the perforating vessels of the selected rectus abdominis muscle intact. Once the flap is ready the rectus sheath is opened and the inferior epigastric artery re- cognised as it leaves the muscle towards the external iliac artery (Fig. 2).
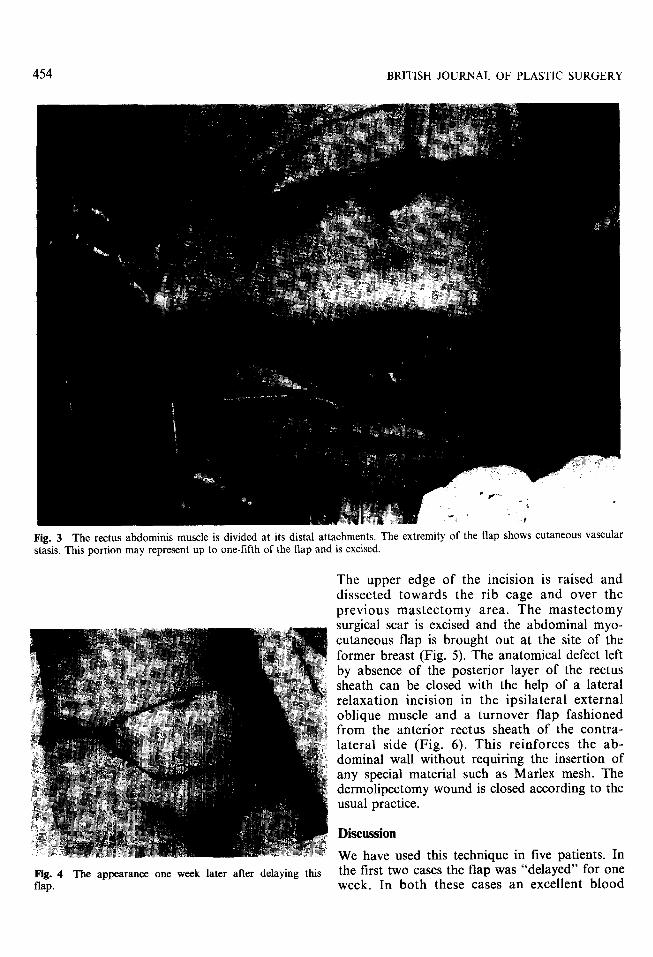
The rectus abdominis muscle is divided at its distal attachment and the muscle with its fascia are lifted preserving the perforating vessels. The large cutaneous flap is raised, the one-fifth of the flap that demonstrates cutaneous stasis is excised (Fig. 3) and the flap is sutured back into position (Fig. 4) as a delay procedure. One week later the flap is lifted without disturbing its blood supply.
Fig. 2 The arrow marks the inferior epigastric artery as it leaves the muscle towards the external iliac artery.
454 BRITISH JOURNAL OF PLASTIC SURGERY
Fig. 3 The rectus abdominis muscle is divided at its distal attachments. The extremity of the flap shows cutaneous vascular stasis. This portion may represent up to one-fifth of the flap and is excised.
Fig. 4 The appearance one week later after delaying this flap.
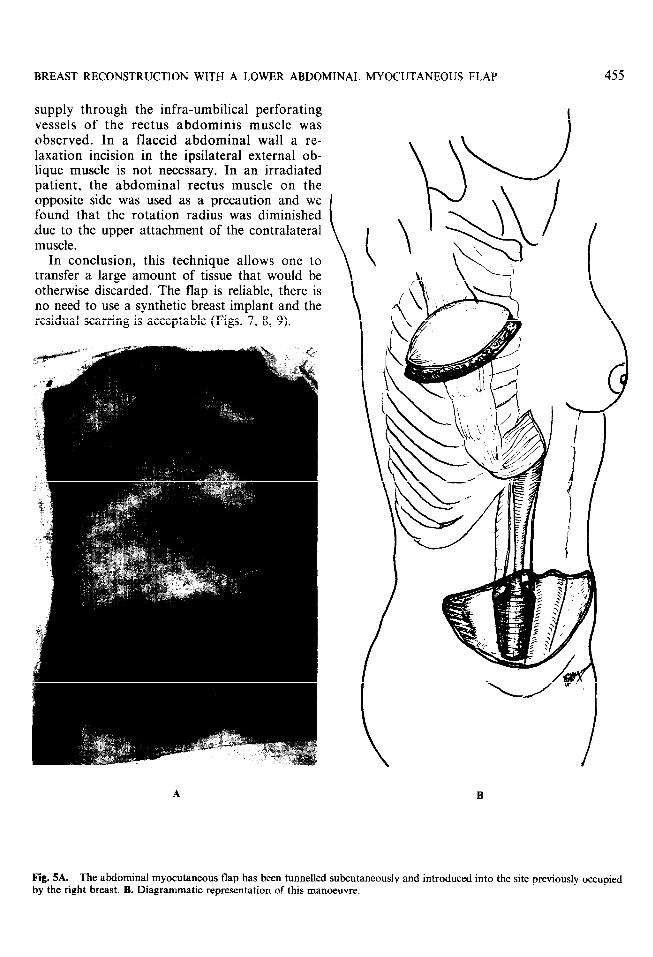
The upper edge of the incision is raised and dissected towards the rib cage and over the previous mastectomy area. The mastectomy surgical scar is excised and the abdominal myo- cutaneous flap is brought out at the site of the former breast (Fig. 5). The anatomical defect left by absence of the posterior layer of the rectus sheath can be closed with the help of a lateral relaxation incision in the ipsilateral external oblique muscle and a turnover flap fashioned from the anterior rectus sheath of the contra- lateral side (Fig. 6). This reinforces the ab- dominal wall without requiring the insertion of any special material such as Marlex mesh. The dermolipectomy wound is closed according to the usual practice.
Discussion
We have used this technique in five patients. In the first two cases the flap was “delayed” for one week. In both these cases an excellent blood
BREAST RECONSTRUCTION WITH A LOWER ABDOMINAL MYOCUTANEOUS FLAP
supply through the infra-umbilical perforating vessels of the rectus abdominis muscle was observed. In a flaccid abdominal wall a re- laxation incision in the ipsilateral external ob- lique muscle is not necessary. In an irradiated patient, the abdominal rectus muscle on the opposite side was used as a precaution and we found that the rotation radius was diminished .due to the upper attachment of the contralateral muscle.
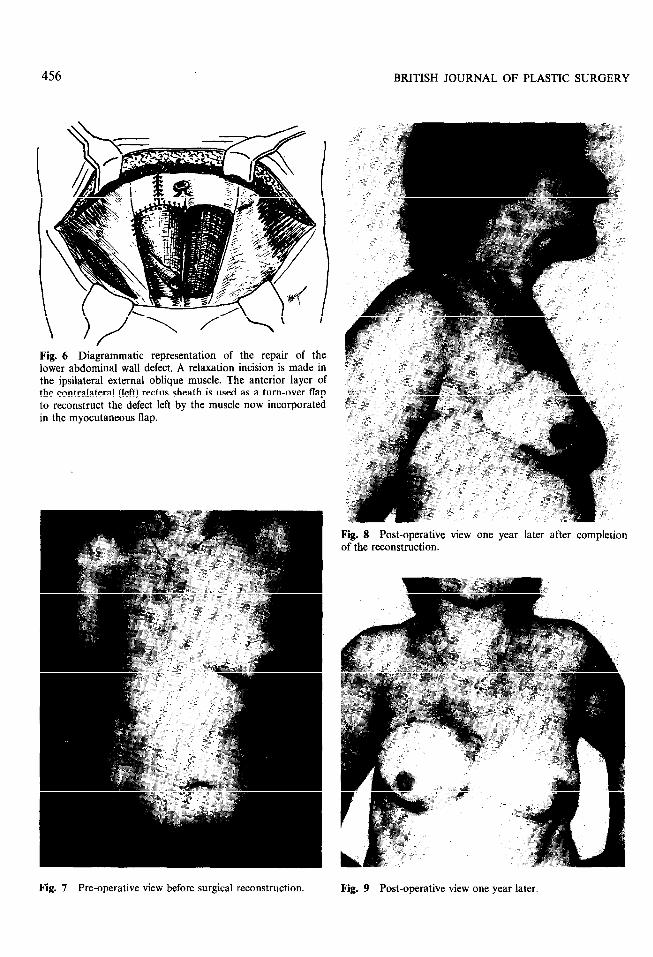
In conclusion, this technique allows one to transfer a large amount of tissue that would be otherwise discarded. The flap is reliable, there is no need to use a synthetic breast implant and the residual scarring is acceptable (Figs. 7, 8, 9).
455
Fig. SA. The abdominal myocutaneous flap has been tunnelled subcutaneously and introduced into the site previously occupied by the right breast. B. Diagrammatic representation of this manoeuvre.
456 BRITISH JOURNAL OF PLASTIC SURGERY
Fig. 6 Diagrammatic representation of the repair of the lower abdominal wall defect. A relaxation incision is made in the ipsilateral external oblique muscle. The anterior layer of the contralateral (left) rectus sheath is used as a turn-over flap to reconstruct the defect left by the muscle now incorporated in the myocutaneous flap.
Fig. 8 Post-operative view one year later after completion of the reconstruction.
Fig. 7 Pre-operative view before surgical reconstruction. Fig. 9 Post-operative view one year later.
BREAST RECONSTRUCTION WITH A LC j \YER ABDOMINAL MYOCUTANEOUS FLAP 457
References
Bostwick, J., Vasconez, L. 0. and Jarkiewicz, M. J. (1978). Breast reconstruction after a radical mastectomy. Plastic and Reconstructive Surgery, 61, 682.
Brown, R. G., Vaaconez, L. 0. and Jarkiewiu, M. J. (1975). Tranverse abdominal flaps and the deep epigastric -Ircade. Plastic and Reconstructive Surgery, 55, 416.
Davis, W. M., McGraw, J. B. and Carraway, J. H. (1977). Use of a direct transverse thoraco-abdominal flap to c!ose difficult wounds of the thorax and upper extremity. Plnsiic~ and Reconstructive Surgery, 60, 5 17.
Femaadez, J. (1968). Reconstruction mamaria. Boletines y Trabajos Sociedud Cirugia De Buenos Aires, SO, 86.
Gies, fi. D. and Millard, D. R. (1957). The Principles and Art of Plastic Surgery. Boston: Little Brown and Company.
MBhud, D. R. (1976). Breast reconstruction after radical mastectomy. Plastic and Reconstructive Surgery, 58, 283.
Pennisi, V. R. (1979). Timing of breast reconstruction after mastectomy. Clinics in Plastic Surgery, 6, 31.
Regnault, P. (1975). Abdominoplasty by the W technique. Plastic and Reconstructive Surgery, 55, 265.
Schwartz, G. F. (1979). Breast reconstruction following mastectomy for malignant disease: a surgical oncologist’s view. Clinics in Plastic Surgery, 6, 5.
Webster, J. P. (1937). Thoraco-epigastric tubed pedicles. Surgical Clinics of North America, 17, 145.
Acknowledgements
The author wishes to acknowledge the help of Dr F. Stengel in the translation, Dr H. Bertone for his help in the anatomical dissections, Dr A. Gregoire for the photographic work and Dr H. Marino for his encouragement and advice.
The work described in this paper was presented at the International Myocutaneous Flap meeting held in Buenos Aires in August 1981 by the Argentine Society of Plastic Surgery.
The Author
Enrique A. Gaadolfo, MD, Chief of the Plastic Surgery Service, Municipal Cancer Hospital, Buenos Aires. Argentina.
Requests for reprints to: Enrique Gandolfo, MD, Chief of the Plastic Surgery Service, Municipal Cancer Hospital, Jose E. Uriburu 1252, 1114 Buenos Aires, Argentina.





























