Embed Size (px)
Citation preview

Review Article
Received: 6 August 2007, Revised: 16 July 2008, Accepted: 21 July 2008, Published online in Wiley InterScience: 11 December 2008
(www.interscience.wiley.com) DOI:10.1002/nbm.1326
Breast cancer screening in women at high riskusing MRIy,z
Martin O. Leacha*
A series of prospective comparative studies have de
NMR Biom
monstrated that MRI has approximately twice the sensitivity ofX-ray mammography for screening women at high familial risk of breast cancer. In these studies, lesions have oftenbeen detected at an early stage, with disease being small and predominantly node negative. The diagnostic featuresin relation to risk and the biological behaviour of disease with risk category and age are being evaluated. The resultsof these studies have resulted in revised recommendations for screening for women at high risk of breast cancer. Inthis article, the results of the UK Magnetic Resonance Imaging in Breast Cancer Screening (MARIBS) study of MRIscreening are described, and compared with results from other studies. Risk factors identifying women who wouldbenefit from MRI screening are discussed, MRI measurement methods are described, and the results of studiesevaluating MRI and mammographic lesions in different risk groups are reviewed. Recommendations for screeningwomen at high risk of breast cancer published by the American Cancer Society and from the National Institute forHealth and Clinical Excellence (NICE) in the UK are summarised. Copyright � 2008 John Wiley & Sons, Ltd.
Keywords: breast cancer; MRI; dynamic contrast enhanced (DCE); screening; genetic mutation; BRCA1; BRCA2
* Correspondence to: M. O. Leach, Institute of Cancer Research and Royal
Marsden NHS Trust, CR UK Clinical Magnetic Resonance Research Group,
Oowns Road, Sutton, Surrey SM5 9PP, UK.
E-mail: [email protected]
a M. O. Leach
Cancer Research UK Clinical Magnetic Resonance Research Group, The
Institute of Cancer Research and The Royal Marsden NHS Foundation Trust,
Sutton, Surrey, UK
y Based in part on an educational contribution to the American Society of
Clinical Oncology [Leach MO. Screening for breast cancer in women at high
risk using MRI: United Kingdom study and other studies. In American Society
of Clinical Oncology Educational Book, Govindaswamy R (ed). American
Society of Clinical Oncology: Alexandria, VA, 2007;142–147.]
z MOL is a Director of speciality Scanners plc, a company developing dedicated
breast magnetic resonance imaging systems, and has patents for breast
cancer analysis, assigneal to the Institute of Cancer Research.
Abbreviations used: AUC, area under the curve; BI-RADS, American College
of Radiologists’ Breast Imaging Reporting and Data System; BRCA1, breast
cancer 1 gene; BRCA2, breast cancer 2 gene; DCIS, ductal carcinoma in-situ;
MARIBS, Magnetic Resonance Imaging in Breast Cancer Screening; MOR,
morphology; NICE, National Institute for Health and Clinical Excellence;
POE, pattern of enhancement; POCW, pattern of contrast washout; QALY,
quality adjusted life year; TP53, tumour protein 53 gene; XRM, X-ray mammo-
graphy. 1
INTRODUCTION
The aetiology of breast cancer is complex, combining sporadicrisks with socio-environmental and endocrine-related factors. Afamilial history of breast cancer also leads to amarkedly increasedrisk (1). Over the last 15 years, a number of gene mutations givingrise to some of the observed familial risk have been identified.These mutations generally occur at various loci in genesresponsible for aspects of DNA damage repair. Mutations inthe BRCA1 and BRCA2 genes (2,3) result in a cumulative risk ofbreast cancer by the age of 70 of 39–87% for BRCA1 and 26–91%for BRCA2 (4), often characterised by early onset of cancer. Oftenfamilies will exhibit raised incidence of several types of cancer,dependent on the gene and locus of mutation. Some rarer genemutations such as TP53 also confer high risks (5), and evidence isgrowing of further mutations in a range of genes that singlycause a small increase in risk, but may increase breast cancer riskin some women by acting together (6,7). Another factor leadingto increased risk of breast cancer is exposure to supradiaphrag-matic irradiation for Hodgkin’s disease before the age of 30.Although this treatment has now been superseded, thetreatments affected a small group of women, resulting in annualcancer risk rates that are similar to those for BRCA1/2 mutationcarriers (8).Subgroups in the population with an elevated risk of breast
cancer can be identified by performing genetic testing for breastcancer predisposition mutations or by evaluating family history.The relative cancer risk in women with predisposing mutations isparticularly high at younger ages. This results in a need forappropriate screening methods (9) for these identified popu-lations. X-ray mammography (XRM) is an effective screeningmethod in the normal population, particularly in those over 50,showing a sensitivity of about 86% (10). However, with the earlyonset of disease in the high-risk population, there is a need toscreen at a younger age, where the higher proportion of breastparenchyma can result in dense mammograms that are hard to
ed. 2009; 22: 17–27 Copyright � 2008 Jo
interpret. Several studies have shown that, in the normalpopulation, the sensitivity of screening mammograms falls withage (11,12). Kerlikowske et al. (11) reported a sensitivity of 77% forfirst screening mammograms in the 30–39-year-old age group.BRCA1 and BRCA2 tumours are also known to differ biologicallyfrom sporadic tumours (13), and this may also affect their visibilityon mammograms. Several small studies in BRCAmutation carriershave reported interval cancer rates of 46–50% within2–10 months of normal mammograms (14–16), suggesting thatannual mammography has limited sensitivity in this group. Thismay in part be due to the rate of tumour growth in this group.
hn Wiley & Sons, Ltd.
7

M. O. LEACH
18
MRI has developed as a standard technique for evaluatingbreast cancer, in addressing clinical problems where otherdiagnostic techniques fail, in follow-up and in surgical planning.The standard examination uses a low-molecular-mass gadoli-nium contrast agent to highlight lesions and their extent, usingeither subtraction of pre-contrast images and/or fat suppressedsequences to maximise lesion visibility. The contrast agent leaksinto the extracellular space in tissues with permeable vasculature,typical of neoangiogenesis, and increases the signal seen onT1-weighted MR images. In the assessment of breast cancer,measurements are usually acquired dynamically (dynamiccontrast enhanced MRI) before, during and at typically five timepoints after bolus injection of the contrast agent, allowing thecontrast agent uptake and washout characteristics of the lesionto be characterised – or at one or two time points (typically �2and 5min) after injection, which can allow higher spatialresolution images, with loss of time resolution. Evaluation isbased on the uptake curve from regions of interest definedwithinthe enhancing parts of the lesion and/or on the morphology ofthe lesion. A large number of studies have shown that MRI hashigh sensitivity for detecting breast cancer in symptomaticwomen, but variable specificity (17–21). Additional imagingsequences often include T2-weighted images, and diffusion-weighted imaging is being increasingly used.
EVALUATION OF MRI FOR BREASTCANCER SCREENING
The growing role of MRI in the evaluation of breast cancer insymptomatic women has identified that MRI may provide asensitive method for screening women at high risk of breastcancer. A number of prospective studies have been undertaken inhigh-risk women to compare MRI with other methods ofscreening (22–29). Here the UK Magnetic Resonance Imagingin Breast Cancer Screening (MARIBS) study (24) will be outlinedand compared with other recent studies.The UKMARIBS study compared MRI with XRM in a prospective
non-randomised trial in women with at least 50% risk of carryingmutations in BRCA1, BRCA2 or TP53, based on direct testing orfamily history (30–32). Women aged 35–49 for BRCA1/2 and25–49 for TP53 mutation carriers were recruited. Randomiseddesigns were considered, but the prevalence of mutation carriersin the UK did not support an adequately powered design.Randomised trials may also raise ethical concerns and adverselyaffect recruitment if one arm is considered to be more effectivebecause of more advanced technology. While determiningthe effect of the intervention on mortality, the extendedtime-course of disease, compared with the rate of technologicaladvance, would reduce the applicability of results from arandomised trial. Women were recruited through genetics clinics,excluding those with symptoms or a prior personal history ofbreast cancer. XRMwas performed in accordance with NHS BreastCancer Screening Programme standards. MRI measurement andassessment was performed as defined by a predefined protocol.All measurements were assessed by blinded double reading, alsoblinded to the other modality (33). The MRI protocol involvedprovision for two visits. The screening examination (Visit A)involved high spatial resolution T1-weighted three-dimensionalspoilt gradient-echo coronal image sets before and aftercompletion of a dynamic contrast enhanced series (below) (TR10–14ms, TE 4.2–4.5ms, flip angle 358, slice thickness 2.5mm,0.66� 0.89mm pixels, matrix 512� 384, 60–64 slices) with the
www.interscience.wiley.com/journal/nbm Copyright � 200
post-contrast set performed with fat suppression if possible. Adynamic three-dimensional series of images using a similarsequence but with 1.33� 1.33mm pixels andmatrix 256� 256 togive an acquisition time of 90 s for each of seven images (twobefore contrast, five after) followed the first high-resolutionsequence. A proton density-weighted sequence with the sameresolution to permit quantitative analysis preceded the dynamicset. A rapid bolus of 0.2mmol gadopentetate dimeglumine(Magnevist; Schering Healthcare Ltd, Burgess Hill, Sussex, UK) wasused. A follow-up examination (Visit B) was used when findingswere equivocal. This used the same high spatial resolution scansbefore and after contrast, but provided for higher temporalresolution T1-weighted spoilt gradient-echo scans in the sagittalor coronal orientation with four to nine slices through the lesionof interest and 50 acquisitions with 12 s time resolution. If therewere multiple lesions to evaluate, the Visit A protocol wasrepeated.Evaluation of the image data used a pre-determined scoring
scheme to be applied to suspicious lesions (33), which identifiedmorphological and dynamic features of contrast uptake, andscored these individually in proportion to the expected likelihoodof malignancy. The features described and the scores applied aredetailed in Fig. 1 and Table 1, respectively. These scores wererecorded and guided the radiologist’s decision. Positive resultswere those that achieved the equivalent of American College ofRadiologists’ Breast Imaging Reporting and Data System(BI-RADS) 3 or greater. When the MRI findings required furtherinvestigation (BI-RADS 0) or were suspicious (BI-RADS 3 or 4),there was a mandatory recall for a further MRI scan. Clinicalpathways were determined by the local lead clinician on the basisof the results. Women proceeded to further investigation, biopsyand localisation, and, where appropriate, resection, as required.Recruitment was performed through 22 centres in the UK, withannual screening for 2–7 years and a follow-up period of 1 yearafter the last screen. When further investigation did notdemonstrate cancer, screening continued. A total of 649 womenreceived 1881 screens by both MRI and XRM, resulting in35 cancers being detected. Nineteen of these were observed byMRI alone, six by XRM alone, and eight by both techniques, withtwo interval cases detected (24). Figure 2 shows an example of ascreen-detected cancer seen only by MRI in a woman with aBRCA1 mutation.The sensitivity and specificity of detection for each modality,
with confidence intervals, is detailed in Table 2. MRI was almosttwice as sensitive as XRM in this high-risk group (77% vs 40%),although the specificity of MRI was lower (81% vs 93%).Combining the techniques gave an overall sensitivity of 94%and a specificity of 77%. Six of the cancers detected were ductalcarcinoma in-situ (DCIS) with no invasive component, with threebeing seen by XRM alone, two by both techniques, and onedetected as an interval cancer. Excluding DCIS increases thesensitivity of MRI to 86% and that of XRM to 31% with an overallcombined sensitivity of 97%. Over a third (38%) of the invasivecancers detected were less than 10mm in size, and 52%were lessthan 15mm, similar to the proportion found in the UK NationalBreast Screening Programme using XRM in women over 50. Mostcancer was grade 3 (66%), with 24% being grade 2, consistentwith the high proportion of BRCA1/2 mutation carriers in thecohort. Most (81%) of the women with invasive cancer were nodenegative. These results show that MRI has considerably greatersensitivity for the detection of breast cancer than XRM in this riskgroup and age range. When the two techniques are combined,
8 John Wiley & Sons, Ltd. NMR Biomed. 2009; 22: 17–27
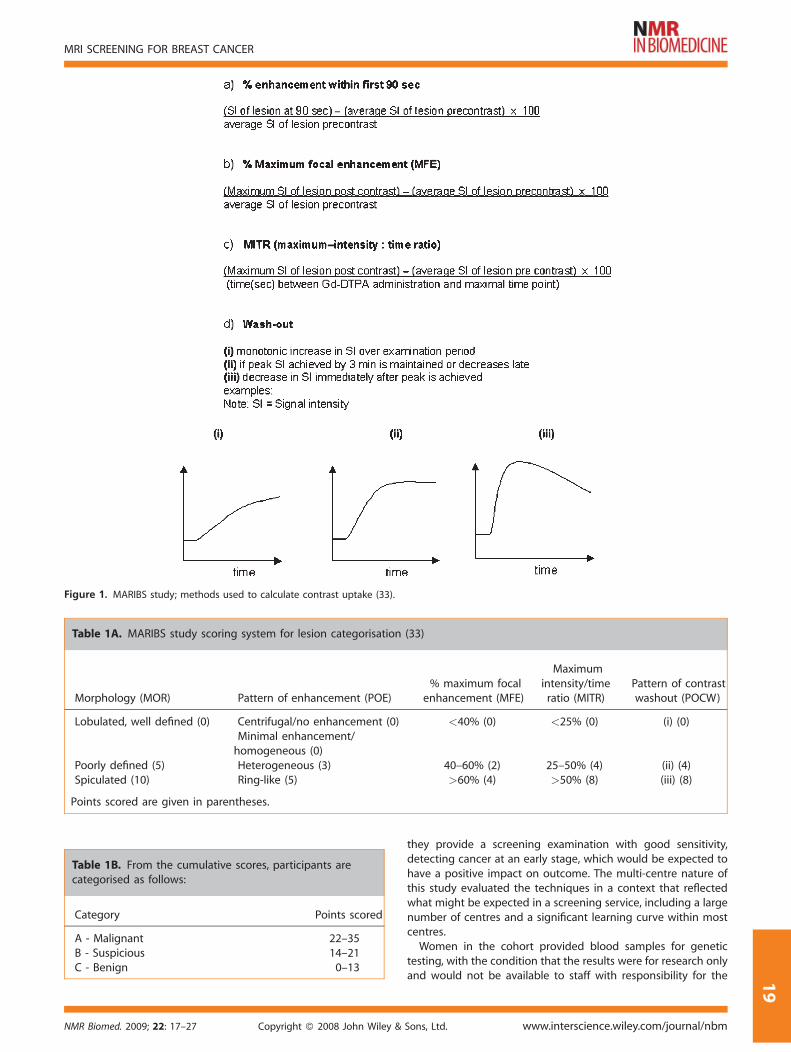
Figure 1. MARIBS study; methods used to calculate contrast uptake (33).
Table 1A. MARIBS study scoring system for lesion categorisation (33)
Morphology (MOR) Pattern of enhancement (POE)% maximum focal
enhancement (MFE)
Maximumintensity/timeratio (MITR)
Pattern of contrastwashout (POCW)
Lobulated, well defined (0) Centrifugal/no enhancement (0) <40% (0) <25% (0) (i) (0)Minimal enhancement/homogeneous (0)
Poorly defined (5) Heterogeneous (3) 40–60% (2) 25–50% (4) (ii) (4)Spiculated (10) Ring-like (5) >60% (4) >50% (8) (iii) (8)
Points scored are given in parentheses.
Table 1B. From the cumulative scores, participants arecategorised as follows:
Category Points scored
A - Malignant 22–35B - Suspicious 14–21C - Benign 0–13
MRI SCREENING FOR BREAST CANCER
1
NMR Biomed. 2009; 22: 17–27 Copyright � 2008 John Wiley &
they provide a screening examination with good sensitivity,detecting cancer at an early stage, which would be expected tohave a positive impact on outcome. The multi-centre nature ofthis study evaluated the techniques in a context that reflectedwhat might be expected in a screening service, including a largenumber of centres and a significant learning curve within mostcentres.Women in the cohort provided blood samples for genetic
testing, with the condition that the results were for research onlyand would not be available to staff with responsibility for the
Sons, Ltd. www.interscience.wiley.com/journal/nbm
9
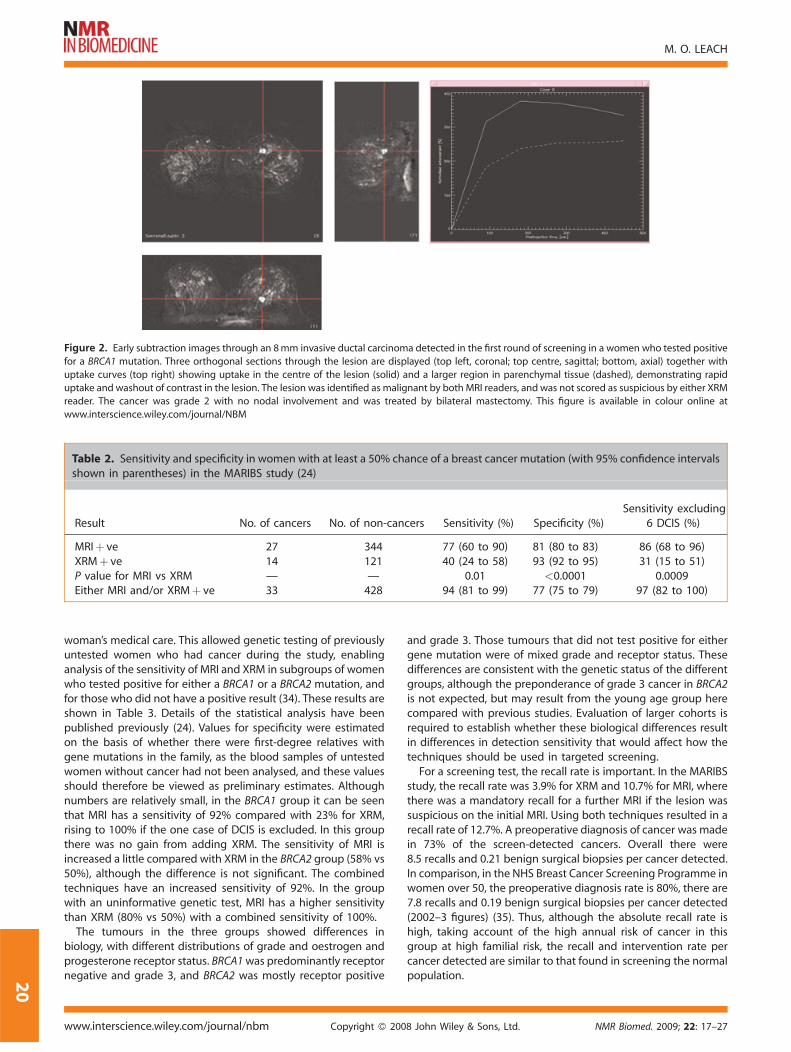
Figure 2. Early subtraction images through an 8mm invasive ductal carcinoma detected in the first round of screening in a women who tested positive
for a BRCA1 mutation. Three orthogonal sections through the lesion are displayed (top left, coronal; top centre, sagittal; bottom, axial) together with
uptake curves (top right) showing uptake in the centre of the lesion (solid) and a larger region in parenchymal tissue (dashed), demonstrating rapid
uptake and washout of contrast in the lesion. The lesion was identified as malignant by both MRI readers, and was not scored as suspicious by either XRMreader. The cancer was grade 2 with no nodal involvement and was treated by bilateral mastectomy. This figure is available in colour online at
www.interscience.wiley.com/journal/NBM
Table 2. Sensitivity and specificity in women with at least a 50% chance of a breast cancer mutation (with 95% confidence intervalsshown in parentheses) in the MARIBS study (24)
Result No. of cancers No. of non-cancers Sensitivity (%) Specificity (%)Sensitivity excluding
6 DCIS (%)
MRIþ ve 27 344 77 (60 to 90) 81 (80 to 83) 86 (68 to 96)XRMþ ve 14 121 40 (24 to 58) 93 (92 to 95) 31 (15 to 51)P value for MRI vs XRM — — 0.01 <0.0001 0.0009Either MRI and/or XRMþ ve 33 428 94 (81 to 99) 77 (75 to 79) 97 (82 to 100)
M. O. LEACH
20
woman’s medical care. This allowed genetic testing of previouslyuntested women who had cancer during the study, enablinganalysis of the sensitivity of MRI and XRM in subgroups of womenwho tested positive for either a BRCA1 or a BRCA2 mutation, andfor those who did not have a positive result (34). These results areshown in Table 3. Details of the statistical analysis have beenpublished previously (24). Values for specificity were estimatedon the basis of whether there were first-degree relatives withgene mutations in the family, as the blood samples of untestedwomen without cancer had not been analysed, and these valuesshould therefore be viewed as preliminary estimates. Althoughnumbers are relatively small, in the BRCA1 group it can be seenthat MRI has a sensitivity of 92% compared with 23% for XRM,rising to 100% if the one case of DCIS is excluded. In this groupthere was no gain from adding XRM. The sensitivity of MRI isincreased a little compared with XRM in the BRCA2 group (58% vs50%), although the difference is not significant. The combinedtechniques have an increased sensitivity of 92%. In the groupwith an uninformative genetic test, MRI has a higher sensitivitythan XRM (80% vs 50%) with a combined sensitivity of 100%.The tumours in the three groups showed differences in
biology, with different distributions of grade and oestrogen andprogesterone receptor status. BRCA1was predominantly receptornegative and grade 3, and BRCA2 was mostly receptor positive
www.interscience.wiley.com/journal/nbm Copyright � 200
and grade 3. Those tumours that did not test positive for eithergene mutation were of mixed grade and receptor status. Thesedifferences are consistent with the genetic status of the differentgroups, although the preponderance of grade 3 cancer in BRCA2is not expected, but may result from the young age group herecompared with previous studies. Evaluation of larger cohorts isrequired to establish whether these biological differences resultin differences in detection sensitivity that would affect how thetechniques should be used in targeted screening.For a screening test, the recall rate is important. In the MARIBS
study, the recall rate was 3.9% for XRM and 10.7% for MRI, wherethere was a mandatory recall for a further MRI if the lesion wassuspicious on the initial MRI. Using both techniques resulted in arecall rate of 12.7%. A preoperative diagnosis of cancer was madein 73% of the screen-detected cancers. Overall there were8.5 recalls and 0.21 benign surgical biopsies per cancer detected.In comparison, in the NHS Breast Cancer Screening Programme inwomen over 50, the preoperative diagnosis rate is 80%, there are7.8 recalls and 0.19 benign surgical biopsies per cancer detected(2002–3 figures) (35). Thus, although the absolute recall rate ishigh, taking account of the high annual risk of cancer in thisgroup at high familial risk, the recall and intervention rate percancer detected are similar to that found in screening the normalpopulation.
8 John Wiley & Sons, Ltd. NMR Biomed. 2009; 22: 17–27

Table 3. Sensitivity and specificity in women testing positive for BRCA1/2 mutations, or having a non-informative test result (with95% confidence intervals in parentheses) in the MARIBS study (24)
ResultNo. ofcancers
No. ofnon-cancers Sensitivity (%) Specificity (%)
Sensitivityexcluding
either 1a or 3b
DCIS (%)
BRCA1 positiveMRIþ ve 12 76 92 (64 to 100) 79 (75 to 83) 100 (74 to 100)XRMþ ve 3 30 23 (5 to 54) 92 (88 to 94) 25 (5.5 to 57)P value for MRI vs XRM — — 0.004 <0.0001 —Either MRI and/or XRMþ ve 12 95 92 (64 to 100) 74 (69 to 78) —
BRCA2 positiveMRI þve 7 41 58 (28 to 84) 82 (77 to 87) 67 (30 to 93)XRM þve 6 13 50 (21 to 79) 94 (91 to 97) 33 (7.5 to 70)P value for MRI vs XRM — — 1.0 0.0001 0.45Either MRI and/or XRM þve 11 51 92 (62 to 100) 78 (72 to 83) —
Mutation test uninformativeMRI þve 8 1022 80 (44 to 97) 82 (80 to 84) —XRM þve 5 1171 50 (19 to 81) 94 (92 to 95) —P value for MRI vs XRM — — 0.45 0.0001 —Either MRI and/or XRM þve 10 967 100 77 (75 to 80) —
aFor BCRA1 positive.bFor BCRA2 positive.
MRI SCREENING FOR BREAST CANCER
2
IMAGE ANALYSIS
The MARIBS study used a scoring scheme for the MRI assessment,based on literature reports, as an aid to identification of malignantdisease, and to allow the relative contribution of differentinformation to the sensitivity of detection and the specificity ofidentification of malignant disease to be evaluated (33). Differentmorphological descriptors (MOR), morphological patterns ofcontrast enhancement (POE), calculated parameters of signalintensity change, and descriptors of contrast uptake and washout(POCW) were assigned scores that increased with the estimatedlikelihood of malignancy. For each lesion, these scores were thenassigned and summed to provide an overall score, which assignedthe lesion as likely to be benign, suspicious or malignant. As thestudy involved double reading of mammograms, the value ofdouble reading could be ascertained. The performance of thescoring scheme was assessed in a cohort including both 638screening cases and a group of 100 women with symptomaticfindings, with 91malignant lesions (36). The sensitivity for detectingmalignant disease for the first and second readers was 81% and89%, and in combination, taking the most malignant score, 91%.The specificities were, respectively, 88%, 88% and 81%. Resultsshowed that, with time in the study, readers evaluated fewersuspicious lesions, suggesting increased experience. A comparisonof results between field strengths of 1.0 T and 1.5 T showed nosignificant difference in sensitivity or specificity.The contribution that different descriptors in the scoring
scheme made to diagnosis has been evaluated (37). The scoringscheme has an overall area under the curve (AUC) of a receiveroperator characteristic curve of 0.88. The POE had an AUC of 0.83,POCW had an AUC of 0.81, and MOR had an AUC of 0.79,indicating that these all contributed to the overall sensitivity.Calculated parameters contributed less to the AUC (0.61–0.71),and a simplified scoring scheme neglecting these calculated
NMR Biomed. 2009; 22: 17–27 Copyright � 2008 John Wiley &
parameters provided a similar performance to the originalscheme (AUC¼ 0.91), with the potential to provide a useful aid todiagnostic decision making.
COMPARISON WITH OTHER STUDIES
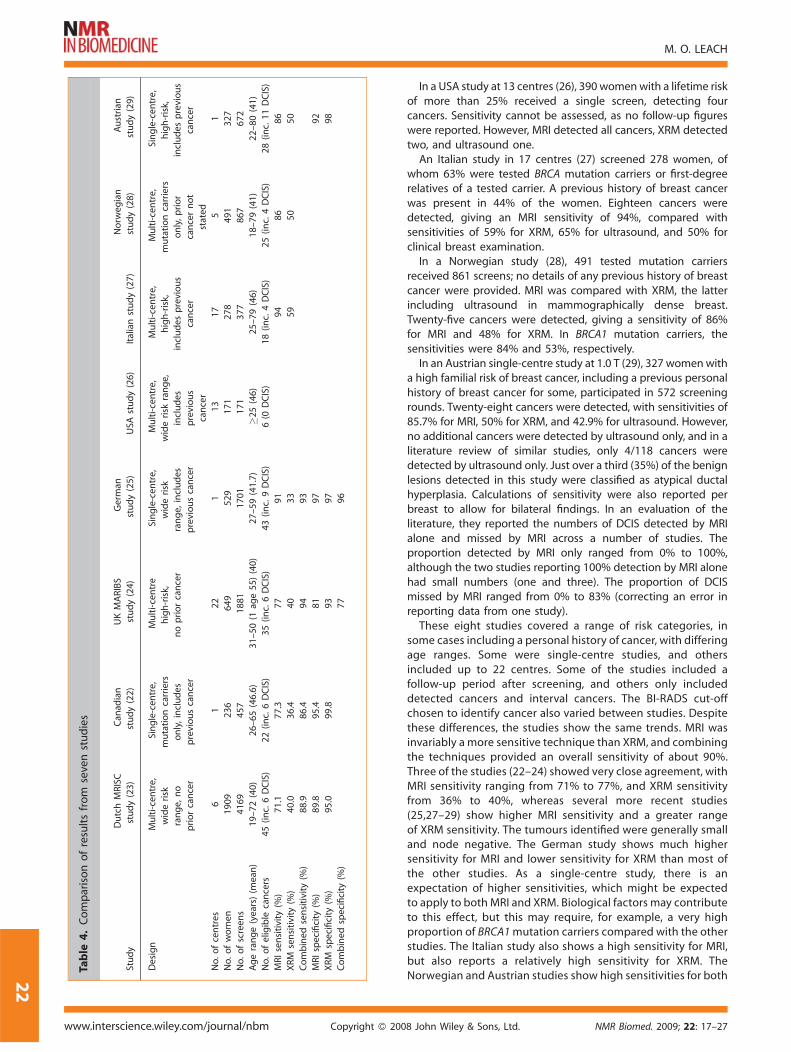
There have been a number of other studies that have investigatedMRI for screening women at high familial risk of breast cancer.Themain findings of these studies are summarised in Table 4. TheDutch MRISC study (23) recruited women with no previoushistory of breast cancer in several risk groups (overall summarydata given in Table 4) with a minimum of 15% lifetime risk. Thestudy was performed at six centres in the Netherlands, with 1909women recruited. Fifty cancers were detected, with a sensitivityof 71% for MRI, 40% for XRM, and 89% for the combinedtechniques. Results were considered positive when the BI-RADSscore was 3 or greater. Screening also included breast self-examination (sensitivity 18%).The Canadian study (22) was performed at a single centre and
screened 236 women with BRCA1/2mutations, including womenwith a personal history of breast cancer, finding 22 cancers.Results were considered positive when the BI-RADS score was4 or 5. The sensitivity was 77% for MRI, 36% for XRM, and 86% forboth. Screening included ultrasound (sensitivity 33%) and breastexamination (sensitivity 9%).In a German single-centre study (25), 529 women with a life
time risk of at least 20%, including women with a personal historyof breast cancer, were screened for a mean period of 5 years;43 cancers were found. Screening included MRI, XRM andultrasound, with sensitivities of 91%, 33% and 40%, respectively.CombiningMRI and XRM gave an overall sensitivity of 93% for thewhole population and 100% in the group without a personal riskof breast cancer. Ultrasound in combination with XRM had asensitivity of 49%.
Sons, Ltd. www.interscience.wiley.com/journal/nbm
1
Table
4.Comparisonofresultsfrom
sevenstudies
Study
DutchMRISC
study(23)
Can
adian
study(22)
UKMARIBS
study(24)
German
study(25)
USA
study(26)
Italianstudy(27)
Norw
egian
study(28)
Austrian
study(29)
Design
Multi-centre,
widerisk
range,
no
priorcancer
Single-cen
tre,
mutationcarriers
only,includes
previouscancer
Multi-centre
high-risk,
nopriorcancer
Single-cen
tre,
widerisk
range,
includes
previouscancer
Multi-centre,
widerisk
range,
includes
previous
cancer
Multi-centre,
high-risk,
includes
previous
cancer
Multi-centre,
mutationcarriers
only,prior
cancernot
stated
Single-cen
tre,
high-risk,
includes
previous
cancer
No.ofcentres
61
22
113
17
51
No.ofwomen
1909
236
649
529
171
278
491
327
No.ofscreen
s4169
457
1881
1701
171
377
867
672
Agerange(years)
(mean
)19–7
2(40)
26–6
5(46.6)
31–5
0(1
age55)(40)
27–5
9(41.7)
�25(46)
25–7
9(46)
18–7
9(41)
22–8
0(41)
No.ofeligible
cancers
45(inc.6DCIS)
22(inc.6DCIS)
35(inc.6DCIS)
43(inc.9DCIS)
6(0
DCIS)
18(inc.4DCIS)
25(inc.4DCIS)
28(inc.11DCIS)
MRIsensitivity
(%)
71.1
77.3
77
91
94
86
86
XRM
sensitivity
(%)
40.0
36.4
40
33
59
50
50
Combined
sensitivity
(%)
88.9
86.4
94
93
MRIspecificity
(%)
89.8
95.4
81
97
92
XRM
specificity
(%)
95.0
99.8
93
97
98
Combined
specificity
(%)
77
96
M. O. LEACH
22
www.interscience.wiley.com/journal/nbm Copyright � 200
In a USA study at 13 centres (26), 390 womenwith a lifetime riskof more than 25% received a single screen, detecting fourcancers. Sensitivity cannot be assessed, as no follow-up figureswere reported. However, MRI detected all cancers, XRM detectedtwo, and ultrasound one.An Italian study in 17 centres (27) screened 278 women, of
whom 63% were tested BRCA mutation carriers or first-degreerelatives of a tested carrier. A previous history of breast cancerwas present in 44% of the women. Eighteen cancers weredetected, giving an MRI sensitivity of 94%, compared withsensitivities of 59% for XRM, 65% for ultrasound, and 50% forclinical breast examination.In a Norwegian study (28), 491 tested mutation carriers
received 861 screens; no details of any previous history of breastcancer were provided. MRI was compared with XRM, the latterincluding ultrasound in mammographically dense breast.Twenty-five cancers were detected, giving a sensitivity of 86%for MRI and 48% for XRM. In BRCA1 mutation carriers, thesensitivities were 84% and 53%, respectively.In an Austrian single-centre study at 1.0 T (29), 327 womenwith
a high familial risk of breast cancer, including a previous personalhistory of breast cancer for some, participated in 572 screeningrounds. Twenty-eight cancers were detected, with sensitivities of85.7% for MRI, 50% for XRM, and 42.9% for ultrasound. However,no additional cancers were detected by ultrasound only, and in aliterature review of similar studies, only 4/118 cancers weredetected by ultrasound only. Just over a third (35%) of the benignlesions detected in this study were classified as atypical ductalhyperplasia. Calculations of sensitivity were also reported perbreast to allow for bilateral findings. In an evaluation of theliterature, they reported the numbers of DCIS detected by MRIalone and missed by MRI across a number of studies. Theproportion detected by MRI only ranged from 0% to 100%,although the two studies reporting 100% detection by MRI alonehad small numbers (one and three). The proportion of DCISmissed by MRI ranged from 0% to 83% (correcting an error inreporting data from one study).These eight studies covered a range of risk categories, in
some cases including a personal history of cancer, with differingage ranges. Some were single-centre studies, and othersincluded up to 22 centres. Some of the studies included afollow-up period after screening, and others only includeddetected cancers and interval cancers. The BI-RADS cut-offchosen to identify cancer also varied between studies. Despitethese differences, the studies show the same trends. MRI wasinvariably a more sensitive technique than XRM, and combiningthe techniques provided an overall sensitivity of about 90%.Three of the studies (22–24) showed very close agreement, withMRI sensitivity ranging from 71% to 77%, and XRM sensitivityfrom 36% to 40%, whereas several more recent studies(25,27–29) show higher MRI sensitivity and a greater rangeof XRM sensitivity. The tumours identified were generally smalland node negative. The German study shows much highersensitivity for MRI and lower sensitivity for XRM than most ofthe other studies. As a single-centre study, there is anexpectation of higher sensitivities, which might be expectedto apply to both MRI and XRM. Biological factors may contributeto this effect, but this may require, for example, a very highproportion of BRCA1mutation carriers compared with the otherstudies. The Italian study also shows a high sensitivity for MRI,but also reports a relatively high sensitivity for XRM. TheNorwegian and Austrian studies show high sensitivities for both
8 John Wiley & Sons, Ltd. NMR Biomed. 2009; 22: 17–27

MRI SCREENING FOR BREAST CANCER
MRI and XRM, although in the former study the mammographyin some cases also included ultrasound.An overview of five recent studies calculated an overall
sensitivity of 80.7% for MRI and 39.5% for mammography (38).This evaluation also calculated that 48.5% of tumours detectedwere� 1 cm, and that 18.9%were node positive. Of those with thegrade reported, 49.1% were grade 3 and 81.5% were invasive. Thecancer detection rate and the intervention rate per cancerdetected in the MARIBS study compares favourably with currentpopulation screening for breast cancer. Several systematic reviewshave considered screening approaches in high-risk women. Lordet al. (39) considered the value of adding MRI to mammography ormammography plus ultrasound and or clinical breast examination,concluding that adding MRI results in the detection of additionalcancers, but that any mortality benefit is unknown. Bermejo-Perezet al. (40) reported similar conclusions. A systematic review wasalso a part of the National Institute for Health and ClinicalExcellence (NICE) guideline development process (see below).
2
DIAGNOSTIC FEATURES OF LESIONS
Most of the screening studies did not report the use of specificguidelines for discriminating lesions, but used radiologicalexperience, combined with the BI-RADS classification systemor a similar approach. As described above, the MARIBS study useda formal scoring scheme for MRI, weighting a range ofdescriptors, and thereby achieving a sensitivity of 91% for dualreading in an evaluation study (36). Both morphological anddynamic features contributed to this sensitivity (37). Two recentpapers have evaluated the imaging characteristics of high-riskwomen. Veltman et al. (41) investigated the mammography andMRI appearance of BRCAmutation carriers, comparing these withcontrols matched for age and tumour type and size. Theyconcluded that, on mammography, BRCA lesions were signifi-cantly more often described as rounded and with sharp marginsthan were control tumours. On MRI, the BRCA group were alsosignificantly more likely to be rounded, with sharp margins andwith rim enhancement than is the case for the control group.However, enhancement kinetics did not differ from the controls.Tumours in the control group were more likely to have vague orspiculated margins, to have an irregular boundary, and/or to beheterogeneous. Thus many of the morphological features ofthe BRCA tumours are those that would be considered to bemoretypical of benign lesions, although accompanied by rapid uptakeand washout of the contrast agent. This emphasises the need torecall and further evaluate a wide range of lesion appearances inwomen at high familial risk. Schrading and Kuhl (42) alsoinvestigated the imaging phenotypes of familial breast cancer,covering a wider range of risk categories encompassing mutationcarriers (20) and groups with a range of familial risk (56). Theynoted that a proportion (15) of the cases had a benignfibroadenoma-like morphological appearance (23%) on mam-mography, and, on MRI, without calcification, or, on MR, thefibroadenoma-like internal appearance or enhancement curve.Twelve (80%) of these occurred in high-risk and documentedBRCA1 mutation carriers. Two-thirds (32/48) of the women whowere BRCA mutation carriers or at high risk had a posteriorlocation of tumours (immediately prepectoral). None of thetumours in BRCA1mutation carriers showed calcifications, and noDCIS were seen in this group. Tumours in BRCA2mutation carriersand in the lower-risk group showed characteristics more
NMR Biomed. 2009; 22: 17–27 Copyright � 2008 John Wiley &
representative of sporadic tumours. A high proportion of theinvasive cancers also showed non-mass-like enhancement, and33% of invasive cancers showed benign kinetic features. Twelvecases of DCIS were seen, eight of which did not result inmammographically initiated recalls, one was not seen on eitherMRI or mammography, and 11 showed non-mass-like asymme-trical enhancement on MRI. Kinetics were typical of benignlesions in 58% of the cases. In a separate report, Kuhl has reportedon the sensitivity or MRI for detection of DCIS (43), and, given thepotential to detect DCIS with MRI, it is likely that the variability ofsensitivity reported by different studies may result fromimplementation of new diagnostic experience over the con-siderable period of some of the studies, spatial resolution used inscreening examinations, and avoidance of motion effects.A number of investigators (44,45) have reported on the
different biological features of tumours arising from BRCAmutation carriers, in particular the high grade and pushingmargins seen in tumours from BRCA1mutation carriers. It appearsthat these differences can affect the appearance of tumours onmammography and on MRI, underlining the need for a widerrange of diagnostic features to be considered characteristic ofmalignancy in this group, potentially inevitably increasing thelikelihood of recall for lesions that may be benign.
PSYCHOLOGICAL IMPACT
Some women find MRI more disturbing than XRM, but themajority (86% for MRI, 92% for mammography) find that thetechniques are ‘not at all’ or ‘a little’ disturbing. A small proportionof women find MRI very disturbing, principally as a result ofclaustrophobia. Where there is concern, this may remain for6 weeks after the scan (46).
IMPACT OF FURTHER DEVELOPMENTSIN IMAGING TECHNIQUES
MRI technology, and its application to screening for breast cancer,is still at a relatively early stage of development, compared withXRM for example. MRI equipment and techniques, together withmeasurement methods, continue to evolve rapidly. As equipmentand techniques develop further, associated with increasingexperience and the outcome of studies using the technology,measurement sensitivity is expected to improve further, leadingto the potential to detect smaller malignant and pre-malignantlesions. These developments may also aid in more effectivediscrimination of malignant disease and DCIS from benigndisease and normal structures. At the same time, XRM is evolving,with increasing uptake of digital mammography, which hasbenefits in the younger age groups particularly at risk in familialbreast cancer. The development of tomosynthesis applied to XRMmay also further improve discrimination of lesions. Furtherdevelopments in cross-sectional ultrasound, XRM and opticalimaging may in time provide increased sensitivity, but there ismuch research and development still required.
GUIDANCE AND IMPLEMENTATION
Moving from the research arena to provision of a service toaffected women requires assessment of the personal, societaland economic benefit likely to result for particular risk and age
Sons, Ltd. www.interscience.wiley.com/journal/nbm
3
M. O. LEACH
24
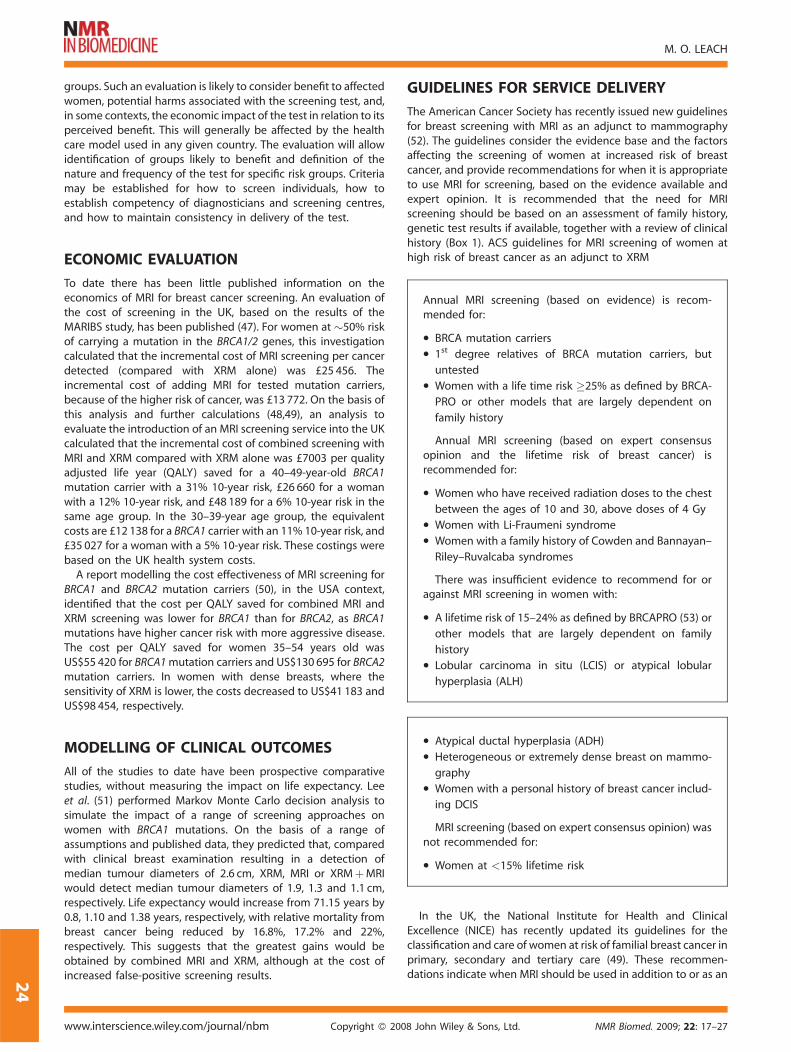
groups. Such an evaluation is likely to consider benefit to affectedwomen, potential harms associated with the screening test, and,in some contexts, the economic impact of the test in relation to itsperceived benefit. This will generally be affected by the healthcare model used in any given country. The evaluation will allowidentification of groups likely to benefit and definition of thenature and frequency of the test for specific risk groups. Criteriamay be established for how to screen individuals, how toestablish competency of diagnosticians and screening centres,and how to maintain consistency in delivery of the test.
Annual MRI screening (based on evidence) is recom-mended for:
� BRCA mutation carriers
� 1st degree relatives of BRCA mutation carriers, but
untested
� Women with a life time risk �25% as defined by BRCA-
PRO or other models that are largely dependent on
family history
Annual MRI screening (based on expert consensusopinion and the lifetime risk of breast cancer) isrecommended for:
� Women who have received radiation doses to the chest
between the ages of 10 and 30, above doses of 4 Gy
� Women with Li-Fraumeni syndrome
� Women with a family history of Cowden and Bannayan–
Riley–Ruvalcaba syndromes
There was insufficient evidence to recommend for oragainst MRI screening in women with:
� A lifetime risk of 15–24% as defined by BRCAPRO (53) or
other models that are largely dependent on family
history
� Lobular carcinoma in situ (LCIS) or atypical lobular
hyperplasia (ALH)
ECONOMIC EVALUATION
To date there has been little published information on theeconomics of MRI for breast cancer screening. An evaluation ofthe cost of screening in the UK, based on the results of theMARIBS study, has been published (47). For women at �50% riskof carrying a mutation in the BRCA1/2 genes, this investigationcalculated that the incremental cost of MRI screening per cancerdetected (compared with XRM alone) was £25 456. Theincremental cost of adding MRI for tested mutation carriers,because of the higher risk of cancer, was £13 772. On the basis ofthis analysis and further calculations (48,49), an analysis toevaluate the introduction of an MRI screening service into the UKcalculated that the incremental cost of combined screening withMRI and XRM compared with XRM alone was £7003 per qualityadjusted life year (QALY) saved for a 40–49-year-old BRCA1mutation carrier with a 31% 10-year risk, £26 660 for a womanwith a 12% 10-year risk, and £48 189 for a 6% 10-year risk in thesame age group. In the 30–39-year age group, the equivalentcosts are £12 138 for a BRCA1 carrier with an 11% 10-year risk, and£35 027 for a woman with a 5% 10-year risk. These costings werebased on the UK health system costs.A report modelling the cost effectiveness of MRI screening for
BRCA1 and BRCA2 mutation carriers (50), in the USA context,identified that the cost per QALY saved for combined MRI andXRM screening was lower for BRCA1 than for BRCA2, as BRCA1mutations have higher cancer risk with more aggressive disease.The cost per QALY saved for women 35–54 years old wasUS$55 420 for BRCA1mutation carriers and US$130 695 for BRCA2mutation carriers. In women with dense breasts, where thesensitivity of XRM is lower, the costs decreased to US$41 183 andUS$98 454, respectively.
� Atypical ductal hyperplasia (ADH)
� Heterogeneous or extremely dense breast on mammo-
graphy
� Women with a personal history of breast cancer includ-
ing DCIS
MRI screening (based on expert consensus opinion) wasnot recommended for:
� Women at <15% lifetime risk
MODELLING OF CLINICAL OUTCOMES
All of the studies to date have been prospective comparativestudies, without measuring the impact on life expectancy. Leeet al. (51) performed Markov Monte Carlo decision analysis tosimulate the impact of a range of screening approaches onwomen with BRCA1 mutations. On the basis of a range ofassumptions and published data, they predicted that, comparedwith clinical breast examination resulting in a detection ofmedian tumour diameters of 2.6 cm, XRM, MRI or XRMþMRIwould detect median tumour diameters of 1.9, 1.3 and 1.1 cm,respectively. Life expectancy would increase from 71.15 years by0.8, 1.10 and 1.38 years, respectively, with relative mortality frombreast cancer being reduced by 16.8%, 17.2% and 22%,respectively. This suggests that the greatest gains would beobtained by combined MRI and XRM, although at the cost ofincreased false-positive screening results.
www.interscience.wiley.com/journal/nbm Copyright � 200
GUIDELINES FOR SERVICE DELIVERY
The American Cancer Society has recently issued new guidelinesfor breast screening with MRI as an adjunct to mammography(52). The guidelines consider the evidence base and the factorsaffecting the screening of women at increased risk of breastcancer, and provide recommendations for when it is appropriateto use MRI for screening, based on the evidence available andexpert opinion. It is recommended that the need for MRIscreening should be based on an assessment of family history,genetic test results if available, together with a review of clinicalhistory (Box 1). ACS guidelines for MRI screening of women athigh risk of breast cancer as an adjunct to XRM
In the UK, the National Institute for Health and Clinical
Excellence (NICE) has recently updated its guidelines for theclassification and care of women at risk of familial breast cancer inprimary, secondary and tertiary care (49). These recommen-dations indicate when MRI should be used in addition to or as an8 John Wiley & Sons, Ltd. NMR Biomed. 2009; 22: 17–27

MRI SCREENING FOR BREAST CANCER
alternative to XRM and underpin introduction of MRI screeningwithin the NHS screening programme. It is recommended thatwomen should receive a clear description of methods ofscreening, intervals, benefits and risks, together with sourcesof support and further information. MRI of both breasts should beperformed with high temporal and spatial resolution, withdynamic sequences post contrast. The images should be doubleread where possible. Where XRM is recommended in womenunder the age of 50, digital mammography should be used wherepossible, provided that it meets the standards current in the NHSBreast Screening Programme.Women who have been referred to a genetics centre who are
not known to have a genetic mutation should be offered anassessment of their 10-year breast cancer risk using a validatedrisk assessment tool (for example, Tyrer–Cuzick (54) or BOADICEA(55)) to assess whether they are or will be eligible for MRI. SeeBox 2 for detailed recommendations. Guidelines for screeningwomen at high risk of breast cancer: NICE guidelines (UK) forwomen at familial risk of breast cancer
Annual MRI surveillance should be offered to:
� Known BRCA1 or BRCA2 mutation carriers between the
ages of 35 and 49
� Known TP53 mutation carriers aged 20 or older� Women aged between 30 and 39 years with a 10-year
risk >8%
� Women between 40 and 49 years with a 10-year risk
>20%, or with a 10-year risk >12% and mammogra-
phically dense breasts
� Women who have not been tested but are at a high risk
of carrying a BRCA1 or TP53 genetic mutation and are
aged 30–49 who have a 50% risk of carrying such a
mutation in a tested family, or a 50% chance of carrying
such a mutation in an untested or inconclusively tested
family with at least a 60% chance of carrying one of
these mutations, equivalent to a 30% chance of them-
selves carrying such a mutation
There is considerable similarity between these two sets ofrecommendations, but it should be borne in mind that the ACSguidelines address the remit of the use of MRI screening inwomen at increased risk of breast cancer, whereas the NICEguidelines refer to women with familial risk. The NICE guidelinesare based on considerations of cost effectiveness, based on theUK health care model, which affects risk level and age rangeconsidered appropriate for MRI screening.
2
ISSUES
The studies detailed above have led to revised recommendationsfor breast cancer screening in high-risk women. However, thereremain limitations in the scope of evidence available. There islimited information on the relative contribution that MRI canmake to detection for different mutation types, ages, and withother factors that affect risk, although some evidence that
NMR Biomed. 2009; 22: 17–27 Copyright � 2008 John Wiley &
imaging characteristics, as well as the biology, may differ with riskgroup and age. None of the studies were randomised, limiting theavailable information on effect on mortality, although it mayprove possible to model the likely impact on mortality, and initialstudies have reported a projected gain in mortality fromscreening. MRI is recognised as resulting in an increased recallrate, with an associated increased rate of intervention. Thestudies to date have not provided evidence of the degree towhich overdiagnosis may be a concern, although this concernmay be mitigated by the evidence for a shorter doubling timeand more aggressive phenotype for these predominantlyhigh-grade tumours in young women. With an increasing abilityof MRI to detect DCIS, this could potentially lead to overdiagnosis,although for DCIS to be seen on MRI, there is likely to be anincreased vascular effect that may be a marker for invasivepotential.Most studies to date have used an annual screening interval,
and this is embodied in current guidelines. In women at high riskof breast cancer, the relative risk at younger ages is high, but theabsolute numbers are low and all of the studies had relatively fewwomen in the youngest age groups. Analysis of data from threeof the studies (MRISC, MARIBS and Canadian) has allowedassessment of tumour growth rate in women with different risksand age ranges (56). This has shown that tumour growth rates aretwice as fast in BRCA1 and BRCA2mutation carriers as in high-riskwomen not known to be mutation carriers. The mean tumourdoubling time was found to be 28 days in mutation carriers aged40 or below, compared with 83 days for high-risk non-carriers inthe same age range, 81 days for carriers over 50, and 173 days forhigh-risk non-carriers over 50. This may lead to a need to considermore intensive screening strategies in some younger women,although the cost benefit of this in terms of increasedsurveillance, recalls and economics needs to be established.MRI screening is a complex investigation, requiring dedi-
cated breast coils and scanner arrangements that provide goodsensitivity and image quality. Readers need to be experienced inthe technique. Currently there are few quality assuranceguidelines or accreditation schemes in place to guide imple-mentation, and to assist those referring patients to identifycentres with appropriate expertise and training, although it islikely that guidelines and accreditation will be established in thenear future. Selection of women who would benefit from MRIscreening also requires appropriate expertise, and a thoroughevaluation of their personal and familial risk of breast cancer,which can best be provided through family cancer or cancergenetics clinics.
CONCLUSIONS
MRI has been shown to be the most sensitive method ofdetecting cancer in women at familial risk of breast cancer. Whenused alone it has a sensitivity almost twice that of XRM and,combined with mammography, it has a sensitivity of �90%.Cancers detected are predominantly small and node negative.There is increasing evidence that the imaging characteristics ofcancers in gene carriers differ from those in the normalpopulation. The studies underlying these findings have led tochanges in national recommendations for the screening ofwomen at high risk of breast cancer, and to the introduction oftargeted MRI screening in a number of countries.
Sons, Ltd. www.interscience.wiley.com/journal/nbm
5
M. O. LEACH
26
REFERENCES
1. Claus EB, Schildkraut JM, Thompson WD, Risch NJ. The genetic attribu-table risk of breast and ovarian cancer. Cancer 1996; 77: 2318–2324.
2. Easton DF, Bishop DT, Ford D, Crockford GP. Genetic linkage analysis infamilial breast and ovarian cancer: results from 214 families. The BreastCancer Linkage Consortium. Am. J. Hum. Genet. 1993; 52: 678–701.
3. Wooster R, Bignell G, Lancaster J, Swift S, Seal S, Mangion J, Collins N,Gregory S, Gumbs C, Micklem G. Identification of the breast cancersusceptibility gene BRCA2. Nature 1995; 378: 789–792.
4. Robson M, Offit K. Clinical practice. Management of an inheritedpredisposition to breast cancer. N. Engl. J. Med. 2007; 357: 154–162.
5. Malkin D, Li FP, Strong LC, Fraumeni JF Jr, Nelson CE, Kim DH, Kassel J,Gryka MA, Bischoff FZ, Tainsky MA. Germ line p53 mutations in afamilial syndrome of breast cancer, sarcomas, and other neoplasms.Science 1990; 250: 1233–1238.
6. Easton DF, Pooley KA, Dunning AM, Pharoah PD, Thompson D,Ballinger DG, Struewing JP, Morrison J, Field H, Luben R, WarehamN, Ahmed S, Healey CS, Bowman R, Meyer KB, Haiman CA, Kolonel LK,Henderson BE, Le Marchand L, Brennan P, Sangrajrang S, Gaborieau V,Odefrey F, Shen CY, Wu PE, Wang HC, Eccles D, Evans DG, Peto J,Fletcher O, Johnson N, Seal S, Stratton MR, Rahman N, Chenevix-Trench G, Bojesen SE, Nordestgaard BG, Axelsson CK, Garcia-Closas M,Brinton L, Chanock S, Lissowska J, Peplonska B, Nevanlinna H, Fager-holm R, Eerola H, Kang D, Yoo KY, Noh DY, Ahn SH, Hunter DJ,Hankinson SE, Cox DG, Hall P, Wedren S, Liu J, Low YL, BogdanovaN, Schurmann P, Dork T, Tollenaar RA, Jacobi CE, Devilee P, Klijn JG,Sigurdson AJ, Doody MM, Alexander BH, Zhang J, Cox A, Brock IW,MacPherson G, Reed MW, Couch FJ, Goode EL, Olson JE, Meijer-s-Heijboer H, van den OA, Uitterlinden A, Rivadeneira F, Milne RL,Ribas G, Gonzalez-Neira A, Benitez J, Hopper JL, McCredie M, SoutheyM, Giles GG, Schroen C, Justenhoven C, Brauch H, Hamann U, Ko YD,Spurdle AB, Beesley J, Chen X, Mannermaa A, Kosma VM, Kataja V,Hartikainen J, Day NE, Cox DR, Ponder BA. Genome-wide associationstudy identifies novel breast cancer susceptibility loci. Nature. 2007;447: 1087–1093.
7. Cox A, Dunning AM, Garcia-Closas M, Balasubramanian S, Reed MW,Pooley KA, Scollen S, Baynes C, Ponder BA, Chanock S, Lissowska J,Brinton L, Peplonska B, Southey MC, Hopper JL, McCredie MR, GilesGG, Fletcher O, Johnson N, Dos SS I, Gibson L, Bojesen SE, Nordest-gaard BG, Axelsson CK, Torres D, Hamann U, Justenhoven C, Brauch H,Chang-Claude J, Kropp S, Risch A, Wang-Gohrke S, Schurmann P,Bogdanova N, Dork T, Fagerholm R, Aaltonen K, Blomqvist C, Nevan-linna H, Seal S, Renwick A, Stratton MR, Rahman N, Sangrajrang S,Hughes D, Odefrey F, Brennan P, Spurdle AB, Chenevix-Trench G,Beesley J, Mannermaa A, Hartikainen J, Kataja V, Kosma VM, Couch FJ,Olson JE, Goode EL, Broeks A, Schmidt MK, Hogervorst FB, Van’t VeerLJ, Kang D, Yoo KY, Noh DY, Ahn SH, Wedren S, Hall P, Low YL, Liu J,Milne RL, Ribas G, Gonzalez-Neira A, Benitez J, Sigurdson AJ, StredrickDL, Alexander BH, Struewing JP, Pharoah PD, Easton DF. A commoncoding variant in CASP8 is associated with breast cancer risk. Nat.Genet. 2007; 39: 352–358.
8. Horwich A, Swerdlow AJ. Second primary breast cancer after Hodg-kin’s disease. Br. J. Cancer 2004; 90: 294–298.
9. Leach MO. MRI for breast cancer screening. Ann. Oncol. 2006;17 Suppl 10: x325–x331.
10. Banks E, Reeves G, Beral V, Bull D, Crossley B, Simmonds M, Hilton E,Bailey S, Barrett N, Briers P, English R, Jackson A, Kutt E, Lavelle J,Rockall L, Wallis MG, Wilson M, Patnick J. Influence of personalcharacteristics of individual women on sensitivity and specificity ofmammography in the Million Women Study: cohort study. BMJ. 2004;329: 477.
11. Kerlikowske K, Grady D, Barclay J, Sickles EA, Ernster V. Likelihoodratios for modern screening mammography. Risk of breast cancerbased on age and mammographic interpretation. JAMA. 1996; 276:39–43.
12. Mushlin AI, Kouides RW, Shapiro DE. Estimating the accuracy ofscreening mammography: a meta-analysis. Am. J. Prev. Med. 1998;14: 143–153.
13. Lakhani SR, Jacquemier J, Sloane JP, Gusterson BA, Anderson TJ, vande Vijver MJ, Farid LM, Venter D, Antoniou A, Storfer-Isser A, Smyth E,Steel CM, Haites N, Scott RJ, Goldgar D, Neuhausen S, Daly PA,Ormiston W, McManus R, Scherneck S, Ponder BA, Ford D, Peto J,Stoppa-Lyonnet D, Easton DF. and. Multifactorial analysis of differ-
www.interscience.wiley.com/journal/nbm Copyright � 200
ences between sporadic breast cancers and cancers involving BRCA1and BRCA2 mutations. J. Natl. Cancer Inst. 1998; 90: 1138–1145.
14. Komenaka IK, Ditkoff BA, Joseph KA, Russo D, Gorroochurn P, Ward M,Horowitz E, El Tamer MB, Schnabel FR. The development of intervalbreast malignancies in patients with BRCA mutations. Cancer 2004;100: 2079–2083.
15. Scheuer L, Kauff N, Robson M, Kelly B, Barakat R, Satagopan J, Ellis N,Hensley M, Boyd J, Borgen P, Norton L, Offit K. Outcome of preventivesurgery and screening for breast and ovarian cancer in BRCAmutation carriers. J. Clin Oncol. 2002; 20: 1260–1268.
16. Meijers-Heijboer H, van Geel B, van Putten WL, Henzen-Logmans SC,Seynaeve C, Menke-Pluymers MB, Bartels CC, Verhoog LC, van denOuweland AM, Niermeijer MF, Brekelmans CT, Klijn JG. Breast cancerafter prophylactic bilateral mastectomy in women with a BRCA1 orBRCA2 mutation. N. Engl. J. Med. 2001; 345: 159–164.
17. Heywang-Kobrunner SH, Bick U, Bradley WG Jr, Bone B, Casselman J,Coulthard A, Fischer U, Muller-Schimpfle M, Oellinger H, Patt R,Teubner J, Friedrich M, Newstead G, Holland R, Schauer A, SicklesEA, Tabar L, Waisman J, Wernecke KD. International investigation ofbreast MRI: results of a multicentre study (11 sites) concerningdiagnostic parameters for contrast-enhanced MRI based on 519histopathologically correlated lesions. Eur. Radiol. 2001; 11: 531–546.
18. Harms SE, Flamig DP, Hesley KL, Meiches MD, Jensen RA, Evans WP,Savino DA, Wells RA. MR imaging of the breast with rotating deliveryof excitation off resonance: clinical experience with pathologic cor-relation. Radiology 1993; 187: 493–501.
19. Boetes C, Barentsz JO, Mus RD, van der Sluis RF, van Erning LJ, HendriksJH, Holland R, Ruys SH. MR characterization of suspicious breastlesions with a gadolinium-enhanced TurboFLASH subtraction tech-nique. Radiology 1994; 193: 777–781.
20. Baum F, Fischer U, Vosshenrich R, Grabbe E. Classification of hyper-vascularized lesions in CE MR imaging of the breast. Eur. Radiol. 2002;12: 1087–1092.
21. Gilles R, Guinebretiere JM, Toussaint C, Spielman M, Rietjens M, PetitJY, Contesso G, Masselot J, Vanel D. Locally advanced breast cancer:contrast-enhanced subtraction MR imaging of response to preopera-tive chemotherapy. Radiology 1994; 191: 633–638.
22. Warner E, Plewes DB, Hill KA, Causer PA, Zubovits JT, Jong RA, CutraraMR, DeBoer G, YaffeMJ, Messner SJ, MeschinoWS, Piron CA, Narod SA.Surveillance of BRCA1 and BRCA2 mutation carriers with magneticresonance imaging, ultrasound, mammography, and clinical breastexamination. JAMA 2004; 292: 1317–1325.
23. Kriege M, Brekelmans CT, Boetes C, Besnard PE, Zonderland HM,Obdeijn IM, Manoliu RA, Kok T, Peterse H, Tilanus-Linthorst MM,MullerSH, Meijer S, Oosterwijk JC, Beex LV, Tollenaar RA, de Koning HJ,Rutgers EJ, Klijn JG. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition.N. Engl. J. Med. 2004; 351: 427–437.
24. Leach MO, Boggis CR, Dixon AK, Easton DF, Eeles RA, Evans DG, GilbertFJ, Griebsch I, Hoff RJ, Kessar P, Lakhani SR, Moss SM, Nerurkar A,Padhani AR, Pointon LJ, Thompson D, Warren RM. Screening withmagnetic resonance imaging and mammography of a UK populationat high familial risk of breast cancer: a prospective multicentre cohortstudy (MARIBS). Lancet 2005; 365: 1769–1778.
25. Kuhl CK, Schrading S, Leutner CC, Morakkabati-Spitz N, Wardelmann E,Fimmers R, KuhnW, Schild HH. Mammography, breast ultrasound, andmagnetic resonance imaging for surveillance of women at highfamilial risk for breast cancer. J. Clin. Oncol. 2005; 23: 8469–8476.
26. Lehman CD, Blume JD, Weatherall P, Thickman D, Hylton N, Warner E,Pisano E, Schnitt SJ, Gatsonis C, Schnall M, DeAngelis GA, Stomper P,Rosen EL, O’loughlin M, Harms S, Bluemke DA. Screening women athigh risk for breast cancer with mammography and magnetic reson-ance imaging. Cancer 2005; 103: 1898–1905.
27. Sardanelli F, Podo F, D’Agnolo G, Verdecchia A, Santaquilani M,Musumeci R, Trecate G, Manoukian S, Morassut S, De Giacomi C,Federico M, Cortesi L, Corcione S, Cirillo S, Marra V, Cilotti A, Di MaggioC, Fausto A, Preda L, Zuiani C, Contegiacomo A, Orlacchio A, CalabreseM, Bonomo L, Di Cesare E, Tonutti M, Panizza P, Del Maschio A.Multicenter comparative multimodality surveillance of women atgenetic-familial high risk for breast cancer (HIBCRIT study): interimresults. Radiology. 2007; 242: 698–715.
28. Hagen AI, Kvistad KA, Maehle L, Holmen MM, Aase H, Styr B, Vabo A,Apold J, Skaane P, Moller P. Sensitivity of MRI versus conventionalscreening in the diagnosis of BRCA-associated breast cancer in anational prospective series. Breast. 2007; 16: 367–374.
8 John Wiley & Sons, Ltd. NMR Biomed. 2009; 22: 17–27
MRI SCREENING FOR BREAST CANCER
29. Riedl CC, Ponhold L, Flory D, Weber M, Kroiss R, Wagner T, FuchsjagerM, Helbich TH. Magnetic resonance imaging of the breast improvesdetection of invasive cancer, preinvasive cancer, and premalignantlesions during surveillance of women at high risk for breast cancer.Clin Cancer Res. 2007; 13: 6144–6152.
30. Leach MO. Protocol 97PRT/4: National study of magnetic resonanceimaging to screen women at genetic risk of breast cancer. Lancet1997. http://www.thelancet.com/journals/lancet/misc/protocol/97PRT-4 (accessed 1 Oct 2008).
31. Brown J, Coulthard A, Dixon AK, Dixon JM, Easton DF, Eeles RA, EvansDGR, Gilbert FG, Hayes C, Jenkins JPR, Leach MO, Moss SM, PadhaniAP, Pointon LJ, Ponder BAJ, Sloane JP, Turnbull LW, Walker LG, WarrenRML, Watson W. Rationale for a national multi-centre study of mag-netic resonance imaging screening in women at genetic risk of breastcancer. Breast 2000; 9: 72–77.
32. Brown J, Coulthard A, Dixon AK, Dixon JM, Easton DF, Eeles RA, EvansDGR, Gilbert FG, Hayes C, Jenkins JPR, Leach MO, Moss SM, PadhaniAP, Pointon LJ, Ponder BAJ, Sloane JP, Turnbull LW, Walker LG, WarrenRML, WatsonW. Protocol for a national multi-centre study ofmagneticresonance imaging screening in women at genetic risk of breastcancer. Breast 2000; 9: 78–82.
33. Brown J, Buckley D, Coulthard A, Dixon AK, Dixon JM, Easton DF, EelesRA, Evans DG, Gilbert FG, Graves M, Hayes C, Jenkins JP, Jones AP,Keevil SF, Leach MO, Liney GP, Moss SM, Padhani AR, Parker GJ,Pointon LJ, Ponder BA, Redpath TW, Sloane JP, Turnbull LW, WalkerLG, Warren RM. Magnetic resonance imaging screening in women atgenetic risk of breast cancer: imaging and analysis protocol for the UKmulticentre study. Magn Reson Imaging 2000; 18: 765–776.
34. LeachMO, TheMARIBS Study Group. Screening women at genetic riskof breast cancer using DCE-MRI: the effect of gene mutation status ondetection sensitivity, specificity and cancer characteristics. Proceed-ings of the International Society of Magnetic Resonance in Medicine.2006; 14: 297.
35. NHSBSP. Cancer Screening Programmes. National Breast ScreeningProgramme 2004 review. 2005. http://cancerscreening.org.uk/breastscreen/publications/2004review.html (accessed 1 Oct 2008).
36. Warren RM, Pointon L, Thompson D, Hoff R, Gilbert FJ, Padhani A,Easton D, Lakhani SR, Leach MO. Reading protocol for dynamiccontrast-enhancedMR images of the breast: sensitivity and specificityanalysis. Radiology 2005; 236: 779–788.
37. Warren RM, Thompson D, Pointon LJ, Hoff R, Gilbert FJ, Padhani AR,Easton DF, Lakhani SR, Leach MO. Evaluation of a prospective scoringsystem designed for a multicenter breast MR imaging screeningstudy. Radiology 2006; 239: 677–685.
38. Sardanelli F, Podo F. Breast MR imaging in women at high-risk ofbreast cancer. Is something changing in early breast cancer detec-tion? Eur. Radiol. 2007; 17: 873–887.
39. Lord SJ, Lei W, Craft P, Cawson JN, Morris I, Walleser S, Griffiths A,Parker S, Houssami N. A systematic review of the effectiveness ofmagnetic resonance imaging (MRI) as an addition to mammographyand ultrasound in screening young women at high risk of breastcancer. Eur. J. Cancer. 2007; 43: 1905–1917.
40. Bermejo-Perez MJ, Marquez-Calderon S, Llanos-Mendez A. Cancersurveillance based on imaging techniques in carriers of BRCA1/2gene mutations: a systematic review. Br. J. Radiol. 2008; 81: 172–179.
41. Veltman J, Mann R, Kok T, Obdeijn IM, Hoogerbrugge N, Blickman JG,Boetes C. Breast tumor characteristics of BRCA1 and BRCA2 genemutation carriers on MRI. Eur. Radiol. 2008; 18: 931–938.
NMR Biomed. 2009; 22: 17–27 Copyright � 2008 John Wiley &
42. Schrading S, Kuhl CK. Mammographic, US, and MR imaging pheno-types of familial breast cancer. Radiology. 2008; 246: 58–70.
43. Kuhl CK, Schrading S, Bieling HB,Wardelmann E, Leutner CC, Koenig R,Kuhn W, Schild HH. MRI for diagnosis of pure ductal carcinoma insitu: a prospective observational study. Lancet. 2007; 370: 485–492.
44. Lakhani SR. The pathology of familial breast cancer: Morphologicalaspects. Breast Cancer Res. 1999; 1: 31–35.
45. Tilanus-Linthorst M, Verhoog L, Obdeijn IM, Bartels K, Menke-PluymersM, Eggermont A, Klijn J, Meijers-Heijboer H, van der KT, Brekelmans C.A BRCA1/2 mutation, high breast density and prominent pushingmargins of a tumor independently contribute to a frequent false-negative mammography. Int. J. Cancer 2002; 102: 91–95.
46. Anderson J, Walker LG, Leach MO. Magnetic resonance imaging: anacceptable way of screening women with a family history of breastcancer. Breast Cancer Res Treat 2004; 88: S188. 27th Annual Charles AColman San Antonio Breast Cancer Symposium.
47. Griebsch I, Brown J, Boggis C, Dixon A, Dixon M, Easton D, Eeles R,Evans DG, Gilbert FJ, Hawnaur J, Kessar P, Lakhani SR, Moss SM,Nerurkar A, Padhani AR, Pointon LJ, Potterton J, Thompson D, TurnbullLW, Walker LG, Warren R, Leach MO. Cost-effectiveness of screeningwith contrast enhanced magnetic resonance imaging vs X-ray mam-mography of women at a high familial risk of breast cancer. Br. J.Cancer 2006; 95: 801–810.
48. Norman RP, Evans DG, Easton DF, Young KC. The cost-utility ofmagnetic resonance imaging for breast cancer in BRCA1 mutationcarriers aged 30–49. Eur. J. Health Econ. 2007; 8: 137–144.
49. NICE. Familial breast cancer: the classification and care of women at riskof familial breast cancer in primary, secondary and tertiary care –update. 2006; 1-75. National Institute for Health and Clinica Excellence,London. http://www.nice.org.uk/guidance/cg41 (accessed 1 Oct 2008).
50. Plevritis SK, Kurian AW, Sigal BM, Daniel BL, Ikeda DM, Stockdale FE,Garber AM. Cost-effectiveness of screening BRCA1/2 mutation carrierswith breast magnetic resonance imaging. JAMA 2006; 295: 2374–2384.
51. Lee JM, Kopans DB, McMahon PM, Halpern EF, Ryan PD, Weinstein MC,Gazelle GS. Breast cancer screening in BRCA1 mutation carriers:effectiveness of MR imaging: Markov Monte Carlo decision analysis.Radiology. 2008; 246: 763–771.
52. SaslowD, Boetes C, BurkeW, Harms S, LeachMO, Lehman CD, Morris E,Pisano E, Schnall M, Sener S, Smith RA, Warner E, Yaffe M, Andrews KS,Russell CA. American Cancer Society guidelines for breast screeningwith MRI as an adjunct to mammography. CA Cancer J Clin. 2007; 57:75–89.
53. Parmigiani G, Berry DA, Aguilar O. Determining carrier probabilities forbreast cancer-susceptibility genes BRCA1 and BRCA2. Am J HumGenet. 1998; 62: 145–58.
54. Tyrer J, Duffy SW, Cuzick J. A breast cancer prediction model incor-porating familial and personal risk factors. Stat. Med. 2004; 23:1111–1130.
55. Antoniou AC, Pharoah PP, Smith P, Easton DF. The BOADICEAmodel ofgenetic susceptibility to breast and ovarian cancer. Br. J. Cancer 2004;91: 1580–1590.
56. Tilanus-Linthorst MM, Obdeijn IM, Hop WC, Causer PA, Leach MO,Warner E, Pointon L, Hill K, Klijn JG, Warren RM, Gilbert FJ. BRCA1mutation and young age predict fast breast cancer growth in theDutch, United Kingdom, and Canadian magnetic resonance imagingscreening trials. Clin Cancer Res. 2007; 13: 7357–7362.
Sons, Ltd. www.interscience.wiley.com/journal/nbm
27





























