Embed Size (px)
Citation preview

Brain Hemorrhage from Intracranial Tumor 283
JOHN R. LITTLE, M.D., BURKE DIAL, M.D., GARRY BELANGER, M.D.,
AND STIRLING CARPENTER, M.D.
SUMMARY Brain hemorrhage from an intracranial tumor was encountered in 7 males and 6 females dur-ing a 4-year period. In 5 patients, hemorrhage was responsible for the first signs of a previously unsuspectedneoplasm. The intracranial lesion was demonstrated by computed tomography (CT scanning) in each patient.Characteristic CT scan findings included: a neoplastic core (high or low density); small, multifocal clotsusually at the margin of the tumor; and, surrounding, often extensive, edema. Enhancement of the tumor tissuewith intravenous injection of 60% Hypaque was observed in the 8 patients so studied. The regions which wereenhanced had a peripheral distribution corresponding to the site of hemorrhage. Microscopic examinationdemonstrated 7 glioblastoma multiforme, 1 oligodendroglioma, 4 metastatic carcinomas (including 1 each ofbronchogenic carcinoma, melanoma, hypernephroma, and adrenal carcinoma), and 1 hemangiopericytoma.High-grade malignancy and extensive, abnormal vascularity appeared to be predisposing factors.
Stroke Vol 10, No 3, 1979
BRAIN HEMORRHAGE from an intracranialtumor is a well-recognized entity.121 Prior to the in-troduction of computed tomography (CT scanning),clinical diagnosis and non-invasive confirmation weredifficult. Since then a small number of patientsdiagnosed by CT scan have been reported.2' 22~25 Theobject of this investigation was to study the clinicalpresentation, CT scan findings, and neuropathologicalchanges in patients with a brain hemorrhage from anintracranial tumor.
Analysis of Cases
Thirteen adult patients with an intracranial tumorand concomitant brain hemorrhage were seen at theMontreal Neurological Institute from February 1974to February 1978. The 6 females and 7 males rangedin age from 18 to 80 years (mean: 53 years). The in-tracranial lesion was demonstrated by CT scan in eachpatient and neoplasia was confirmed by microscopicexamination of tissue obtained at operation and/orat postmortem examination.
Clinical Presentation
The clinical presentation of the 13 patients is sum-marized in table 1. Five were asymptomatic prior tohemorrhage and 8 had previous symptoms ofprogressive neurological dysfunction.
Deterioration in the level of consciousness was themost common neurological finding followinghemorrhage. Five patients became drowsy or ob-tunded and 7 became comatose. Progressive brainstem dysfunction, similar to that seen with uncal orcentral transtentorial herniation, developed in 9patients. Only one patient remained alert and orientedwithout evidence of brain stem compression.
Arterial blood pressure was found to be elevated in8 patients during or shortly following hemorrhage.Two of them had a previous history of hypertension.
From the Departments of Neurosurgery (Drs. Little and Dial),Neuroradiology (Dr. Belanger), and Neuropathology (Dr.Carpenter), Montreal Neurological Institute and McGill Uni-versity, Montreal, Quebec, Canada.
Reprints: Dr. Little, Dept. Neurosurgery, Montreal NeurologicalInstitute, 3801 University St., Montreal, Quebec H3A 2B4,Canada.
Investigations
CT Scan. The 13 patients had 26 scans. Intravenousinfusion of 60% Hypaque was carried out on 9 oc-casions in 8 patients. The results of these studies arelisted in tables 2 and 3.
CT scans on 6 patients were obtained prior tohemorrhage. The findings were similar to thosereported previously for brain tumors.25'26 Infusionstudies in 3 of them revealed enhancement of tumortissue, most marked at the periphery.
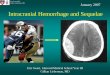
Ten patients had CT scans following hemorrhage,performed within 12 hours of the bleed in 9. The brainhemorrhage in 9 was multifocal with 2 or more clots inthe vicinity of the tumor (figs. 1, 2). Usually they werelocated at the interface between tumor and sur-rounding edematous brain. A large homogeneoushematoma obliterating most of the tumor wasobserved in 1 patient only (case 8). This patient had atumor arising from the diencephalic region. Brainhemorrhage distant from the tumor site was not seen,but extension into the ventricular system was presentin 4 patients. Enhancement of the tumor with in-travenous Hypaque was observed in the 6 patients sostudied (fig. 3). The regions which enhanced generallyhad a peripheral distribution corresponding to thelocation of the hematomas.
During the period 1974-78 ten of 172 patients withbrain hemorrhage diagnosed by CT scan were foundto have an associated tumor.
Cerebral Angiography. Cerebral angiography wascarried out in 6 patients, including 4 with aglioblastoma multiforme, 1 with an oligoden-droglioma and 1 with a metastatic adrenal carcinoma.Abnormal tumor vessels and early venous filling weredemonstrated in the patients with glioblastoma andmetastatic carcinoma. Aside from tumor mass effect,no pathological vascularity was seen in the patientwith the oligodendroglioma.
Treatment
Four patients did not have surgery because of exten-sive neoplastic disease. Treatment in these cases con-sisted of radiation and/or chemotherapy. Four otherpatients, including a 42-year old male with a
by guest on March 24, 2018
http://stroke.ahajournals.org/D
ownloaded from

284 STROKE VOL 10, No 3, MAY-JUNE 1979
TABLE 1 Clinical Presentation in Patients with an Intracranial Tumor and Concomitant Brain Hemorrhage
Casenumber Age/Sex
Symptoms prior tohemorrhage Onset
Neurological findings followinghemorrhage findings
Course(survival time)
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
18/f
48/f
53/f
56/m
57/m
68/m
80/f
19/f
71/m
52/m
55/f
71/m
42/m
headache; lethargy;R. hemiparesispersonality changes; lassitude;seizuresL. homonymous hemianopsia;L. hemiparesis; hypertensionnone
none
L. facial weakness; unsteadygaitconfusion; hypertension
headache; diplopia
headache; R. hemiparesis;seizuresconfusion; dysphasia
none
none
none
acute
acute
acute
acute
acute
acute
subacute
acute
subacute
acute
acute
acute
acute
obtunded; pathological posturing dead (2 weeks)
comatose; pathological posturing; dead (2 days)oculomotor palsycomatose; pathological posturing; fixed dead (1 day)pupils; BP 180/100 mm Hgalert; L. homonymous hemianopsia; dead (2 mos.)L. hemiparesis (mild)comatose; pathological posturing; oculomotor dead (5 days)palsy; BP 190/90 mm Hg
drowsy; L. homonymous hemianopsia; dead (5 weeks)L. hemiparesis; BP 180/100 mm Hg
drowsy; L. hemiparesis; meningismus dead (1 mo.)
comatose; pathological posturing; dead (3 weeks)oculomotor palsy; BP 160/110 mm Hgdrowsy; R. hemiparesis dead (3 weeks)
comatose; pathological posturing; dead (1 day)fixed pupils; BP 150/130 mm Hgdrowsy; dysarthria; R. facial palsy; alive (1 year)Babinski responses; BP 180/110 mm Hgcomatose; pathological posturing; Cheyne- dead (1 day)Stokes respiration; BP 200/100 mm Hg
comatose; pathological posturing; absent dead (2 days)oculocephalic and oculovestibular responses; .BP 240/100 mm Hg
hemangiopericytoma, were not treated surgicallybecause of severe brain stem injury secondary tocerebral herniation.
Craniotomy with evacuation of the clot and sub-total removal of a cerebral glioblastoma multiformewas done in 2 patients (cases 4 and 5). Another patient(case 11) had a suboccipital craniectomy with evacua-tion of a cerebellar hematoma and excision of ahypernephroma nodule. In these 3 patients, thehematomas were found to be multifocal and appearedto arise at the margin of the tumors. Hemorrhage hadextended into surrounding edematous brain tissue.Two patients with diencephalic tumors had insertion
of a ventricular drain to relieve acute obstructivehydrocephalus.
Results
The length of survival is listed in table 1. None ofthe patients receiving medical therapy alone livedlonger than 4 weeks. Two of the 3 patients decom-pressed surgically left the hospital. One subsequentlydied 2 months later from progressive growth of aglioblastoma multiforme. The other is alive 1 yearfollowing resection of a hypernephroma nodule andassociated cerebellar hematoma, but multiple brain
TABLE 2
Casenumber
CT Scan Findings
Location
Prior to HemorrhageFindings before
TumorAppearance
hemorrhage
EdemaEnhancement withhypaque infusion
1.
3.
7.
8.
9.
10.
hypothalmus;L. thalamus
R. temporal;R. basal ganglia
R. frontal
hypo thalamus
L. parieto-occipital;L. frontal; R. temporal
L. frontal
low density; ? cystic
isodense lesion
low density lesion
cystic lesion
multiple isodense lesions
low density lesion
not done
not done
not done
0 = none; + = mild; + + = moderate; + + + = marked.
by guest on March 24, 2018
http://stroke.ahajournals.org/D
ownloaded from

HEMORRHAGE FROM INTRACRANIAL TUMOR/Little et al. 285
TABLE 3 CT Scan Findings Following Hemorrhage
Cawinumber Location
Hem* to maFindinfi after hemorrhage
Appearance EdemaEnh&nQemAnt withhypaque infusion
1.
4.5,ftS,
11*12.13.
hypothalamus; L. thalamus
R. parietal
R. parieto-occipital
R. frontal
R. temporal
hypothalamus;R. basal ganglia
L. parieto-occipital
R. cerebellum
L. parieto-occipital
R. parieto-occipital
multifocal
multifocal
multifocal
multifocal
multifocal
discrete;homogeneous
multifocal
multifocal
multifocal
multifocal
not done
not done
+ +not done
not done
0 — none; + — mild; + + — moderate; + + + — marked.
metastases subsequently have been identified. The 2patients with a diencephalic tumor died 2 and 3 weeksfollowing hemorrhage without apparent benefit fromventricular drainage.
Pathology
The results of the microscopic examination oftumor tissue are listed in table 4. The gross findings inthe 11 patients undergoing postmortem examinationcorrelated closely with the CT scan findings.
Discussion
Intracranial tumors are a well-established cause ofhemorrhage into brain tissue. However, hemorrhage isbelieved to occur infrequently.1- '•10' "• u Tumors werefound in 2% of the 461 autopsied cases of "spontan-eous" intracerebral hemorrhage reported by Russell1*and less than 1% of the 225 reported by Mutlu et al.10
In our series, bleeding originated from an intracranialtumor in 6% of patients with brain hemorrhagediagnosed by CT scan. Diagnosis of brain tumor wasmade in 3 other patients having a CT scan only prior
FIGURE 1. CT scan of patient 1 following hemorrhageshows a miltifocal hematoma surrounding a low density,left thalamic tumor. There is moderate ventricular dilata-tion and periventricular edema.
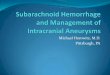
FIGURE 2. CT scan of patient 11 following hemorrhageshows a multifocal hematoma in the right cerebellar hemi-sphere. Extensive edema is demonstrated.
by guest on March 24, 2018
http://stroke.ahajournals.org/D
ownloaded from

286 STROKE VOL 10, No 3, MAY-JUNE 1979
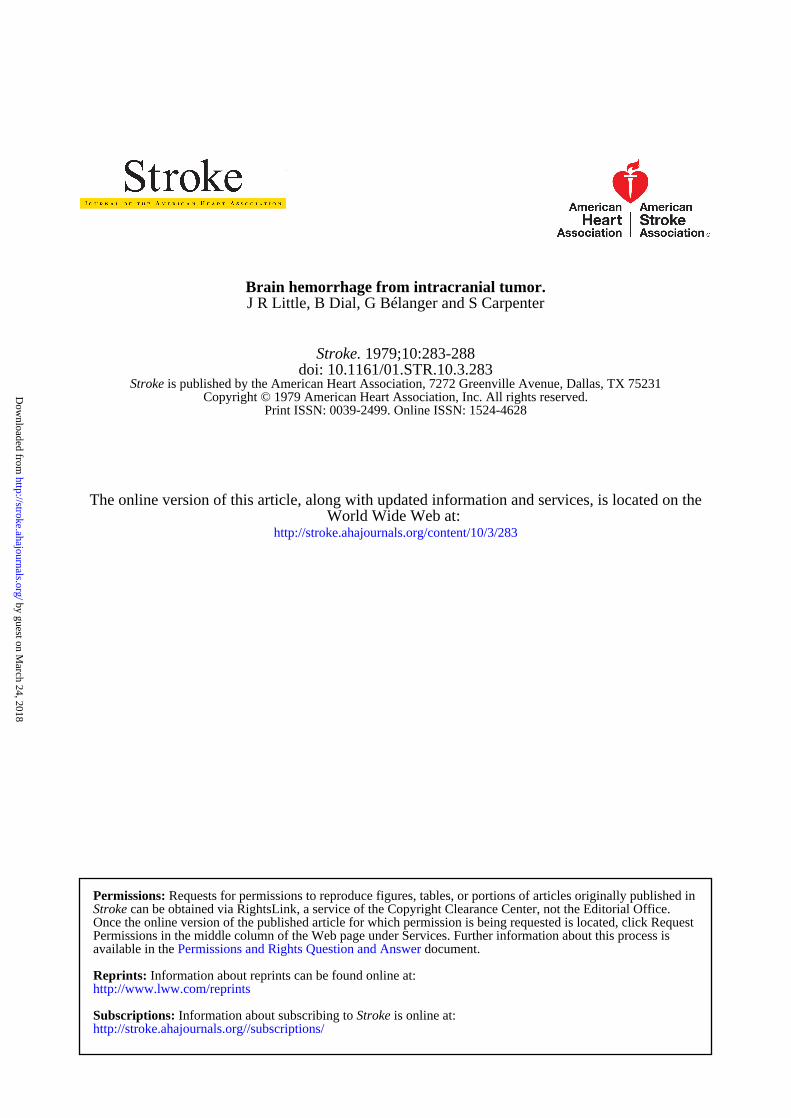
FIGURE 3. (Left) CT scan without Hypaque infusion of patient 4 performed I week followinghemorrhage. A partially attenuated, multifocal hematoma is present (arrow) at the periphery ofthe right parietal tumor. There is considerable brain edema surrounding the tumor andassociated hematoma. (Right) CTscan of same case with infusion ofHypaque. Enhancement atthe periphery of the tumor at sites distant from the resolving clot suggests the presence of con-siderable abnormal vascularity at the tumor-brain interface.
to hemorrhage. The higher incidence of tumor hemor-rhage reported here is related to the more accurateand reliable identification of brain hematoma with CT
TABLE 4 Microscopic Findings in Patients with an Intro-cranial Tumor and Concomitant Brain Hemorrhage
C u enumber
i.
2.
3.
4.
5.
6.7.
8.
9.
10.
11.
12.
13.
Microeoopio 1Tumor typ«
glioblastoma multiforme
glioblastoma multiforme
glioblastoma multiforme
glioblastoma multiforme
glioblastoma multiforme
glioblastoma multiformeglioblastoma multiforme
oligodendroglioma
bronchogenic carcinoma(anaplastic)
melanoma
hypernephroma
adrenal carcinoma
hemangiopericytoma
Vasculanty
highly vascular withfoci of large, thin-walled vessels; mod-erate to extensiveendothelial prolifera-tion; multifocal areasof necrosis
numerous clusters ofthin-walled vessels;mild endothelialproliferation
highly vascular
moderately vascularwith clusters of thin-walled vessels
highly vascular
focal clusters ofthin-walled vessels
highly vascular withnumerous thin-walledvessels throughouttumor
scanning. It suggests that this phenomenon is morecommon than previously believed.
The mechanism of bleeding has not been defined,but high-grade malignancy and extensive, abnormalvascularity appear to be predisposing factors."113> "• "Brain hemorrhage from metastatic and primary intra-cranial malignant tumors is encountered approxi-mately with equal frequency. Hemorrhage from abenign neoplasm, such as a meningioma, is rareand usually is attributed to angiomatous tumor ves-sels.*1 *• •• " Hypertension and/or coagulopathy couldbe important contributing factors in these patients.Elevated systemic arterial pressure was observed in 8of our patients during or shortly following hemor-rhage, however, it was not possible to determinewhether the hypertension was the cause or result of theintracranial bleed. None of our patients had clinicalevidence of a generalized bleeding disorder and nonehad received anticoagulants prior to the hemorrhage.
Glioblastoma multiforme was found in 7 of our 8patients with glial neoplasia. The hemorrhagicpropensity of glioblastomas has been describedpreviously.8' "• "• " • " According to Zulch,11 thepathogenesis of ruptured blood vessels is under-standable in view of" the "huge, disorderly, fistulousvessels" invariably present. Proliferation of en-dothelium, clusters of dilated thin-walled vessels, andareas of necrosis were common findings in tumortissue examined microscopically.
Hemorrhage into a well-differentiated astrocytomais uncommon12'18 and was not seen in our investiga-tion. This is likely related to the infrequent occurrenceof pathological blood vessels and absence of necrosis
by guest on March 24, 2018
http://stroke.ahajournals.org/D
ownloaded from

HEMORRHAGE FROM INTRACRANIAL TUMOR/Little et al. 287
in these tumors. Oligodendrogliomas appear toproduce bleeding more frequently thanastrocytomas.16 The reason for this is unclear,although the presence of numerous dilated, thin-walled vessels (i.e., glomeruloid formation) and en-dothelial proliferation as observed in our patient havebeen implicated as important predisposing factors.
Bronchogenic carcinoma, melanoma, and hy-pernephroma each occurred in one patient. Thesetumors, as well as choriocarcinoma, are implicatedmost frequently when brain hemorrhage results from ametastatic lesion.2' "•13-17~19 The incidence of bleedingfrom metastatic choriocarcinoma, a rare tumorusually found in young females, is particularly high,occurring in more than 50% of patients with a brainmetastasis. In most instances of metastatic tumor,hemorrhage is thought to arise from the rapidly grow-ing peripheral portion of the tumor or from adjacent,damaged. brain tissue.8 The inherent capacity ofchoriocarcinoma for vascular invasion appears to be aparticularly important factor in the pathogenesis ofhemorrhage with this neoplasm.18-19
Benign;meningeal tumors constitute a rare but im-portant clause of intracranial hemorrhage.4'6> 9> n
Highly Vascular meningotheliomatous and angio-blastic meningiomas are most frequently involved.Gruszkiewicz6 et al. stated that "nearly all reportedcases of meningioma associated with intracranialhemorrhage deal with subarachnoid hemorrhagerather than intracerebral hemorrhage or hemorrhagewithin the substance of the tumor itself." One patientwith extensive intracerebral hemorrhage from ahemangiopericytoma arising from the falx cerebri wasincluded in our series. Numerous thin-walled vesselswere observed on microscopic examination of thistumor.
Bleeding from a tumor usually is symptomatic andmay be responsible for the first signs of a previouslyunsuspected neoplasm.3- 5- 7- 13-16-22 The bleedingsimulates a primary vascular disorder such as hyper-tensive hemorrhage or ruptured saccular aneurysm.Five of our 13 patients were asymptomatic prior tohemorrhage. Likewise, the existence of a tumor wasnot suspected in 5 of 12 patients described by Padt etal.13 with bleeding into a brain tumor. Similar findingshave been reported by other investigators.3-5- '•16
The presence of tumor was not clear-cut in 8 of the10 non-infusion CT scans performed following hemor-rhage. A high density or low density neoplastic corewith small, multifocal clots at its periphery were con-sistently demonstrated. Usually there was extensivesurrounding edema. These features were useful indifferentiating tumor hemorrhage from the othermore common causes of brain hemorrhage (i.e.,hypertension, saccular aneurysm, etc.). The locationof the hematomas (i.e., in the cerebral hemispheres)was not typical of hypertensive hemorrhage, the mostcommon cause of "spontaneous" intracerebralhemorrhage.
Enhancement with an intravenous Hypaque injec-tion was observed in 8 patients. This technique wasuseful in confirming the diagnosis of tumor prior to
hemorrhage and demonstrated the abundantvascularity of the neoplasms involved. The location ofthe hematomas generally corresponded to the areas ofenhancement, that is, at the periphery of the tumor.Five of the 6 patients with peritumoral enhancementfollowing hemorrhage had the study within 24 hoursof the bleed. Consequently, the enhancement seen wasconsidered the result of abnormal vascularity existingprior to the hemorrhage and not the enhancementcommonly present 6 days or longer following hemor-rhage from other causes.27 The patient (case 4) whohad infusion and plain CT scans 1 week followinghemorrhage, had a complete ring of enhancementaround the tumor which included areas distant fromthe clot. Although enhancement in the vicinity of thehematoma could have been the result of thehemorrhage, the more distant enhancement likely wasrelated to abnormal tumor vessels at the tumor-braininterface.
Emergency surgical decompression is sometimeshelpful in those patients without previous demonstra-tion of extensive malignant disease and withoutclinical findings of severe brain stem injury secondaryto herniation. The hemispheric location of most ofthese tumors and associated hematomas allowsrelatively easy access and removal. The excision of anoccasional benign tumor, such as a meningioma, orsolitary metastatic nodule, may result in long-termsurvival.28
References
1. Falconer MA: The pathology of spontaneous intracranialhemorrhage. Proc Roy Soc Med 47: 693-704, 1954
2. Gildersleeve N, Koo AH, McDonald CJ: Metastatic tumor pre-senting as intracerebral hemorrhage. Computed Tomography124: 109-112, 1977
3. Globus JH, Saperstein M: Massive hemorrhage into braintumor. JAMA 120: 348-352, 1942
4. Goran A, Ciminello VJ, Fisher RG: Hemorrhage intomeningiomas. Arch Neurol 13: 65-69, 1965
5. Gross SW, Bender MB: Massive hemorrhage in brain tumors.Arch Neurol Psychiat 60: 612-617, 1948
6. Gruszkiewicz J, Doron Y, Gellei B, et al: Massive intracerebralbleeding due to supratentorial meningioma. Neurochir 12:107-111, 1969
7. Hyland HH: Nonaneurysmal intracranial hemorrhage.Neurology (Minneap) 11: 165-168, 1961
8. Mandybur TI: Intracranial hemorrhage caused by metastatictumors. Neurology (Minneap) 27: 650-655, 1977
9. Modesti LM, Binet EF, Collins GH: Meningiomas causingspontaneous intracranial hematomas. J Neurosurg 45:437-441, 1976
10. Mutlu N, Berry RG, Alpers BJ: Massive cerebral hemorrhage.Arch Neurol 8: 644-661, 1963
11. Nakao S, Sato S, Ban S, et al: Massive intracerebralhemorrhage caused by angioblastic meningioma. Surg Neurol7: 245-248, 1977
12. Oldberg E: Hemorrhage into gliomas. Arch Neurol Psychiat30: 1061-1073, 1933
13. Padt JP, De Reuck J, Vander Eecken H: Intracerebralhemorrhage as initial symptom of a brain tumor. Acta NeurolBelg 73: 241-251, 1973
14. Russell DS: The pathology of spontaneous intracranialhemorrhage. Proc Roy Soc Med 47: 689-693, 1954
15. Russell DS, Rubinstein LS: Pathology of Tumors of the Ner-vous System. Baltimore, Williams and Wilkins, 1971 (3rd ed),pp 147-154
16. Schultz OT: Sudden death due to hemorrhage into silentcerebral gliomas. Am J Surg 30: 148-153, 1935
by guest on March 24, 2018
http://stroke.ahajournals.org/D
ownloaded from

288 STROKE VOL 10, No 3, MAY-JUNE 1979
17. Scott M: Spontaneous intracerebral hematoma caused bycerebral neoplasms. J Neurosurg 42: 338-342, 1975
18. Shuangshoti S, Panyathanya R, Wichienkur P: Intracranialmetastases from unsuspected choriocarcinoma. Neurology(Minneap) 24: 649-654, 1974
19. Vaughan HG, Howard RG: Intracranial hemorrhage due tometastatic chorionepithelioma. Neurology (Minneap) 12:771-777, 1962
20. Zimmerman HM: Cerebral apoplexy: mechanism and differen-tial diagnosis. NY State J Med 49: 2153-2157, 1949
21. Zulch KJ: Neuropathology of intracranial hemorrhage. ProgBrain Res 30: 151-165, 1968
22. Weisberg LA, Nice CN: Intracranial tumors simulating thepresentation of cerebrovascular syndromes. JAMA 63: 517,1977
23. Hayward RD, O'Reilly, GVA: Intracerebral hemorrhage.Lancet 1: 1-4, 1976
24. Little JR, Blomquist GA, Ethier R: Intraventricularhemorrhage in adults. Surg Neurol 8: 143-149, 1977
25. New PJ, Scott W: Computed Tomography of the Brain and Or-bit. Baltimore, Williams and Wilkins, 1975, pp 123-257
26. Weisbert LA, Nice C, Katz M: Cerebral ComputedTomography — A Text-Atlas. Philadelphia, WB Saunders,1978, pp 105-161
27. Zimmerman RD, Leeds NE, Naidlich TP: Ring blushassociated with intracerebral hematoma. Radiology 122:707-711, 1977
28. Salerno TA, Munro DD, Little JR: Surgical treatment ofbronchogenic carcinoma with a brain metastasis. J Neurosurg48: 350-354, 1978
Effect of Altered Availability of Energy-YieldingSubstrates Upon Survival from Hypoxia in Mice
JEFFREY R. KIRSCH, B.S. AND LOUIS G. D'ALECY, D.M.D., P H . D .
SUMMARY The duration of survival during a hypoxic or ischemic incident can be altered by barbiturateanesthesia. If this effect on the brain results from a reduction in lactic acid production by hypoxia, then asimilar protective effect may be produced by altering substrate availability. Six groups of mice were subjectedto hypoxia (4 to 5% O2, balance N2) at 30 to 35°C: 1. Hypoglycemia was induced by 2 U insulin injected ip 30min prior to hypoxia. 2. Ketotic hypoglycemia was induced by fasting 85 to 90 hours prior to hypoxia. 3.Hyperglycemia was induced by iv dextrose. 4. Diabetic-ketotic-hyperglycemia was induced by iv alloxan 5days prior to hypoxia. 5. One group was given both the insulin and dextrose in the above sequence. 6. In con-trols, saline was given iv or ip when appropriate. The mean survival time for ketotic-hypoglycemic and diabetic-ketotic-hyperglycemic mice was significantly higher than control. The mean survival time for the insulin-hypoglycemic mice was significantly lower than control. The remaining groups showed no difference from con-trol. The observed improvement in survival time from hypoxia seen in the ketotic animals suggests that duringhypoxia, the brain metabolizes ketones selectively and minimizes the production of lactic acid to maintainneuronal viability.
Stroke Vol 10, No 3, 1979
BARBITURATE ANESTHESIA1 5 and alterationsin blood glucose6'8 have been reported to modify sur-vival time or brain damage in various animal modelsof brain hypoxia and ischemia. If the increase in sur-vival time6 and the decrease in brain injury8 are relatedto a reduction in hypoxia-induced production of lacticacid, then supplying the brain with a substrate otherthan glucose may afford protection from hypoxia.Under normal circumstances, the mammalian brain isan obligatory glucose user. During a prolonged fast,or in the uncontrolled diabetic state, ketosis developsand the brain adapts by metabolizing acetoacetate andbeta-hydroxybutyrate.9-10 The metabolism of theseketones requires the consumption of oxygen, but doesnot involve the production of lactic acid. Lactic acid,itself, or the hydrogen ion changes associated with theproduction of lactic acid have been suggested as a
From the Department of Physiology, The University of MichiganMedical School, Ann Arbor, MI 48109.
Supported by the American and Michigan Heart Associations;U.S. Public Health Service Grants NS12386, HL 20399 and AM20572.
possible mediator of the neuronal damage associatedwith ischemia or hypoxia.7'8> u It is assumed in thepresent study and previous studies using this animalmodel4'5 that neuronal metabolic derangements areresponsible for the death of the animal during hypox-ia. We tested the hypothesis that an alteration in thetype or amount of substrate available for energy pro-duction could increase survival time during hypoxia.
Materials and Methods
The animal model used has been previouslydescribed by Wilhjelm and Arnfred4 and Steen andMichenfelder.5 Adult, male Sprague-Dawley albinomice (ICR-ARS-HA) weighing between 15 and 30 gwere pretreated and then subjected to hypoxia (4 to5% oxygen). The pretreatment involved a modifica-tion in the availability of substrate for the metabolismof brain. This modification was induced by combina-tion of dextrose infusion, insulin injection, fasting, orexperimental alloxan-diabetes. For each group thesurvival time, and blood glucose and ketone levelswere determined.
by guest on March 24, 2018
http://stroke.ahajournals.org/D
ownloaded from
J R Little, B Dial, G Bélanger and S CarpenterBrain hemorrhage from intracranial tumor.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1979 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.10.3.283
1979;10:283-288Stroke.
http://stroke.ahajournals.org/content/10/3/283World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on March 24, 2018
http://stroke.ahajournals.org/D
ownloaded from