Embed Size (px)
Citation preview
1007
ratio-then surely we have arrived almost at theend of our endeavour.
Will our work stand the final test: Does lead arrestmalignant disease in man ? Here, indeed, is the cruxof the central problem. I can assure you that inthis respect also we have the fullest confirmation ofall I have said. By " fullest " I do not mean that wecan cure every case of malignant disease. We cannot;that, unfortunately, will never be possible, as allthose who deal with the disease must know. In thecure we may sometimes kill. I have in mind twocases, the first that of a young man with diffusesarcoma of the stomach, as proved by laparotomyand histological section. The treatment by intra-venous injections of lead caused total liquefaction ofthe stomach, and he died with acute peritonealsymptoms. At the post-mortem examination Prof.Glynn could find no stomach, simply a mush of deadtissue. The second case was that of a woman with alarge, rapidly-growing post-cricoid carcinoma. Aftertreatment the entire growth became cedematous andshe was suffocated. At the post-mortem examinationit was found that the entire tumour had undergoneacute necrosis.Some would say, What further evidence than
that is required ? P If it is, we have it in the fifty orso patients who are believed well, out of about 200,mostly hopeless, cases treated. We have not selectedour patients in any way. We have treated practicallyall who have been sent to us. Many have died withina few weeks of their arrival, before treatment had beenhardly more than just begun.
I know you will want to hear very much about oursuccesses. In the next month or so these will bepublished in THE LANCET. However, I may perhapsrisk wearying you and mention two, for we havebeen fortunate enough to make for them yesterdayand to-day days of thanksgiving.On Nov. 9th, 1920-five years ago yesterday-a woman
was admitted to my maternity ward at the Royal Infirmary,Liverpool, for her confinement, which took place a few dayslater. She was suffering with an extensive, ulceratedcarcinoma of the left breast with glands in the axilla.Operation had been considered useless six months previouslyby two of my surgical colleagues. The growth had beenaccelerated during pregnancy, as is usual in these circum-stances. I
I was looking for just such a hopeless case. A section wasprepared from a piece of tissue adjacent to the ulceratedarea, and intravenous injections of lead were given. Not only ’
is the patient well to-day, five years and one day later, butalso she has had two more babies in the interval, both ofwhom she has suckled at the breast that was affected.
For sentimental reasons of a different characterI may tell you about another patient who is now38 years of age.
This lady was sent to me over a year ago. She hadsubmitted to an exploratory operation at the hands ofanother surgeon. He found the abdomen full of malignantgrowth, which he correctly diagnosed as sarcoma, andpromptly closed his incision. When she came to Liverpool, ’’’,thin and ill, I reopened the abdomen to obtain a piece ofgrowth for section, for this had not been done at the formeroperation. I, too, found the entire abdomen involved.Intestines were mixed up in the growth, and the wholeoutlook seemed most serious. In ordinary circumstances shehad a few weeks to live, for sections showed the growth tobe a most rapidly growing spindle-cell sarcoma. Treatmentwith lead injections has led to a considerable decrease in thesize of the tumour, while the patient has herself increased inweight by 21 lb., and is now in robust health and withouta symptom. She has been married to-day-November 10th.
CONCLUSION.I have undertaken to present to you some of the
confirmatory evidence obtained by a band of fellow-workers, that the hypothesis expounded is not onlycorrect in its essential particulars, but also from everypossible angle, including that of the ultimate test,it appears to be-may I say-proven.
I set out to show you that malignant neoplasiais a specific growth process in that it is a reversionon the part of the starving cell to the nutriment-seeking proclivities of its ancestral type, the chorionicepithelium.
A comparison between the chemical constitutionof different tissues in regard to the factors concernedin growth processes demonstrates clearly not onlythat malignant tumours are richer in this respectthan the corresponding normal structures and innocentneoplasms of the same parts, but also that the physio-logically malignant chorionic villi show even highervalues than pathologically cancerous tissues. Thechorionic epithelium is super-malignant.
In the search for a substance that will arrest orhave a specific lethal action on cells which possessthe chemical constitution associated with malignancywe have found only lead. This metal is specificallyactive in regard to the chorionic epithelium, to thecells of cancerous growth, to normal embryonicgrowth, and to mature cells rich in phosphatides.Some day we hope that a substance, less toxic to
the organs of the patient that are rich in phosphatides,and even more effective than lead in arresting anddestroying cancerous tissues, will be found. If thatshould ever happen, and it is not unlikely, we shallhave still further confirmation of our belief thatcauses are as nothing in comparison with the impor-tance of the realisation that malignant neoplasia isa specific process of the nature, and subject to thecontrol I have described.
Bradshaw LectureON
GASTRO-JEJUNOSTOMY.Delivered at the Royal College of Surgeons of England
on Nov. 11th, 1925,BY JAMES SHERREN, C.B.E., F.R.C.S. ENG.,
VICE-PRESIDENT OF THE COLLEGE ; SURGEON TO THELONDON HOSPITAL.
I MUST apologise for having selected an operationas my subject. I did so because of a firm belief thatgastro-jejunostomy has had a more profound influenceon abdominal surgery, and has done as much, if notmore, for the good of the human race than any surgicalprocedure. On the other hand, carried out in unsuitablecases, or in suitable cases in an incorrect manner, ithas, I regret to say, done as much, if not more harm,not only to the patient but to surgery in generalthan any operation. In suitable cases and correctlyapplied it has altered the whole outlook of countlesschronic dyspeptics, and saved numerous valued livesfor long service to the community. In addition toits widespread influence on abdominal surgery, thelight it sheds on the aetiology of ulcerative lesions ofthe stomach and duodenum and on the cause of theirsymptoms was also a factor which convinced me, andI hope will convince you, that its study is eminentlysuitable for a Bradshaw lecture.The present time seems opportune to review the
matter, as from many sides we hear of its failure tocure conditions that are found curable by its aid inthe hands of other surgeons. We have large andcomplicated procedures devised to supplant it, pro-cedures that carry with them a mortality greater thanthat of the operation under discussion, and I ventureto say that the death-rate of these would at leastapproximate to that of gastro-jejunostomy and to allits unsuccessful cases if they were considered as
fatalities. Not even the most ardent advocate ofthese new operations would claim that every survivorwas cured.
I should like first to draw your attention to a fewpoints of historical interest. It was first carried outon Sept. 28th, 1881, in Vienna, by Anton W61fer,lwhile assistant in Billroth’s clinic. The patient wasa male of 38, Michael Gold, surely a name to beremembered in the annals of surgery. He was suffer-ing from pyloric carcinoma. Convalescence was
uneventful and he was reported well four weeks later.The second case was done by Billroth himself on
1008
Oct. 2nd, the patient being a man of 45. Biliousvomiting supervened the following day and continueduntil death on the tenth day. A post-mortem examina-tion showed spur formation. Thus, the distressing post-operative symptom of regurgitant vomiting appearedearly in its history. The course of abdominal surgerymight have been different had this been the first case
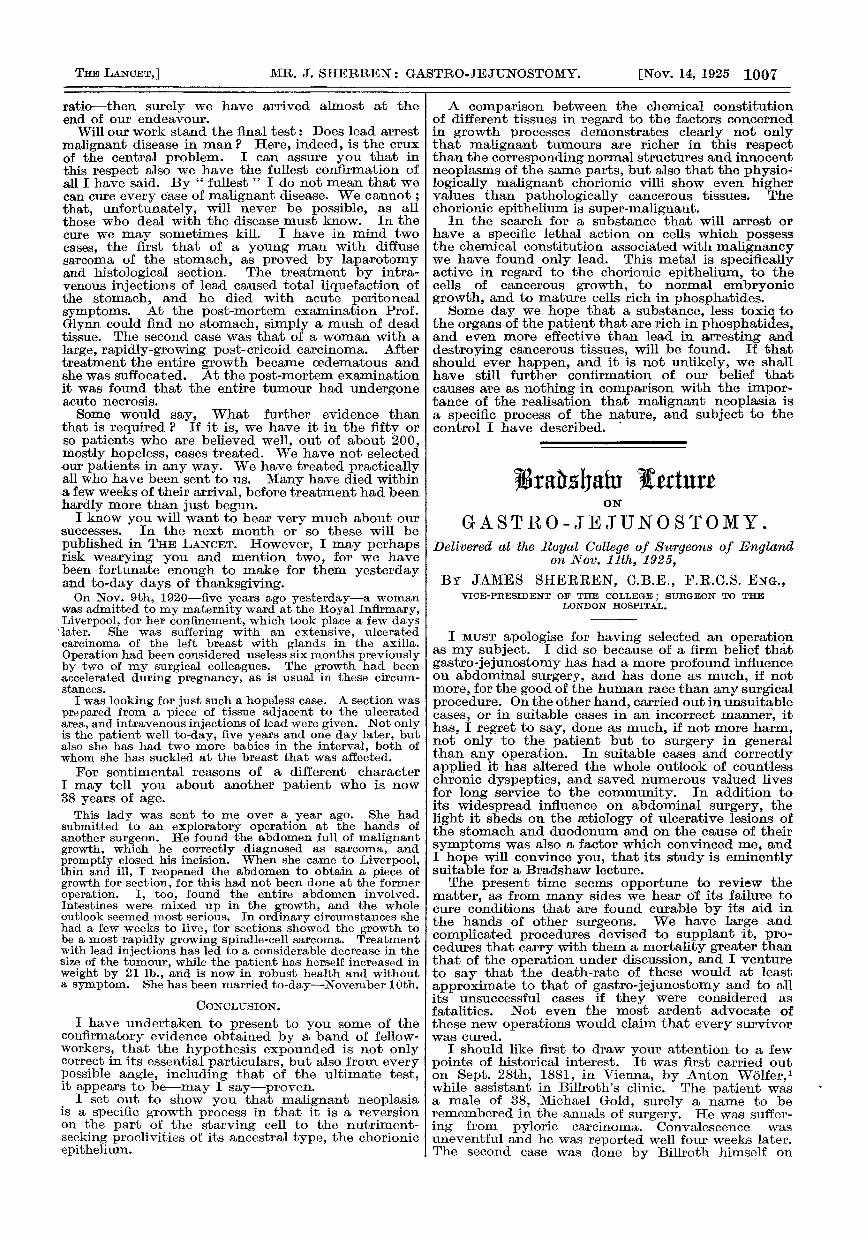
FIG. 1.
Showing the posterior surface of the stomach brought throughthe mesocolon and held vertically from the greater to lessercurvature, ready for the application of the clamp.
operated on. A surgeon must be thoroughly con-vinced of the soundness of his conception and itspotentialities who would attempt it a second timein the face of such a result. The first successful gastro-jejunostomy in this country was carried out by Barker2for carcinoma of the pylorus on Jan. 5th, 1886. Aday previously Morse,3 assistant surgeon to theNorfolk and Norwich Hospital, had done a similaroperation and both surgeons sutured the jejunum tothe stomach before opening them. It was firstperformed in this country at the London Hospitalby Reeves 4 on May 9th, 1885, on a woman of 40,with carcinoma of the pylorus. Tt is difficult fromthe brief account to follow exactly what was done,but it was a two-stage operation. I have been unableto obtain any information other than the short notepublished, and a careful search of the hospital recordsand operation books has not enabled me to trace thepatient.
Carried out first for the relief of symptoms inirremovable carcinoma of the pylorus, it has beenused in the treatment of most abdominal ills and,in cases that have come ’mer my own observation,has been done or advised for the vomiting of preg-nancy, disease of the spine and spinal cord, of thekidneys, and even of the middle ear and brain. Itwas not until llyears after its introduction that Doyen 5employed it in the treatment of chronic gastric ulcer.This is recorded in a most instructive paper. He wasled to undertake the operation on the suppositionthat pyloric spasm played a large part in producingsymptoms. The first patient was operated on in 1892for the round type of chronic gastric ulcer, and wasquite well at the time of his report three years later ;during this interval he had operated on 14 otherpatients suffering from chronic gastric ulcer withoutpyloric stenosis. He was rapidly followed by others,and on March 22nd, 1893, it was first employed byCodiviUa in the treatment of chronic duodenal ulcer.This was in a male of 40 who was quite well five yearslater, and it was not until after this, to be exact onMay 5th, 1898, that the second case was operatedon by this surgeon. Surely an example of surgical
patience we should all take to heart. If every operationwere tested for a few years before being generallyemployed many procedures would be justly unknownto any but their inventors.
i The first gastro-jejunostomy was anterior with along loop, the jeiunum being sutured to the stomachalong a horizontal line with its proximal portiontowards the pylorus (retro-peristaltic). In 1885 vonHacker introduced the posterior operation, leavinga loop 20 cm. from the duodeno-jejunal flexure.It was 15 years later that Petersen further improvedit by shortening the loop and adopting the iso-peristaltic positipn of the jejunum introduced byRockwitz 9 in 1887.We thus see the international character of surgical
work. This operation was conceived in Vienna andits first modifications came from the continent ofEurope. Its extension to the treatment of chronicgastric ulcer we owe to the French, to chronic duodenalto the Italians. I do not think, however, we shallbe claiming too much for the English-speaking racesif we say it was brought to perfection by them, andthe names of Moynihan and Mayo will always beassociated with this.
It is impossible to give the many variations thathave been advised and carried out from time to time,but the next great advance was the advocacy of thevertical position of the anastomosis by Sir BerkeleyMoynihan. This was in an important paper entitled" Gastro-enterostomy and After,"’’ which was the firstserious estimation of the value of this operation andits after-results. It contains these striking words:" I am an ardent and a sanguine advocate of thisoperation, than which I think there is none in allsurgery more completely satisfactory." When carriedout in suitable cases this is an opinion which I to-daystill share. It is difficult to understand the veryconflicting results reported as obtained after gastro-jejunostomy except on the supposition that they aredue to want of appreciation of its indications and ofthe correct method of carrying it out; if success is to
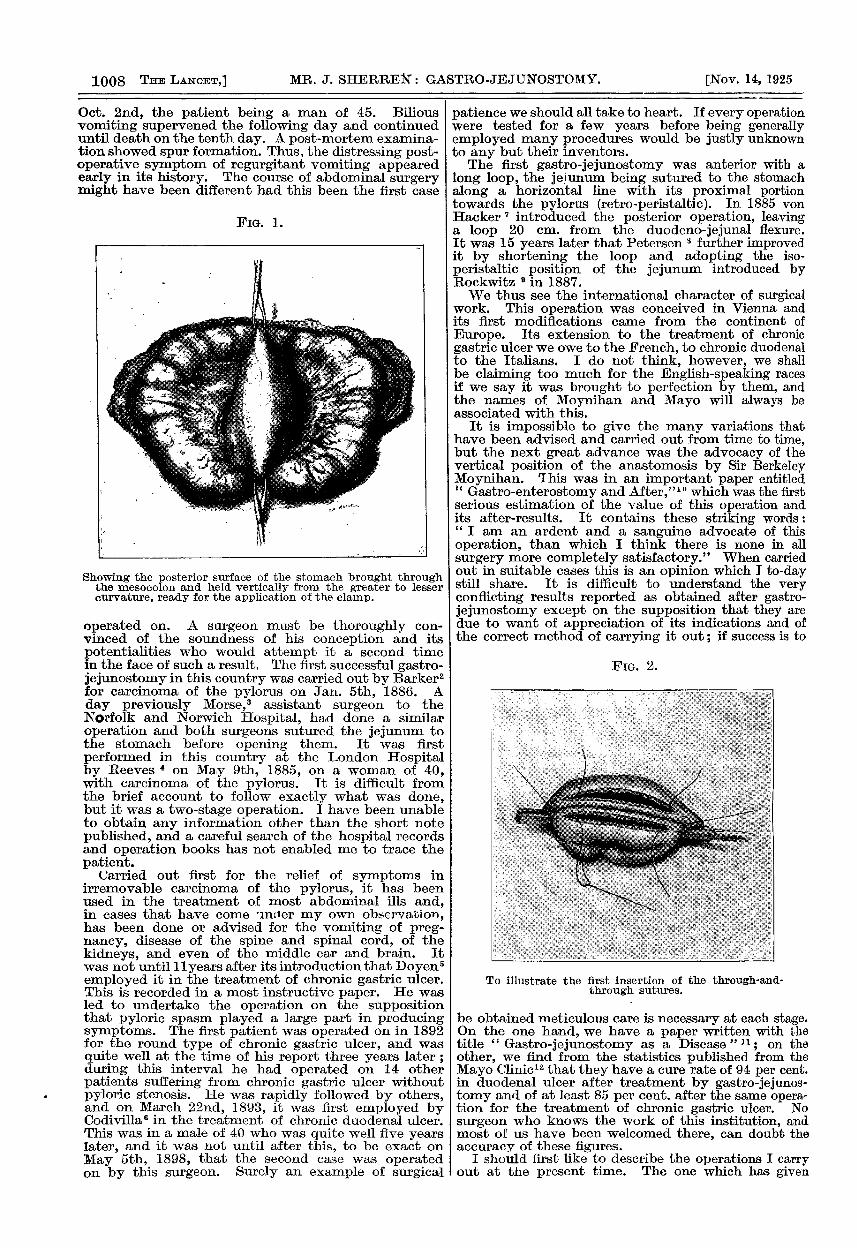
FiG. 2.
To illustrate the first insertion of the through-and-through sutures.
be obtained meticulous care is necessary at each stage.On the one hand, we have a paper written with thetitle " Gastro-jejunostomy as a Disease" 11; on theother, we find from the statistics published from theMayo Clinic" that they have a cure rate of 94 per cent.in duodenal ulcer after treatment by gastro-jejunos-tomy and of at least 85 per cent. after the same opera-tion for the treatment of chronic gastric ulcer. Nosurgeon who knows the work of this institution, andmost of us have been welcomed there, can doubt theaccuracy of these figures.
I should first like to describe the operations I carryout at the present time. The one which has given

1009
uniform success in my hands is the posterior retrocolicwith vertical opening. The jejunum is taken at theduodeno-jejunal flexure and brought to the stomachso as to lie easily without tension on the one handor looping on the other ; the exact part therefore ofthe jejunum which is anastomosed to the stomachdepends on the size and position of that organ. An
Fl&. 3.
Showing the posterior surface of the stomach exposed and broughtout through the gastro-colic omentum, the jejunum beingbrought to it in front of the colon.
opening is made in the transverse mesocolonimmediately above the flexure, sufficiently large thatits edges can be easily sutured to the stomach after theanastomosis has been made without causing deformityto it or the jejunum. The stomach just to the rightof the cardiac orifice is clamped vertically from thegreater to the lesser curvature (Fig. 1). If the operationis being carried out for a chronic gastric ulcer theanastomosis must be to its cardiac side ; making itelsewhere is useless and the cause of many failures.This is even now not recognised universally, andsufficient stress has not been laid on this elementaryfact. However the curative results are brought about,good cannot be anticipated when the opening is madeto the pyloric side of the ulcer.The jejunum is brought to the stomach without a
clamp and fixed to it at either end by stay suturesplaced so as to secure its opening being exactly at theantimesenteric border and thereby avoid any rotationof the gut on its longitudinal axis. I find this muchsimpler to accomplish if no clamp is placed on thejejunum. Further, as I have stated before, it ispossible that pressure of the clamp may in someinstances be one of the causes of jejunal ulceration.No rule can be laid down with regard to the size of theanastomosis; it should extend when possible fromthe greater to the lesser curvature. This, of course,cannot be done if there is great dilatation ; here,while falling short of the lesser, it should reach to thegreater curvature. The viscera are then openedand the stitch through all their coats inserted. It ismost important to get absolute apposition of mucousmembrane so that I do not remove any that isredundant, and pay particular attention to the endsof the incision, uniting these first (Fig. 2). Nowadaysthe rare cases of gastro-jejunal ulcer are usually foundat either end of the anastomosis, I believe due tofailure of primary union of mucous membrane here,and it is for this reason that great care is necessary atthese points. Before inserting the anterior layer ofsutures I loosen the clamp and look for bleedingpoints. Finally the edges of the opening in the meso-
colon are carefully united to the stomach at leasthalf an inch away from the line of anastomosis.Where the mesocolon is very fatty, and the fact thatthe great omentum is in similar condition makes theposterior operation advisable, I carry this out as thefirst stage, so as to be certain that the oozing edgesshall be well removed from the suture line and soavoid puckering or obstruction from adhesions later.Special care is necessary in dealing with these edges ; -,all oozing should be stopped and the points I havestressed adhered to to avoid the possibility of latepost-operative vomiting.
It may, however, be impossible or unwise toperform this retrocolic posterior operation on accountof changes in the mesocolon, or adhesions of jejunumto its under surface. If the mesocolon is loaded withfat, or if it is shrunken and adherent to the posteriorabdominal wall, operation through an opening in itmay lead to severe late regurgitant vomiting. I amalso very much averse for the same reason, whena considerable length of the jejunum is united to theunder surface of the mesocolon, to separate it, as theseadhesions may re-form and cause obstruction. I alsothink it is unwise to attempt the retrocolic operationif an opening of sufficient size cannot be obtainedwithout dividing one of the vascular arcades. Forseveral years I have carried out an antecolic posterioroperation with a short loop in this type of case. Theposterior surface of the stomach is exposed by anopening in the gastrocolic omentum, and thejejunum, brought in front of the colon at the splenicflexure, is united vertically to it (Fig. 3). In my handsthis has given excellent results. When the posteriorsurface of the stomach is adherent and partialgastrectomy is unwise or not indicated, I do theanterior no-loop operation that I first performed in1904 and published in 1907,13 bringing the jejunumto the anterior surface of the stomach through thetransverse mesocolon and gastro-colic omentum
FIG. 4.
Illustrating anterior no-loop gastro-jejunostomy, the jejunumbeing brought to the anterior surface of the stomach throughthe mesocolon and gastro-colic omentum.
(Fig. 4). The opening is finally sutured around theanastomosis in the way I have described in dealingwith the normal posterior operation. I have usedLukens’ special catgut, No. 0, for suturing gastro-intestinal anastomoses for many years with uniformsuccess.
I believe that many of the recorded bad resultsof this operation are due to the way in which it isperformed. It is not enough to unite the jejunumto the stomach anywhere, the spot must be chosen asI have indicated, and the opening must be of sufficientsize. I should like to illustrate published examples of
1010
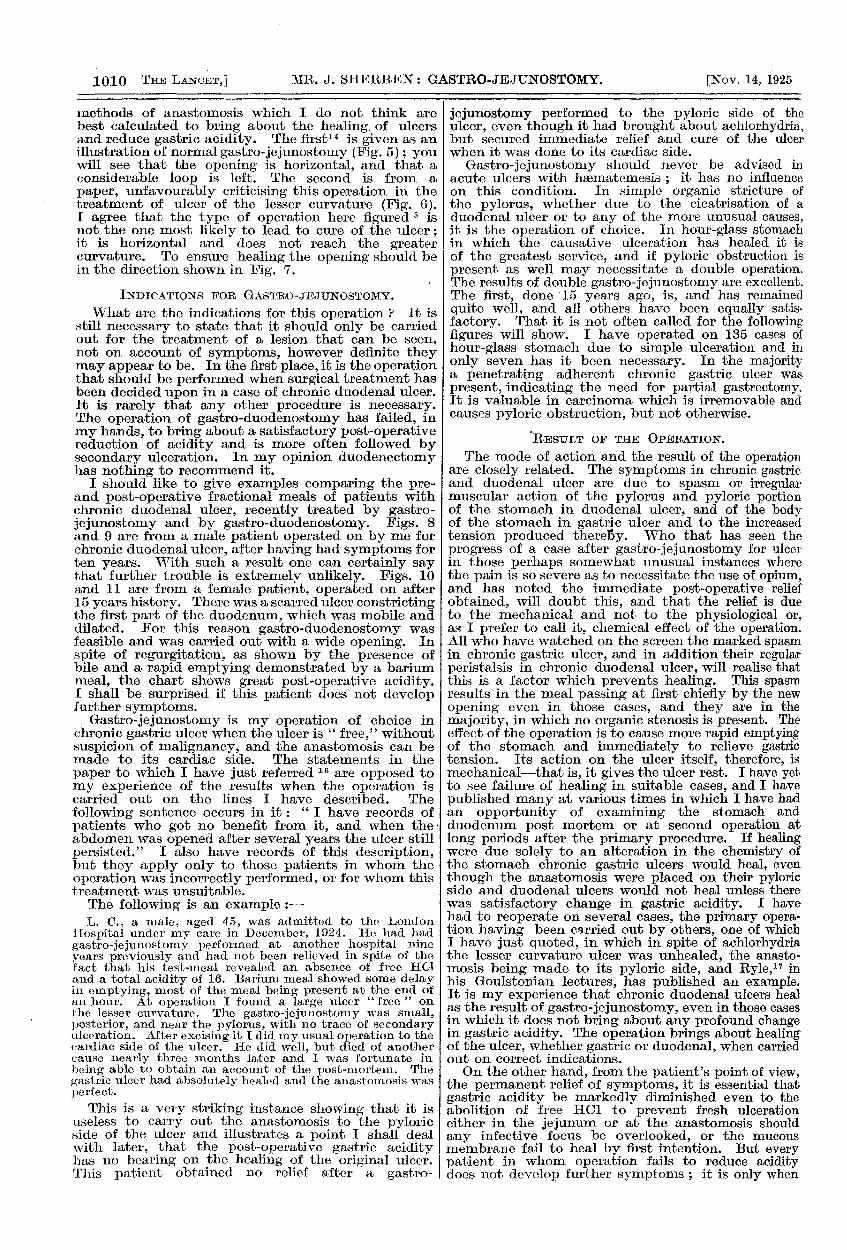
methods of anastomosis which I do not think arebest calculated to bring about the healing of ulcersand reduce gastric acidity. The first14 is given as anillustration of normal gastro-jejunostomy (Fig. 5) ; youwill see that the opening is horizontal, and that aconsiderable loop is left. The second is from a
paper, unfavourably criticising this operation in thetreatment of ulcer of the lesser curvature (Fig. 6).I agree that the type of operation here figured s isnot the one most likely to lead to cure of the ulcer;it is horizontal and does not reach the greatercurvature. To ensure healing the opening should bein the direction shown in Fig. 7.
INDICATIONS FOR GASTRO-JEJUNOSTOMY.What are the indications for this operation ? t It is
still necessary to state that it should only be carriedout for the treatment of a lesion that can be seen,not on account of symptoms, however definite theymay appear to be. In the first place, it is the operationthat should be performed when surgical treatment hasbeen decided upon in a case of chronic duodenal ulcer.It is rarely that any other procedure is necessary.The operation of gastro-duodenostomy has failed, inmy hands, to bring about a satisfactory post-operativereduction of acidity and is more often followed bysecondary ulceration. In my opinion duodenectomyhas nothing to recommend it.
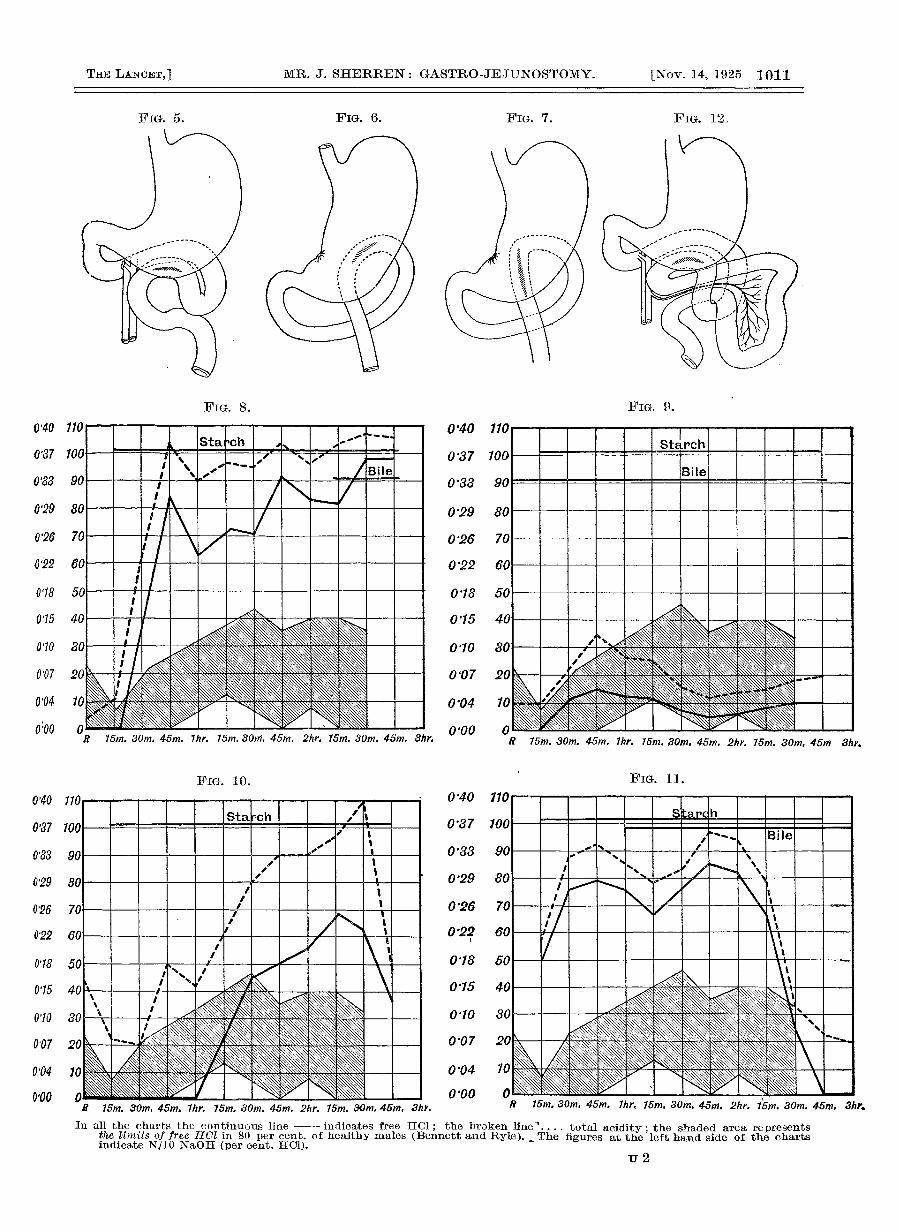
I should like to give examples comparing the pre-and post-operative fractional meals of patients withchronic duodenal ulcer, recently treated by gastro-jejunostomy and by gastro-duodenostomy. Figs. 8and 9 are from a male patient operated on by me forchronic duodenal ulcer, after having had symptoms forten years. With such a result one can certainly saythat further trouble is extremely unlikely. Figs. 10and 11 are from a female patient, operated on after15 years history. There was a scarred ulcer constrictingthe first part of the duodenum, which was mobile anddilated. For this reason gastro-duodenostomy wasfeasible and was carried out with a wide opening. Inspite of regurgitation, as shown by the presence ofbile and a rapid emptying demonstrated by a bariummeal, the chart shows great post-operative acidity.I shall be surprised if this patient does not developfurther symptoms.
Gastro-jejunostomy is my operation of choice inchronic gastric ulcer when the ulcer is " free," withoutsuspicion of malignancy, and the anastomosis can bemade to its cardiac side. The statements in thepaper to which I have just referred 16 are opposed tomy experience of the results when the operation iscarried out on the lines I have described. Thefollowing sentence occurs in it: " have records ofpatients who got no benefit from it, and when the’abdomen was opened after several years the ulcer stillpersisted." I also have records of this description,but they apply only to those patients in whom theoperation was incorrectly performed, or for whom thistreatment was unsuitable.The following is an example :-L. C., a male, aged 45, was admitted to the London
Hospital under my care in December, 1924. He had hadgastro-jejunostomy performed at another hospital nineyears previously and had not been relieved in spite of thefact that his test-meal revealed an absence of free HCI
and a total acidity of 16. Barium meal showed some delayin emptying, most of the meal being present at the end ofan hour. At operation I found a large ulcer " free " onthe lesser curvature. The gastro-jejunostomy was small,posterior, and near the pylorus, with no trace of secondaryulceration. After excising it I did my usual operation to thecardiac side of the ulcer. He did well, but died of anothercause nearly three months later and I was fortunate inbeing able to obtain an account of the post-mortem. Thegastric ulcer had absolutely healed and the anastomosis wasperfect.
This is a very striking instance showing that it isuseless to carry out the anastomosis to the pyloricside of the ulcer and illustrates a point I shall dealwith later, that the post-operative gastric acidityhas no bearing on the healing of the original ulcer. IThis patient obtained no relief after a gastro-
jejunostomy performed to the pyloric side of theulcer, even though it had brought about achlorhydria,but secured immediate relief and cure of the ulcerwhen it was done to its cardiac side.
Gastro-jejunostomy should never be advised inacute ulcers with hsematemesis ; it has no influenceon this condition. In simple organic stricture ofthe pylorus, whether due to the cicatrisation of aduodenal ulcer or to any of the more unusual causes,it is the operation of choice. In hour-glass stomachin which the causative ulceration has healed it isof the greatest service, and if pyloric obstruction ispresent as well may necessitate a double operation.The results of double gastro-jejunostomy are excellent.The first, done 15 years ago, is, and has remainedquite well, and all others have been equally satis-factory. That it is not often called for the followingfigures will show. I have operated on 135 cases ofhour-glass stomach due to simple ulceration and inonly seven has it been necessary. In the majoritya penetrating adherent chronic gastric ulcer waspresent, indicating the need for partial gastrectomy.It is valuable in carcinoma which is irremovable andcauses pyloric obstruction, but not otherwise.
RESTJI,T OF THE OPERATION.The mode of action and the result of the operation
are closely related. The symptoms in chronic gastricand duodenal ulcer are due to spasm or irregularmuscular action of the pylorus and pyloric portionof the stomach in duodenal ulcer, and of the bodyof the stomach in gastric ulcer and to the increasedtension produced thereby. Who that has seen theprogress of a case after gastro-jejunostomy for ulcerin those perhaps somewhat unusual instances wherethe pain is so severe as to necessitate the use of opium,and has noted the immediate post-operative reliefobtained, will doubt this, and that the relief is dueto the mechanical and not to the physiological or,as I prefer to call it, chemical effect of the operation.All who have watched on the screen the marked spasmin chronic gastric ulcer, and in addition their regularperistalsis in chronic duodenal ulcer, will realise thatthis is a factor which prevents healing. This spasmresults in the meal passing at first chiefly by the newopening even in those cases, and they are in themajority, in which no organic stenosis is present. Theeffect of the operation is to cause more rapid emptyingof the stomach and immediately to relieve gastrictension. Its action on the ulcer itself, therefore, ismechanical-that is, it gives the ulcer rest. I have yetto see failure of healing in suitable cases, and I havepublished many at various times in which I have hadan opportunity of examining the stomach andduodenum post mortem or at second operation atlong periods after the primary procedure. If healingwere due solelv to an alteration in the chemistry ofthe stomach chronic gastric ulcers would heal, eventhough the anastomosis were placed on their pyloricside and duodenal ulcers would not heal unless therewas satisfactory change in gastric acidity. I havehad to reoperate on several cases, the primary opera-tion having been carried out by others, one of whichI have just quoted, in which in spite of achlorhydriathe lesser curvature ulcer was unhealed, the anasto-mosis being made to its pyloric side, and Ryle," inhis Goulstonian lectures, has published an example.It is my experience that chronic duodenal ulcers healas the result of gastro-jejunostomy, even in those casesin which it does not bring about any profound changein gastric acidity. The operation brings about healingof the ulcer, whether gastric or duodenal, when carriedout on correct indications.On the other hand, from the patient’s point of view,
the permanent relief of symptoms, it is essential thatgastric acidity be markedly diminished even to theabolition of free HCI to prevent fresh ulcerationeither in the jejunum or at the anastomosis shouldany infective focus be overlooked, or the mucousmembrane fail to heal by first intention. But everypatient in whom operation fails to reduce aciditydoes not develop further symptoms ; it is only when
1011
FiG. 6. FiG. 7. FIG. 12.
FIG. 8. FIG. 9.
In all the charts the continuous line - indicates free HC1; the broken line’’ total acidity; the shaded area representsthe limits of free H01 in 80 per cent. of healthy males (Bennett and Ryle). - The figures at the left hand side of the chartsindicate N/IO NaOH (per cent. HCl).
u2
1012
some other cause is present such as I have jnst Imentioned.
Failure to reduce gastric acidity has no bearingwhatever on the healing of the original ulcer; theoperation is "mechanical" so far as this isconcerned, " chemical " in its prevention of furtherdisease. I am convinced that post-operative acidityis the predisposing cause of post-operative ulcerationand that its great reduction is to a certain extentwithin our control; a large opening far removed fromthe pylorus brings about a greater lowering than asimilar or smaller one close to the pylorus. I gavemy reasons for this belief in my Hunterian lecture.I8Recently Walton 1-1 has advocated a similar positionfor the anastomosis.What are the causes of the post-operative lowering
of acidity which almost invariably takes place aftergastro-jejunostomy carried out for the treatment ofchronic gastric ulcer, usually to as large a degree asafter partial gastrectomy, and fails in some cases ofchronic duodenal ulcer ? I am certain that refluxof duodenal contents into the stomach is the principalfactor. It has been satisfactorily proved that thepancreatic juice is the neutralising agent. In mostcases of chronic gastric ulcer the anastomosis mustfrom the necessities of the case be made well to thecardiac end of the stomach. But there is another factorbesides that of the position of the stoma. The opera-tion may be carried out on exactly similar lines intwo patients of the same age and sex on the same dayfor the same condition with similar pre-operative meals.In one the post-operative meal reveals an absence offree HC1 and a total acidity of 20, in the other oneof 0.1 and 50. I shall have much more to say on thissubject later, but I am convinced that it is in someway bound up with the use of the pylorus. It ispossible that the production of secretin in the duodenumactivating the pancreatic secretion may play a part,but I am inclined to the opinion that for the mostefficient reduction neutralisation via the pylorus aswell as the stoma is required. In support of the viewthat want of sufficient neutralisation is the cause ofpost-operative hyperacidity I will quote Bolton’s 20words on the subject :-"The essential cause of hyperacidity of the gastric
contents is a deficiency in the neutralising process whichregulates the acidity of the contents." And again, " Theimportant point to note is that the condition hyperchlor-hydria is the result of neuromuscular irritability of thestomach in which the pylorus plays chief part."
In the section dealing with gastric acidity followinggastro-enterostomy, he writes as follows :-
"Following gastro-enterostomy the secretion’of gastricjuice remains unchanged, any alteration in the aciditycurves being due to neutralisation by regurgitation ofintestinal contents through the stoma."
H. J. Paterson,21 who has been an ardent supporterof gastro-jejunostomy and whose writings on thesubject are classical, holds the reduction of acidity tobe due partly to regurgitation through the stoma andpartly to a diminution in the total chlorides secreted,and considers the action of the operation physiological,the result of this reduction of acidity, which he rightlydeems necessary for the certain cure of the patient.But the ulcer heals after the operation correctly per-formed no matter what the gastric acidity, so thatfrom the point of view of healing of the original lesionits action is not physiological.
Although failure to reduce post-operative acidityhas no bearing on the healing of the original ulcer, itis of the utmost importance in the future welfare ofthe patient. I have on several occasions drawn atten-tion to this, the last time in these words when speakingof secondary ulceration :—
" If the operation permanently abolishes free HC1 in thegastric juice, chronic ulceration does not occur. I drewattention to this in my Hunterian lecture, and, for reasonsthere given, consider it an important cause. I think thereis no doubt that a large opening removed from the pylorusproduces the greatest lowering of gastric acidity, and inter-ference with the pylorus by exclusion or the presence ofadhesions is an important factor in keeping up the post-operative acidity." 22
I have revised the figures there given up to the endof June, 1925. Out of 195 personal cases of chronicga,stric ulcer treated by gastro-jejunostomy in whompre- and post-operative test-meals were given, in notless than 157 free I3Cl was abolished and total aciditymarkedly reduced, in all to below 30. In 26 it wasgreatly diminished, and in only 12 was it not reducedbelow normal. Of the duodenal ulcers, similarlybrought up to date, 340 in number, in 206 there wasabsence of free HC1 in the post-operative test-mealwith a low total acidity, in 79 there was a satisfactoryreduction, and in 55 there was little or no reduction.I wish to repeat again what I consider of the utmostimportance-no case of secondary ulceration arose
among those in whom the post-operative acidity wasgreatly reduced, and that the patients in whom furthersymptoms developed were from the group in whichthere was little or no reduction. It has been myexperience that in many of the cases in which there isinsufficient lowering of gastric acidity there is inter-ference with the free action of the pylorus, and inthese X ray examination shows that the barium mealis leaving chiefly or only by the stoma.
I am convinced that pyloric occlusion at the timeof operation is a fertile cause of failure to reducegastric acidity. Much has been written on this subjectwhich it is difficult to reconcile. Donald Hunter 23states that it had no effect on post-operative acidity,but on looking at Table VIII. I found these figures :19 cases without pyloric occlusion, free HCI abolishedin 10, remained high in 5, became higher in 4 ; 21 caseswith pyloric occlusion, in only 8 was free HCIabolished, it remained high in 8, and became higherin 5. This is surely evidence that it affects unfavour-ably the post-operative reduction of gastric acidity.Apperley 24 studied 27 cases by post-operative frac-tional test-meals and was convinced that pyloricocclusion had no effect on gastric acidity, but thatfailure in reduction was due to a faulty stoma. I havealready mentioned that a failure in satisfactoryreduction may be due to the anastomosis being madenear the pylorus ; a small inefficient stoma will alsobe a cause, but neither is the sole explanation. In themajority of my own cases there has been no differencein the size or position of the new opening, and in veryfew did I have to make a note that for some reason theopening had to be smaller than I like and its positionunusual. Investigation by X ray after a bariummeal in those in whom there was little or no
reduction showed that the stomach emptied as
rapidly by the stoma as is usual after gastro-jejunostomy. I could discover no difference in thisrespect between those in whom free HC1 was abolishedand those with a high post-operative acidity.Uuy 5 examined by the fractional method 26 cases
after gastro-jejunostomy. They were distributed asfollows : gastric ulcer, 3 ; pyloric ulcer, 9 ; duodenalulcer, 14. He argues that the reduction in gastricacidity is more marked in gastric ulcer because thepre-operative acidity is less and applies the same topyloric ulcer, a misleading term that I should like tosee abolished. Speaking of duodenal ulcer he states :-
" Since duodenal ulcers are accompanied by such markedhypersecretion, a much smaller reduction in acidity aftergastro-enterostomy is to be expected. It has been foundinvariably that a considerable degree of acidity exists afteroperation, and a study of the acid curves shows that areduction to about half of the pre-operative acidity is themaximum that has been obtained. That is, the gastricsecretion is now brought within the limits of normal acidity."
This is totally opposed to my experience of thecondition. The figures I have quoted entirely dis-proved this, at least for my own cases. He traversesthe view that pyloric exclusion has any bearing on thepost-operative result in these words :-
" The view expressed by Sherren that duodenal exclusionis the cause of post-operative hyperacidity is not borne out,as it has been demonstrated that a high acid level afteroperation is but the natural result of an excessive pre-operative hypersecretion and is not affected by variationsin operative procedure apart from. the provision of a stoma,"but does not give the evidence upon which he bases.the statement. Bonar,26 in a study of gastric function.
1013
before and after gastro-jejunostomy, also used thefractional method. In 14 cases of chronic gastric ulcerthere was an absence of free HCI in 80 per cent., and inthe remaining 20 per cent. a marked hypochlorhydria.In 33 cases of duodenal ulcer the fractional meal beforeoperation showed a high acidity in an hour-that is,at the time corresponding with the Ewald meal. Afteroperation he states that marked hyperchlorhydria wasstill present and that it was marked in three-quartersto one hour-that is, at the corresponding interval tothat before operation. This again is not my experi-ence. My results certainly do not bear out his state-ment that, " In the case of ulcers with high aciditiesgastro-jejunostomy does not cause to any extent areduction of the acidity." I have notes of a consider-able number of cases examined by the fractionalmethod, though small when compared with thosedone by the single examination, the results at thehour both before and after operation correspond fairlywell with those obtained by the single meal. I am stillof the opinion that for diagnostic purposes the singletest-meal before and after operation gives all theinformation necessary; certainly in hospital work ithas given me results which correspond more closely tothe clinical and operative findings than the fractional.Thus in the case illustrated by Fig. 10, in the frac-tional meal it will be seen that at the end of an hourthere was no free HC1 and a total acidity of 43, whereasthe Ewald meal that I had given, as this was sounconvincing, showed free HCI 0’23 and total acidity72, a test-meal corresponding with the condition foundat operation. In a long experience of Ewald test-meals in chronic duodenal ulcer I have never hada result of this sort, but have had similar verypuzzling discrepancies with the fractional meal. Ihave abandoned examination by this method exceptin an endeavour to throw light on exceptionallydifficult cases. My medical colleague, Dr. RobertHutchison, agrees that the " old ’ single ’ or Ewaldtest-meal is to be preferred to the more modern’ fractional ’ type. 11 2 7 The investigations were alldone in the London Hospital clinical laboratoryunder the supervision of Dr. P. N. Panton, withoutwhose help these conclusions would have beenimpossible.
Ryle,28 in his admirable Goulstonian lectures, dealsin the third with gastro-jejunostomy and its sequel.Speaking of the post-operative reduction of gastricacidity he says that a case with deficient or lowmotility is more likely to respond to gastro-jejunostomythan one with increased motility ; or in terms of thetest-meal, a case with a steadily climbing curve ismore likely to give a good result than one with ahigh abrupt peak of acidity and rapid evacuation.In my experience there is certainly no direct connexionbetween the time of emptying before and after gastro-jejunostomy and the acidity. He quotes me as sayingwe have yet to learn what is the cause of the failure toreduce post-operative acidity, but did not give myviews on the subject that it is due to insufficient use ofthe pylorus and that for the most effective lowering ofacidity it is essential that the pylorus be used as wellas the new opening.
The results of the operation when done for chronicduodenal ulcer and picked cases of chronic gastriculcer have been excellent. Failure to cure the patientaccurs, apart from gross mechanical causes of which Ishall speak later, or from overlooking lesions of otherabdominal organs, only in that group in which thereis insufficient reduction of post-operative acidity.Realisation of this is essential and improvement in ourresults will only come when our work is checked by thisknowledge. Devine 29 states that " 65-70 per cent. ofgastro-jejunostomies for all types of duodenal ulcerwere successful. This seems to depend chiefly onthe ability of the operation to diminish greatly orabolish acidity." He adds, " Gastro-jejunostomy musttherefore remain the basis of average gastric surgery,"and considers that it should be, but is not, an idealprocedure. He mentions that the unsuccessful gastro-jejunostomies fell into a group in which there was anincrease or little modification of acidity after operation,
and that this was due to failure of alkaline regurgita-tion.
Success with this operation will depend on thecare with which it is carried out along thelines I have suggested. Those of us who haveobtained good results have been criticised. Pannett,30for example, speaking of those who claim90 per cent. successes, says there is "obviouslysome radical difference in the manner of evaluation."I should rather say in the exact manner in which theoperation is carried out. In a further paper 31 hegives the names of those with cure rates in the regionof 90 per cent. Speaking of my own figures I havefollowed these cases up from the very first and havecounted as " quite well " only those patients whohave been perfectly well throughout; if they haveany digestive complaints they may be included amongthose improved, but not among the 90 per cent. Allpatients are seen at 3, 6, and 12 months after operationand heard from yearly till after the third year. I shallgive an example later. I have again brought theearlier cases up to date and confirm what I have saidbefore, that the longer the cases are traced the betterthe result, and most of those who had minor troublesin the first year lost them later and had completelyforgotten eight or ten years after that -they hadoccurred. I can speak for the thoroughness of thefollow-through method of my colleague Mr. Walton,32who has recently described it. The Mayo Clinic needsno defence from me. The results published in thepaper from which my figures are taken 33 are betterthan those of four years previously, owing, I believe,to increased skill in carrying out the operation due tofollowing up all the patients carefully and improvingtechnique ; several of the patients then not well arenow well. Balfour’s 34 figures in chronic duodenalulcer are an eloquent testimony, 88 per cent. quitewell among 1000 patients. Metraux 35 in the study ofcases in Roux’s clinic found that in 90 per cent. of thecases of chronic gastric or duodenal ulcer treated bygastro-jejunostomy alone a good result was obtained.Peck 36 wrote that simple gastro-jejunostomy properlyperformed is curative and adequate in the greatmajority of chronic duodenal ulcers, and that from80 to 90 per cent. are completely relieved of theirsymptoms and remain well as they are followed fromyear to year. We cannot dismiss these figures as dueto insufficient care in estimating results as Pannetthas done, but rather look to the nature of theoperation that others are doing and see if this willnot account for their less satisfactory results. If thefigures I have quoted from various writers of the failureto reduce gastric acidity after gastro-jejunostomy forduodenal ulcer are an index there is certainly a reasonfor its failure in many cases.To sum up, gastro-jejunostomy carried out on
modern lines will bring about the healing of alluncomplicated cases of simple chronic gastric andduodenal ulcer. Cases in which the floor of theulcer is formed by pancreas or liver, or in which thereis any suspicion that it is malignant, must be treatedby partial gastrectomy. Cure of the patient-that is,complete and permanent abolition of symptoms-willbe brought about in at least 90 per cent. of the cases,among the eight or nine not cured seven will be minorcomplaints, and not more than 2 per cent. secondaryulceration. When such a result can be brought aboutat a risk of less than 1 per cent. it is obvious that thisoperation has a permanent place in surgery. I havefound no difference in the cure rate of those withorganic pyloric obstruction, chronic duodenal ulcerwithout obstruction, or free lesser curve ulcers. I haveobtained equally good results when I have beencompelled to use my anterior operation. The firstcase was in December, 1904, and in this instance Iwas able to prove that the ulcer was healed at post-mortem 18 months later after accidental death. I havetraced a woman operated on in January, 1908, now74 years of age, without abdominal trouble. A malepatient of 39 with a very indurated lesser curve ulceroperated on in July, 1913, remains quite well. I firstcarried it out in the treatment of chronic duodenal
1014
ulcer in a male of 48 on Nov. llth, 1908. He hadan indurated ulcer involving both surfaces of theduodenum ; he is now, and has remained throughoutthe 17 years, quite well.
COMPLICATIONS.We now come to the principal complications. They
may be divided into : (1) Failure to produce healingof the original ulcer or its recurrence ; (2) secondaryulceration ; (3) intestinal obstruction includingregurgitant vomiting ; (4) late development ofcarcinoma.
Failure to Secure Healing or Recurrence.(1) As I have many times stated I have never found
a duodenal or gastric ulcer unhealed at a secondoperation or post-mortem when an efficient gastro-jejunostomy had been carried out in a suitable case,and my experience now extends to over 100. Toprevent anyone thinking this is evading the issueI will state if the ulcer was free and the anastomosiscarried out on the lines I have laid down. Wherethere has been chronic perforation with erosion ofthe pancreas or liver, a small part of the ulcer some-times remained unhealed. They are cases in whichI recognise that gastro-jejunostomy is not the idealprocedure, but even in many of these it has promotedhealing. I was astonished recently on going over myold operation notes to find in how many, in whichI had recorded that partial gastrectomy was theideal operation but could not justifiably be done,the patient had remained absolutely free from all
symptoms when traced for as long as 10 to 20 years.The first case of this nature I operated on in which this
note appears was a little over 20 years ago-a man of 33with a seven years’ history, which included two attacks ofhaematemesis. At the operation on Oct. 4th, 1905, I founda large saddle-shaped ulcer of the lesser curvature adherentto the pancreas and carried out posterior gastro-jejunostomyto its cardiac side. I traced him in the way in which I keepin touch with all the patients ; I saw him three and sixmonths after operation and heard in 1907, 1908, 1910, 1911,1913 1914, 1916, 1919, 1922, and saw him two months ago.He has never had any digestive complaint.I cannot conceive of a better testimony to the valueof the operation.
I have on several occasions found a chronic gastriculcer unhealed at a second operation in cases in whichthe gastro-jejunostomy was done to its pyloric side;even if excision is added to this procedure and thegastro-jejunostomy done to the pyloric side of theexcision wound, fresh ulceration is usual in thescar. Recurrence of the ulcer or failure in healingmay occur in cases in which the gastro-jejunostomyopening has closed or become much contracted as theresult of secondary ulceration. In the oft-quotedcase recorded by Corner 3’ of the fatal perforation of achronic duodenal ulcer in a patient upon whom SirBerkeley Moynihan had performed a posterior gastro-jejunostomy three years previously there was con-traction of the opening. Corner stated : " There was nojejunal ulcer present; indeed, the gastro-enterostomyopening was very contracted." It is my experiencethat gastro-jejunostomy openings do not contract toany extent except as the result of marginal ulceration,and as, from the history, the patient had not beenreally free from symptoms this was undoubtedly thecase. I would remark that the original operation wasdone in the early days in which marginal ulcerationdue to unsuitable sutures was by no means unusual.I can give a recent example which illustrates the twopoints, failure of healing or recurrence of the ulcerand closure of the gastro-jejunostomy opening.A man at the age of 42 was operated on in 1915 by a
surgeon, since retired, for a chronic duodenal ulcer with ahistory of 20 years’ standing. Silk was used for the anas-tomosis. He remained quite well for 12 months and thenbegan to get pain, which differed from that before operationby being in the lower abdomen. The attacks of pain were atfirst infrequent, but the intervals became shorter and theattacks longer, and when I saw him in February, 1925, hehad had severe abdominal pain, which would wake him atnight and for two or three years this had been in the upper I
abdomen. lie was a thin man with an obviously dilatedstomach. X ray examination showed that it still containedmuch of the barium meal at the end of seven hours and thatlittle, if any, had passed by the stoma. At operation I founda large anterior duodenal ulcer. The gastro-jejunostomyopening was so small that it certainly measured no more thani inch in diameter. My note says : " I have never seenan opening so contracted, it would have been possible tosay that it had completely closed." I carried out posteriorgastro-jejunostomy and he lost his symptoms at once.
In speaking of the development of fresh ulceration’I have operated for chronic gastric ulcer ten yearsafter gastro-jejunostomy for chronic duodenal ulcerand am able to show the specimen which is now in ourmuseum.
In February, 1913, T operated on a woman of 43, who for16 years had been having periods of pain after food with oneattack of profuse haematemesis and melsena a year after theonset of symptoms. Her test-meal was 0-25 and 100. I founda large ulcer on the anterior surface of the first part ofduodenum and did a gastro-jejunostomy nearer to thepylorus than I do now, and removed her appendix. Unfor--tunately no post-operative test-meal was given ; at that timeI did not have it carried out as a routine. She remained’well for two years and then got an attack for which shekept her bed two weeks, a similar one in 1919, and againin 1923. Her barium meal report was: Penetrating ulcerlesser curvature towards cardiac end. Stoma normal..Duodenum functioning normally. Test-meal 0-10 and 35.At operation on June 8th, 1923, I found the duodenal ulcerhealed and the gastro-jejunostomy opening perfect. Well to.its cardiac side was an ulcer the size of a shilling, which hadperforated and was adherent to the pancreas. I did apartial gastrectomy and she remains quite well. On examin-ing the specimen the stoma was as large as the day I madeit ten years previously.
In this case the ulcer was either overlooked by meat the first operation or formed later on the cardiacside of the anastomosis. It illustrates once again theuselessness of a stoma to the pyloric side of an ulcer.
Secondary Ulceration.(2) Secondary ulcers are those which develop in
the region of the anastomosis either true jejunal orgastro-jejunal. I still believe, in spite of Walton’s 38-experience,that these are separate conditions, althoughwe cannot differentiate them by their symptoms ortheir causation. Both are due to the action of gastricjuice on tissue whose vitality is lowered. This maybe from haemorrhage, infection, or by the failure ofunion of mucous membrane exposing the underlyingtissue. They occur in those cases and those only inwhich operation fails efficiently to reduce gastricacidity. I should like to repeat again that I have-never known the development of secondary ulcerationin any patient in whom operation has abolished orvery greatly reduced the amount of free HCI in thegastric contents as noted in an Ewald meal. I shouldagain like to emphasise its rarity in women and afteroperation for gastric ulcer ; this I attribute to theinfrequency of duodenal ulcer in this sex and afterchronic gastric ulcer to the greater proportion of casesin which free acid is abolished and the total acidity ismuch lowered. In the unusual instances of chronicgastric ulcer with high acidity in which gastro-jejunostomy fails to reduce it there is a liability similarto that in chronic duodenal ulcer. The following isan example and illustrates several important points.On July 10th, 1917, I operated on a male, aged 40, with
the following history. He had five attacks of indigestion,pain late after food, not relieved by it but by occasionalvomiting. In his last attack the pain waked him at night.In an attack a year previously he had been in hospital withhaematemesis ; test-meal 0’2 and 78. My own notes are asfollows : Gall-bladder normal. Two very indurated ulcerson the lesser curvature, close to the pylorus. There were nooutlying nodules and nothing definitely to suggest malignantdisease, but had his condition been better I should havedone partial gastrectomy. The jejunum was adherent to theunder surface of the transverse mesocolon. I made myanastomosis nearer the pylorus than usual and found aconsiderable loop of adherent gut had been left between itand the duodeno-jejunal flexure. Appendix not removed.His post-operative test-meal-0-12 and 56-was unsatis-factory. I saw him on Sept. 3rd, 1917, and Nov. 4th, 1917,

1015
and heard on August 8th, 1918, and Dec. 30th, 1922, thathe was in perfect health. He then began to get attacks ofpain two hours after food, relieved by vomiting recurringevery four to six months. He was admitted to St. Mary’sHospital, and I am indebted to Prof. Pannett for thesenotes : X ray examination showed delay in the pyloricantrum, but the stoma functioning. Unfortunately no test-meal was given. At operation a gastro-jejunal ulcer wasfound at the left lower margin of the stoma. The gastriculcers had completely healed.
This is one of the last cases in which thread wasused for the outer layer, and I had to resort to it
owing to a shortage of Luken gut. The ulcer wasin the usual situation for a gastro-jejunal-that is, atone of the extremities-and I attribute it to workingout of the knot of the suture leaving an ulcer whichcould not heal on account of the high gastric acidity.It is extremely uncommon for symptoms to recur aftera lapse of over two years, even after the use of silkor thread for the outer layer of sutures and this isonly the second case I have seen. It is an apparentexception to the " rule " that patients free fromsymptoms for two years do not develop secondaryulceration, but it is obvious that this could not applyto ulcer directly due to unabsorbable suture materialin the outer layer as it may take years to work itsway out, and if this occurs in a patient with normal orincreased gastric acidity the formation of a chroniculcer is probable.
There are thus, I believe, two factors. One is thefailure to reduce gastric acidity. If this remains highthen an area of lowered resistance, the result ofundiscovered infection in the mouth or abdomen, orof haemorrhage from puncture of a vessel during sutureor bruising from the use of a clamp, may bring aboutulceration in the jejunum. If, either from faultysuturing or unabsorbable material being used, themucous membrane of the anastomosis does not healby first intention, or, if healed, a suture or its knotworks its way out, then gastro-jejunal ulcer may occur.The last true jejunal ulcer upon which I operated waslast December. The history is so characteristic ofthe condition that I must quote it.
In November, 1920, I operated on a male of 45 for duodenalulcer with a typical history extending over ten years. Hisbarium meal showed the ulcer and his test-meal was 0-23 and90. At operation : Gall-bladder normal, large ulcer anteriorsurface first part. Posterior gastro-jejunostomy carried outwithout difficulty and a fibrotic appendix was removed. Hispost-operative meal was 0-2 and 81. He remained well forfive months only and then began to get pain late after foodin the epigastrium and left iliac fossa. I took him in fortreatment a year after operation with relief for a time ; histest-meal was then 0-13 and 62. The attacks became worse,so that I operated last December ; his test-meal was 0- 19 and62. The duodenal ulcer had healed ; there was a chroniculcer in the jejunum immediately distal to the anastomosisadherent to the colon. I excised it, closed the opening in thestomach and jejunum, and carried out pyloroplasty, withthe result that his post-operative meal 14 days later was0 and 33 and the stomach was empty in 25 minutes. Heremains well.The case I quoted last year 39 as an example of jejunal
ulcer after gastro-jejunostomy was treated by partialgastrectomy on June 21st, 1921. He remained well fornearly two years and then began to get pain two hours afterfood. I admitted him again on Dec. 29th, 1923, and foundthat his gastric acidity was 0-09 and 40. He lost his symptomswhile in bed, but ten months later developed diarrhcea andfaecal vomiting, and at operation on Nov. 21st, 1924, I founda jejuno-colic fistula. In this instance I had been unable torestore the lumen of the jejunum so as to carry out the usualpartial gastrectomy, as I endeavour to do in cases of thistype, and had to do a T-shaped anastomosis of jejunum tojejunum below the gastro-jejunal one, and this accounts forthe recurrence.
The condition of secondary ulceration in my ownpractice is getting rarer with each series of cases.
With regard to malignancy supervening on a gastro-jejunal ulcer, I have yet no definite case, but I stillconsider it a remote possibility.To sum up, secondary ulcer is the result of failure of
the gastro-jejunostomy to lower gastric acidity. Butthis post-operative excess of acid is not in itselfenough, as we see that the ulcer for which the
operation was performed heals. There must be somelowering of resistance, either a gap in the mucousmembrane from faulty suturing, removal of too muchmucous membrane, working out of unabsorbablesuture, haemorrhage, or infection. Their incidence canbe lessened even if the condition cannot be completelyabolished by careful dealing with all infection andscrupulous attention to all the details of the operation.
There is to my mind no doubt of the necessityfor avoiding pyloric exclusion. A case published byFrankau 40 shows its effect experimentally. I ammuch indebted to him for further notes on the casewhich enabled me to trace the patient to his originalsurgeon and obtained fuller details.
In 1914 a man of 29 was operated on for duodenal ulcer.His test-meal was 0’2 and 76, but no post-operative mealwas given. Symptoms recurred in nine months, and he wasadmitted to St. George’s Hospital after several severe
attacks of hsematemesis and melrena. His test-meal thenwas 0’2 and 82. At operation an unusual condition wasfound, in that there was still a chronic duodenal ulcerpresent, but there were no signs of ulcer at the anastomosisor in the jejunum. The pylorus was clamped and divided.He remained well for 14 months, and then had abdominalpain, diarrhoea, and vomiting. He was reoperated uponand a jejuno-colic fistula was discovered.
The unfavourable result with pyloric exclusion isborne out by the experience of others. Haberer’s 41figures are instructive ; among 265 cases of gastro-jejunostomy there were three cases of jejunal ulcer,but in 71 cases in which pyloric exclusion was addedin the treatment of duodenal ulcer no less than14 developed jejunal ulcers. Kurnme]l 42 had pre-viously pointed out its frequency under these circum-stances. Finsterer,43 who is now an ardent advocateof wide partial gastrectomy in the treatment ofduodenal ulcer, writes that Haberer had 25 per cent.secondary ulcers with pyloric exclusion and posteriorgastro-jejunostomy. Norman Dott 44 demonstratedexperimentally that chronic peptic jejunal ulcer isthe constant sequel of gastro-jejunostomy with pyloricexclusion in dogs. Von der Hiltter 45 found in hisexperiments on dogs that jejunal ulcer did not developin those cases in which the pylorus was patent, butthat it was produced when pyloric exclusion by vonEiselsberg’s method was carried out. Gussio,46 froma study of cases of jejunal ulcer, came to the conclusionthat its development is favoured by impermeabilityof the pylorus. Enderlen, Freudenberg, and vonRedwitz, 4’ as the result of experimental investigationson dogs, came to the conclusion that pyloric exclusionshould be abandoned.As we know that jejunal ulcers only arise in those
cases in which there is failure to reduce post-operativeacidity it seems to me obvious that interference withthe pylorus is one of the causes of this. In 1921" Istated that most of my cases of jejunal ulcer occurredin those patients operated on between 1911 and 1913,when I carried out pyloric exclusion, and my observa-tions since then on cases in which from any causethere was interference with the free function of thepylorus confirms this as there was a failure of post-operative reduction.
Ryle 49 states, " There is a greater liability togastro-jejunal ulcers in young adults and in cases witha short dyspeptic history." As this was not myexperience I have put it to the test so far as possible.I took all the cases of secondary ulcer, whether jejunalor anastomotic, that I have operated on, 44 innumber ; the youngest was 25 at the time of theoriginal operation, the oldest 55, and the average agewas 41-7. I then took the same number of consecutivecases of chronic duodenal ulcer, operated on overtwo years ago ; the youngest was 17, the oldest 62,average age 40-4. I then took duration of symptomsbefore operation in the cases that developed secondary
ulcer ; the average was ten years, in the consecutivecases the average was 9-5. The number of cases issmall, but there is an astonishing correspondence inthe two series sufficient, I think, to controvert Ryle’sstatement. Such varying estimates have been givenof the frequency of secondary ulceration that it is
1016
difficult to discuss. In a recent paper Lewisohn 60
states that in a series of 68 cases re-examined 4-9 years after gastro-jejunostomy, 34 per cent. suffered from Igastro-jejunal ulceration. As in a following paragraphhe states, " Gastro-enterostomy does not reduce thehyperacidity even after many years," we seem tohave the reason for this high percentage. Myexperience coincides with that of the Mayo Clinic thatit is met with in less than 2 per cent. of the cases.Although in large series done in the one clinic thepercentage is between 1 and 2 per cent., I still believethat even this can be lowered and should not liketo think, as suggested by Walton, 51 " that the failureof the acid to fall in these gastro-jejunal ulcer casesmay be due to an anatomical variation, the acid-producing cells in a certain number of duodenalulcer cases (about 2 per cent.) being more widelydistributed over the gastric surface and thus beingless affected by the gastro-enterostomy." To me thisis tantamount to saying we can do no more.
It must be remembered that excision of the ulcerwith pyloroplasty or even doudenectomy does notprotect the patient from secondary ulceration, and Isuspect that its frequency is greater after both these,as pyloroplasty does not usually bring about so greata reduction of gastric acidity, and duodenectomy, likeresection of gastric ulcer, will probably be given upon account of recurrence. Mann and Kawamura 52.found that after complete duodenectomy in dogsjejunal ulcer developed in two cases out of ten leadingto perforation at 515 days after operation in one, andin the other it was found post mortem 383 days after.None of the arguments from the secondary ulcer
standpoint that have been brought against gastro-jejunostomy seem to me to be valid. It is the mostserious drawback, but it is one that we are getting tounderstand as we realise that what is necessary is notmerely a mechanical opening, but control of acidity.In many of the cases of failure to cure the patientother lesions in the abdomen have been overlooked,and I have had to remove the gall-bladder and appendixin these patients on many occasions after the failure ofgastro-jejunostomy to cure all their abdominal ills.This should, of course, always be done if practicableat the time of the original operation and as part of thetreatment in removing all possible sources of infection.
Intestinal Obstruction and Regurgitant Vomiting.(3) The bugbear of the early operations, that of
regurgitant vomiting, has almost disappeared. It isalways due to obstruction. The gross variety whichbegan immediately and continued till death or secondoperation has disappeared in modern practice. If itoccurs now it is from the seventh to the tenth day,the obstruction being the result of the contraction ofadhesions, due in most instances, I think, to organisa-tion of blood-clot, causing change in and around theopening in the transverse mesocolon and is alwaysmechanical. It needs one’s ingenuity to circumventthe fat or contracted mesocolon and care to control allpoints of oozing, but I mentioned this in the earlierpart of my lecture. But even this is now uncommon,and if it occurs usually yields readily to lavage. Theminor cases of occasional bilious vomiting are theresult of slight obstruction from rotation of the
jejunum.There are rare and late causes of intestinal obstruc-
tion that have been published from time to time,the commonest being that in which the jejunum passesfrom right to left behind the gastro-jejunostomy, thefirst published by Barker 53 in 1904 occurred twoyears after the operation. It is well seen in thedrawings of the last case published 5-1 (Fig. 12) and inanother by Bryan. 55 5 They all seem similar in thatpractically the whole of the small intestine passesthrough. It is a complication unlikely to occur afterthe posterior vertical operation ; in both theanastomosis was horizontal. Hernise through theopening in the transverse mesocolon occurred untilthis was obliterated by suture. This was recognisedas early as 1902 by Moynihan. Retrograde intus-susception has been recorded. The late Hamilton
Drummond 56 published a case of retrograde intus-susception following gastro-jejunostomy and was ableto collect and review 13 others. These, however, areall extremely rare conditions and do not detract fromthe value of the operation.
Late Development of Carcinoma.(4) We now turn to the possibility of the develop-
ment of carcinoma in the scar of an ulcer at a timeremote from the gastro-jejunostomy. Were this afrequent occurrence it would, of course, be a strongargument for carrying out partial gastrectomy in everycase of chronic gastric ulcer. I would say at once thatI have never met with this complication followinggastro-jejunostomy for a duodenal ulcer, but in onefurther patient to the one quoted in my Hunterianlecture carcinoma of the stomach developed.
This was a man of 35 upon whom I operated in July, 1916,after a two years’ typical history of duodenal ulcer. Atoperation he had a large ulcer of the anterior surface of thefirst part of the duodenum. The stomach was normal.He remained well for over three years and served in France.At the end of 1920 he began to lose his appetite and sufferedfrom pain and vomiting. He died in February, 1921, andpost-mortem revealed scirrhous carcinoma of the pyloriccanal with the thickest and densest part of the carcinomaon the lesser curvature about 2 cm. from pylorus. Theduodenal ulcer had healed.
When I reviewed the question in my Hunterianlecture in 1920 I had had three cases in which I hadcarried out gastro-jejunostomy for chronic gastriculcer, which died at seven, five, and four years afteroperation with abdominal malignant disease. All wereof the type I now treat by partial gastrectomy. Innone was there a post-mortem examination. Sincethat date no case has occurred, so that I must concludeit is a very rare sequence and one that should notinfluence us in the treatment of the small free ulceron the lesser curvature which heals so readily aftergastro-jejunostomy.We must be careful in accepting the presence of
a malignant mass in the abdomen after a gastro-jejunostomy as evidence of carcinoma of the stomachor duodenum, or the presence of secondary depositselsewhere.
I have recently reoperated upon a female patient whoseduodenal ulcer I treated by gastro-jejunostomy nearly threeyears previously. I found carcinoma of the body of thepancreas with secondaries in the liver and spleen. Theduodenal ulcer had healed and the anastomosis was perfect.Another unusual case was a male patient of 37, who died ofcarcinoma of lung one year after gastro-jejunostomy forchronic duodenal ulcer. We were able to obtain a post-mortem and found a thin scar in the duodenum and a perfectgastro-jejunostomy opening. A somewhat similar case wasa male of 44, upon whom I carried out partial gastrectomyfor a very indurated lesser curve ulcer and a chronic duodenalulcer. Microscopic examination showed both to be simple.He was readmitted 18 months later with discomfort. Hewas found to be suffering from carcinoma of his left lung.All three might have been considered as starting in thestomach but for the result of operation in the first, thepost-mortem in the second, and the microscopic examinationin the third.
I have recently operated upon a case of chronicduodenal ulcer with secondary deposits in the liverfrom a primary focus in the lung. The case is worthquoting briefly :-
R. M., a male aged 52, was admitted under my care inJune, 1925, with a history of almost continuous discomfortafter food for nine weeks with vomiting and loss of weight.He was wasted and a definite mass could be felt in the righthypochondrium. His test-meal was 0-28 and 92 and thebarium meal showed deformity of duodenal cap. OnJuly 7th I operated, found that the mass I had felt was theliver with a deposit of growth to which the duodenum wasadherent. There were several small nodules ; I removed onefor examination and then found on separating the duodenumthat there was a chronic ulcer with a small perforation.I excised it and carried out posterior gastro-jejunostomy.He lost his symptoms and left hospital four weeks later.Microscopic examination of the duodenal ulcer revealed noevidence of malignancy. The deposit from the liver wascarcinoma, and it was suggested that the primary was in thelung. I then had the chest X rayed. The report said:" Dense shadow in left hilum. Neoplasm almost certainly."
1017
I have quoted these cases to show that no reliancecan be placed on records of carcinoma developing onulcer after gastro-jejunostomy unless demonstratedat second operation or post-mortem. Moynihan, 5 7however, has recorded operating for carcinoma of thestomach 13 years after gastro-jejunostomy for a
simple chronic ulcer, the malignant growth beingfound at its site. This must be a very uncommonoccurrence. I can see no reason why carcinoma shoulddevelop in a thin scar such as results when a chroniculcer heals as the result of gastro-jejunostomy, andshould look on this solitary case rather as a coincidence.My experience is that carcinoma develops in such asmall proportion-certainly less than half of 1 percent.-of cases treated by gastro-jejunostomy alonethat we should not let it influence us, and I am sureI am right in saying that were every case of chroniculcer to be treated on suspicion as malignant the risein the immediate death-rate would be far greater thanthe number of those who might after a lapse of yearssuccumb to carcinoma.
I think it is too often forgotten by physician andpatient, and possibly by the surgeon, that gastro-jejunostomy cannot give a new digestive apparatus,but that it can and does. if properly carried out, leadto the healing of the ulcer, prevents its recurrence,and in only a small percentage of cases is it followedby secondary ulceration. But these patients may sufferas other dyspeptics without organic lesions fromdiscomfort after food, and considering this, 90 percent. of cures without any digestive disturbances isremarkable.
In conclusion, I should like to say as my matureopinion that gastro-jejunostomy is still the mostsatisfactory treatment for duodenal ulcer and all casesof free gastric ulcer, that its results equal, if they donot excel, those of any other major surgical operation.
References.1. Wölfer, A.: Cent. für Chir., 1881, No. 45, 705.2. Barker, A. E. : Brit. Med. Jour., 1886, i., 292 and 618.3. Morse, Thos. H. : Ibid., 1886, i., 488.4. Reeves, H. A.: Ibid., 1885, i., 954.5. Doyen : Verhandlungen der Deutschen Gesellsch. für Chir.,
1895, p. 57.6. Quoted Moynihan: Duodenal Ulcer, second edition, 1912,
p. 22.7. von Hacker : Archiv. für klin. Chir., 1885, xxxii., 621.8. Petersen: Beitr. klin. Chir., xxix., 597.9. Rockwitz, C.: Deutsche Zeits. für Chir., 1887, p. 502.
10. Moynihan: Brit. Med. Jour., 1908, i., 1092.11. Pribram, B. O.: Klin. Wochenschrift, 1923, ii., 1542.12. Mayo, W. J. : Surg., Gyn., Obst., August, 1924, p. 241.13. Sherren, James : Trans. Clinical Soc. of London., xl., 156.14. Keene, Reginald: Brit. Jour. Surg., No. 48, xii., 791.15. Pannett, C. A.: Brit. Med. Jour., 1925, i., 489.16. Pannett: Loc. cit.17. Ryle, J. A.: THE LANCET, 1925, i., 758 (Chart 25).18. Sherren, James : Ibid., 1920, i., 691.19. Walton, A. J. : Ibid., 1925, ii., 800.20. Bolton, Chas. : Brit. Med. Jour., 1923, ii., 269.21. Paterson, H. J. : THE LANCET, 1907, ii., 815 ; Proc. Roy.
Soc. Med. (Surg. Sect.), April, 1914, p. 211, and March,1920, p. 141.
22. Sherren, James : THE LANCET, 1924, i., 477.23. Hunter, Donald : Quarterly Journal of Medicine, 1923,
No. 62, xvi., 95.24. Apperley, F. L. : Med. Jour. of Australia, 1924, i., 256.25. Guy, E. F. : Brit. Jour. Surg., January, 1923, p. 403.26. Bonar, T. D. G. : THE LANCET, 1924, ii., 261.27. Hutchison, Robert : Lectures on Dyspepsia, 1925, p. 17.28. Ryle, J. A.: Loc. cit.29. Devine, H. B.: Surg., Gyn., Obst., January, 1925, p. 1.30. Pannett, C. A.: Brit. Med. Jour., 1925, i., 489.31. Pannett: THE LANCET, 1925, i., 538.32. Walton, A. J. : Loc. cit.33. Sherren, James : THE LANCET, 1924, i., 477.34. Balfour, Donald C.: Jour. American Med. Assoc., 1924,
lxxxiii., 603.35. Metraux, A.: Rev. méd. de la Suisse Rom., 1920, xl., 569.36. Peck, Chas. H.: Annals of Surgery, 1924, lxxx., 31.37. Corner, E. M. : THE LANCET, 1913, i., 600.38. Walton, A. J. : Loc. cit.39. Sherren, James : THE LANCET, 1924, i., 477.40. Frankau, Claude : Brit. Med. Jour., 1922, i., 184.41. Haberer, H. : Centr. für Chir., May 28th, 1921, p. 762.42. Kummell : Ibid., March 6th, 1920, p. 223.43. Finsterer, H. : Surg., Gyn., Obst., April, 1923, p. 454.44. Dott, Norman : Brit. Med. Jour., 1924, i., 351.45. Hütter, Von der: Beiträge z. klin. Chir., 1923, cxxx., 20.46. Gussio, S.: Policlin., Rome, 1924, xxxi., 323, 345, 427, 476;
47. Abstract Surg., Gyn., Obst., January, 1925, p. 26.
47. Redwitz, E. V. : Zeits. für die Gesamte ExperimentelleMedizin, Bd. 32, Heft 1-4, S. 41.
(Continued at foot of next column.)
EXPERIMENTAL AND CLINICAL
INVESTIGATION OF MERCUROCHROME.
BY A. T. TODD, M.B. EDIN., M.R.C.P. LOND.,ASSISTANT PHYSICIAN, BRISTOL ROYAL INFIRMARY ; DEMON-
STRATOR OF PATHOLOGY, BRISTOL UNIVERSITY.
THE following account of an investigation ofmercurochrome may be of some interest. The prepara-tion is an antiseptic acting powerfully in weak dilu-tion even in the presence of albumin’3; it penetratesdeeply and, although it contains 24 per cent. ofmercury, it is feebly toxic. By several local surgeons,particularly Mr. F. Walters, this substance was foundto give excellent results in some cases, but in others,apparently identical, its action was disappointing.It was this variability which suggested the investiga-tion. Mercurochrome is stated to be disodium-dibrom-oxy-mercury-fluorescein. It is freely solublein water, but in distilled water, which has a faintacidity, it is rapidly broken down, especially whenexposed to light. In normal saline which is feeblyalkaline it is much more stable and appears to keepindefinitely in the dark. A solution in this solventsix months old was recently tested and no alterationwas noted. Four samples have been examined,one from the stock of the Bristol Royal Infirmary,and three others obtained by Mr. A. Taylor, thedispenser. For brevity it may be said that nodifferences in toxicity or antiseptic activity could bedetermined.
Action of Mercurochrome on Organisms under VaryingConditions.
Its antiseptic power was determined in the followingway. Carefully measured amounts, by pipette, of a 1 percent. solution in normal saline were added to 50 c.cm.
of a standard broth ; after mixing 5 c.cm. were measuredinto sterile tubes, giving ten tubes of a constant dilution.To these tubes were added varying amounts of acid, alkali,emulsion of micro-organism, and normal saline. Theseadditions were made with standard Dreyer pipettes. Theseries was incubated overnight and notes made of increasedturbidity, indicating growth in the conditions present,the next day ; then subculture of a fixed amount was madeto determine survival.The action of four different samples in solutions aged
up to four weeks, dilutions from 1 in 1000 to 1 in 500,000,was tested against nine strains of B. coli, one of S. aureU8,one B. pyocyaneu8, and three streptococci. The followingacids were tested : phosphoric, sulphuric, hydrochloric,nitric, formic, acetic, and lactic ; as, however, no appreciabledifferences were found between them they require no furtherdiscussion. On the alkaline side sodium hydroxide wasused.
As the full tabulation of these tests would requireconsiderable space, verbal condensation must besubstituted.
Effect on S. aureus.-Dilution 1 in 50,000 : growthoccurred in acidities from neutrality to pH 6’8—6’5. Survivaloccurred in this dilution to acidity pH 6-0. Dilution1 in 100,000 : growth to pH 6-0 ; survival to pH 5-0.Dilution 1 in 200,000 : growth to pH 5-6; survival topH 4-7.
It is seen from the above that the actual acidity ofthe solution is of more importance than the concentra-tion of the antiseptic. At acidities near to the neutralpoint the antiseptic is so little powerful that theorganism can grow in its presence ; a relatively
48. Sherren, James : Lectures on the Surgery of the Stomachand Duodenum, p. 54.
49. Ryle, J. A.: Loc. cit.50. Lewisohn, R. : Surg., Gyn., Obst., January, 1925, p. 70.51. Walton, A. J. : Loc. cit.52. Mann and Kawamura: Annals of Surgery, February, 1922,
p. 208.53. Barker, A. E. : THE LANCET, 1904, ii., 1277.54. Keene, Reginald : Brit. Jour. Surg., April, 1925, p. 791.55. Bryan, R. C.: Surg., Gyn., Obst., January, 1920, p. 82.56. Drummond, Hamilton : Brit. Jour. Surg., 1923, No. 41,
p. 79.57. Moynihan: Brit. Med. Jour., 1919, ii., 33.





























