Embed Size (px)
Citation preview

Bowels Behaving Badly
BAHSHE Conference
05-07-2005

Functional Bowel Disorders
• Classification and Diagnostic Criteria
• Epidemiology
• Pathophysiology
• Role of psychosocial factors.
• Diagnosis
• Treatment recommendations
• When or if to refer.

Definitions
• No objective biological markers exist.
• Spectrum of FGD defined by symptoms in the absence of structural pathology.
• Manning Criteria
• Rome I and II

Manning criteria
• Pain relieved by defaecation
• Looser stools with pain
• More frequent stools with pain
• Abdominal distension
• Passage of mucus
• Sensation of incomplete evacuation

Rome II criteria
• At least 12 weeks or more in preceding 12months of abdominal discomfort or pain with 2 of the following– Relieved by defaecation– Onset associated with change in frequency of
stool– Onset associated with change in consistency
of stool.
• Supportive features

Supportive features
• Altered stool frequency
• Altered stool form
• Altered stool passage (straining, urgency, incomplete evacuation)
• Passage of mucus
• Bloating

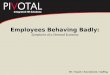
Prevalence of IBS as judged by Manning Criteria
No of symptoms
1 2 3 4 5 6
Male 27 10.7 5.0 2.3 1.3 0.9
Female 46.8 24 13.1 6 2.9 1.4

Epidemiology
• Prevalence – 14-24% women, 5-19% men
• Any age but decrease after 60
• 15% seek medical attention
• 25-50% of all referrals to gastroenterologists
• 2nd highest cause of work absenteeism
• Direct cost in USA $1.7billion in 2000

Social Impact
• Social activities restricted• Fear of travel• Work absenteeism (14.8 days per year v
8.7)• Anxiety• Extreme lethargy• In extreme virtually housebound.• Unnecessary surgery

Aetiology
• Gastrointestinal motility
• Visceral hypersensitivity
• Psychological discomfort
• Emotional distress
• Post-infectious
• Post-surgical
• Food intolerance

Gastrointestinal motility
• Basal motility is not consistently altered in IBS patients
• Gastro-colonic response in IBS results in increased duration of rectosigmoid contractions, compared with controls.
• Stress and anger increase colonic motility in IBS.
• In general motility studies are inconsistent and the normal range is wide.

Visceral Hypersensitivity
• Patients with bloating do not have increased quantities of gas in GI tract.
• Many have lowered tolerance of balloon distension in rectum (and elsewhere).
• Repetitive stimulation of the sigmoid can induce visceral hyperalgesia in IBS patient but not in controls.
• Stress and meals increase sigmoid contractions and hence may induce transient hyperalgesia in IBS.

Visceral Hypersensitivity
• BUT no increased visceral hypersensitivity is found in IBS “non-presenters”
• Visceral hypersensitivity is also found in patients with other chronic pain syndromes.
• Recent work involving functional MRI suggests that visceral hypersensitivity probably results from altered CNS processing of sensory information.

Psychosocial Factors
• IBS patients referred to hospital have an increased prevalence of anxiety, depression, phobias and somatisation.
• 25% think they have cancer.• Increased history of abuse in this group (20-
30%).• Non-presenters have same prevalence of these
as controls.• Psychological distress thus appears to influence
experience of IBS rather than cause it.

Stress
• Acute stress mimicked by CRF infusion– Increased colon motility– Decreased upper gut motility– Induces abdominal pain
• Chronic stress– >50% link onset to stressful life-event– In one study 60% of patients without chronic
stressor improved compared with 0% with .

Postinfectious
• IBS found in 20-30% after acute bacterial infection
• RR of IBS after proven infection =14 (nested case-control of 318 pts with bacterial gastroenteritis and 584,308 controls)
• Risk increased if long duration initial attack, female, younger age.

Possible mechanism
• Mucosal damage particularly with invasive organisms causing neural injury.
• Bile-salt malabsorption.
• Reduced disaccharidase activity.
• Altered bacterial flora
• Increased enteroendocrine cells.
• Unmasked IBD.

Postsurgical
• Hysterectomy, cholecystectomy, appendicectomy and any other abdomino-pelvic surgery may precipitate IBS.
• Prospective studies show about 10% develop new bowel symptoms within 6 months, usually constipation predominant IBS.

Mechanisms include
• Altered bowel flora after antibiotics,
• Neural damage with subsequent aberrant regeneration.
• Bile salt diarrhoea.
• Misdiagnosis of original problem.

Diet
• Intolerance– 30-60% have specific intolerance– Wheat, dairy, potato, corn, coffee, onions,
beef, oats, white wine
• Allergy– Much less common– Asthma, urticaria, angioedema– RAST or pinprick

Diagnosis in General Practice
• Careful detailed history over time• Examination including rectal examination
where relevant.• If typical features, <45y, no alarm
symptoms then make a positive diagnosis– Especially if female, frequent attender, long
history.
• If atypical or short history then screening investigations +/- referral.

When to refer
• Older patient presenting for first time.
• Atypical symptoms– Bleeding– Weight loss– Nocturnal symptoms– Anaemia
• Reassurance in patients with longstanding FGD but with new or worse symptoms.

Diagnosis in Hospital
• Cannot rely on symptom criteria alone
• History
• Examination
• Tests

History
• Onset• Alarm symptoms• Family history• Diet• Travel• Systemic symptoms• Drugs• Stool characteristics

Examination
• Disparity between well looking patient and desperate symptoms.
• Signs of systemic illness eg thyroid
• Abdominal mass
• Rectal examination, sphincter tone.

Investigations
• FBC, ESR, CRP
• TFTs
• Stool microbiology
• Sigmoidoscopy and biopsy
• Hydrogen breath test

Using these tests
• 1452 IBS patients in US study– 6% thyroid disease– 1% occult IBD– 20% lactose intolerance
• Other logical screening tests include– Anti-endomysial antibodies– Albumin– Calcium

Further tests
• Colonoscopy if>45y or FH
• Barium enema
• Barium follow through
• Ultrasound rarely helpful

Treatment of IBS
• General principles
• Therapeutic relationship
• Patient education
• Dietary modification
• Psychological approaches
• Simple drugs
• Complicated drugs

General Principles
• No known cure but “benign disease”
• Focus on symptom relief
• Alleviate concerns
• Simple explanation
• Consider hidden agenda
• Identify exacerbating factors
• Identify psychiatric comorbidity

Dietary Modification
• Fibre
• Lactose avoidance
• Avoidance of foods that increase flatulence– Beans, onions, carrots, sprouts, prunes etc
• Modified exclusion diet ( eg as per Hunter), >50% remission in 2 studies.

Modified Exclusion Diet
• Meat
• Fish
• Fruit (not citrus)
• Vegetables (not sweetcorn, onion, potato)
• Rice

Psychological Therapies
• Relaxation
• Biofeedback
• Hypnotherapy
• Cognitive Behavioural therapy.
• Psychiatry

Simple Drugs –symptom based
• Antispasmodics– Antimuscarinics- dicyclomine, hyoscine– Others- alverine, mebeverine, peppermint– Meta-analysis of 23 controlled trials found a
small but significant benefit (53 v 41%)– Mebeverine failed to show improvement in
pain but did result in global improvement.– Dicyclomine was best for pain.

Simple Drugs
• Loperamide
• Codeine
• Cholestyramine
• Laxatives

Antidepressants
• Several trials show benefit of low and high dose antidepressants.
• Tricyclics can normalise rapid transit times and modify visceral sensation.
• SSRIs can accelerate transit

New Drugs
• 5HT3 antagonists decrease diarrhoea
• 5HT4 antagonists decrease constipation
• Alosetron reduced diarrhoea in females with IBS.
• Tegaserod 5HT4 partial agonist, decrease colonic transit time.

Prognosis
• Incidence of new significant diagnosis is low– One study 0/104 at 5y– Another 3/112 at 5yrs (1 ca pancreas, 1
thyrotoxicosis, 1 gallstones)
• Symptoms persist in 30-95% in various studies.

Treatment Summary
• Positive Diagnosis
• Listen
• Explain and Reassure
• Dietary Advice
• Psychological considerations and treatment
• Pharmacological Treatment