Embed Size (px)
Citation preview

8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 1/18
New Government Payment Initiativesfor Physicians
Presented by:
2014 MGMA/Alabama Winter Conference
March 5-7, 2014
Birmingham, Alabama
Howard E. Bogard
Burr & Forman LLP | Attorney at Law
420 North Twentieth Street | Suite 3400 | Birmingham, Alabama 35203
[email protected] | www.bu rr.com | 205-458-5416
20340844
Topics
Factors Driving a Change in Government
Accountable Care Act ("ACA") Payment Initiatives
New Insurance Coverage Initiatives
Accountable Care Organizations ("ACO")
Medicaid Regional Care Organizations ("RCO")
2
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 2/18
Topics
Factors Driving a Change in Government
3
20340844
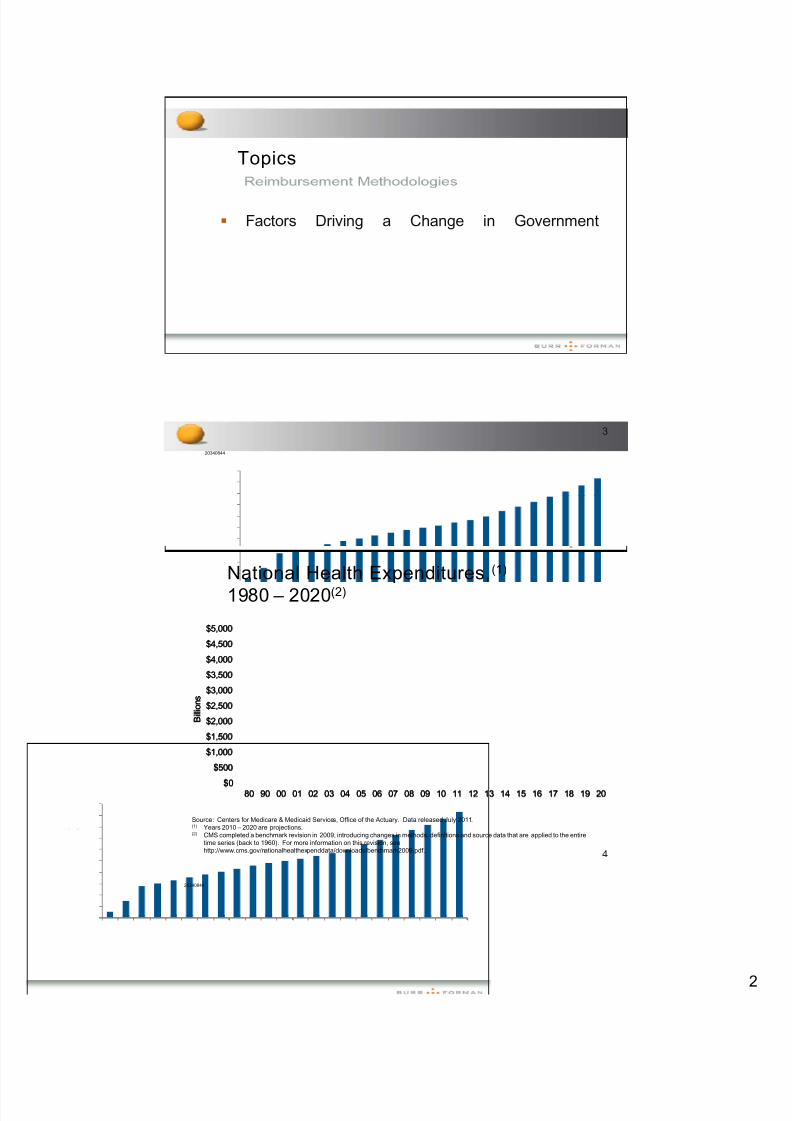
National Health Expenditures,(1)
1980 – 2020(2)
$4,000
$4,500
$5,000
$500
$1,000
$1,500
$2,000
$2,500
$3,000
$3,500
B i l l i o n s
$080 90 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20
Source: Centers for Medicare & Medicaid Services, Office of the Actuary. Data released July 2011.(1) Years 2010 – 2020 are projections.(2) CMS completed a benchmark revision in 2009, introducing changes in methods, definitions and source data that are applied to the entire
time series (back to 1960). For more information on this revision, seehttp://www.cms.gov/nationalhealthexpenddata/downloads/benchmark2009.pdf. 4
20340844
$0
$500
$1,000
$1,500
$2,000
$2,500
$3,000
$3,500
$4,000
$4,500
$5,000
80 90 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20
B i l l i o n s
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 3/18
. 9 . 6 . 3 6 . 9 7
. 5
3 8 . 1
3 8 . 4
3 8 . 8
3 9 . 1
3 9 . 7
4 0 . 1
4 0 . 5
4 1 . 2
4 1 . 9
4 2 . 6
4 3 . 4
4 4 . 4
4 5 . 5
4 6 . 6
4 7 . 7
4 8 . 7
45
50
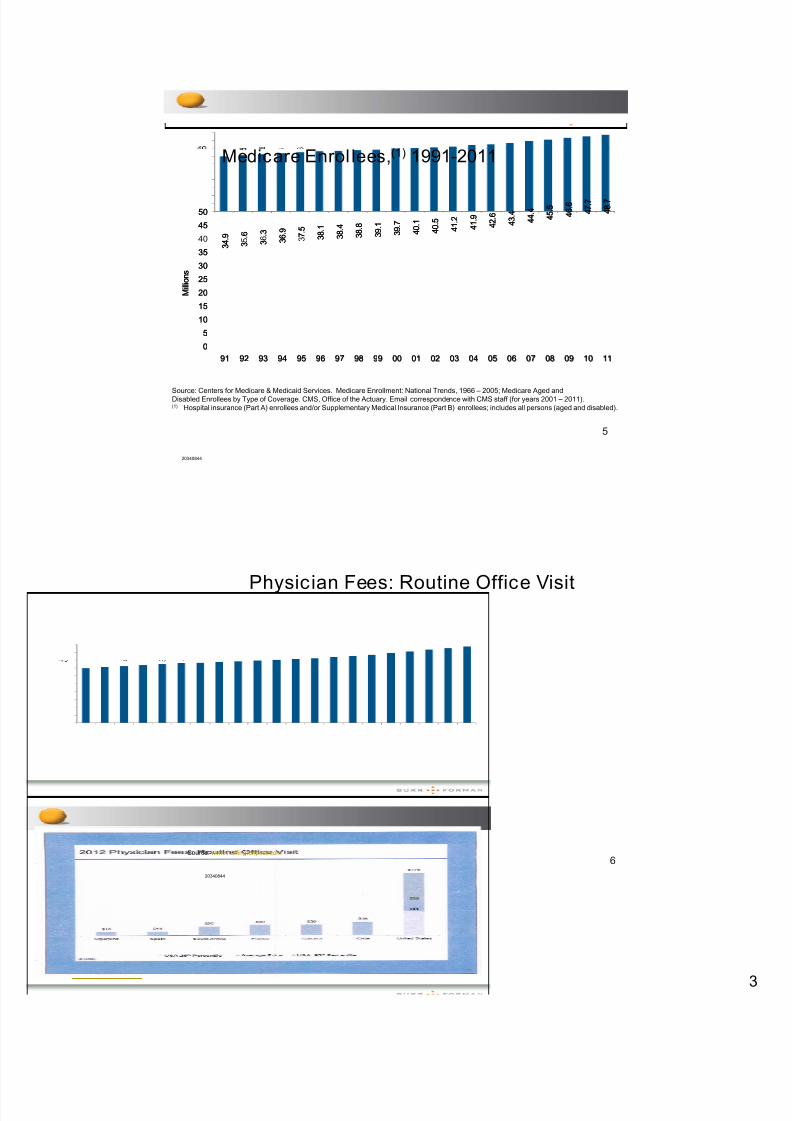
Medicare Enrol lees,(1) 1991-2011
3 4 3 3 3
0
5
10
15
20
25
30
35
M i l l i o n s
Source: Centers for Medicare & Medicaid Services. Medicare Enrollment: National Trends, 1966 – 2005; Medicare Aged andDisabled Enrollees by Type of Coverage. CMS, Office of the Actuary. Email correspondence with CMS staff (for years 2001 – 2011).(1) Hospital insurance (Part A) enrollees and/or Supplementary Medical Insurance (Part B) enrollees; includes all persons (aged and disabled).
91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10 11
5
20340844
3 4 . 9
3 5 . 6
3 6 . 3
3 6 . 9
3 7 . 5
3 8 . 1
3 8 . 4
3 8 . 8
3 9 . 1
3 9 . 7
4 0 . 1
4 0 . 5
4 1 . 2
4 1 . 9
4 2 . 6
4 3 . 4
4 4 . 4
4 5 . 5
4 6 . 6
4 7 . 7
4 8 . 7
0
5
10
15
20
25
30
35
40
45
50
91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10 11
M i l l i o n s
Physician Fees: Routine Office Visit
20340844
6Source: www.huffingtonpost.com
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 4/18
SGR – An Initial Attempt to Control Medicare Spending
Sustainable Growth Rate (SGR) was part of theBalanced Budget Act of 1997
Designed to curb growth of Medicare Part Bexpenditures
SGR is based on a spending target linked to thenation's gross domestic product. Actual spendingon physician's services is compared to the target ─ Spending less than target = Increase in Part B fees ─ Spending more than target = Decrease in Part B fees
Initially SGR benefitted physicians because of strong economic growth
In early 2000s, expenditures exceeded target and
cuts to the physician fee schedule proposed
7
20340844
SGR Delayed – Again
Reductions now stand at 24.4% Congress has recognized that the SGR is flawed Instead of fixing the problem, Congress delayed the
cuts yet again – but only through March 31, 2014!
8
20340844

8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 5/18
Current Change in Reimbursement Methodologies
Payment Reform ─ Move awa from an e isodic a ment a roach that
provides financial incentives based on volume ─ Move to a payment system that rewards outcomes,
quality, prevention, patient satisfaction and reducedcosts to Medicare (i.e., efficiency)
Delivery Reform ─ Move away from uncoordinated care where each
provider (e.g., physician, hospital, home health, .
fashion ─
Move to a coordinated and accountable approach tocare involving providers along the entire patient carespectrum
9
20340844
Topics
Accountable Care Act ("ACA") Paymentn a ves
10
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 6/18
Emphasis on Primary Care/Preventative Services
The ACA creates a 10 percent bonus payment for
physicians beginning January 1, 2011
General surgeons practicing in a healthprofessional shortage area will be provided a 10percent bonus payment for certain major surgicalprocedures
The ACA emphasizes preventative care. Sectiono e prov es or e care coverage o
annual wellness visits, mammograms,
colonoscopies and personalized preventative plans,with no co-payments or deductibles
11
20340844
Payment Changes for Medicaid
The expansion of the Medicaid program willexacerbate the current shortage of primary care
y
The ACA seeks to enhance primary care capacityby increasing Medicaid physician fees for primarycare physicians to Medicare rates, with the federalgovernment picking up the added expense in theinitial years
— r mary are ys c ans = am y me c ne, n ernamedicine and pediatric medicine
— According to The Academy of Family Physicians, theaverage reimbursement will increase 34%
12
20340844

8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 7/18
Quality and Value Requirements
The ACA extends the Physician Quality Reporting Initiative("PQRI") (now called the Physician Quality ReportingSystem) bonus payment through 2014 (1% in 2011; 0.5%n - ; pena es . eg nn ng or a ureto report 2013 data; 2% penalty for 2016 for failure to report2014 data
Medicare Value-Based Payment Modifier ("VBPM").Beginning in 2015, providers who do not meet "value" and"quality" requirements will face a reduced reimbursementrate
— In 2015 only impacts physician practices of 100 or more;2017 all physicians
— Program moves physician reimbursement to a system thatrewards value rather than volume
— Based on PQRS performance13
20340844
Changes in Delivery Model of Care – Bundled
Payments
Section 3023 of the ACA directs HHS to establish a 5-year,national, voluntary pilot program by January 2013
Hospitals, physicians and post-acute care providers will" "
beneficiary
The "episode of care" will center around a hospitalization anda bundled payment will be paid reflecting the savings realizedas a result of integrated care
"Episode of care" – 3 days prior to an admission, length of hospital stay (including ED services), 30 days post-discharge
"Bundled payment" models – establish a single DRG that
includes post-acute care; bundling of physician and hospitalpayment
Some payment models being tested place providers at risk for Medicare expenditures above an established threshold
14
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 8/18
Changes to Hospital Reimbursement
Hospital Value-Based Purchasing Program ─ Ties payment to performance ─ ,
heart failure, (3) pneumonia, (4) surgeries, and (5)infections
Hospital Readmissions Reduction Program ─ Reduced payment (up to 1%) for readmissions within
30 days of discharge Will create pressure on physicians to meet higher
expectations r v ng osp a emp oymen o car ovascu ar
physicians, increased use of hospitalists, emphasis on
post-discharge care coordination and collaborativeagreements with physicians
15
20340844
Topics
New Insurance Coverage Initiatives
16
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 9/18
Changes to Insurance Coverage
Insurers are prohibited from denying coverage basedon re-existin conditions
Coverage for children until age 26
Lifetime limits on coverage eliminated
Annual limits on coverage eliminated
Medicare Part D Prescription Drug coverage gap("donut hole") is closed (phased in from 2010 to 2020)
All plans must cover certain preventative servicessuch as mammograms and colonoscopies without anypatient deductible or co-pay
Expansion of Medicaid – but not for Alabama
17
20340844
Health Insurance Exchanges
Must have coverage by January 1, 2014 or payenalt :
— 2014: greater of $95 per adult/$47.50 per child or 1% of family income
— 2015: $325/$162.50 or 2%
— 2016: $695/$347.50 or 2.5%
Individuals and families that fall within 138% FederalPoverty Level (FPL) and 400% FPL will have access
— Under 138% of poverty level in some states qualify for Medicaid, but not Alabama
18
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 10/18
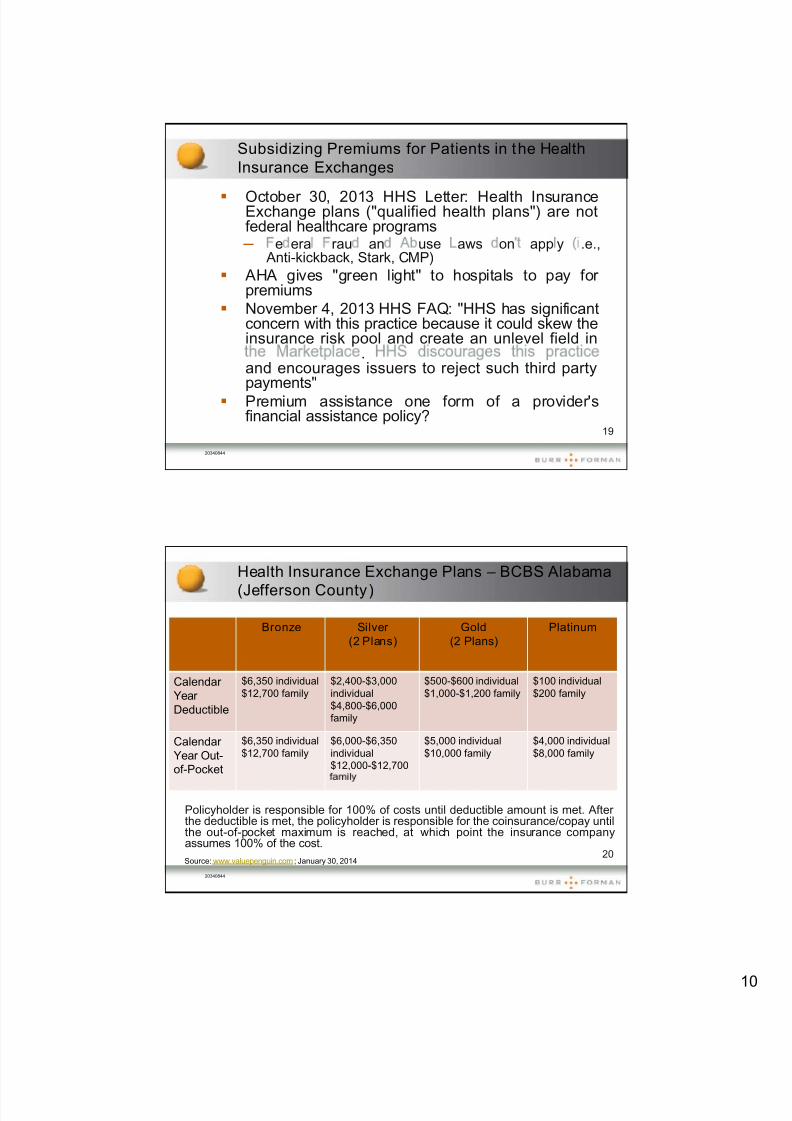
Subsidizing Premiums for Patients in the Health
Insurance Exchanges
October 30, 2013 HHS Letter: Health InsuranceExchange plans ("qualified health plans") are notfederal healthcare programs ─ e era rau an use aws on app y .e.,
Anti-kickback, Stark, CMP)
AHA gives "green light" to hospitals to pay for premiums
November 4, 2013 HHS FAQ: "HHS has significantconcern with this practice because it could skew theinsurance risk pool and create an unlevel field in
.and encourages issuers to reject such third partypayments"
Premium assistance one form of a provider'sfinancial assistance policy?
19
20340844
Health Insurance Exchange Plans – BCBS Alabama
(Jefferson County)
Bronze Silver
(2 Plans)
Gold
(2 Plans)
Platinum
CalendarYearDeductible
$6,350 individual$12,700 family
$2,400-$3,000individual$4,800-$6,000family
$500-$600 individual$1,000-$1,200 family
$100 individual$200 family
CalendarYear Out-of-Pocket
$6,350 individual$12,700 family
$6,000-$6,350individual$12,000-$12,700
$5,000 individual$10,000 family
$4,000 individual$8,000 family
Policyholder is responsible for 100% of costs until deductible amount is met. After the deductible is met, the policyholder is responsible for the coinsurance/copay untilthe out-of-pocket maximum is reached, at which point the insurance companyassumes 100% of the cost.
20
20340844
Source: www.valuepenguin.com; January 30, 2014

8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 11/18
Collecting Deductible Up Front
Except in emergency situations
Inform patient before appointment of financial responsibility
Collect after appointment but before patientleaves the office
Consider payment plans
— Credit cards
— Auto bank drafts
21
20340844
Topics
Accountable Care Organizations
22
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 12/18
ACO Background Information
Section 3022 of the ACA requires the establishmentof a "Medicare Shared Savin s Pro ram" bJanuary 1, 2012 ─ Promote accountability for a patient population ─ Coordinate items and services under Medicare Parts
A and B ─ Encourage investment in infrastructure and
redesigned care processes for high quality andefficient service delivery
Program requirements can receive "shared
savings" if quality and financial performancestandards are met
23
20340844
ACO Summary
In general, an ACO is a network of physicians and
a common set of delivery and financing principles toprovide high-quality efficient care
ACO providers continue to receive fee-for-servicepayments under Medicare Parts A and B
If an ACO meets its quality and financialperformance goals, it will receive "shared savings"
rom e care Shared savings = difference between anticipated
Medicare expenditures for an identified populationless actual expenditures
24
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 13/18
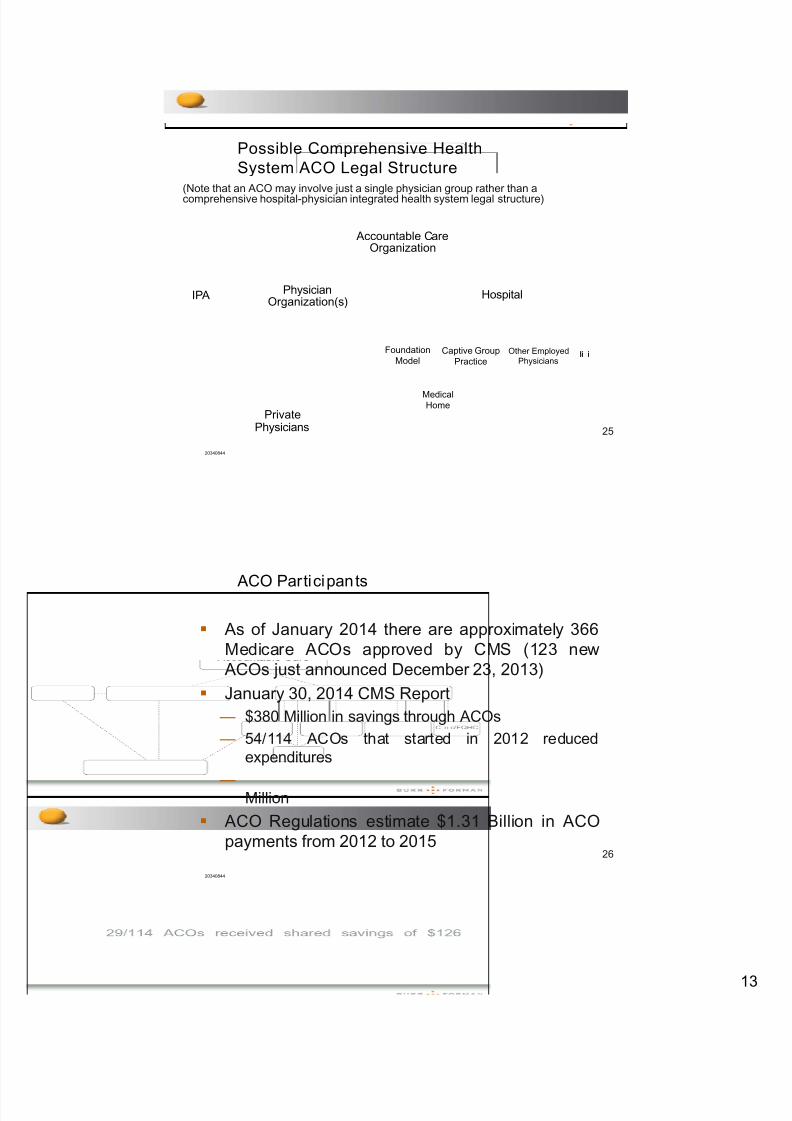
Possible Comprehensive Health
System ACO Legal Structure(Note that an ACO may involve just a single physician group rather than acomprehensive hospital-physician integrated health system legal structure)
Accountable CareOrganization
IPA PhysicianOrganization(s)
Hospital
Foundation Captive Group Other Employed li i
25
20340844
PrivatePhysicians
Model Practice Physiciansli i
MedicalHome
ACO Participants
As of January 2014 there are approximately 366Medicare ACOs approved by CMS (123 new
ACOs just announced December 23, 2013)
January 30, 2014 CMS Report
— $380 Million in savings through ACOs
— 54/114 ACOs that started in 2012 reducedexpenditures
— Million
ACO Regulations estimate $1.31 Billion in ACOpayments from 2012 to 2015
26
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 14/18
Special Considerations for Physicians
Will you be invited to participate in an ACO? /Do you want to participate?
─ participation not exclusive (unless PCP)
Risk v. Reward ─ financial and administrative "costs" to participate ─ will participation result in increased patients / not
participating result in a loss of patients ─ how will shared savings and losses be allocated
Will the cost of reducing utilization inorder to achieve the minimum savingsra e, n a on o me ca ma prac cerisks associated with a change in the
treatment plan, be offset by the sharedsavings?
27
20340844
Topics
Medicaid Regional Care Organizations
28
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 15/18
Alabama Medicaid
Approximately 940,000 Medicaid Enrollees (up from904,000 in 2003) (out of 4.8 million people in
Alabama
In 2011, 22 percent of Alabamians qualified for Medicaid for at least a portion of the year
Medicaid covers 53 percent of births, 47 percent of children, and almost 66 percent of nursing homeresidents
Fiscal Year 2012 Medicaid expenditures were$5.63 billion (67.4% Federal; 32.6% State ($1.835billion))
Governor Bentley elected not to expand Medicaidrolls to 138 percent of the poverty level under the
ACA 29
20340844
Regional Care Organizations (RCOs) An organization of health care providers that
contracts with the Medicaid Agency to provide acom rehensive acka e of benefits to Medicaidbeneficiaries in a defined region of the State
Through a capitated payment, RCOs would providephysical (e.g., physician and hospital), behavioral,pharmacy and long-term care services (e.g., post-acute and rehab)
Pro ected savin s between 748 million and 1.079billion over five years
30
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 16/18
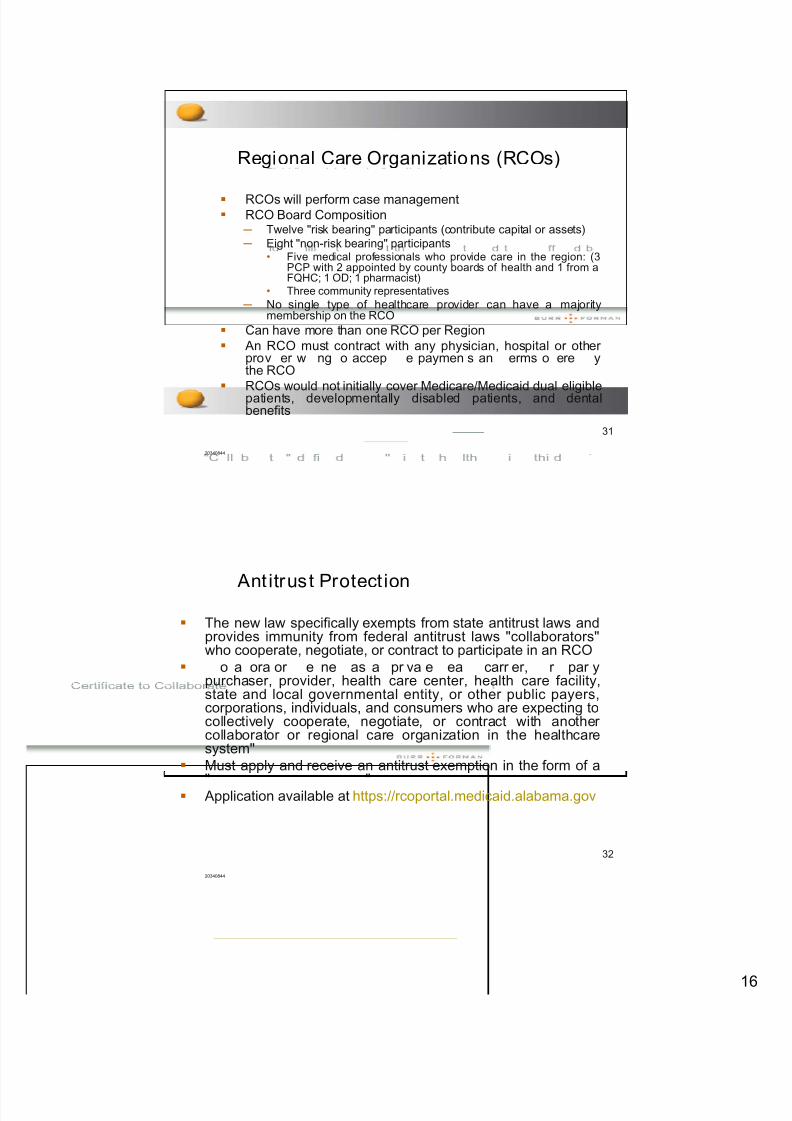
Regional Care Organizations (RCOs)
RCOs will perform case management RCO Board Composition
─ Twelve "risk bearing" participants (contribute capital or assets) ─ Eight "non-risk bearing" participants
• Five medical professionals who provide care in the region: (3PCP with 2 appointed by county boards of health and 1 from aFQHC; 1 OD; 1 pharmacist)
• Three community representatives
─ No single type of healthcare provider can have a majoritymembership on the RCO
Can have more than one RCO per Region An RCO must contract with any physician, hospital or other
prov er w ng o accep e paymen s an erms o ere ythe RCO
RCOs would not initially cover Medicare/Medicaid dual eligiblepatients, developmentally disabled patients, and dentalbenefits
31
20340844
Ant itrust Protect ion
The new law specifically exempts from state antitrust laws andprovides immunity from federal antitrust laws "collaborators"who cooperate, negotiate, or contract to participate in an RCO
o a ora or e ne as a pr va e ea carr er, r par ypurchaser, provider, health care center, health care facility,state and local governmental entity, or other public payers,corporations, individuals, and consumers who are expecting tocollectively cooperate, negotiate, or contract with another collaborator or regional care organization in the healthcaresystem"
Must apply and receive an antitrust exemption in the form of a
" " Application available at https://rcoportal.medicaid.alabama.gov
32
20340844
8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 17/18
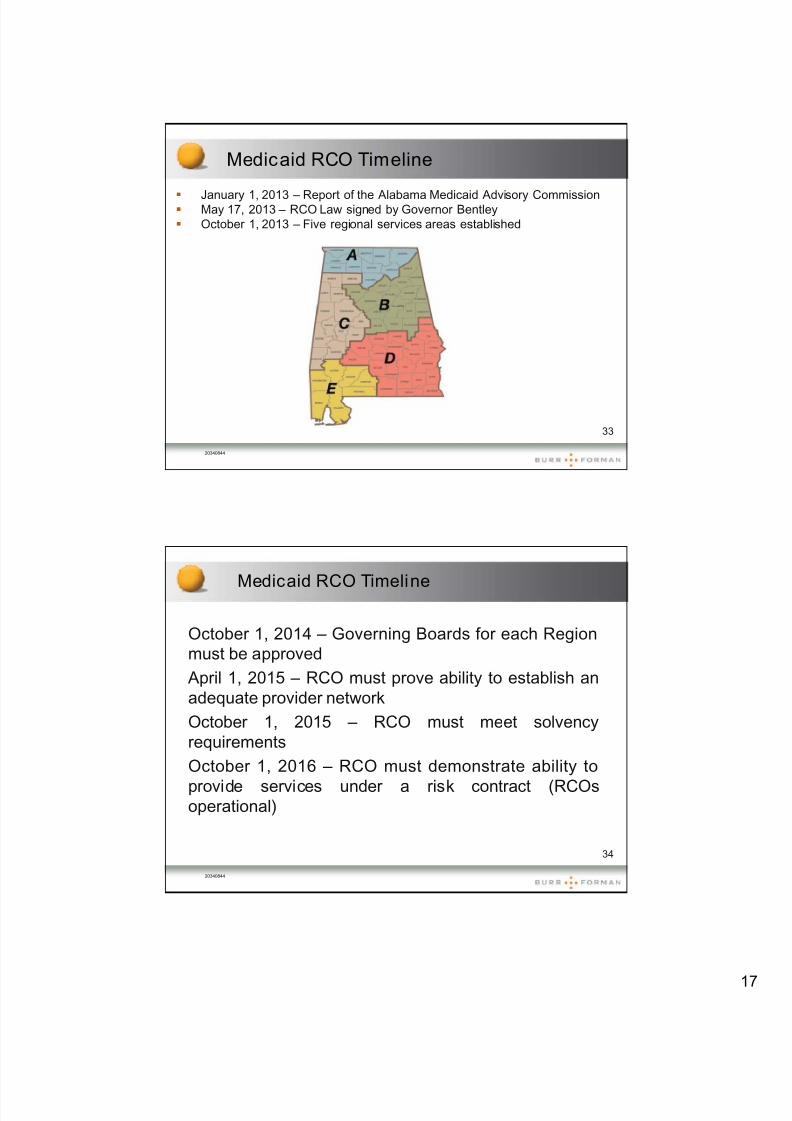
Medicaid RCO Timeline
January 1, 2013 – Report of the Alabama Medicaid Advisory Commission
May 17, 2013 – RCO Law signed by Governor Bentley October 1, 2013 – Five regional services areas established
33
20340844
Medicaid RCO Timeline
October 1, 2014 – Governing Boards for each Regionmust be approved
April 1, 2015 – RCO must prove ability to establish anadequate provider network
October 1, 2015 – RCO must meet solvencyrequirements
October 1, 2016 – RCO must demonstrate ability to
provide services under a risk contract (RCOsoperational)
34
20340844

8/12/2019 Bogard - New Government Payment Initiatives for Physicians
http://slidepdf.com/reader/full/bogard-new-government-payment-initiatives-for-physicians 18/18
Take Aways
Shift away from "fee-for-service" to "fee-for-value"
Learn the new vocabular : "Pa for Value ""Bundled Payments," "Accountability," "PQRS,""VBPM," "RCOs," and "ACOs"
Determine your costs of care
Create Efficiencies
— Purchasing
— Clinical best practices; benchmarks
— Information management — Billing (avoid errors)
35
20340844
Questions?
Howard E. Bogard
Burr & Forman LLP
420 North Twentieth Street
Suite 3400
Birmingham, Alabama 35203
(205) 458-5416
36
20340844