Embed Size (px)
Citation preview
BCH OBlGYN PATIENT PORTAL
*ALL OF YOUR NORMAL LAB RESULTS WILL COME TO YOU VIA OUR SECURE PORTAL*
You will also be able to view your health information, see your medications, request an appointment, see your upcoming appointments or ask your provider questions concerning your health. Get it all, through our FREE and SECURE patient portal.
Steps to join: @ Say "yes" I want to join 4? Our staff will send you an invitation B Click on the link @ To login, create a username with FMH or use your existing Yahoo, G-Mail,
Facebook, or Microsoft account, etc. 42 You will then agree to use this user name and password to follow your health
You will have a one time invitation code (the last 4 of your SSN or the year you were born) -
Q! Read our HlPPA statement 42 You will then go to your health record @ You can send messages to our office by hittirlg "messages" and then hit
"message icon" (not the one with the plus sign) @ Use the "My Health" tab to access your labs, vitals, and medication list
If you need assistance Support Hotline: (888) 670-9775
Beach " -8""";+* 8 % 3 kl. y
L 2 ** ; 3
Follow and be engaged in your health! Sign up below; you will receive an invitation in your email shortly. Keep this sheet, follow
the instructions and be on you way to a convenient way to manage your health! Get the FREE app in the iTunes or Google Play store.
(Tear here)
Sign up to receive your patient portal invitation (PLEASE WRITE LEGIBLY)
Name
Date of Birth
Email address
f- Nortn fi'lorlda VB/G Y 1Y
BEACHES DMSION 1577 Roberts Drive Suite $--5, Jacksonville Beach, FL 32150 Phone: (90 11-9775 Pu: (904) 249-3638
(Please fill out all information to the best of your ability)
'atient's Name: Today's Date: Age: DOB:
teferred by: Race: Marital Status: LMP:
leason for Appt: Pharmacy: (Local and Mail Order)
~1lergyReaction: Primary Care Physician: (Please list anything you are allergic to and the reaction it causes.)
ledications & Dosages:
Past Medical Historv: Have vou ever had any of the following illnesses? Circle Yes or No.
i N Have you ever had a blood transfusion? Y N Are you wining to have a blood transfusion to save your life?
i N Ever had an abnormal Pap Smear? Eyes, treatment - ., & Year(s): i N Heart Trouble Y N Osteoporosis Y N Diabetes Y N GonorrheaIChlamydia i N KidneyiBladder Problems Fibroids
-or- Urinary Incontinence Y N Bleeding DisordersiBlood Clots Y N Hepatitis
! N EIigh ~ l o o d Pressure I N Low Blood Pressure
Y N Pelvic Prolapse Y N Breast Discharge/Problem
! N Migraine Headaches Y N DepressionIAwiety Y N Hemorrhoids Y N Herpes I N Thyroid Problem Y N Endometriosis Y N Anesthesia Problems Y N Genital Warts I N Rectal Bleeding Y N Seizures Y N Heart Murmur/MVP Y N Syphilis I N Ulcer Y N Anemia Y N Antibiotic for dental work Y N RPV I N IBS Y N High Cholesterol Y N Polycystic Ovarian Syndrome ~ C O S ) Y N Abnormal Mammo I N Infertility Y N Anxiety Y N Ovarian Cysts Cancer History:
Obstetrical History Please list the number of. ~ o ~ r
Premature Births Miscarriages
ILLNESSES or OPERATIONS I COmD'icatiOns YES or NO
Abortions Times Pregnant
Pregnancv History: Please list all premancies (including: ectopic/miscarriage/abortion~. Date Delivery Type (vaginallcesarean) Sex LbsIOz Complications
Familv Historv: Please list illnesses of these family members: children/mother/father/siblings/g;randparents Y N Diabetes
Other Significant Family
Y N Breast Cancer Y N Uterine Cancer Y N Skin Cancer Y N Ovarian Cancer 1 I Y N Blood Disorder
History:
Y N Heart Disease Y N HighBlood Pressure Y N High Cholesterol
Y N Colon Cancer
Social Histo I Use of alcohol: NeveriDailyIModerate ( Tobacco Use: Have you evezmoked? Y N
1 Y N Thyroid Disease
1 Drug use: Y N I Current Smoker: packs per day OR Former Smoker: quit date
History of Domestic Violence: Y N I
Sexuallv active: Y N Birth control method:
Revised 121312012
Felix N. Acholonu. M.D. Christina S. A d m . M.D. Karhi A. Aultman. M.D. Sarah Campbell Austin. M.D. E m ~ a i r d . M.D. Emily L. Balanhy. MD. Wade Barnes. M.D. Kathryn F. Bing, M.D. John G. Bordelon. M.D. Marijane Q. Boyd. MD. W. David Boyd. M.D. C. Leanne Browning, M.D. Craig Cantor. M.D. Caroline 1. Canion Zarapza M.D. James K. Cbafin. M.D. B. Veeren Chirhriki. M.D. Samuel A. Christian. M.D. W l l l i ~ L . Cody. M.D. Angela S. Collier. M.D. Patrick M. Connor. MD. Stacie Cwl i M.D. S h m n Desmarais. MD. Roben E. Dupree Jr.. M.D. Eric 1. Edelenbos. D.O. Kristin P. Femande~ D.O. Lindsay DeNicola Foun. M.D. Martin A. Garcia. MD. % D. (31%. M.D. Steven E. Goldwasser. MD. C. Cameron Grccne. MD. Joseph C. Greenhaw, M.D. Amy D. Greenwald, MD. Caron D. Gutovin. M D . Richard A. Harren Jr.. M.D. LatoyaT. Kuester. M.D. Annette Laubscher. M.D. Meng-~hu Lin. M.D. Wdliam H. Long, M.D. Richard A. McCauley, M.D. E. William McGrarh, Jr., M.D. Catherine J. McIntyre. MD. Richard L. Myers. M.D. Carole L. Neuman, M.D. Wdford E. Paul t M.D. T. Michael Phelan. M.D. R. Roland Powers, D.O. Michelle Quinones. M.D. Paul Rebenack M.D.
Leandro 1. Rodriguez. M.D. Lorraine Rodriguez. M.D. Neil Sager. D.O. Patricia Sciuoeder. M.D. Arjav Ted Shah. M.D. Sayra C. S ievm M.D. Kelley K Stoddard. M.D. Frank E. Trogolo. M.D. Jason L. VanBennekom. M.D. ,Thornas R Vucue. M.D. Elizabeh Mogan Walsh. M.D. Mary Ellen Wechter. M.D..M.P.H. David Scon Wells. M.D. Tracy Wells. M.D. Amy Wrennick. M.D.
Nonh Florida Central Senices Sandra 0 . Dooliule. Executive Director 11437 Ccnml Parkway. Suite 105 Jacksonville, FL 32724 (904) 471-300 Website: www.nfobgyn.com
NORTH FLORIDA OB GYN, LLC Fellows of the American College of Obstetricians and Gynecologists
PATIENT OUESTIONNAIRE
Patient Name: Date:
Family Planning:
Are you finished having children?
Yes No Maybe
Would you be interested in permanent birth conk01 with no cutting, no scarring, & no hormones?
Yes No Maybe
Heavy Bleeding:
What is the hequency of your period?
dl days 21-35 days >35 days
How long does your period last?
>7 days 5-7 ddays
How would you describe your period?
Heavy Medium Light
Does your period disrupt your Life?
Frequently Sometimes Never
Urinary Incontinence:
Do you leak urine when you cough, sneeze, laugh, or during physical activities?
Frequently Sometimes Never
Do you suffer hom urinary frequency?
Always Sometimes Never
Do you usually have a strong sense of urgency to urinate?
Frequently Sometimes Never
Does the loss of urine or overactive bladder a££ect your quality of Life?
Frequently Sometimes Never
1577 Roberts Drive Suite 323 Jacksonville Beach, Florida 32250 (904) 241-9775 FAX.(904) 249-3638
Risk Assessment for Lynch Syndrome and Hereditary Breast and Ovarian Cancer Syndrome
Patient Name: Physician:
Date o f Birth: Date Completed:
Instructions: Please circle Y fo r those tha t apply t o YOU andlor YOUR FAMILY (on both your mother'slmaternal or father's/ paternal side). Next to each statement, please l ist the relationship t o you and age o f diagnosis. You and the following family members should be considered:
Mother Father Brother Sister Children Paternal UnclelAunt Maternal UnclelAun t Erst Cousins NiecelNephew Maternal Grandmother/Grandfather Paternal GrondmotherlGrandfather
Each statement should be answered individually, so you may list t he same cancer diagnosis more than once as you answer these questions. This is a screening tool fo r the common features o f hereditary breast and ovarian cancer syndrome and Lynch syndrome. Share this information w i th your healthcare professional t o help determine your hereditary cancer risk.
Y N * uterine (endometrial) cancer before age 50
Y N Colorectal cancer before age 50
Two or more Lynch syndrome cancers* in the same person or on the same side o f the family rLynch syndrome cancers include: colorectal, uterinelendometrial, ovarian, stomach. ureterlrenal pelvis, biliarv tract, small bowel,
oancreas. brain or sebaceous adenomas)
Y N Breast cancer a t age 50 or younger
Y N Ovarian cancer
Two primary (unrelated) breast cancers i n the
- same person or on the same side o f the family
Y N Male breast cancer --- Triple negative breast cancert (ER-. PR-, HER2- pathology)
Pancreatic cancer wi th breast or Y N ovarian cancer in the same person or on
the same side o f the family
Ashkenazi Jewish ancestry w i th breast, Y IN ovarian or pancreatic cancer i n the same
person or on the same side o f t he family
, ,, Have you or any member o f your family ever been tested fo r hereditary risk o f cancer? I IY
If yes, please explain:
Patient's Signature Date
1 FOR OFFICE USE ONLY Patient offered genetic testing:
I Candidate for further risk assessment and/or genetic testing: Lynch !l HBOC Accepted Cl Declined
I Information given to patient to review
I El Follow-up appointment scheduled Date: I
/ Healthcare Professional's Sionarure Date
i For a better undersbnding of triple negative breast cancer, p leas ask your healthcare provider. Assessment criteria based on medical society guidelines. For these individuals society guidelines go to www.myriadtests.comlpatient~guidelines Myriad, and the Myriad logo are either trademarks or registered trademarks of Myriad Genetics. Inc, in the United States and otherjurisdictions. q O l l
North Florida 0 5 GYN
Beaches OB GYN
ENIR - Patient Update Form
Last Pap Smear:
Last Mammogram:.
Last Bone Density:
. .
Last Colonoscopy:
Last Pneumo Shot:
Last Flu Shot:
Patient Name:
Patient Signature:
Date:
Page TWO NORTH FLORIDA OB GYN, LC l?IPUNCIAL AGREEMENT
I. Annual 'kvell-women" exams are preventive visits and are not paid for by all insurance carriers. Medicare only pavs for a ?ortion of this exam Pap. Pelvic and Breast Exam', once every two (2) years. I understand I am responsible for payment, if the exam or portion of the exam is not covered by my insurance.
( Annual exams do not rypically include problems I may be having - as problem visits may require longer h e . If1
I hereby consent and authorize the performance of all appropriate procedures and courses of trealment, the admimshtion of all anesthetics, and any and all medications which in the judgment of my provider may be considered necessary or advisable for my diagnosis andlor treatment. North Florida OB GYN, LLC and other PA subsidiaries may share one el.ectronic medical record (TMR"). To facilitate the provision of my medical care, I consent for North Florida OB GYN, LLC to access my medical records maintained by any other PA subsidiary.
I understand additional charges are applied to my account for any returned checks used to pay on my account, for 1 certified letters sent to me for collection on my account.and collection agency fees. I may also be charged if I do not cancel my scheduled appoinbnenf for not my co-pay andlor co-insurance or patient responsibihty including deductiale at the time of Service, for telephone management services, for educational materids, for payment agreements which extend beyond'l2 months, and for other administrative expenses not covered by my
,
.
.
1 insurance pIan.
Payment may be made to the PA in the form of: Cash, Check, Debit and Credit Cards. h. the event I receive payment fiom my ikurancg canier, I agree to endorse any payment due for Services rendered to me by North .
Florida OB GYN, LLC. Patient credits are applied to other outstanding patient balances prior to any refinds that may be issue&. including balances owed to other wholly. owned subsi.diaries of-the 'PA.. . . . . . . .. . . - -
I consent I
-
For the services rendered by North Florida OB GYN, LLC, I authorize the release of any medical. or other dormation necessary to process .claims to my insurance canier. This may include the diagnosis and records in the course of my examination or keatment. I also request payment of government benefits either to myself or to the party who accepts assignment (North Florida Obstetrical & Gynecological Associates, PA.). I agree to hold North Florida OB GYN, LLC harmless bom any and all costs, liability and damages of and nature wktsoever includ.ing reasonable attorney's fees, resulting directly from the release of my medical records plirsuant to this
I BY SIGNING THIS AGREEMENT, I ACKNOWLEDGE THAT I ELAVE CAREFULLY READ, 1
'
UNDERSTAND AND AGREE TO T H ~ ABOVE TERMS AND CONDITIONS.
Patient's Printed name Patient's Date of ~ i h h :
Patieht's Signature: Date signed:
.P'arent, Guardian or Legal Representative Signature:
'Employee's sipature who reviewed intake of form:
Patient Name: NORTH FLORIDA OB GYN, LC FINANCIAL A,GREEMENT
I aclmowledge that I have had the opportunity to review a copy of North Florida OB GYN LLC's Privacy Notice dated September 01, 2013 ('T-fotice"). I'understand that I am responsible to read this Notice and not& North Florida OB GYN, in writing, of any request for restrictions in the use or disclosure of my individually identifiable health mformation. I understand thenotice included eleckonic access to my medication hstory. NO& Florida OB GYN has the right to revise h s Notice at a n m e and will post a copy of the current Notice in the ofice in a visible locati~n at all -times and on their website at www.nfobgyn.com. North Florida OB GYN dl provide me with, a copy of its most recent Notice upon my request. Patient Signature: Date of Birth: .
Parent, Guardian or Legal Representative Signature: I-
North Florida OB GYN, ,LLG is a wholly owned subsidiary of North Florida 0bste~ca.l & Gynecoiogical Associates, P.A. ("PA") who may 5le a claim for payment and accept assignment with my insurance company as required by contractual agreement. If the insurance compgny fails to pay a h e l y manner for aiiy reason, then I understand that I will be responsible for prompt payment of all amounts owed. Should thc account be referred to a collection agency or attorney for collection, the undersigned shall pay all fees for collection, includmg a reasonable attorney's fee.
I understand that in consideration of the services provided to the patient, I am directly and primarily responsible to pay the amount of all charges ih&red for services and procedures rendered at North Florida OB GYN, LLC. I am responsible for any zpplicable deductible, co-insurance or co-payments prior to the provision of services. For surgery and pregnancy, North Florida OB GYN LLC will provide me with an e s b a t e of my total h c i a l responsibility and the date by which this amount must be paid in full. I understand that due to the individual needs of each beakaent, procedure or pregnancy, this fee is only an estimate. In the event my care exseeds the ~ . g ~ - o L L & e - g ~ a . t e T ~ - ~ - b e e h G i & j y r e s p ~ . n s ~ ~ l e - f ~ ~ - ~ e & a l . ~ ~ ~ ~ ~ ~ - ~ ~ t .me&~-~-be- :a$p~ed-~o. -my other outstanding patient balances pripr to any refund issued. I further understand that such payment is not conhgent on any insurance, settlement or judgment payment
.. .
I understand that if I do not have a copy of a current imumnce card andlor valid referral, North Florida OB GYN is not obligated to see me. But if I still wish to be seen, I can be seen as a "Private Pay" patient. I agree that neither the PA, nor I, will 5le a claim for the visit I will be required to pay the total cost of the visit in advance. In addition, there may be a service I desire, suggested or provided that is not covered under my insurance plan 'Won-Covered Services"; I understand I must pay for Non-Covered Services. If feasible, a waiver will be
-- -- completed for each Private Pay visit or Non-Covered Service. I understand services sent to an outside lab are -- - ----- billed to my insurance or me by the lab and I will receive a separat=voice fiom the lab.
'
.
I understand that it is my responsibility to provide North Florida OB GYN with a copy of my current insurance card and, if required by my insurance, t o obtain a referral from my.Primary Care Physician. North Florida OB
, GYN is not obligated to see patients without a valid referral. If I do not have insurance, I will bei considered a Private Pay (or Self Pay) patient and I am hancially responsible.for the total amount of the services provided I will notify North Florida OB GYN immediately-upon any'change t o my insurance.
NORTH FLORIDA OB GYN, LLC Fellows of the American College of Obstetcicians and Gynecologists
F,,
&.&a -I3 w P$$'=-- 7.- Q \ ; , ! i ' 4 1 6 .
b- L;' :LI N. A&olona MD. k&Cm S. A h MD. &j A Aulhmu MD. d CampCn Austin MD. un Baird MJ).
mily L Bd*. M.D. rade Barn= MD. Notice to Our Patients ahyn F . B i i MD. ~ h n G. Ba&lon MD. Izrijime Q. Boyd. MD. I. ~~~d B V ~ . MD. ***PT's THAT ARE 15 MINUTESLATE FOR AN APPOINTMENT .
-Lc;mneBmmiqMD. big Ca;lmr MD.
COULD BE RESCHEDULED 'AT THE D O ~ O R ' S DISCRETION*** Amline J. Canion Z8;1.on. MD. nu= K Chafin M D . .vcerm ~~ MD. Due to increasing costs and complexity of regulations, we have found it ~ ~ A - E N ) . necessary to-charge for some servkes, which we have provided free in the ma L Cody. MD. m=da S. C O ~ U MD.
p a s t Insurance carriers d o not cover these services and we must request ' a h i c k ~ ~ ~ M D . payment a t t h e time of service. bck Cook MD. hLTunizklmmkMD. tobm E ~ r r p h e k- MD. These IUON-COVERED SERVlCES include: :kc I. Edclmbos. D.O. Srisrin P. Fcmaodu D.O. Adsay DcNicoLa Fonp m. vl&AGHdaMD.
. A "NO-SHOW" charge of $40.00 for appointments which are 3 k a D . G k s . ~ . missed without notifying this office 24 hours in advance. StcpaE Goldvmscc MD. c-Grtmr.MD. J o s e C Grunhaw. MD. Amy D. G r r m W MD. Caron D. ~ o m v i ~ MD. Forms to b e completed such as Disability, Life Insurance, Short Richard A H a m h M13. Lamya 1. pcsrsr. MD ,
Term Disab,ility and FMLA, etc. Our fee is $25.00 per form. Please -re L a n b s k M.D. leave form with u s and aUow7-10 business days for completion. -Sba Lb. MD. William K ,La= MD. Richard A McCmlcy, MD. ~~~~GladL3r.m. c a r h a i n e ~ . ~ r l n ~ ~ ~ .
Copies of Medical Records, requested by the patient In accordance- F-khaid L MY= MD. with Florida Administrative Code 64B8-10.003 t he se t price is $1.00 CamL L NUU~LUL MD. w~lford~mhr~~. per page up t o 25 pages, then 25C per page for the remaining T. ~ i c k l phclaa MD. pages. FL Roland Powers. D.O. Mi&& Quinons. M.D. PaalPabcUackMD. Leandm L Rodiipz MD. Lmainc R o d r i : ~ ~ MD. Neil S q q D.O. =la Schrocder. MD. Ajav T d Shah MD. S W ~ C sicvar MD. Patient Signature: Date: =ley Lt s t o w MD. Franl; E ~r0p10. m. Jason L VanBumckDm MD. ~ ~ ~ ~ V m n r . r n . -ah M o w Wdsh MD.
weehe. MD.WH Staff Witness: Date: David Sma Weh. MD. f W c k M.D. b y Wrrnnick m.
NCrh ~lorida ~ m k d Scrvictz 0. Doolitrlc b v c -r
1 1437 cerrrm p e a y . 10s J a c b m w i i FL 3 7 2 a (904) 472-300
w . n f o b m c o m 1577 Roberts Drive - Suite 323 Jacksonville Beach. Florida 3 7 7 0 - (904) 7-41-9775 - FAX (904)
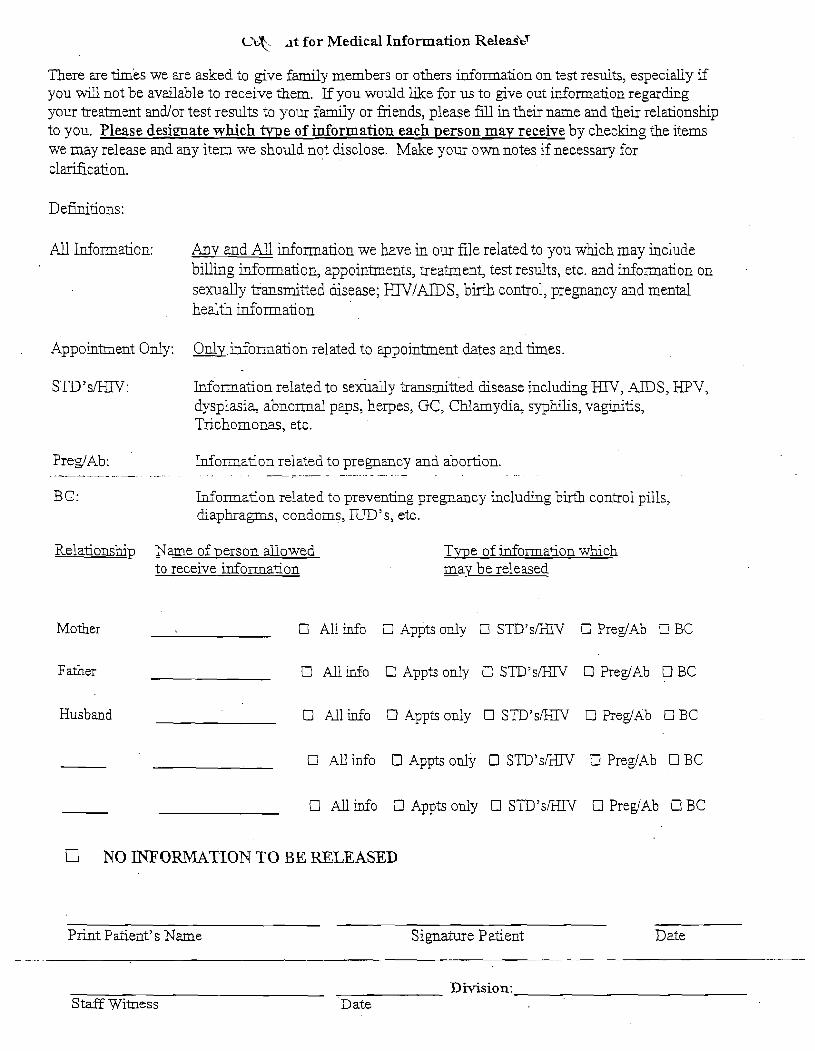
L ' L ~ ~t for Medical Information Releas'ty
There are times we are asked to give family members or others dormation on test results, especially if you vd l not be available to receive them. lf you would Use for us to give out information regarding your treatment andlor test results to your family or fiiends, please fill in their name and their relationshrp to you. Please desiaate which m e of information each person may receive by checking the items we may release and any item we should not disclose. Make your own notes if necessary for
All Information: h v and All mformation we have in our file related to you whch may include billing mformation, appoinhnents, treament, test results, etc. and ~nformation on sexudly transmitted dsease; HIVIAIDS , bnth control, pregnancy and mental health mformation
Appoinkent Only: 0nlv.iaformation related to appoinment dates and fines.
Information related to sexuaily transmitted disease includmg HIV, AIDS, HPV, dysplasia, abnormal paps, herpes, GC, Chlamydia, syphilis, vaginitis, Trichomonas, etc.
Preg!Ab : Information related to pregnancy and abortion. . . .. - -- . - . - .. . . - . . - -. . . . . . . . . . . - - - . - - -- . . - . - - . . . - - - - -. - . . - . . . .. .
BG: Information related to prevenkg pregnancy including b i rd control pills, diaphragms, condoms, IUD's, etc.
Relationship Name of Derson allowed to receive information
Tvpe of dormation which may be released
Mother All info ~ p p t s only STD'sEXV PregIAb B.C
Father All info Appts only STD'sEXV PreglAb BC
Husband U All rnfo Appts only STD's/HN PregIAb BC
All info A~pts only STD's/HSV PreglAb BC
All d o O Appts only STD's/HSV PreglAb 0 BC
NO INFORhlATION T O BE RELEASED
Print Patient's Name Signature P atient Date
Division: St& Witness Date
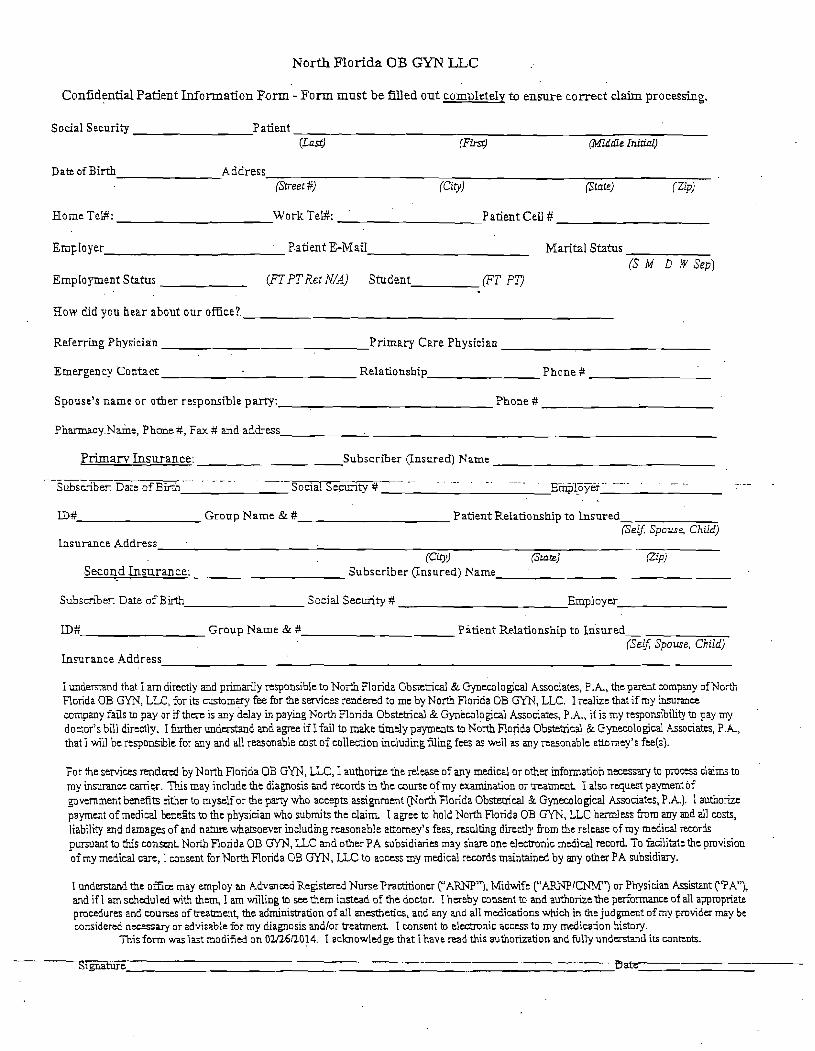
North Florida OB GYN LLC
Confidential Patient In fo rma t ion P o r m - F o r m must be ?Xed o u t completely to ensu re cor rec t claim processing.
Social Security Patient (Lad (Fir.$) (Miidle Inirinl)
Date of Birth Address (Street Q f c i ~ ) (St~te) f zip)
Home Tel#: \Vork Tel#: Patient CeU #
Employer P.atient E-Mail Marital Status (S M D W Sep) . .
EmpIojment Status (FT PT Rer N/A) Student (FT PT)
Row did jlou hear about our office?.
Referring Physician Primary Care Physician
Emergency Contact Relationship Phone #
Spouse's name o r other responsible party: Phone #
PharmacyN&e, Phone #, Fax # and address
Pr iman Insurance : Subscriber (Insured) Name
---.--. . .. ... -- - . . Social-sF~ty#- - . - . . Etnp.IEyer .. . . . . - -. Subscriber: Date of B?h .,
. . LD# Group Name & # Patient Relati.onship to Insured
(Self; Spouse, Child) Lnsurance Address .
(Cio!J (Srarel Pipi Second Insurance : Subscriber (Insured) Name .
Subscriber. Date of Birth Social Security # Employer
LD # Group Name & # Patient Relationship to h u r e d - (Serf; Spouse, Child)
Lnsurance Address
I understand that I am directly and primarily responsible to North Florida Obstebical & Gynecological Associates, P.A., the parent company ofNorth Florida OB G W , LLC, for its customary fee for the services rendered to me by North Florida OB GYN, LLC. I realize that if my insurance company fails to pay or if there is any delay in paying N ~ r t h Florida Obstetrical & Gynecological Associates, P.A., if is my responsibility to pay my doctor's bill directly. I further understand and agree if I fail to make timely payments to North Florida Obstetrical & Gynecological Ass~ciates, P.A, that I will be responsible for any and d l reasonable cost of collection including filing fees as well a s any reasonable attorney's fee(s).
For the services rendered by North Florida OB GYN, LLC, I authorize the release of any medical or other information necessary to process claims to my insurance carrier. This may include the diagnosis and records in the course of my examination or treatment I also request payment of government benefits either to myself or the party who accepts assignment Porth Florida Obstetrical & Gynecological Associates, P A ) . 1 authorize payment of medical benefits to the physician who submits the claim I agree to hold North Florida OB GYN, LLC harmless h m any and all costs, liability and damages of and nature whatsoever including reasonable attorney's fees, resulting directly %om the release of my medical records pursuant to this conscnt North Flo~ida OB GYN, LLC and other PA subsidiaries may share one electronic medical record To facilitate the pmvision of my medical care, 1 consent for North Florida OB GYN, LLC to access my medical records maintained by any other PA subsidiary.
1 u n d m d the oEce may employ an Advanced Registered NursePractitioner ("ARNP'), Midwife ("AP.NPICNM") or Physician Assistant r'PA"), and if l am scheduled with them, I am willing to see them instead of the doctor. I hereby consent to and authorize the performance of all appropriate procedures and courses of b-eabnenf t!ne administration of all anesthetics, and any and all medications which in the judgment of my provider may be considered necessary or advisable for my diagnosis andlor treatment I consent to electmnic access to my medication history.
This form wa last modified on 021261'20!4. I acknowledge that I have read this authorization and fully understand its contmk.
- Signature --- ---- L l a r e - - -
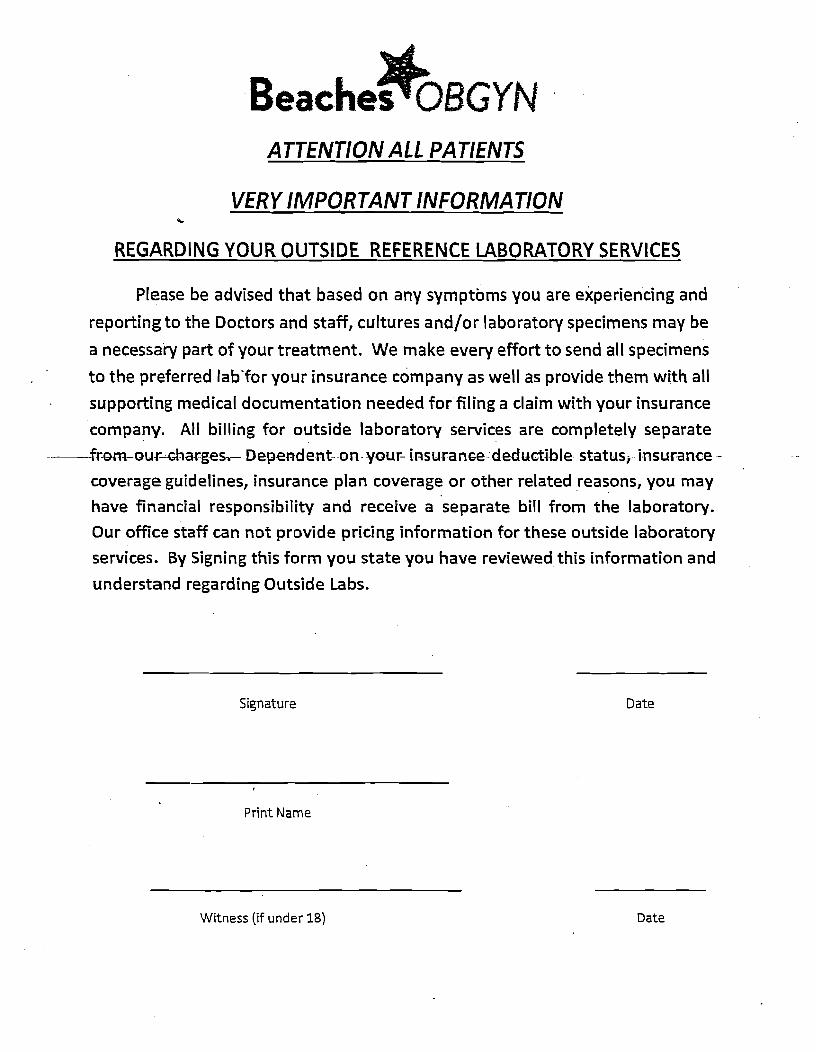
rQ- Beaches OBGYN ATTENTION ALL PATIENTS
VERY IMPORTANT INFORMATION
REGARDING YOUR OUTSIDE REFERENCE LABORATORY SERVICES
Please be advised that based on any symptoms you are experiencing and
reporting to the Doctors and staff, cultures and/or laboratory specimens may be
a necessary part of your treatment. We make every effort to send all specimens
to the preferred lab'for your insurance company as well as provide them with all
supporting medical documentation needed forf i l ing a claim with your insurance
company. All billing for outside laboratory services are completely separate
---fr-om-ourxha-rges,- Dependent--on- your- i~suranc-e- deductible statusj insurance -
coverage guidelines, insurance plan coverage or other related reasons, you may
have financial responsibility and receive a separate bill from the laboratory.
Our office staff can not provide pricing information for these outside laboratory
services. By Signing this form you state you have reviewed this information and
understand regarding Outside Labs.
Signature Date
Print Name
- - -
Witness (if under 18) Date
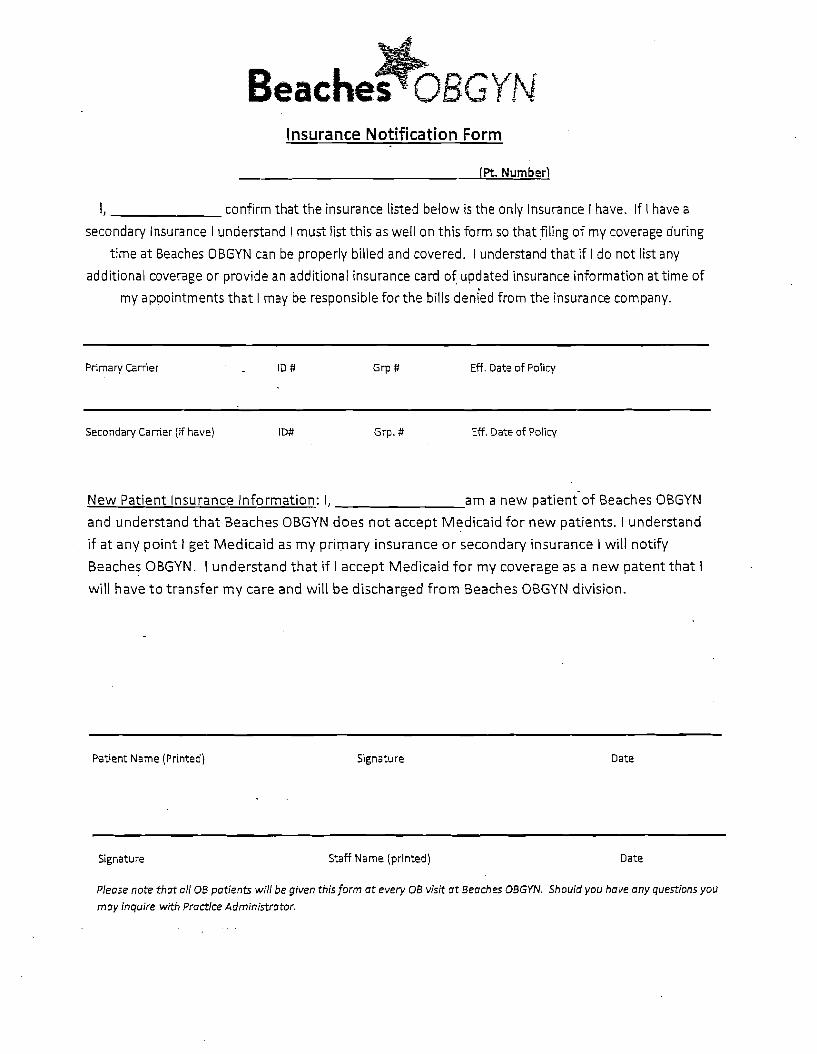
lnsurance Notification Form
(Pt. Number)
1, confirm tha t t h e insurance listed below is t h e only Insurance I have. If I have a
secondary lnsurance I understand I must list th is a s well o n th is form s o t h a t filing of my coverage during
t ime a t Beaches OBGYN can be properly billed and covered. I understand t h a t if I d o n o t list any
additional coverage o r provide an additional insurance card of updated insurance information a t t ime of
my appointments t h a t I may be responsible fo r t h e bills denied from t h e insurance company.
Primary Carrier ID # Grp # Eff. Date of Policy
-
Secondary Carrier (if have) ID# Grp. # Eff. Date of Policy
N e w P a t i e n t I n s u r a n c e Informat ion: I, a m a n e w pat ient 'of B e a c h e s OBGYN
a n d u n d e r s t a n d t h a t B e a c h e s OBGYN d o e s n o t a c c e p t M e d i c a i d f o r n e w pa t i en t s . I u n d e r s t a n d
if a t a n y p o i n t I g e t M e d i c a i d a s m y p r i m a r y i n s u r a n c e o r s e c o n d a r y i n s u r a n c e I will notify
B e a c h e s OBGYN. I u n d e r s t a n d t h a t if I a c c e p t M e d i c a i d f o r m y c o v e r a g e a s a n e w p a t e n t t h a t I
will h a v e t o t r a n s f e r m y c a r e a n d will b e d i s c h a r g e d f r o m B e a c h e s OBGYN division.
Patient Name (Printed) Signature Date
Signature Staff Name (printed) Date
Please note that all OB patients wil l be given this form a t every OB visit a t Beaches OBGYN. Should you have any questions y o ~ j
may inquire with Practice Administrator.





























