Embed Size (px)
Citation preview
Banned Drugs in SportDoes the International Olympic Committee (IOC) List Need Updating?
David R. MottramSchool of Pharmacy and Chemistry, Liverpool John Moores University, Liverpool, England
Abstract The International Olympic Committee (IOC) published the first list of dopingclasses in 1967. Since that time, there have been significant problems associatedwith doping control in sport. Sport is a high profile, internationally recognisedactivity. However, operational inconsistencies exist between countries and be-tween sports federations. Endogenous substances, such as testosterone, humangrowth hormone (hGH) and erythropoietin (Epo) present particular problems indetermining what constitutes ‘normal’ levels in athletes. In addition, there is noreliable method available for the detection of hGH and Epo through urine testing.Athletes continue to test positive for banned drugs that are available over-the-counter despite their having been taken inadvertently, without intent to enhanceperformance. Marijuana use is becoming widespread in society and the impactof this in sport is becoming evident.
Doping control, through the IOC list, must continue as a primary objective forthe IOC and the sports federations. Constant vigilance and a continued willing-ness to respond rapidly to change is a prerequisite for such a list. The IOC appearsto recognise this need. There are, however, more fundamental issues to be con-sidered. The concept of doping control must be supported by high quality re-search, effective education and international collaboration. More research isneeded into the factors which induce an athlete to take drugs and into the effect,if any, that education on drugs is having on competitors. The most important areafor change is the overriding need for international collaboration between the IOC,governments and sports federations. This applies to uniformity in the rules andregulations, consistency in the application and level of sanctions and cooperationon the dissemination of information and development of education policies.
CURRENT OPINION Sports Med 1999 Jan; 27 (1): 1-100112-1642/99/0001-0001/$05.00/0
© Adis International Limited. All rights reserved.
1. History of the International OlympicCommittee (IOC) List of Doping Classesand Methods
Although the use of substances to enhance per-formance is probably as old as sport itself, the in-crease in doping in sport parallels the pharmaco-logical revolution which began in the 1960s.[1]
By the late 1960s, despite the lack of data, sports’officials believed that drugs had the potential to
enhance performance and therefore introduceddrug testing on a wide scale.[2] The InternationalOlympic Committee (IOC) set up a Medical Com-mission, which published the first IOC list of dop-ing classes in 1967.[3]
Compulsory drug testing by the IOC was intro-duced in 1968 at the Winter Olympic Games inGrenoble, and then again in 1968 at the OlympicGames in Mexico. At that time, the IOC list in-cluded sympathomimetic amines, psychomotor

stimulants, miscellaneous CNS stimulants and nar-cotic analgesics. Anabolic steroids were suspectedof being used at that time[4] but were not listedbecause testing methods were insufficiently devel-oped. The list of banned substances remained thesame for the 1972 Olympic Games in Munich,where the first full-scale testing programme wasintroduced.[5]
Unofficial tests for androgenic anabolic steroidswere undertaken at the 1972 Games, with the firstofficial tests being conducted at the 1976 Gamesin Montreal. The first testing procedure for ana-bolic steroids was based on radioimmunoassay.[6]
This was followed by an assay based on gaschromatography-mass spectrometry,[7] used at theLos Angeles Olympic Games in 1984.[8] The cate-gory of doping methods was introduced to the IOClist after the 1984 Olympic Games. Diuretics andβ-blockers were added to the classes of dopingagents in 1985 and peptide hormones were in-cluded in 1989.[2]
The current IOC list (table I) reflects changesmade in 1993, which included the renaming of theandrogenic anabolic steroids class to anabolicagents, to incorporate nonsteroidal anabolic agentssuch as clenbuterol.
2. Prevalence of Drug Misuse in Sport
The prevalence of drug misuse in sport has beenvery difficult to determine. However, one indica-tion can be obtained by reviewing statistics fromthe 25 IOC accredited laboratories. In recent years,the percentage of positive drug test results fromthese laboratories has been between 1.0 and 2.5%per year.[9] However, IOC statistics have not nec-essarily been representative of the level of misuse,which is probably considerably higher.[9] It hasbeen noted that few countries have an IOC accred-ited laboratory and the mean number of samplesanalysed by each laboratory per week is about 80,a figure that contrasts sharply with the millions ofathletes who participate in sport each week.[10]
There have been many survey-based studies onthe prevalence of drug misuse in sport.[11] Oneepidemiological review[12] indicated that amongchildren, prevalence was about 3 to 5%; in adults,in self-reported use studies, prevalence was esti-mated at 5 to 15% and in projected use studies themean value was near 15 to 25%. However, preva-lence studies have tended to be highly selectivewith regard to their target population, concentratedon anabolic steroid use, and have failed to relatedrug misuse to individual sports.[11]
3. Problems Associated with DopingControl in Sport
3.1 Organisational Aspects
Sport is a high profile, internationally recog-nised activity. Many governments have seen inter-national sporting success as an important propa-ganda weapon.[13] The role of the former GermanDemocratic Republic in this context has been doc-umented.[14]
Inconsistencies have been found between coun-tries, where short-notice, out-of-competition test-ing with lifelong bans may apply in one country butnot another.[2] Similarly, there have been inconsis-tencies between sports federations in terms of theclarity of their rules for drug testing and sanc-tions,[15,16] the status of doping agents[17] and theapplication of threshold levels for determining a
Table I. Prohibited classes of substances and prohibited methodsas defined by the International Olympic Committee Medical Com-mission (at 31 January 1998)
I. Prohibited classes of substancesA. StimulantsB. NarcoticsC. Anabolic agentsD. DiureticsE. Peptide and glycoprotein hormones and analogues
II. Prohibited methodsA. Blood dopingB. Pharmacological, chemical and physical manipulation
III. Classes of drugs subject to certain restrictionsA. Alcohol (ethanol)B. MarijuanaC. Local anaestheticsD. CorticosteroidsE. β-Blockers
2 Mottram
© Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)
positive result.[18] Even the vagueness of the termi-nology used in doping control literature may leadto confusion in the athlete’s mind.[19]
In recent years, a number of high profile casesof athletes who have tested positive for bannedsubstances have highlighted some of the inconsis-tencies within the organisational framework. Typ-ical defences have included inadvertent use or lackof understanding that some over-the-counter (OTC)drugs contained a prohibited drug, or that the pos-itive result was attributable to a mistake in the col-lection of the sample, a break in the chain of cus-tody, a laboratory error or sabotage.[15] Althoughloopholes in the regulations have been exposed,their exposure has not always led to changes in theregulations, resulting in a lack of trust in or respectfor the system.[20]
It is clear that the role of the testing bodies iscritical. IOC rules apply only to the OlympicGames. Elsewhere, each international sports feder-ation or national governing body sets the rules.[15]
It would make sense for all governing bodies insport to operate under the same rules and regula-tions. This has yet to be achieved, although theIOC has set up a working group to unify the rulesand penalties against doping within Olympicsports.[21]
3.2 Testosterone
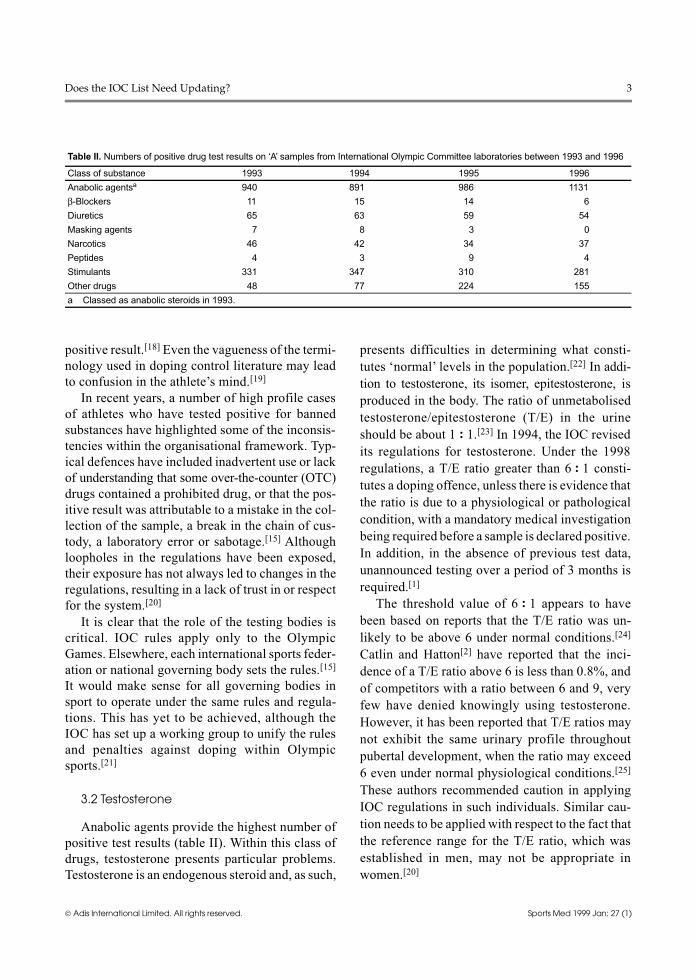
Anabolic agents provide the highest number ofpositive test results (table II). Within this class ofdrugs, testosterone presents particular problems.Testosterone is an endogenous steroid and, as such,
presents difficulties in determining what consti-tutes ‘normal’ levels in the population.[22] In addi-tion to testosterone, its isomer, epitestosterone, isproduced in the body. The ratio of unmetabolisedtestosterone/epitestosterone (T/E) in the urineshould be about 1 : 1.[23] In 1994, the IOC revisedits regulations for testosterone. Under the 1998regulations, a T/E ratio greater than 6 : 1 consti-tutes a doping offence, unless there is evidence thatthe ratio is due to a physiological or pathologicalcondition, with a mandatory medical investigationbeing required before a sample is declared positive.In addition, in the absence of previous test data,unannounced testing over a period of 3 months isrequired.[1]
The threshold value of 6 : 1 appears to havebeen based on reports that the T/E ratio was un-likely to be above 6 under normal conditions.[24]
Catlin and Hatton[2] have reported that the inci-dence of a T/E ratio above 6 is less than 0.8%, andof competitors with a ratio between 6 and 9, veryfew have denied knowingly using testosterone.However, it has been reported that T/E ratios maynot exhibit the same urinary profile throughoutpubertal development, when the ratio may exceed6 even under normal physiological conditions.[25]
These authors recommended caution in applyingIOC regulations in such individuals. Similar cau-tion needs to be applied with respect to the fact thatthe reference range for the T/E ratio, which wasestablished in men, may not be appropriate inwomen.[20]
Table II. Numbers of positive drug test results on ‘A’ samples from International Olympic Committee laboratories between 1993 and 1996
Class of substance 1993 1994 1995 1996Anabolic agentsa 940 891 986 1131β-Blockers 11 15 14 6Diuretics 65 63 59 54Masking agents 7 8 3 0Narcotics 46 42 34 37Peptides 4 3 9 4Stimulants 331 347 310 281Other drugs 48 77 224 155a Classed as anabolic steroids in 1993.
Does the IOC List Need Updating? 3
© Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

3.3 Peptide Hormones
The IOC introduced the doping class ‘Peptidehormones and analogues’ in 1989. This class in-cludes human chorionic gonadotrophin (hCG),adrenocorticotrophic hormone (ACTH), humangrowth hormone (hGH), all releasing factors forthese hormones and erythropoietin (Epo). Thereare strong indications that there is increasing useof hGH, because of its anabolic effect,[23] and ofEpo because of its ability to increase the oxygencarrying capacity of the blood through the increasein red blood cell production.[26] Evidence for theincreasing use of peptide hormones comes frominnumerable anecdotes from physicians and others,reports of thefts and forged prescriptions, enquiriesto drug hotlines and magazine articles.[2]
Athletes misuse peptide hormones because theybelieve that hGH can produce desired effects with-out the risk of the adverse effects associated withanabolic steroids and because there is no reliablemethod available for the detection of hGH throughurine testing.[27] In 1992, it was suggested thathighly specific immunoassays combined with suit-able purification techniques may be sufficient towarrant IOC approval as confirmatory tests forhGH.[28] However, an IOC-approved testing proce-dure is still being sought (see section 4).
3.4 Blood Doping
Blood boosting through legal altitude trainingor illegal blood doping is widely practiced by ath-letes. Blood doping involves transfusion of wholeblood or packed red blood cells and may be autol-ogous (the athlete’s own blood) or homologous(another person’s blood).[26] The IOC defines dop-ing as the use of physiological substances in abnor-mal amounts and via abnormal methods with theexclusive aim of attaining an artificial and unfairincrease of performance in competition. Hence, theIOC has included blood doping in its list of prohib-ited methods. Unfortunately, techniques to detectartificially-induced erythrocythaemia are difficultto apply, particularly where autologous transfusionis involved.[2] Even if tests were available, their
validity would be confounded by altitude acclim-atisation, hydration status and individual variationin normal haematocrit.[29] It is therefore likely thatthis manipulation is used by athletes, particularlyin endurance sports.[30]
3.5 Over-the-Counter Drugs
Banned drugs which are available over-the-counter (OTC) continue to cause concern for manyathletes.[31,32] Statistics, such as those of the UKSports Council results of testing for 1996/1997,[33]
show that half of the positive results for stimulantswere for OTC drugs. Furthermore, in half of thesecases no action was taken or a warning, rather thana suspension, was administered to the athlete in-volved. This indicates an acceptance by the author-ities of the fact that banned OTC drugs may havebeen taken without intent to enhance performance.
Drugs, such as ephedrine, are relatively less po-tent and lack selectivity compared with other stim-ulants; hence, they have been available withoutprescription.[34] This lack of selectivity, with theconcomitant likelihood of adverse effects, particu-larly if used in supratherapeutic doses, makes themless desirable as potential performance-enhancingdrugs, especially since no improvement in perfor-mance has been found in the few research studieson these drugs.[35,36]
Codeine is an OTC drug which was recently ‘de-classified’ by the IOC. Prior to 1993, codeine ac-counted for a large proportion of the positive testresults in the narcotic analgesic class.[1] Many‘guilty’ competitors claimed to be unaware thatthey had taken the drug. In March 1993, the IOCremoved codeine from the list and permitted its usefor therapeutic purposes. In September 1994, theIOC allowed 2 further narcotic analgesics,dihydrocodeine and dextromethorphan, for thera-peutic use. However, not all researchers agree thatcodeine should have been declassified.[18]
3.6 Drug Treatment of Asthma
Asthma may be triggered by a number of fac-tors, not least of which is exercise.[34] Drug treat-ment for asthma is complex and may involve a
4 Mottram
© Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

number of drugs which variably act as prophylacticagents to prevent an asthma attack or as broncho-dilators to relieve the symptoms of an attack. Twoof the main groups of anti-asthma drugs are corti-costeroids and β2-adrenoceptor agonists. Bothgroups of drugs are subject to IOC doping controlregulations. Indeed, the β2-adrenoceptor agonistsare classed as both stimulants and as anabolicagents. The IOC regulations compound the prob-lem for the athlete in that, in the case of the β2-adrenoceptor agonists, certain drugs are allowed(salbutamol, terbutaline and salmeterol) while oth-ers are banned, and the only allowable route ofadministration is by inhalation. Corticosteroids arepermitted for approved medical conditions but re-stricted by their route of administration. In allcases, a declaration as to the use of these drugsmust be made prior to competition.
It is not surprising that athletes and their physi-cians need to be especially vigilant in the selectionof an appropriate therapeutic drug regime.[17] It hasbeen reported that, in some sports, an inordinatelylarge number of declarations for the use of anti-asthma drugs are submitted compared with the in-cidence of asthma in the community.[15]
3.7 Recreational Drugs
‘Recreational’ drugs encompass a diverse groupof pharmacological agents which are banned undervarious headings on the IOC list. These includecocaine and amphetamines (stimulants), heroin(narcotic analgesic) and alcohol (ethanol) and mar-ijuana (drugs subject to certain restrictions). It hasbeen suggested that the use of recreational drugs ismore prevalent amongst professional athletes thanin the general population, because athletes can af-ford them.[37] However, there is little evidence thatsuch substances give unfair advantage to the user,and there is no reason to think that a desire to winmotivates abuse.[37]
The few studies on cocaine and exercise suggestthat little or no improvement in performance is pro-duced. Indeed, the sense of euphoria may providethe illusion of a better performance than was actu-ally achieved.[35] The behavioural effects of
cocaine may have consequences for fellow com-petitors, especially where aggressive instincts havebeen altered.[38]
Marijuana use is becoming widespread insociety and the effect of this in sport is becomingevident (see section 5.4). Events surrounding thedisqualification and subsequent reinstatement ofRoss Rebagliati, following a positive test for mar-ijuana at the Winter Olympic Games at Nagano inFebruary 1998, serves to highlight another prob-lem associated with banning recreational drugs insport. There appeared to have been no formalagreement between the International Ski Federa-tion and the IOC regarding testing for marijuana atthe Games, an organisational problem alreadyhighlighted in section 3.1.
4. Developments in Drug Testing
In the past, the methods for effective testing forsome drugs, particularly anabolic steroids, havelagged behind their use in sport. There has been amarked increase in the volume of published re-search on drug misuse in sport since the 1988Olympic Games in Seoul, most notably in the areaof drug testing.[39] The main objective of recentresearch has been to develop improved testingmethods for anabolic steroids, particularly testos-terone and peptide hormones.
Androgenic anabolic steroids are tested in IOClaboratories by a method involving gas chromatog-raphy linked to mass spectrometry. This providesa relatively sensitive method of analysis, capableof detecting urinary steroid concentrations of aslittle as 10 μg/L in a 2 to 5ml sample.[9] Confirma-tory analysis uses full-scan mass spectrometry. Atthe 1996 Olympic Games in Atlanta, high resolu-tion mass spectrometry was used, providing addi-tional selectivity and improving detectability byapproximately 10-fold.[9]
As described in section 3.2, the endogenous ste-roid testosterone has created significant problemswith regard to doping control. IOC regulations forthe detection of testosterone use depend on theanalysis of the T/E ratio of urine. A method fordistinguishing between a testosterone user and an
Does the IOC List Need Updating? 5
© Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

outlier from the biological norm, based on therequirement of a competitor taking the drug keto-conazole, has been described.[40,41] However, thismethod has not been adopted by the IOC, possiblybecause of the ethical consideration of requiring acompetitor to take a drug for which there is no ther-apeutic indication. More recent approaches fortesting for testosterone use have investigated theratio of 12C : 13C, on the basis that synthetic tes-tosterone has a higher proportion of 13C than en-dogenous human testosterone,[42,43] and the use ofelectrospray mass spectrometry for detecting tes-tosterone esters.[44] Clearly, the concomitant use byathletes of epitestosterone with testosterone cancomplicate the testing procedures;[45,46] however, amethod for analysis of urinary markers of oral tes-tosterone in the presence of masking epitestos-terone is being developed.[47] It is interesting tonote the development of inter-laboratory collabor-ations in the area of research into the control oftestosterone doping.[48]
Particular attention is being paid to researchinto hGH. A multicentre research project, entitledGH2000, was established in 1996. This project hasbeen financed through joint funding from theEuropean Union, the IOC and the pharmaceuticalindustry. The main objectives of the project havebeen to define the limits of acceptable physiologi-cal ranges for hGH in the population as a whole andin elite athletes, and to establish an acceptable test-ing procedure for the 2000 Olympic Games in Syd-ney. Prior to the GH2000 project, a test to detecthGH in urine, based on an enzyme-linked immuno-sorbent assay, had been developed.[49] This test wasonly applied in out-of-competition situations. Amore recent study described insulin-like growthfactors being used as markers of doping withhGH;[50] however, testing for these markers re-quired blood sampling. Similarly, the detection ofEpo using urine and blood samples has been underinvestigation.[30,51] There have been, however, ser-ious concerns about the use of blood sampling indoping control.[52] As an alternative, the use of hairsamples, which are not subject to degradation and
can reveal a historical record of drug exposure overa period of months, has been investigated.[53]
5. Does the IOC List Need Updating?
5.1 Do We Need an IOC List?
The IOC states that its IOC Medical Code isintended to safeguard the health of athletes and en-sure respect for the ethical concepts implicit in ‘fairplay’, the ‘Olympic spirit’ and medical practice.[54]
The health of athletes is clearly at risk due to thewell documented adverse reactions associated withtaking drugs, often in doses far in excess of thoserecommended for therapeutic use. However, re-ports of adverse effects associated with doping insport are often anecdotal and circumstantial. Thereported incidence of acute life-threatening eventsassociated with anabolic steroid abuse is low, butthe actual risk may be underrecognised or under-reported.[55] The adoption of double-blind control-led trials, along the lines of those employed by thepharmaceutical industry, would provide a muchclearer picture of the effectiveness, if any, and tox-icity of potential performance-enhancing drugs.Unfortunately, the ethical hurdles associated withsuch trials would be insurmountable. The recorded,but previously unreported, incidence of the damag-ing adverse effects of anabolic steroids adminis-tered the German Democratic Republic’s dopingprogramme provides evidence in support of theIOC objective to safeguard the health of ath-letes.[14]
The ethical basis for testing for performanceenhancing drugs in sport has been questioned onthe grounds of the infringement of an individual’sliberty and the impossibility of distinguishing be-tween acceptable technologies of performance en-hancement by improved training and equipmentand unacceptable technologies of drug use.[15,37]
A counter-argument can be proposed by consid-ering the infringement of the liberty of fellowcompetitors subjected to the potential adverse re-actions induced by pharmacologically modifiedbehaviour.
6 Mottram
© Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

5.2 Is it Time for a Radical Change?
Millar[56] perceives the need for a new approachto anabolic steroid use in sport. He has argued thatathletes rely on unscientific literature, publishedby uncritical writers and concluded that the medi-cal management of anabolic steroid use would pro-vide the best answer to the problem by reducingthe potential for harm due to its use. This view isechoed elsewhere.[57] Bird and Wagner[58] statethat the current regulatory approach to doping con-trol relies entirely on centralised bureaucraticmethods and is ineffective. Their preferred ap-proach proposes the use of drug diaries to encour-age honest rather than secret drug use and a colleg-iate enforcement system for drug diaries. Theyargue that these systems would encourage anti-doping norms that may be powerful enough toeliminate improper drug use.
The introduction of such radical changes couldbe contemplated only after considerable debate onthe likelihood of success for such schemes and onthe consequences resulting from failure.
5.3 Should the IOC List be Expanded toInclude Nutritional Supplements?
In an attempt to enhance performance throughergogenic aids, without contravening IOC regula-tions, many athletes have used nutritional supple-ments. Unlike drugs, nutritional supplements arenot required to have strong scientific and clinicalevidence that they are effective before being al-lowed to be marketed.[59] This encourages the man-ufacturers to make claims that their products haveergogenic properties.[60] There is little, if any, evi-dence that nutritional supplements possess ergo-genic properties in athletes consuming a balanceddiet. Moreover, some products have the potentialfor harm.[60] Studies in which diet was manipulatedto induce metabolic acidosis, by reducing carbohy-drate intake or increasing fat and protein intake,have resulted in impaired performance.[61]
Creatine has been the subject of many studies,but whether it is capable of producing ergogeniceffects is equivocal.[59,62] From research evidence,
the IOC’s decision to include caffeine on its list ofbanned substances would appear to be correct.[59]
The IOC regulations concerning caffeine specify alimit on how much may be consumed prior to com-petition. Williams[63] has asked if the same type ofreasoning should apply to nutrients or derived by-products that are shown to be ergogenic.
In the absence of convincing evidence for ergo-genic properties of nutritional supplements, theirinclusion in the IOC list would serve no useful pur-pose.
5.4 Do the IOC Regulations Need Refining?
The regulations on doping control in sport re-quire frequent review to take into account the ever-changing strategies adopted by athletes intent ondoping and the continuing advances in research.
Table II shows the number of positive drug testsfrom IOC-accredited laboratories in recent years.As discussed in section 2, these statistics do notnecessarily reflect the true prevalence of drug mis-use in sport but provide an indication as to wherethe problems may lie; however, these data requiresome comment.
Positive test results for the drug classes of nar-cotics, β-blockers and diuretics occur infrequently.Since the testing methods for these drugs are welldeveloped, it would seem reasonable to concludethat these rates of detection reflect a low incidenceof use. With respect to narcotic analgesics, most ofthe positive test results recorded were for dextro-propoxyphene, which under current IOC regula-tions is permitted.
About 60 to 65% of the positive test results forstimulants involve OTC drugs. Action taken bysports federations in such cases often involves areprimand rather than a sanction. The IOC has re-cently attempted to clarify their regulations con-cerning these OTC drugs by introducing thresholdlimits (5 mg/L urine for ephedrine, cathine andmethylephedrine; 10 mg/L urine for phenylpro-panolamine and pseudoephedrine). In the future,the argument to deregulate all OTC drugs may pre-vail.
Does the IOC List Need Updating? 7
© Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

Positive test results for peptide hormones rarelyoccur but these low rates of detection are mislead-ing because of the absence of an IOC-approvedmethod for identification. Anabolic agents areclearly the most frequently detected drugs and thisundoubtedly confirms that these drugs are, by far,the most widely misused in sport.
The most significant trend evident in table II isthat for ‘Other drugs’, where the number of posi-tive results increased dramatically between 1994and 1996. Virtually all of the positive tests for‘Other drugs’ involved marijuana. To what extentthis drug is being used for performance enhance-ment is difficult to ascertain, but the potentialknock-on effect of its use on other competitorsshould not be underestimated.
In response to these trends, the IOC has tendedto be reactive rather than proactive. In 1993, thedoping class of ‘anabolic steroids’ was changed to‘anabolic agents’ to encompass the increasing useof β2-adrenoceptor agonists, such as clenbuterolwhich although they are nonsteroidal, produce an-abolic effects. Codeine and a number of other nar-cotic analgesics have been removed from thebanned list, on the basis of their marginal benefitin sports performance and the potential for theirinadvertent use. Regulations regarding T/E ratioswere changed in 1994. Most recently, the IOC havespecified threshold limits for OTC sympathomi-metics, in recognition of the fact that athletes mayhave taken these substances unknowingly by self-medication for minor ailments. It has been sug-gested, however, that these threshold concentra-tions may be too low.[36]
More controversial still, peptide hormones andblood doping have been included in the IOC listdespite there being no conclusive, urine-based testto confirm the use of these substances and methods.Many research groups are investigating blood test-ing as a means for a more accurate method fordetecting misuse of endogenous substances; how-ever, recent research has highlighted the limita-tions of blood sampling.[64,65] Moreover, the inva-sive nature of blood sampling and the associatedpractical, medical, ethical, legal and moral difficul-
ties lead some to question the validity of such atechnique.[52,66] It is unlikely that blood testing willbe introduced by the IOC in the near future.
Clearly, the IOC recognises the need for the con-tinual refinement of its regulations and has shownthat it is prepared to remove, as well as add, drugsto the IOC list. The latest problem is the associationbetween the use of marijuana and sport; and a num-ber of questions need to be answered.• Can marijuana be considered to be performance-
enhancing?• Is recreational drug use more prevalent in ath-
letes?• What are the consequences for fellow competi-
tors?• Are threshold concentrations the answer?These issues require urgent review by the IOC.
6. Conclusions
Doping control, through the IOC list, must con-tinue to be a primary objective for the IOC and thesports federations. Constant vigilance and a contin-ued willingness to respond rapidly to change areprerequisites for such a list. There are, however,more fundamental issues to be considered. Theconcept of doping control must be supported byhigh quality research, effective education and in-ternational collaboration.
It is encouraging to note that research into drugmisuse in sport has increased significantly sincethe Seoul Olympic Games and that this researchhas focused on the problem areas, at least in termsof drug testing.[39] Moreover, collaboration on re-search by laboratories is taking place.[48,67] What islacking is research into the factors which induce anathlete to take drugs and into the effect, if any, thateducation on drugs is having on competitors. Theneed for quality education has been identified as ahigh priority by all sectors in sport, from adminis-trators to elite athletes.[39] Educational messagesaimed at abstinence alone have not been success-ful[68] and messages should therefore be based onmotivating athletes not to abuse drugs.[19] Educa-tion concerning drug misuse in sport should ex-tend beyond internationally regulated competitive
8 Mottram
© Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)
sports and into recreational sports, where testingand sanctions do not apply.[52] There is a contin-uum between recreational and internationally reg-ulated sport, with recreational sport providing theinitial training ground for elite competitors who, inturn, become role models for those competing atthe recreational level.[52]
The most important area for change is the over-riding need for international collaboration betweenthe IOC, governments and sports federations. Thisapplies to developing uniformity in the rules andregulations regarding drug testing, consistency inthe application and level of sanctions and cooper-ation on the dissemination of information and de-velopment of education policies. Clearly, suchmeasures require significant funding but, as Bow-ers has observed,[69] ‘Given the amount of finan-cial resources invested in sport, the athletes (andfans) have the right to competition decided byinnate ability and hard work not by potentiallydangerous pharmacological intervention’.
References1. Verroken M, Mottram DR. Doping control in sport. In: Mottram
DR, editor. Drugs in sport. London: E & FN Spon, 1996;235-63
2. Catlin DH, Hatton CK. Use and abuse of anabolic and otherdrugs for athletic enhancement. Adv Intern Med 1991; 36:399-424
3. Beckett AH, Cowan DA. Misuse of drugs in sport. Br J SportsMed 1979; 12: 185-94
4. Wade N. Anabolic steroids: doctors denounce them, but athletesaren’t listening. Science 1972; 176: 1399-403
5. de Merode A. Doping tests at the Olympic Games in 1976. JSports Med 1979; 19: 91-6
6. Brooks RV, Firth RG, Sumner NA. Detection of anabolic ster-oids by radioimmunoassay. Br J Sports Med 1975; 9: 89-92
7. Ward JL, Shackleton CHL, Lawson AM. Gas chromatographic-mass spectrometric methods for the detection and identifica-tion of anabolic steroid drugs. Br J Sports Med 1975; 9: 93-7
8. Catlin DH, Kammerer RC, Hatton CK, et al. Analytical chem-istry at the games of the XXIIIrd Olympiad in Los Angeles.Clin Chem 1984; 33: 319-27
9. Cowan DA. Testing for drug abuse. In: Reilly T, Orme M, edi-tors. Esteve Foundation Symposium. Vol. 7. The clinicalpharmacology of sport and exercise. Amsterdam: ExcerptaMedica, 1997: 13-23
10. Benzi G. Pharmacoepidemiology of the drugs used in sports asdoping agents. Pharmacol Res 1994; 29: 13-26
11. Mottram DR, Reilly T, Chester N. Doping in sport: the extentof the problem. In: Reilly T, Orme M, editors. Esteve Foun-dation Symposium. Vol. 7. The clinical pharmacology ofsport and exercise. Amsterdam: Excerpta Medica, 1997: 3-12
12. Laure P. Epidemiologic approach of doping in sport. J SportsMed Phys Fitness 1997; 37: 218-24
13. Waddington I. The development of sports medicine. SociolSport J 1996; 13: 176-96
14. Franke WW, Berendonk B. Hormonal doping and androgeniza-tion of athletes: a secret program of the German DemocraticRepublic government. Clin Chem 1997; 43: 1262-79
15. Catlin DH, Murray TH. Performance-enhancing drugs, faircompetition, and Olympic sport. JAMA 1996; 276: 231-7
16. Ng TL. Dope testing in sports: scientific and medico-legalissues. Ann Acad Med Singapore 1993; 22: 48-53
17. Frumkin LR, Price JM. The International Olympic Committeeand doping status of antiasthma drugs. Pediatr Asthma AllergyImmunol 1996; 2: 41-6
18. Delbeke FT. Doping in cyclism: results of unannounced con-trols in Flanders (1987-1994). Int J Sports Med 1996; 17:434-8
19. Uzych L. Drug testing of athletes. Br J Addiction 1991; 86:25-31
20. Honour J. Steroid abuse in female athletes. Curr Opin ObstetGynecol 1997; 9: 181-6
21. Anon. Major breakthrough in the fight against doping. OlympicReview 1993: 309/10: 298-300
22. Yesalis C. Anabolic steroids in sport and exercise. Champaign(IL): Human Kinetics Inc., 1993
23. George A. The anabolic steroids and peptide hormones. In:Mottram DR, editor. Drugs in sport. London: E & FN Spon,1996: 173-218
24. Chan SC. Doping control of anabolic steroids. J Forensic SciSoc 1991; 31: 217-20
25. Raynaud E, Audran M, Pages JC, et al. Determination of urinarytestosterone and epitestosterone during pubertal develop-ment: a cross-sectional study in 141 normal male subjects.Clin Endocrinol 1993; 38: 353-9
26. Armstrong DJ, Reilly T. Blood boosting in sport. In: MottramDR, editor. Drugs in sport. London: E & FN Spon, 1996:219-34
27. Wadler GI. Drug use update. Med Clin North Am 1994; 78:439-55
28. Kicman AT, Cowan DA. Peptide hormones and sport: misuseand detection. Br Med Bull 1992; 48: 496-517
29. Anon. American College of Sports Medicine position on blooddoping as an ergogenic aid. Med Sci Sport Exerc 1987; 19:540-3
30. Ekblom B. Blood doping, erythropoietin and altitude. In: ReillyT, Orme M, editors. Esteve Foundation Symposium. Vol. 7.The clinical pharmacology of sport and exercise. Amsterdam:Excerpta Medica, 1997: 199-212
31. Radford P. Drug testing and drug education programs. SciencePeriodical on Research and Technology in Sport 1992; 12:1-5
32. UK Sports Council. Doping control in the UK: survey of theexperiences and views of elite competitors. London: UKSports Council, 1995
33. UK Sports Council. Ethics and Anti-Doping Directorate annualreport 1996/97. London: UK Sports Council, 1997
34. Armstrong DJ. Sympathomimetic amines and their antagonists.In: Mottram DR, editor. Drugs in sport. London: E & FN Spon,1996: 56-85
35. Clarkson PM, Thompson HS. Drugs and sport: research find-ings and limitations. Sports Med 1997; 24: 366-84
36. Swain RA, Harsha DM, Baenziger J, et al. Do pseudoephedrineor phenylpropanolamine improve maximum oxygen uptakeand time to exhaustion? Clin J Sports Med 1997; 7: 168-73
37. Fost N. Banning drugs in sports: a skeptical view. Hastings CentRep 1986; 16: 5-10
38. Voy R. Drugs, sport and politics. Champagne (IL): Human Kin-etics Inc., 1993
Does the IOC List Need Updating? 9
© Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

39. Reilly T, Mottram DR, Chester N, et al. Review of research intodrug misuse in sport. London: UK Sports Council, 1996
40. Kicman AT, Oftebro H, Walker C, et al. Potential use of keto-conazole in a dynamic endocrine test to differentiate betweenbiological outliers and testosterone use by athletes. Clin Chem1993; 39: 1798-803
41. Oftebro H, Jensen J, Mowinckel P, et al. Establishing a ketocon-azole suppression test for verifying testosterone administra-tion in the doping control of athletes. J Clin Endocrinol Metab1994; 78: 973-7
42. Becchi M, Aguilera R, Farizon Y, et al. Gas chromatogra-phy/combustion/isotope ratio mass spectrometry analysis ofurinary steroids to detect misuse of testosterone in sport.Rapid Commun Mass Spectrom 1994; 8: 304-8
43. Anguilera R, Becchi M, Casabianca H, et al. Improved methodof detection of testosterone abuse by gas chromatogra-phy/combustion/isotope ratio mass spectrometry analysis ofurinary steroids. J Mass Spectrom 1996; 31: 169-76
44. Shackleton CHL, Chuang H, Kim J, et al. Electrospray massspectrometry of testosterone esters: potential for use in dopingcontrol. Steroids 1997; 62: 523-9
45. Kicman AT, Brooks RV, Collyer SC, et al. Criteria to indicatetestosterone administration. Br J Sports Med 1990; 24: 253-64
46. Catlin DH, Hatton CK, Starcevic SH. Issues in detecting abuseof xenobiotic anabolic steroids and testosterone by analysisof athletes’ urine. Clin Chem 1997; 43: 1280-8
47. Dehennin L, Peres G. Plasma and urinary markers of oral tes-tosterone misuse by healthy men in presence of maskingepitestosterone administration. Int J Sports Med 1996; 17:315-9
48. Catlin DH, Cowan DA, de laTorre R, et al. Urinary testosterone(T) to epitestosterone (E) ratios by GC/MS: 1. initial compar-ison of uncorrected T/E in 6 international laboratories. J MassSpectrom 1996; 31: 397-402
49. Saugy M, Cardis C, Schweizer C, et al. Detection of humangrowth hormone doping in urine: out of competition tests arenecessary. J Chromatogr B 1996; 687: 201-11
50. Kicman AT, Miell JP, Teale JD, et al. Serum IGF-I and IGFbinding proteins 2 and 3 as potential markers of doping withhuman GH. Clin Endocrinol 1997; 47: 43-50
51. Gareau R, Brisson GR, Chenard C, et al. Total fibrin and fibrin-ogen degradation products in urine: a possible probe to detectillicit users of the physical-performance enhancer erythropoi-etin? Horm Res 1995; 44: 189-92
52. Hoppeler HH, Matthias MF, Melia PS. Doping and preventionof doping: international cooperation. Clin J Sports Med 1995;5: 79-81
53. Polettini A, Montagna M, Segura J, et al. Determination of β2-agonists in hair by gas chromatography/mass spectrometry. JMass Spectrom 1996; 31: 47-54
54. IOC Medical Code. Lausanne: International Olympic Commit-tee, 1995
55. Wu FCW. Endocrine aspects of anabolic steroids. Clin Chem1997; 43: 1289-92
56. Millar AP. Licit steroid use – hope for the future. Br J SportsMed 1994; 28: 79-83
57. Black T, Pape A. The ban on drugs in sports: the solution or theproblem? J Sport Soc Iss 1997; 21: 83-92
58. Bird EJ, Wagner GG. Sport as a common property resource: asolution to the dilemmas of doping. J Conflict Resolut 1997;41: 749-66
59. Clarkson PM. Nutrition for improved sports performance: cur-rent issues on ergogenic aids. Sports Med 1996; 21: 393-401
60. Beltz SD, Doering PL. Efficacy of nutritional supplements usedby athletes. Clin Pharm 1993; 12: 900-8
61. MacLaren DPM. Alkalinizers: influence of blood acid-basestatus on performance. In: Reilly T, Orme M, editors. EsteveFoundation Symposium. Vol. 7. The clinical pharmacology ofsport and exercise. Amsterdam: Excerpta Medica, 1997: 157-65
62. Balsom PD. Creatine supplementation in humans. In: Reilly T,Orme M, editors. Esteve Foundation Symposium. Vol. 7. Theclinical pharmacology of sport and exercise. Amsterdam: Ex-cerpta Medica, 1997: 167-77
63. Williams MH. The use of nutritional ergogenic aids in sport: isit an ethical issue? Int J Sport Nutr 1994; 4: 120-31
64. Souillard A, Audran M, Bressolle F, et al. Pharmacokinetics andpharmacodynamics of recombinant human erythropoietin inathletes: blood sampling and doping control. Br J Clin Phar-macol 1996; 42: 355-64
65. Birkeland KI, Donike M, Ljungqvist A, et al. Blood samplingin doping control: first experiences from regular testing inathletes. Int J Sports Med 1997; 18: 8-12
66. Council of Europe, Anti-Doping Convention, Monitoring Group.4th Meeting; 1993 Jun 15-17. Strasbourg: Council of Europe,1993 Jun 25: Meeting report [doc. T-DO (93) 12]
67. Bruunshuus I, Klempel K, Cowan D, et al. Transmission of theresults of tests for International Olympic Committee-defineddrugs of abuse. J Chromatogr B 1996; 687: 157-82
68. Littlepage BNC, Perry HM. Misusing anabolic drugs: possibil-ities for future policies. Addiction 1993; 88: 1469-71
69. Bowers LD. Analytical advances in detection of performance-enhancing compounds. Clin Chem 1997; 43: 1299-304
Correspondence and reprints: Dr David R. Mottram, Schoolof Pharmacy and Chemistry, Liverpool John Moores Uni-versity, Byrom Street, Liverpool L3 3AF, England.E-mail: [email protected]
10 Mottram
© Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)





























