Embed Size (px)
Citation preview

Transplant Immunology 28 (2013) 193–197
Contents lists available at SciVerse ScienceDirect
Transplant Immunology
j ourna l homepage: www.e lsev ie r .com/ locate / t r im
Balance of pro- and anti-inflammatory cytokines in cirrhoticpatients undergoing liver transplantation☆
Gianni Biancofiore a,⁎, Lucia Bindi a, Mario Miccoli b, Maria R. Metelli c, Erica Panicucci c,Angelo Baggiani b, Franco Filipponi d
a Liver Transplant Anaesthesia and Critical Care Medicine, Azienda Ospedaliera Universitaria Pisana, Pisa, Italyb Epidemiology and Biostatistics Unit, Department of Experimental Pathology, University School of Medicine, Pisa, Italyc Department of Laboratory Medicine, University School of Medicine, Pisa, Italyd Liver Transplant Surgery, University School of Medicine, Pisa, Italy
☆ No grants and other financial support were used to⁎ Corresponding author at: Liver Transplant Anaesthe
Azienda Ospedaliera Universitaria Pisana; Ospedale Cisan050995409; fax: +39 050996984.
E-mail address: [email protected] (G. Bianc
0966-3274/$ – see front matter © 2013 Elsevier B.V. Allhttp://dx.doi.org/10.1016/j.trim.2013.04.001
a b s t r a c t
a r t i c l e i n f oArticle history:Received 25 December 2012Received in revised form 7 April 2013Accepted 8 April 2013
Keywords:Transplantation, liverInflammation mediatorCytokineCirrhosis, liver
This study was prospectively aimed at having better information about the natural history of serum cytokinesin cirrhotic patients undergoing liver transplant surgery and at assessing their ability to set up an appropriatedynamic relationship between pro-inflammation and anti-inflammation. The levels of six cytokines (TNF-α,IL-1, IL-2, IL-6, IL-8, IL-10) were measured in blood samples collected at different time points before, duringand after (48 h) the transplant procedure from the radial artery of 62 consecutive cirrhotic patients whounderwent orthotopic liver transplantation.IL-1 always stayed within the normal range; IL-2 showed elevated baseline levels but decreased up to half atthe end of the study (p b 0.0001). IL-6 peaked at the end of surgery and returned to baseline 48 h afterwards.The same happened to IL-8 concentrations. IL-10 levels shown above the normal threshold at baseline, peakedat the end of surgery (p b 0.0001) and were halved at the end of the study (p b 0.0001). TNF-α peaked at theend of surgerywithout, however, being different from baseline levels (p = 0.6). The physiologic pattern of cy-tokine release and their dynamic relationship was found to be preserved with a quick return to a balance be-tween pro-inflammation and anti-inflammation as shown by the IL-6/IL-10 and TNF-α/IL10 ratios (used toassess the inflammatory balance). A correlation was found between perioperative pro-inflammatory cytokinelevels and the severity of the liver disease necessitating OLT. In summary, cirrhotic patients can achieve a bal-anced inflammatory response to surgery which is considered a primary requirement for uneventful grafts andpatients' postoperative recovery.
© 2013 Elsevier B.V. All rights reserved.
1. Introduction
Cytokines are a group of endogenous proteins which play a pivotalrole in regulating the inflammatory response to surgery through a pre-dictable set of adaptive events. This process, which is designed to maxi-mize the organism's healing potential, is initiated locally, at the site ofsurgical trauma, by macrophages and monocytes that release pro-inflammatory cytokines. In particular, tumour necrosis factor alpha(TNF-a) and interleukin-1 (IL-1) initiate a cascade of mediators whichare directly responsible for the various events associatedwith inflamma-tion [1–6]. The increase in the circulating blood of pro-inflammatorycytokines triggers immune cells to release anti-inflammatory cytokines(e.g., IL-10) with the aim of downregulating, through complex feedback
perform this research.sia and Critical Care Medicine,ello; 56100 Pisa, Italy. Tel.: +39
ofiore).
rights reserved.
mechanisms, the pro-inflammatory process so to maintain homeostasis[1–6]. From the clinical point of view, the role of circulating inflam-matory cytokines is not much clear yet. They might serve as biomarkersfor certain clinical events, such as infections (i.e., IL6 in sepsis) or inflam-mation [7]. In addition, they might serve as marker for metabolicchanges or stress [3–5]. It has been also reported that pre-existingchronic diseases can interact with the patients' capability to set up a bal-anced inflammatory response to surgery which, therefore, may result inbeing exaggerated (leading to hyper-inflammation) or inadequate(leading to immunosuppression) possibly causing compromised out-comes and organ dysfunction [2,3,7,8]. In particular, it has been shownthat liver cirrhosis leads to an over-expression of various pro- andanti-inflammatory cytokines resulting in a significant derangement ofthe whole inflammatory response [9–12]. Therefore, we designed astudy to obtain better information about the natural history of serum cy-tokines in cirrhotic patients undergoing liver transplantation with theaim of assessing if they are still capable to set up an appropriate physio-logic relationship between pro-inflammation and anti-inflammationleading to a balanced response to surgery trauma.

194 G. Biancofiore et al. / Transplant Immunology 28 (2013) 193–197
2. Materials and methods
This study involved all of the patients who underwent orthotopicliver transplantation (OLT) at our Centre during 9 consecutive monthswho gave their informed consent. Anaesthetic and intraoperative man-agement were the same in all cases as previously described [13].According to the standard protocol at our Centre, a centrifugal pump-driven veno-venous extracorporeal by-pass with heparinised tubingwas placed to drain the infra-diaphragmatic venous circulation intothe superior vena cava to allow better haemodynamic stability duringthe anhepatic phase. All of the transplant procedures were performedby the same surgeon. Routine postoperative medications included anti-biotics (Cefuroxim 1 g 3 times/day for 2 days) and Morphine. The im-munosuppressive protocol included oral cyclosporin A (SandimmunNeoral®, Novartis Pharma S.A., Huningue, France) at a dose of15 mg/day on the day of surgery, subsequently titrated to maintainblood trough levels of 200–250 ng dL; intravenous Basiliximab(Simulect®, Novartis Pharma S.A., Huningue, France) 20 mg in postop-erative days 1 and 4; oral mycophenolate mophetil (Cellcept®, RochePharma S.A., Milan, Italy) at a dose of 1 g twice a day and methylpred-nisolone (Solu-Medrol®, Pharmacia & Upjohn, Puurs, Belgium) at anintra-operative dose of 10 mg/kg subsequently reduced by 50% perday to a prednisolone dose of 20 mg/day. Patientswith HCV-related cir-rhosis did not receive steroids. Liver transplant recipients were classi-fied according to the Model for End Stage Lived Disease (MELD).MELD is a scoring system assessing the severity of chronic liver diseasethat was found to be useful in determining prognosis and for prioritiz-ing allocation of liver transplants [14].
2.1. Study protocol
The levels of six cytokines (TNF-α, IL-1, IL-2, IL-6, IL-8, IL-10) weremeasured in blood samples collected from the radial artery of the stud-ied patients at the following time points: T0 (2 h before surgery), T1(before the start of the veno-venous bypass), T2 (immediately beforethe by-pass was discontinued), T3 (15 min after graft's reperfusion),
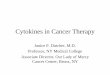
Fig. 1. Cytokine changes in the study population. 0: T0 (2 h before surgery). 1: T1 (befodiscontinued). 3: T3 (15 min after graft's reperfusion). 4: T4 (30 min after ICU admissionICU admission). *** = p b 0.0001 vs baseline (ANOVA).
T4 (30 min after ICU admission), T5 (12 h from ICU admission), T6(24 h from ICU admission), and T7 (48 from ICU admission).
2.2. Laboratory techniques
Blood sampleswere collected in tubes kept in ice, centrifuged at 0 °Cand the plasma was stored at −70 °C until assayed. Measurements ofcytokines were performed quantitatively by an enzyme-linked immu-nosorbent assay kit (ELISA, Bender MedSystems GmbH, Vienna,Austria).
2.3. Statistical analysis
Values are presented as mean ± standard deviation. Pro- vs. anti-inflammatory balance was assessed by calculating IL-6/IL-10 andTNF-α/IL10 ratios at each time point. During the preliminary phasewe performed the Shapiro–Wilk test and the Hartley test to verifynormality and homoscedasticity of distributions.
Subsequently we used ANOVA with Bonferroni's correction tocompare variable values at each time. We calculated the Pearson's co-efficient (with specific p-values) to study the correlations between ILpeak concentrations and AST/ALT levels and to analyse the correla-tions between IL peak concentrations and INR. We performed statisti-cal power analysis (ex post) to estimate the sample sizes used for thestatistical tests. The 1-β values of the significant variables were >0.8,assuring a low risk of type II error and appropriate sample sizes. Thelevel of significance was 0.05 and the analysis was carried out usingthe SPSS software (version 12.0, SPSS Inc., Chicago, USA).
3. Results
Data from 62 of the 67 enrolled patients were analysed (47 males, 15 females). Fivepatients were excluded because theywere transplanted for liver cancerwithout cirrhosis.Our patients' age was 51.7 ± 8.6 years (range 26–64) and BMI was 24.7 ± 2.2 kg m2.The underlying diseases necessitating liver transplantationwere 59 cases of liver cirrhosis(45 viral, 10 alcoholic and 4 cryptogenic) and three of primary biliary cirrhosis. TheMELDscore of the study population was 19 ± 6.
re the start of the veno-venous bypass). 2: T2 (immediately before the bypass was). 5: T5 (12 h from ICU admission). 6: T6 (24 h from ICU admission). 7: T7 (48 from
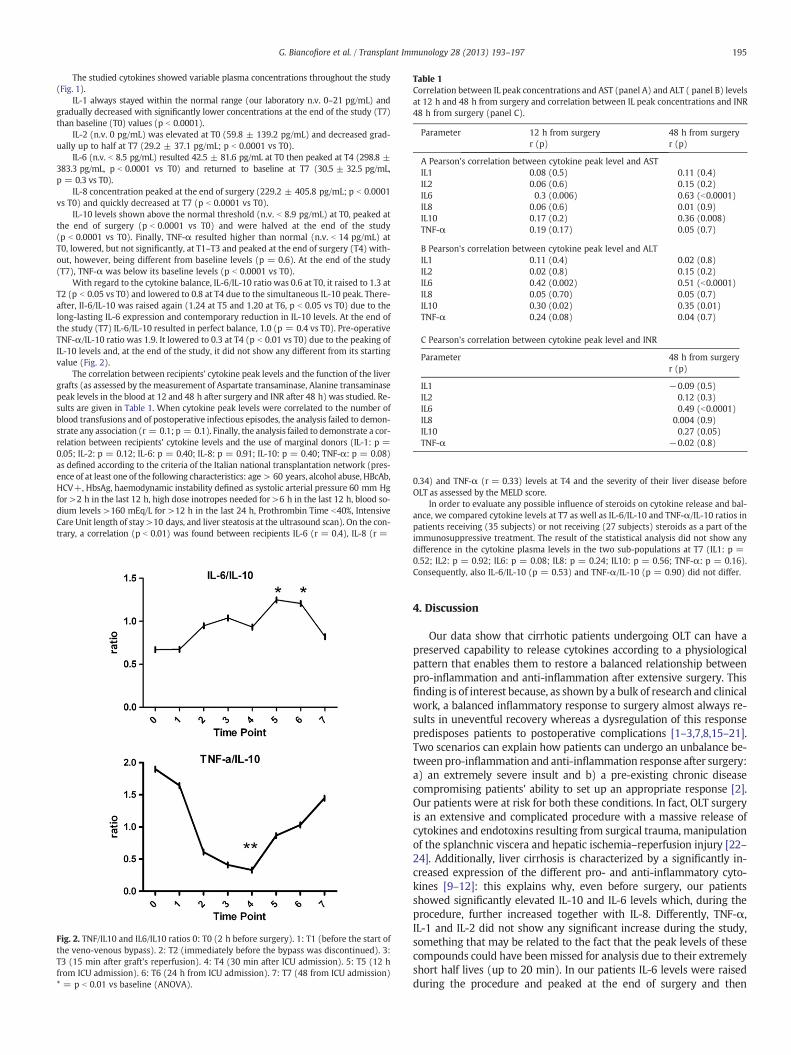
Table 1Correlation between IL peak concentrations and AST (panel A) and ALT ( panel B) levelsat 12 h and 48 h from surgery and correlation between IL peak concentrations and INR48 h from surgery (panel C).
Parameter 12 h from surgeryr (p)
48 h from surgeryr (p)
A Pearson's correlation between cytokine peak level and ASTIL1 0.08 (0.5) 0.11 (0.4)IL2 0.06 (0.6) 0.15 (0.2)IL6 0.3 (0.006) 0.63 (b0.0001)IL8 0.06 (0.6) 0.01 (0.9)IL10 0.17 (0.2) 0.36 (0.008)TNF-α 0.19 (0.17) 0.05 (0.7)
B Pearson's correlation between cytokine peak level and ALTIL1 0.11 (0.4) 0.02 (0.8)IL2 0.02 (0.8) 0.15 (0.2)IL6 0.42 (0.002) 0.51 (b0.0001)IL8 0.05 (0.70) 0.05 (0.7)IL10 0.30 (0.02) 0.35 (0.01)TNF-α 0.24 (0.08) 0.04 (0.7)
C Pearson's correlation between cytokine peak level and INR
Parameter 48 h from surgeryr (p)
IL1 −0.09 (0.5)IL2 0.12 (0.3)IL6 0.49 (b0.0001)IL8 0.004 (0.9)IL10 0.27 (0.05)TNF-α −0.02 (0.8)
195G. Biancofiore et al. / Transplant Immunology 28 (2013) 193–197
The studied cytokines showed variable plasma concentrations throughout the study(Fig. 1).
IL-1 always stayed within the normal range (our laboratory n.v. 0–21 pg/mL) andgradually decreased with significantly lower concentrations at the end of the study (T7)than baseline (T0) values (p b 0.0001).
IL-2 (n.v. 0 pg/mL) was elevated at T0 (59.8 ± 139.2 pg/mL) and decreased grad-ually up to half at T7 (29.2 ± 37.1 pg/mL; p b 0.0001 vs T0).
IL-6 (n.v. b 8.5 pg/mL) resulted 42.5 ± 81.6 pg/mL at T0 then peaked at T4 (298.8 ±383.3 pg/mL, p b 0.0001 vs T0) and returned to baseline at T7 (30.5 ± 32.5 pg/mL,p = 0.3 vs T0).
IL-8 concentration peaked at the end of surgery (229.2 ± 405.8 pg/mL; p b 0.0001vs T0) and quickly decreased at T7 (p b 0.0001 vs T0).
IL-10 levels shown above the normal threshold (n.v. b 8.9 pg/mL) at T0, peaked atthe end of surgery (p b 0.0001 vs T0) and were halved at the end of the study(p b 0.0001 vs T0). Finally, TNF-α resulted higher than normal (n.v. b 14 pg/mL) atT0, lowered, but not significantly, at T1–T3 and peaked at the end of surgery (T4) with-out, however, being different from baseline levels (p = 0.6). At the end of the study(T7), TNF-α was below its baseline levels (p b 0.0001 vs T0).
With regard to the cytokine balance, IL-6/IL-10 ratio was 0.6 at T0, it raised to 1.3 atT2 (p b 0.05 vs T0) and lowered to 0.8 at T4 due to the simultaneous IL-10 peak. There-after, Il-6/IL-10 was raised again (1.24 at T5 and 1.20 at T6, p b 0.05 vs T0) due to thelong-lasting IL-6 expression and contemporary reduction in IL-10 levels. At the end ofthe study (T7) IL-6/IL-10 resulted in perfect balance, 1.0 (p = 0.4 vs T0). Pre-operativeTNF-α/IL-10 ratio was 1.9. It lowered to 0.3 at T4 (p b 0.01 vs T0) due to the peaking ofIL-10 levels and, at the end of the study, it did not show any different from its startingvalue (Fig. 2).
The correlation between recipients' cytokine peak levels and the function of the livergrafts (as assessed by the measurement of Aspartate transaminase, Alanine transaminasepeak levels in the blood at 12 and 48 h after surgery and INR after 48 h) was studied. Re-sults are given in Table 1. When cytokine peak levels were correlated to the number ofblood transfusions and of postoperative infectious episodes, the analysis failed to demon-strate any association (r = 0.1; p = 0.1). Finally, the analysis failed to demonstrate a cor-relation between recipients' cytokine levels and the use of marginal donors (IL-1: p =0.05; IL-2: p = 0.12; IL-6: p = 0.40; IL-8: p = 0.91; IL-10: p = 0.40; TNF-α: p = 0.08)as defined according to the criteria of the Italian national transplantation network (pres-ence of at least one of the following characteristics: age > 60 years, alcohol abuse, HBcAb,HCV+, HbsAg, haemodynamic instability defined as systolic arterial pressure 60 mm Hgfor >2 h in the last 12 h, high dose inotropes needed for >6 h in the last 12 h, blood so-dium levels >160 mEq/L for >12 h in the last 24 h, Prothrombin Time b40%, IntensiveCare Unit length of stay >10 days, and liver steatosis at the ultrasound scan). On the con-trary, a correlation (p b 0.01) was found between recipients IL-6 (r = 0.4), IL-8 (r =
Fig. 2. TNF/IL10 and IL6/IL10 ratios 0: T0 (2 h before surgery). 1: T1 (before the start ofthe veno-venous bypass). 2: T2 (immediately before the bypass was discontinued). 3:T3 (15 min after graft's reperfusion). 4: T4 (30 min after ICU admission). 5: T5 (12 hfrom ICU admission). 6: T6 (24 h from ICU admission). 7: T7 (48 from ICU admission)* = p b 0.01 vs baseline (ANOVA).
0.34) and TNF-α (r = 0.33) levels at T4 and the severity of their liver disease beforeOLT as assessed by the MELD score.
In order to evaluate any possible influence of steroids on cytokine release and bal-ance, we compared cytokine levels at T7 as well as IL-6/IL-10 and TNF-α/IL-10 ratios inpatients receiving (35 subjects) or not receiving (27 subjects) steroids as a part of theimmunosuppressive treatment. The result of the statistical analysis did not show anydifference in the cytokine plasma levels in the two sub-populations at T7 (IL1: p =0.52; IL2: p = 0.92; IL6: p = 0.08; IL8: p = 0.24; IL10: p = 0.56; TNF-α: p = 0.16).Consequently, also IL-6/IL-10 (p = 0.53) and TNF-α/IL-10 (p = 0.90) did not differ.
4. Discussion
Our data show that cirrhotic patients undergoing OLT can have apreserved capability to release cytokines according to a physiologicalpattern that enables them to restore a balanced relationship betweenpro-inflammation and anti-inflammation after extensive surgery. Thisfinding is of interest because, as shown by a bulk of research and clinicalwork, a balanced inflammatory response to surgery almost always re-sults in uneventful recovery whereas a dysregulation of this responsepredisposes patients to postoperative complications [1–3,7,8,15–21].Two scenarios can explain how patients can undergo an unbalance be-tween pro-inflammation and anti-inflammation response after surgery:a) an extremely severe insult and b) a pre-existing chronic diseasecompromising patients' ability to set up an appropriate response [2].Our patients were at risk for both these conditions. In fact, OLT surgeryis an extensive and complicated procedure with a massive release ofcytokines and endotoxins resulting from surgical trauma, manipulationof the splanchnic viscera and hepatic ischemia–reperfusion injury [22–24]. Additionally, liver cirrhosis is characterized by a significantly in-creased expression of the different pro- and anti-inflammatory cyto-kines [9–12]: this explains why, even before surgery, our patientsshowed significantly elevated IL-10 and IL-6 levels which, during theprocedure, further increased together with IL-8. Differently, TNF-α,IL-1 and IL-2 did not show any significant increase during the study,something that may be related to the fact that the peak levels of thesecompounds could have been missed for analysis due to their extremelyshort half lives (up to 20 min). In our patients IL-6 levels were raisedduring the procedure and peaked at the end of surgery and then

196 G. Biancofiore et al. / Transplant Immunology 28 (2013) 193–197
decreased during the postoperative course. This pattern of IL-6 dependson surgical trauma and its extent. In fact, it has been shown that IL-6 el-evation after major abdominal surgery is greater than after minor sur-gery and that its levels after laparoscopic procedures are lower thanafter open procedures [8,23].
Our data clarify for the first time that cirrhotic patients, despite theinflammatory over-expression characterizing them, can show a pre-served capability to manage the inflammatory response to surgeryaccording to a physiological relationship between IL-6 and IL-10where the rise of IL-6 triggers a counterbalancing elevation of IL-10which, in turn, reduces the stimulation for the release of IL-6 whoselevels quickly return to baseline thus reducing the triggering forIL-10 (Fig. 1). The result of this dynamic relationship is a balancedIL-6/IL-10 ratio, something fundamental for an appropriate immuneresponse to surgery [1–3,7,8,15–24]. Indeed, cytokine balance canbe assessed also by means of the TNF-α/IL-10 ratio which, in our ex-perience, was mostly influenced by the changes of IL-10 concentra-tions because TNF-α did not show relevant changes. However, it hasbeen highlighted that the IL-6/IL-10 ratio assesses better the inflam-matory balance status after surgery whereas the TNFα/IL-10 ratio ismore reliable in septic patients [8,20,21].
There is evidence indicating that a shift toward inflammation is asso-ciated to liver dysfunction after hepatic resection and transplantation.Boros et al. [25] found that IL-1, IL 6, and IL-8 concentrations in the he-patic vein at the time of reperfusion were higher in patients who suf-fered poor postoperative graft function, and Hassan et al. [26] reportedthat plasma concentrations of IL-6 and IL-10 might be useful as predic-tive indicators for postoperative complications in liver transplant recip-ients. Finally, Mueller et al. [27] also reported that several cytokinessecreted during liver transplantation, including IL-2, were correlatedwith postoperative graft function. The proposedmechanism is excessivesecretion of cytokines promoting graft inflammation and resulting in aloss of graft function [27]. Moreover, the inability to quickly reach an ef-fective balance between pro-inflammation and anti-inflammation candetermine severe postoperative complications like infections and respi-ratory failure [28–31]. In our experience, pro- and anti-inflammationafter OLT surgery were quickly balanced. This finding can explain whywe did not find any correlation between cytokine peak levels, earlypostoperative complications and function of the liver grafts. This samereason could explain the lack of correlation that we found betweenthe use of marginal donors and the inflammatory response to surgery.On the contrary, our data confirm a correlation between perioperativepro-inflammatory cytokine levels and the severity of the liver diseasenecessitatingOLT as assessed by theMELD scorewhich could be accord-ingly considered an interesting tool for predicting the severity of thesystemic inflammatory reaction in this class of patients [32,33].
According to our data, exposing patients to the artificial surfaces ofthe veno-venous extracorporeal circulation did not further activatecytokine release. On the other hand, as the veno-venous by-pass decom-presses the splanchnic venous circulation and reduces intestinaloedema, its use may result in a decreased stress and inflammation ofthe viscera. In fact, a significant correlation was found between portalclamping, a condition that increases visceral venous pressure, and the in-crease of IL-6 in patients undergoing liver resection surgery and OLTwithout the use of the bypass [34–37]. From this point of view, ourdata might imply a possible benefit of the bypass in restraining theintraoperative proinflammatory burst. Finally, in our patients the admin-istration of cortisone as a part of the immunosuppressive therapy did notchange their inflammatory pattern nor affected the cytokine balance byshifting it, for example, towards over-immunosuppression. However,this finding needs to the confirmed in a more numerous population.
One limitation to our study is represented by the fact that humansare not equal in terms of inflammatory responses. This is due to the ge-netic polymorphisms for many pro- and anti-inflammatory cytokinesassociated with the amplitude of the inflammatory response [38,39].Additionally, another polymorphism exists in terms of target cell
reactivity in response to cytokine signalling [40]. This individual hetero-geneity has to be considered when addressing the inflammatory re-sponse. Another limitation to draw universal conclusions is thelimited number of the enrolled patients. Nevertheless, it must be con-sidered that our population is themost numerous studied so farwith re-gard to OLT surgery [25–40]. It should be also considered that anotherstrength of our study lies in the well-defined blood sampling initiatedbefore surgery and in the cohort of consecutive OLT patients treatedaccording to the same standard of care.
In conclusion, before surgery, cirrhotic patients are characterized byan over-expression of both pro- and anti-inflammatory cytokines. Ex-tensive OLT surgery induces a cytokine response characterized by a sig-nificant and transient elevation of IL-6, IL-8 and IL-10 but, differentlyfrom sepsis, not of IL-1 and TNF-α. Cirrhotic patients can achieve a bal-anced inflammatory response to surgery which is considered a primaryrequirement for uneventful grafts and patients' postoperative recovery.The predictive value of the IL-6/IL-10 ratio for postoperative orgraft's-related complications still needs to be determined. In futurestudies an increasing attention should be turned towards the conceptof cytokine balance rather than cytokine absolute plasma concentrations.
References
[1] Dinarello CA. Proinflammatory cytokines. Chest 2000;118:503–8.[2] Lin E, Calvano SE, Lowry SF. Inflammatory cytokines and cell response in surgery.
Surgery 2000;127:117–26.[3] Ni Choileain N, Redmond HP. Cell response to surgery. Arch Surg 2006;141:
1132–40.[4] Khol BA, Deutschman CS. The inflammatory response to surgery. Curr Opin Crit
Care 2006;12:325–32.[5] Asimakopoulos G. Mechanics of the systemic inflammatory response. Perfusion
1999;14:169–277.[6] Nystrom PO. The systemic inflammatory response syndrome: definitions and
aetiology. J Antimicrob Chemother 1998;41(Suppl. A):1–7.[7] Dimipoulu I, Armaganidis A, Douka E, Mavrou I, Augustatou C, Kopterides P, et al.
Tumor necrosis facto-alpha (TNF-α) and interleukin-10 are crucial mediators inpost-operative systemic inflammatory response and determine the occurrenceof complications after major abdominal surgery. Cytokine 2007;37:55–61.
[8] Menger MD, Vollmar B. Surgical trauma: hyperinflammation versus immunosup-pression? Langenbecks Arch Surg 2004;389:475–84.
[9] Tilg H, Diehl AM. Mechanisms of diseases: cytokines in alcoholic and non alcoholicsteatohepatitis. Lancet 2000;343:1467–76.
[10] Tang J, Fang J, GuWQ, Li EL. T cell immune response is correlated with fibrosis andinflammatory activity in hepatitis B cirrhotics. World J Gastroenterol 2006;12:3015–9.
[11] Naveau S, Balian A, Capron F, Raynard B, Fallik D, Agostini H, et al. Balancebetween pro and anti inflammatory cytokines in patients with acute alcoholichepatitis. Gastroenterol Clin Biol 2005;29:269–74.
[12] Fainboim L, Chernavsky A, Paladino N, Flores AC, Arruvito L. Cytokines and chronicliver disease. Cytokine Growth Factor Rev 2007;18:143–57.
[13] Biancofiore G, Critchley LA, Lee A, Bindi L, Bisà M, Esposito M, et al. Evaluation of anuncalibrated arterial pulse contour cardiac output monitoring system in cirrhoticpatients undergoing liver surgery. Br J Anaesth 2009;102:47–54.
[14] Kamath PS, Kim WR. The model for end-stage liver disease (MELD). Hepatology2007;45:797–805.
[15] Cavaillon JM. PRO- versus ANTI-inflammatory cytokines: myth or reality. Cell MolBiol 2001;47:695–702.
[16] Mokart D, Capo C, Blache JL, Delpero JR, Houvenaeghel G, Martin C, Mege JL. Earlypostoperative compensatory anti-inflammatory response syndrome is associatedwith septic complications after major surgical trauma in patients with cancer. Br JSurg 2002;89:1450–6.
[17] Stensballe J, Christiansen M, Tonnesen E, Espersen K, Lippert FK, Rasmussen LS.The early IL-6 and IL-10 response in trauma is correlated with injury severityand mortality. Acta Anaesthesiol Scand 2009;53:515–21.
[18] Zhao X, Koshiba T, Fujimoto Y, Pirenne J, Yoshizawa A, Ito T, et al. Proinflammatoryand antiinflammatory cytokine during ischemia–reperfusion injury in a case ofidentical twin living donor liver transplantation using no immunosuppression.Transplant Proc 2005;37:392–4.
[19] Taniguchi T, Koido Y, Aiboshi J, Yamashita T, Suzaki S, Kurokawa A, et al. Change inthe ratio of interleukin-6 to interleukin-10 predicts a poor outcome in patientswith systemic inflammatory response syndrome. Crit Care Med 1999;27:1262-124.
[20] van Dissel JT, van Langevelde P, Westendorp RG, Kwappenberg K, Frolich M.Anti-inflammatory cytokine profile and mortality in febrile patients. Lancet1998;351:950–3.
[21] Gogos CA, Drosou E, Bassaris HP, Skoutelis A. Pro- versus anti-inflammatory cyto-kine profile in patients with severe sepsis: a marker for prognosis and future ther-apeutic options. J Infect Dis 2000;181:176–80.
[22] Frangogiannis NK. Chemokines in ischemia and reperfusion. Thromb Haemost2007;97:738–47.

197G. Biancofiore et al. / Transplant Immunology 28 (2013) 193–197
[23] Helmy SA, Wahby MA, El-Nawaway M. The effect of anaesthesia and surgery onplasma cytokine production. Anaesthesia 1999;54:733–8.
[24] Kimura F, Shimizu H, Yoshidome H, Ohtsuka M, Kato A, Yoshitomi H, et al. Circu-lating cytokines, chemokines, and stress hormones are increased in patients withorgan dysfunction following liver resection. J Surg Res 2006;133:102–12.
[25] Boros P, Suehiro T, Curtiss S, Sheiner P, Emre S, Guy S, Schwartz ME, Miller CM.Differential contribution of graft and recipient to perioperative TNF-α, IL-1β,IL-6 and IL-8 levels and correlation with early graft function in clinical liver trans-plantation. Clin Transplant 1997;11:588–92.
[26] Hassan L, Bueno P, Ferrón-Celma I, Ramia JM, Garrote D, Muffak K, et al. Earlypostoperative response of cytokines in liver transplant recipients. TransplantProc 2006;38:2488–91.
[27] Mueller AR, Platz KP, Haak M, Undi H, Müller C, Köttgen E, Weidemann H,Neuhaus P. The release of cytokines, adhesion molecules, and extracellular matrixparameters during and after reperfusion in human liver transplantation. Trans-plantation 1996;62:1118–26.
[28] Lee KW, Son TS, Joh JW, Kim SJ, Park JH, Chon SE, et al. Perioperative cytokine re-sponse after liver transplantation. Transplant Proc 2003;35:407–8.
[29] Sautner T, Függer R, Götzinger P, Mittlböck M, Winkler S, Roth E, Steininger R,et al. Tumour necrosis factor-alpha and interleukin-6: early indicators of bacterialinfection after human orthotopic liver transplantation. Eur J Surg 1995;161:97–101.
[30] Wen X, Kong H, Zhu S, Xu J, Huang S, Chen Q. Plasma levels of tumor necroticfactor-alfa and interleukin-6,-8 during orthotopic liver transplantation and theirrelations to postoperative pulmonary complications. Hepatobiliary Pancreat DisInt 2004;3:38–41.
[31] Duran JA, González AA, García DD, Falcón RC, Pereda PS, Alvárez SM. Variation inthe levels of inflammatory cytokines depending on ischemic time: effects on re-spiratory variables. Transplant Proc 2009;41:980–2.
[32] Koh HJ, Ryu KH, Cho ML, Heo YJ, Lee J. Factors influencing the concentration ofcytokines during liver transplantation. Transplant Proc 2010;42:3617–9.
[33] Hong SH, Kim JE, Cho ML, Heo YJ, Choi JH, Choi JH, et al. Comparison of the Child–Turcotte–Pugh classification and the model for end-stage liver disease score aspredictors of the severity of the systemic inflammatory response in patients un-dergoing living-donor liver transplantation. J Korean Med Sci 2011;26:1333–8.
[34] Studzinski A, Scheinichen D, Stenger K, Weissig A, Becker T, Juettner B. The role ofportal vein clamping for cytokine release and neutrophils activity during liver re-section and transplant. Exp Clin Transplant 2008;6:254–60.
[35] Faybik P, Hetz H, Krenn CG, Baker A, Baker A, Berlakovich GA, Steltzer H. Periop-erative cytokine during orthotopic liver transplantation without venovenous by-pass. Transplant Proc 2003;35:3019–21.
[36] Baía CE, Abdala E, Massarollo P, Beduschi T, Palma TM, Mies S. Inflammatory cyto-kines during liver transplantation: prospective randomized trial comparing con-ventional and piggyback techniques. Hepatogastroenterology 2009;56:1445–51.
[37] Bezinover D, Kadry Z, McCullough P, McQuillan PM, Uemura T, Welker K, et al. Re-lease of cytokines and hemodynamic instability during the reperfusion of a livergraft. Liver Transpl 2011;17:324–30.
[38] Turner DM,WilliamsDM, SankaranD, LazarusM, Sinnott PJ, Hutchinson IV. An inves-tigation of polymorphism in the interleukin-10 gene promoter. Eur J Immunogenet1997;24:1–8.
[39] Danis VA, Millington M, Hyland VJ, Grennan D. Cytokine production by normalhuman monocytes: inter-subject variation and relationship to an IL-1 receptorantagonist (IL-1Ra) gene polymorphism. Clin Exp Immunol 1995;99:303–10.
[40] Pociot F, Briant L, Jongeneel CV, Mölvig J, Worsaae H, Abbal M, et al. Association oftumor necrosis factor (TNF) and class II major histocompatibility complex alleleswith the secretion of TNF and TNF-a by human mononuclear cells: a possible linkto insulin dependent diabetes mellitus. Eur J Immunol 1993;23:224–31.