Embed Size (px)
Citation preview

Autogenous breast reconstruction with the deep inferior
epigastric perforator flap
James E. Craigie, MDa,*, Robert J. Allen, MDb, Frank J. DellaCroce, MDb,Scott K. Sullivan, MDb
aEast Cooper Plastic Surgery, 1300 Hospital Drive, Suite 120, Mt. Pleasant, SC 29464, USAbDivision of Plastic Surgery, LSU Health Sciences Center, 4429 Clara Street, Suite 440, New Orleans, LA 70115, USA
The perfect method for breast reconstruction
would be safe, reliable, reproducible, applicable to
all patients, and have no donor site morbidity. The
ideal reconstructed breast would provide symmetric,
permanent, and natural results. The pursuit of these
goals has fueled the development and refinement of
autogenous methods of breast reconstruction. In
1976, Fugino et al [1] described the gluteus maximus
myocutaneous flap for breast reconstruction. This
was followed in 1979 by Holmstrom’s [2] use of
the rectus abdominus myocutaneous free flap, and in
the early 1980s, Hartrampf et al [3,4] popularized the
pedicled transverse rectus abdominus flap (TRAM).
The TRAM flap remains the most popular method
of autogenous reconstruction. This popularity is due to
the relative ease with which the procedure is per-
formed and the fact that no microsurgical expertise is
required. Proponents also argue that the pedicled
TRAM is quicker to perform, and, thus, saves oper-
ative time and expense; this has not been borne out in
the literature [4]. The pedicled TRAMhas proven to be
a basically reliable method of reconstruction but the
rate of partial flap necrosis may approach 25% [5].
This can be a problemwhen open wounds cause delays
in chemotherapeutic protocols, and, later, when the
differentiation of fat necrosis from a recurrent tumor is
required. The high rate of partial flap necrosis is the
result of a basic anatomic problem with the flap, which
requires reversal of flow through intramuscular choke
vessels into the inferior vasculature. This, combined
with folding and tunneling of the pedicle at its pivot
point, can compromise vascular exchange within the
flap. Tunneling may also affect the medial breast
contour [6]. The free TRAM flap has been used in an
effort to increase flap perfusion but it suffers from the
same limitation of rectus muscle sacrifice. When
patients with rectus sacrifice are compared with those
in which it is preserved, the importance of this con-
sideration is clear.
The deep inferior epigastric arttery perforator
(DIEP) flap for breast reconstruction was innovated
to improve the donor site morbidity that is associated
with the TRAM flap [7]. Patients who are recon-
structed with the DIEP flap experience substantially
less postoperative pain than those who are subjected
to muscle sacrifice (TRAM) [8]. Muscle sacrifice in
pedicle flaps is also responsible for abdominal asym-
metries, hernias, pain, and impaired ability to perform
daily, occupational, and sporting activities. Kroll et al
[9] and Mizgala et al [10] reported that abdominal
wall morbidity was significant and proportional to the
amount of muscle that was removed after TRAM flap
breast reconstruction. The ‘‘muscle sparing’’ free
TRAM is considered less morbid to the abdominal
wall. Some studies indicated, however, that the integ-
rity of the remaining rectus muscle is lost if a small
portion is removed with the flap [11–13]. Weakness
and atrophy of the remaining muscle occur when the
insertion is sacrificed and the quality of the abdom-
inal wall after the free TRAM has been described as
comparable to a pedicle TRAM donor site [14].
0094-1298/03/$ – see front matter D 2003 Elsevier Inc. All rights reserved.
doi:10.1016/S0094-1298(03)00037-3
* Corresponding author.
E-mail address: [email protected]
(J.E. Craigie).
Clin Plastic Surg 30 (2003) 359–369

The inherent advantage of muscle preservation
depends on maintaining the biomechanical stability
and balance of the trunk musculature. The rectus
abdominus is a keystone in the body’s ‘‘powerhouse’’
that enables balanced movement, heavy lifting, and
upright work against external resistance while main-
taining posture and healthy alignment of the spine.
This important point becomes apparent when one
considers the three physiologic types of muscle
activity and how they relate to the role of the rectus
abdominus in abdominal wall function. Isometric
static tension and eccentric lengthening are the two
most important physiologic activities of the rectus
abdominus and directly affect physical capacity. The
integrity of these components maintains biomechan-
ical stability and was shown to be intact after DIEP
flaps; the integrity is significantly impaired when
even a portion of the muscle is removed during free
TRAM flaps [15,16]. The third physiologic muscle
activity, which occurs during a sit-up, is less impor-
tant clinically and involves muscle shortening during
concentric muscle contraction. If concentric contrac-
tion has been weakened secondary to intramuscular
scar formation, then the intact internal oblique
muscles can easily compensate and minimize the
clinical impact. Closure of a defect in the rectus
fascia, however, causes a shift in the contralateral
rectus muscle toward the midline and alters the
mechanical advantage of the internal oblique
muscles. Therefore, the inherent donor site advantage
of the DIEP flap over other flaps that contain even a
small portion of muscle, is related to maintaining the
most important components of muscle activity and
avoiding the additional distortion of the abdominal
wall that occurs when a muscle and fascia defect must
be repaired. Minimizing the impairment of the
abdominal wall results in lower rates of donor site
asymmetries, donor site pain, back pain, hernias,
weakness, and functional impairments. These advan-
tages are exponentially accentuated when bilateral
reconstructions are performed.
The efforts to minimize donor site morbidity and
maximize aesthetic quality helped to usher in the next
generation of autogenous breast reconstructive tech-
niques. In 1989, Koshima and Soeda [17] pioneered
the transfer of abdominal fat and skin without muscle
sacrifice. In 1992, Allen and Treece [7] developed the
DIEP flap for breast reconstruction, based on the
premise that the inclusion of muscle in a flap that is
designed to replace fat and skin is unnecessary. The
muscle-sparing techniques that were used to develop
the DIEP flap have been applied to other donor sites.
Perforator flaps and arterialized skin flaps, including
the deep inferior epigastric artery perforator flap, the
superior gluteal artery perforator flap, and the super-
ficial inferior epigastric artery flap, have moved the
state of the art closer to the ‘‘ideal’’ breast recon-
structive technique [18,19].
Surgical technique
The DIEP flap uses the lower abdomen as a donor
site, as does the TRAM flap. The essential difference
is that the DIEP is based on perforating vessels that
emerge through the rectus sheath from the deep
inferior epigastric vessels. These vessels are followed
through the sheath down to the main feeders and,
therefore, the pedicle is much increased in length.
Preoperative markings are applied while the
patient is in the supine and standing position. Flap
dimensions are marked out in a manner similar to
abdominoplasty planning (Fig. 1). An effort to
Fig. 1. Preoperative markings for a bilateral reconstruction.
Two patterns are demonstrated; the upper design is placed to
safely capture the paraumbilical perforators. Alternatively,
a more aesthetic lower pattern can be used when the
superficial system is used or with beveling in a superior
direction when the DIEP is used.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369360

include para-umbilical perforators, which are often
dominant, may require shifting of the marked region
slightly superiorly. Alternatively, a more aesthetically
pleasing, lower incision can be used if subcutaneous
beveling in a superior direction is performed (Fig. 2).
A vertical dimension that is greater than 12 cm is
rarely necessary. Horizontal extensions are fashioned
in an effort to limit lateral ‘‘dog ears.’’ The Doppler
probe is used to identify the main perforators of the
medial and lateral branches of the deep inferior
Fig. 2. (A) This demonstrates the more aesthetically oriented, lower donor site incision with beveling in a superior direction during
DIEP flap harvest. (B) This demonstrates the level of undermining in the superior direction to capture the paraumbilical perforators.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369 361

epigastric artery. On the chest, the inframammary
crease is outlined. With immediate reconstruction,
suggested markings are made for a skin-sparing
mastectomy to include the nipple-areola complex
and biopsy site. A radial extension may be required
to improve access, especially with an axillary dissec-
tion. When a contralateral reduction is planned, the
skin-sparing mastectomy can be performed through a
breast reduction incision to improve symmetry.
The patient is positioned in a supine position with
the arms tucked by her sides. A two-team surgical
approach is used, with simultaneous preparation of the
recipient area and flap harvest. The internal mammary
vessels (IMVs) at the level of the third rib are the
preferred recipients. The advantages of the IMVs over
the thoracodorsal vessels, include ease of positioning
for themicrosurgical assistant, better exposure through
a limited skin sparing incision, and increased liberty
with flap inset [20]. In our experience, preoperative
radiation of the internal mammary vessels has not been
a problem. Radiated vessels are usually more tedious
to dissect but there has not been any increased evi-
dence of postoperative complications compared with
patients who have not undergone radiation.
Flap dissection proceeds with careful elevation of
the skin-fat composite from the underlying rectus
fascia until the lateral perforators are encountered
(Fig. 3). If a large perforator is located, the flap can
be based on this alone or with one or two other lateral
perforating vessels. If no suitable perforators are
identified in the lateral row, the dissection continues
over to the medial row of perforating vessels. The
largest perforators are selected regardless of ‘‘row’’
and the location of these vessels can usually be
predicted preoperatively with the 8 mHz Doppler.
The number of perforators to include in the flap is
based on the size and the perfusion of the flap in vivo.
It is a simple maneuver to isolate the perforators and
individually occlude each significant vessel and check
arterial bleeding at the dermal level. This simple test
can be performed before committing to the perforators
or before complete dissection of the pedicle and
eliminates doubt about perfusion. Conversion to a
muscle flap is never considered. A sensory branch of
the intercostal nerves to the skin paddle can often be
identified accompanying the perforating vessels.
These nerves are dissected along with the vascular
bundle and are used to anastomose to an intercostal
sensory branch in the recipient bed in an effort to
provide sensation in the reconstructed breast.
After the desired perforating vessels are selected,
the defect in the anterior rectus sheath is opened
Fig. 3. Flap dissection proceeds with careful elevation of the skin-fat composite from the underlying rectus fascia until the lateral
perforators are encountered.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369362

around them (Fig. 4). Loupe magnification and micro-
surgical technique are used to dissect the perforating
artery and veins through the rectus muscle. Often a
second or third perforator, in line with the first, is
maintained with the flap (Fig. 5). In our experience,
approximately 25% of flaps are based on one perfo-
rator, 50% of flaps are based on two perforators, and
25% of flaps are based on three perforators. As
dissection continues, side branches of the vessels are
divided with bipolar coagulation, silk ligatures, or
Fig. 4. The fascia has been opened around two lateral row perforators. The sensory nerve can often be identified with the
perforating vessels.
Fig. 5. Loupe magnification and microsurgical technique are used to dissect the perforating artery and veins through the rectus
muscle. Often, a second or third perforator that is in line with the first is maintained with the flap.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369 363

clips. The muscle is split along the direction of its
fibers to expose the lateral or medial branch of the deep
inferior epigastric vessels. Intercostal nerves that cross
the pedicle and do not lie between two selected
perforators are preserved. The pedicle is doubly ligated
and divided superior to the take-off point of the most
superior chosen musculocutaneous perforator. The
anterior rectus sheath is split inferiorly and the muscle
fibers are separated to obtain the desired pedicle
length, which typically ranges from 9 cm to 14 cm.
The dissection is usually continued past the point
where the medial and lateral branches converge into
the main deep inferior epigastric artery and vena
comitantes to assure adequately-sized vessels to match
the diameter of the recipient vessels (Fig. 6). After
branches of the pedicle are divided, the skin and fat
flap is a tissue island based on the deep inferior
epigastric artery and vein.
For patients who undergo immediate reconstruc-
tion, the mastectomy specimen is weighed and the
size and shape of skin resection are noted. With
secondary reconstruction, the mastectomy scar is
resected and the chest skin flaps are elevated. The
pectoralis muscle fibers that overlie the third rib at its
junction with the sternum are freed with electro-
cautery, which exposes the underlying costal carti-
lage. For thin patients, the fourth cartilage may be
considered to ensure that the flap covers a potentially
visible depression in the rib donor site. After the
perichondrium is elevated, 2 cm to 3 cm of costal
cartilage is removed. The posterior perichondrium is
carefully opened to expose the internal mammary
vessels. Using loupe magnification, the vessels are
isolated for a distance of 3 cm to 4 cm. The internal
mammary artery (IMA) is usually an excellent recipi-
ent vessel with a diameter of 2 mm to 3 mm. Of the
one or two veins present, the larger vein’s diameter
varies from 2 mm to 4 mm. Although these veins are
often thin-walled, damage during the dissection has
not been problematic when meticulous technique is
used. Care should be taken to avoid opening the
pleura. This has occurred in less than 1% of our
cases; those two cases did not result in pneu-
mothorax. The pedicle is divided and passed under
any crossing intercostal nerves. The harvested flap is
weighed and transferred to the chest wall. It is rotated
180� and the pedicle is laid into the recipient site,
taking care not to twist of the vessels. The flap is
secured in place with #0 silk suture and the operating
microscope is positioned. The larger or only internal
Fig. 6. The dissection is usually continued past the point where the medial and lateral branches converge into the main deep
inferior epigastric artery and vena comitantes to assure adequately sized vessels to match the diameter of the recipient vessels.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369364

mammary vein is ligated distally and divided. The
anastomosis is completed to the flap vein with a
microvascular coupling device (Micro Companies
Alliance, Birmingham, AL). Attention is then direc-
ted to completion of the anastomosis of the IMA to
the deep inferior epigastric artery with 9.0 nylon
suture. Upon completion of the microvascular ana-
stomosis, an implantable Doppler cuff (Cook Vas-
cular, Inc., Leechburg, PA) is placed around the vein
to provide postoperative monitoring. The cuff is
stabilized with 9.0 nylon sutures and the wire pro-
tector is secured to the chest wall. The handheld
Doppler probe is used to mark the location on the
skin paddle where the perforating arteries enter.
The flap is tailored to achieve the desired breast
size and shape, paying close attention to the weight
of the mastectomy specimen. Using the IMA as the
recipient vessel facilitates medial positioning. Lateral
fullness may be minimized with tacking sutures to
the serratus or lateral pectoralis major muscle. A
closed suction drain is placed and the skin island,
incorporating the arterial perforator marking, is
sutured into place. A temperature strip is applied to
the skin island and a control site to further the
postoperative monitoring.
The opening in the anterior rectus sheath is
closed without tension with a layer of running #0
Panacryl (Fig. 7). The remaining donor site closure
follows standard abdominoplasty closure of the skin
flaps with umbilicoplasty. A suction drain is brought
out through the lateral incision.
Postoperatively, the patient is monitored in the
surgical intensive care unit for 24 hours. No anti-
coagulants are given during or after surgery. Often, a
unit of autologous blood is given, but banked blood is
rarely needed. Monitoring by the nursing staff
includes flap skin color, capillary refill, temperature
referenced to control, and venous and arterial Doppler
signal confirmation. Usually, on the morning after
surgery, the Foley catheter is removed, the intrave-
nous fluids are stopped, and the patient is cleared to
get out of bed. Oral analgesics are typically sufficient
at this point and the patient is usually discharged
home on the fourth postoperative day. Activities are
resumed over the next several weeks and the patient
is given precautionary instructions, including avoid-
ance of prone positioning for 3 to 4 weeks.
Nipple reconstruction and any necessary donor
site revisions are performed at a second stage 6 to
12 weeks after the initial surgery. The patients who
Fig. 7. The opening in the anterior rectus sheath can be closed without tension. The rectus muscle remains intact and viable.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369 365
undergo immediate reconstructions and skin-sparing
techniques are often afforded the aesthetic benefit of
little or no visible or residual flap skin paddle. Nipple
tattooing follows as the third and final stage of the
reconstructive protocol.
Discussion
Advances in breast reconstruction have been in
response to an increase in demand. The incidence of
breast cancer throughout the industrialized world is
high; the advent of genetic testing, combined with
well-defined clinical and pathologic risk factors,
have increased the indications for therapeutic and
prophylactic mastectomies. Bilateral reconstructions
are frequently required and place more demands than
ever on the plastic surgeon to achieve symmetric and
natural results while minimizing donor site morbid-
ity. Breast reconstruction advances, using perforator
flaps and arterialized skin flaps, have made autoge-
nous reconstruction available to more patients with
less morbidity.
As experience with the DIEP flap has grown
throughout the country, so has the acceptance of the
procedure as a significant step forward in reconstruc-
tive surgery of the breast. Avoidance of muscle
destruction, with a resultant decrease in abdominal
weakness and hernia, are the basic factors that have
established the DIEP flap’s place in the reconstructive
menu. Arguments against the use of this flap as a first
line choice for the patient undergoing mastectomy
have included increased operative time and the need
for microsurgical expertise. The need for microsurgi-
cal proficiency is a given. The procedure requires
meticulous technique and attention to detail. The
surgeon who performs ‘‘occasional’’ microsurgery
would probably do better with a less demanding
operation. Microsurgery has evolved to the point
where high failure rates and marathon surgical times
are no longer a valid counterargument against using a
free flap for breast reconstruction, especially when the
patient is afforded less morbidity compared with
pedicled and free TRAM reconstructions. Our review
of more than 800 cases performed at our institution
showed that the operative times are no longer than the
free TRAM, and may, on occasion, be shorter, as mesh
repair of the abdomen is never required with the DIEP.
The average operative time in this series was 5.4 hours
for unilateral reconstructions and 8 hours for bilateral
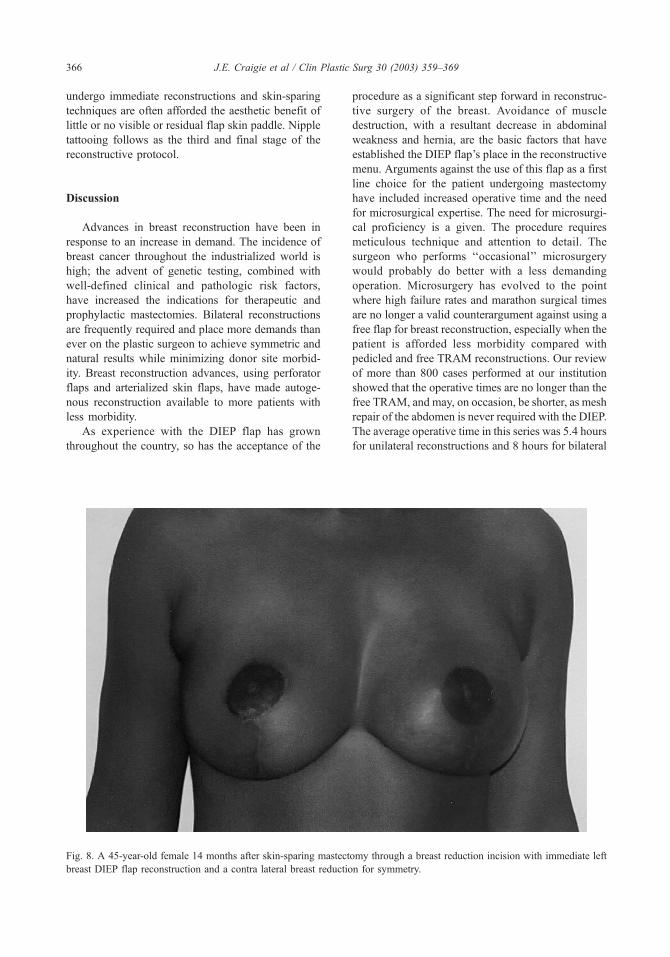
Fig. 8. A 45-year-old female 14 months after skin-sparing mastectomy through a breast reduction incision with immediate left
breast DIEP flap reconstruction and a contra lateral breast reduction for symmetry.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369366

procedures. We have found that the DIEP flap is
particularly well suited for simultaneous, bilateral
reconstruction. Harvesting two skin flaps from the
lower abdomen, without sacrifice of the anterior rectus
sheath or rectus abdominus muscle, significantly
reduces the donor site morbidity that is often associ-
ated with bilateral TRAM flap reconstruction. Avoid-
ing a tight fascial closure and the use of synthetic mesh
allows the patient to be ambulatory on the first post-
operative day. We have found that most patients are
comfortable on oral analgesics alone by postoperative
Day 1. The hospital stay averaged 4.3 days in our
patient population.
Early complications were comparable to other
procedures in this series. The incidence of take-back
to the operative suite was 6.5%. The venous occlusion
rate was 5% and the arterial occlusion rate was 1%.
Since adopting the coupling device as our preferred
method of venous anastomosis, our take-back rate has
dropped even further. Hematoma occurred in 1% of
patients and the total flap loss rate was 1%.
Late complications included seromas in 4% of
patients and delayed abdominal wound healing in
2%. Mesh was never required for fascial repair.
Hernia formation in five of our patients was the result
of unraveling in a continuous suture that was used to
repair the fascial incision; this was easily repaired
with resuturing at a second operation. Fat necrosis
that required revision surgery occurred in 16 of our
patients. These revisions were usually done at the
same time as nipple reconstruction and abdominal
scar revisions, when required.
Smoking did not significantly increase the inci-
dence of early complications; however, late compli-
cations of delayed wound healing and fat necrosis
were significantly increased. The incidence of fat
necrosis that required revision was 13.5% for smok-
ers and 3% for nonsmokers. This compares to
previous reports, which are as high as 26% for
smokers [21]. The incidence of delayed wound
healing was 9% in smokers and 3% in nonsmokers.
Other series have reported rates of delayed wound
healing that ranged from 8% to 27% [22].
The effects of radiation therapy on our patients
were reviewed recently [23]. We found that post-
operative radiation significantly increased the late
Fig. 9. A 45-year-old female, 15 months after right skin-
sparing mastectomy through a periareolar incision and
immediate right breast reconstruction with a DIEP flap.
Fig. 10. A 49-year-old female 19 months after bilateral skin-
sparing mastectomies and immediate bilateral breast recon-
struction with bilateral DIEP flaps.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369 367

occurrence of fat necrosis in the reconstructed breast
and can substantially compromise the aesthetic result.
We no longer recommend immediate reconstruction
for patients who are scheduled for radiation after
surgery. Delayed reconstruction is undertaken in this
group 6 months after completion of their therapy to
allow the acute effects of their treatments to settle.
Recent publications by other investigators on their
experience with the DIEP flap raised questions about
venous congestion and the selection criteria for the use
of the flap [24,25]. Proponents of muscle flaps often
convert to a free TRAM to avoid congestion and
perfusion problems if the perforator vessels do not
appear robust or if flap volume requirements are large.
We do not share this philosophy and rarely have
experienced venous congestion. To manage this prob-
lem, our strategies are to include multiple perforators
in the flap and to preserve the superficial inferior
epigastric vein to provide additional venous outflow if
needed. Additional routes for venous outflow with an
additional microvascular anastomosis rarely are
needed, but we are prepared to address this problem
with additional efforts intraoperatively to avoid the
increased donor site morbidity that is associated with
muscle sacrifice. Our experience with this flap has
been extensive and our success has not been compro-
mised by muscle preservation.
Fig. 11. A 53-year-old female 6 months after bilateral skin-
sparing mastectomies and immediate bilateral reconstruction
with bilateral DIEP flaps.
Fig. 12. A 55-year-old female 19 months after delayed reconstruction of a right modified radical mastectomy defect and
simultaneous left breast reduction.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369368

Summary
Muscle-sparing autogenous breast reconstruction
has enhanced the multidisciplinary care that is avail-
able to patients who have breast cancer. The DIEP flap
has proven reliability, a low complication rate, and is
applicable to many clinical scenarios (Figs. 8–12).
Avoidance of muscle sacrifice in the abdomen ulti-
mately translates into greater patient satisfaction. The
increased demands, in terms of surgical expertise, are
more than offset by decreased postoperative pain and
decreased donor site morbidity. The methods that were
used to innovate the DIEP flap have been applied to
other donor sites and the available options for patients
have been expanded.
References
[1] Fujino R, Harashina R, Enomoto K. Primary breast
reconstruction after a standard radical mastectomy
by free flap transfer. Plast Reconstr Surg 1976;58:
371–4.
[2] Holmstrom H. The free abdominoplasty flap and its
use in breast reconstruction. Scand J Plast Reconst
Surg 1979;13:423–7.
[3] Hartampf CR, Scheflan M, Black PW. Breast recon-
struction with a transverse abdominal island flap. Plast
Reconstr Surg 1982;69:216–25.
[4] Hartrampf CR, Bennet GK. Autogenous tissue recon-
struction in the mastectomy patient: a critical review of
300 patients. Ann Surg 1987;205:508–19.
[5] Kroll SS, Evans G, Reece RD, et al. Comparison of
resourcecosts of free and conventional TRAM flap
breast reconstruction. Plast Reconstr Surg 1996;98:
74–7.
[6] Baldwin BJ, Schusterman MD, Miller MJ, et al. Bilat-
eral breast reconstruction: conventional versus free
TRAM. Plast Reconstr Surg 1994;93:1410–6.
[7] Allen RJ, Treece P. Deep inferior epigastric perforator
flap for breast reconstruction. Ann Plast Surg 1994;
32:32–8.
[8] Kroll SS, Sharma S, Koutz C, et al. Postoperative
morphine requirements of free TRAM and DIEP flaps.
Plast Reconstr Surg 2001;107(2):338–41.
[9] Kroll SS, SchustermanMA, Reece GP, et al. Abdominal
wall strength, bulging and hernia after TRAM flap
breast reconstruction. Plast Reconstr Surg 1995;96:
616–9.
[10] Mizgala CL, Hartrampf CR, Bennet GK. Assessment of
the abdominal wall after pedicled TRAM flap surgery:
5 to 7 year follow-up of 150 consecutive patients. Plast
Reconstr Surg 1994;93:988–1002.
[11] Suominen S, Asko-Seljavaara S, Von Smitten K, et al.
Sequelae in the abdominal wall after pedicled or free
TRAM flap surgery. Ann Plast Surg 1996;36:629–36.
[12] Duchateau J, Declety A, Lejour M. Innervation of the
rectus abdominis muscle: implications for rectus flaps.
Plast Reconstr Surg 1988;82:223–7.
[13] Suominen S, Tervahartiala P, von Smitten K, et al.
Magnetic resonance imaging of the TRAM flap donor
site. Ann Plast Surg 1997;38:23–8.
[14] Futter CM. Abdominal donor site morbidity: impact of
the TRAM and DIEP flap on strength and function.
Semin Plast Surg 2002;16(1):119–30.
[15] Blondeel PN, Vanderstraeten GG, Monstrey SJ, et al.
The donor site morbidity of free DIEP flaps and free
TRAM flaps for breast reconstruction. Br J Plast Surg
1997;50:322–30.
[16] Futter CM, Webster MHC, Hagen S, et al. A retrospec-
tive comparison of abdominal muscle strength follow-
ing breast reconstruction with a free TRAM or DIEP
flap. Br J Plast Surg 2000;53:578–83.
[17] Koshima I, Soeda S. Inferior epigastric artery skin flap
without rectus abdominus muscle. Br J Plast Surg 1989;
42:645–8.
[18] Perforator Guerra A, Allen RJ, Dupin CL. Breast re-
construction with the superior gluteal artery (S-GAP)
flap. Semin Plast Surg 2002;16(1):27–34.
[19] Allen RJ, Heitland A. Superficial inferior epigastric ar-
tery flap for breast reconstruction. Sem Plast Surg 2002;
16(1):35–43.
[20] Vath SD, Dupin CL, Allen RJ. Internal mammary ves-
sels as a recipient site for free flap breast reconstruction.
Semin Plast Surg 2002;16(1):109–17.
[21] Padubidri AN, Yetman R, Browne E, et al. Complica-
tions of post mastectomy breast reconstruction in smok-
ers, ex-smokers, and non-smokers. Plast Reconstr Surg
2001;107:342–9.
[22] Kroll SS. Necrosis of abdominoplasty and other sec-
ondary flaps after TRAM flap breast reconstruction.
Plast Reconstr Surg 1994;94:637.
[23] Rogers NE, Allen RJ. Radiation effects on breast re-
construction: a review. Semin Plast Surg 2002;16(1):
19–25.
[24] Nahabedian MY, Momen B, Galdino G, et al. Breast
reconstructionwith the free TRAMorDIEP flap: patient
selection, choice of flap, and outcome. Plast Reconstr
Surg 2002;110(2):466–75.
[25] Namnoum JD. Discussion of breast reconstruction with
the free TRAM or DIEP flap: patient selection, choice
of flap, and outcome by Nahabedian MY, et al. Plast
Reconstr Surg 2002;110(2):476–7.
J.E. Craigie et al / Clin Plastic Surg 30 (2003) 359–369 369





























