Embed Size (px)
Citation preview

Review articlejir_1197 852..873
Autism spectrum disorders in genetic syndromes:implications for diagnosis, intervention andunderstanding the wider autism spectrum disorderpopulation
J. Moss & P. Howlin
Department of Psychology, Institute of Psychiatry, King’s College, London, UK
Abstract
Background An emerging literature on behaviouralphenotypes has highlighted apparent associationsbetween autism spectrum disorders (ASDs) orASD-related phenomenology and a number of dif-ferent genetically determined syndromes.Method A systematic review of the current litera-ture regarding the association with ASD and ASDcharacteristics was conducted in the following syn-drome groups: Fragile X, Rett,Tuberous SclerosisComplex, Down, Angelman, CHARGE and Phe-nylketonuria. Specific consideration was given to therole of intellectual disability in assessing the associa-tion between ASD and these syndrome groups.Results The review highlights that while formaldiagnostic assessments may indicate an associationbetween ASD and specific syndrome groups,detailed investigation has revealed subtle but quali-tative differences in the presentation of ASD-likephenomenology in particular syndrome groups. Thedegree of ID of the individual clearly has a role toplay with regard to the development and presenta-tion of ASD-like characteristics, and caution shouldbe taken when assessing ASD symptomatology in
genetically determined syndromes associated withsevere ID. However, degree of ID cannot solelyaccount for the heightened prevalence of ASD char-acteristics in some specific syndrome groups.Conclusions There is a need for caution in inter-preting the significance of superficial similaritiesbetween ASD and the behavioural phenotypes ofcertain genetically determined syndromes. However,recognition of ASD-like characteristics (even wherea true diagnosis of ASD may not be relevant) inindividuals with genetic syndromes is crucial inensuring that individuals receive appropriate behav-ioural management and educational placement.Further research in this field requires fine-grainedinvestigation of behavioural phenomenology withinindividual syndrome groups.
Keywords autism spectrum disorder, behaviouralphenotypes, genetic syndromes
Introduction
Autism spectrum disorders (ASDs) are classified byDSM-IV-TR (APA 2000) and ICD-10 (WHO1992) as pervasive developmental disorders (PDD)characterised by the presence of three core features:qualitative impairments in communication and insocial interaction and the presence of repetitive
Correspondence: Dr Jo Moss, Department of Psychology, Instituteof Psychiatry, Henry Wellcome Building, PO 77, De CrespignyPark, London SE5 8AF, UK (e-mail: [email protected]).
Journal of Intellectual Disability Research doi: 10.1111/j.1365-2788.2009.01197.x
volume 53 part 10 pp 852–873 october 2009852
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

behaviour and restricted interests. ASDs1 occur inup to 1% of children in the general population(Baird et al. 2006) and in up to 40% of individualswith ID (La Malfa et al. 2004).
The specific causes of ASD remain unknown, butare largely considered to be genetically linked(Abrahams & Geschwind 2008). However, while anumber of chromosomes and genetic loci have beenimplicated, there is little evidence to suggest thatany one of these is solely linked to ASD diagnosis.The large number of identified risk loci has ledresearchers to suggest that ASD is caused bycomplex multigenetic interactions rather thansimple single-gene mutations (Zhao et al. 2007).Recent evidence from a population-based studysuggests that there may be different aetiologicalpathways contributing to each of the different diag-nostic domains of ASD (Ronald et al. 2006). Someresearchers, therefore, consider it to be more helpfulto conceptualise the aetiology of ASD in terms of a‘network’ of dysfunctions that occur on a numberof levels, including genetic and neuronal pathways.The underlying aetiology of ASD now appears to bea highly complex process, involving various genesthat affect downstream proteins and neural sub-strates that subsequently lead to the behaviouralmanifestations of ASD (Belmonte & Bourgeron2006; Persico & Bourgeron 2006; Abrahams &Geschwind 2008). An alternative approach to themultigenetic hypothesis is proposed by Zhao et al.(2007) who suggest that most cases of autism aredue to de novo mutations in the paternal germ linethat can affect any number of critical loci. It is sug-gested that de novo mutations may be carried bysome protected and asymptomatic individuals, par-ticularly women, who will transmit the mutation ina dominant pattern to male offspring.
There has been an increasing interest in the asso-ciation between ASD and a number of geneticallylinked conditions. The presence of ASD or autisticcharacteristics has been reported in a wide varietyof disorders, including those with variable aetiology(e.g. anorexia nervosa, Tourette syndrome, ADHD);
physical and sensory disorders (cerebral palsy, mus-cular dystrophy, Leber’s congenital amaurosis) andsyndromes with a known genetic cause [e.g. Tuber-ous Sclerosis Complex (TSC), Fragile X syndrome(FXS), Down syndrome (DS), Angelman syndrome(AS), Coffin-Lowry, Cohen Laurence-Moon-Biedel,Marinesco-Sjogren, Moebius syndromes, Rettsyndrome (RS) and Williams syndrome; seeFombonne 1999 and Gillberg & Coleman 2000 forreviews].
The apparent overlap between various syndromeswith known genetic causes and ASD symptomatol-ogy clearly has implications with regard to ourunderstanding of ASD at both the behavioural andbiological levels. Some researchers propose thatgenetic syndromes may be influential in identifyingand understanding the genetic and neural pathwaysunderlying ASD more widely (Persico & Bourgeron2006). One suggestion is that although each syn-drome may arise from different genetic abnormali-ties, with multiple molecular functions, the effectsof these abnormalities give rise to common effectsdownstream, in the biological pathway or neuralcircuits, which result in the presentation of ASDcharacteristics (Abrahams & Geschwind 2008). Analternative stance is proposed by Skuse (2007) whosuggests that the list of genetic syndromes with anapparent association with ASD is growing to suchan extent and with such diversity that these associa-tions are unlikely to provide specific answers withregard to the gene loci and network pathwaysinvolved in ASD. In fact, this emergence of associa-tion across a range of genetically determined syn-dromes makes the interpretation and understandingof their significance more complex. Skuse arguesthat genetic susceptibility for ASD does not mani-fest in the behavioural phenotype of specific geneticsyndromes. Rather, the ID associated with manygenetic syndromes simply increases the risk thatASD or autistic characteristics will be revealed.Skuse suggests that this is due to the fact thatimpaired intellectual ability diminishes the possibil-ity for cognitive compensation of independentlyinherited autistic-type traits. In this way, thepresence of a genetic syndrome and the associateddegree of ID may simply act as an additional riskmarker for ASD characteristics, rather than playinga causal role. According to this model of associationwe would expect to find that genetic syndromes
1 For the purposes of this review, the term ASD will be employedthroughout the text to refer to all conditions classified by theDSM-IV-TR (2000) within the category of Pervasive Developmen-tal Disorder with the exception of Rett syndrome and Child Disin-tegrative Disorder. When referring to particular studies, theterminology used by the authors of the study will be employed.
853Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

associated with more severe ID will be more likelyto manifest ASD-like symptoms. In the followingreview, we consider this position in a range of syn-drome groups that have been reported to be associ-ated with ASD.
The following annotation is divided into two sec-tions. Section I presents a brief systematic review ofthe association between ASD and a number of dif-ferent genetic syndromes. In this section we aim toprovide a broad understanding of the nature of theassociation between ASD and these various geneticsyndromes. We also consider the role of ID in theassociation between a given syndrome and ASD.Section II focuses on the specific clinical implica-tions of understanding the association betweenASD and genetic syndromes in terms of diagnosisand intervention and also the conceptual implica-tions of these associations.
Section I: the association between autismspectrum disorders and genetic syndromes
For the purpose of this review a systematic search,using the Web of Science, of papers published since1970 was conducted. All articles with the terms
‘autism’ OR ‘autistic’ AND each of the differentneurodevelopmental genetic syndromes identified ashaving an association with ASD in the reviews ofGillberg & Coleman (2000) or Fombonne (1999)were scrutinised. Only papers in which the titleindicated an association between ASD and the syn-drome concerned were considered. Series of papersinvolving the same participant samples werecounted as a single study. Table 1 summarises thedates/number of articles identified. For somesyndromes (e.g. Klein-Levin, Smith Magenis, San-filippo and Steinert’s myotonic dystrophy), althoughan association with ASD has been suggested,no articles with the words ‘autism’ or ‘autistic’ inthe title were identified, hence these are notincluded in Table 1.
Based on this search, this section of the annota-tion focuses first on syndromes in which the asso-ciation with ASD has been most frequentlyreported – Fragile X Syndrome and Rett Syndromeand Tuberous Sclerosis Complex. We include hereonly studies that have employed standardisedassessments with good psychometric properties/diagnostic criteria. We then consider several othergenetic disorders that have received comparatively
Table 1 Number of articles identified vialiterature search
Syndrome Dates of studiesNumber of articles withdifferent samples
Fragile X 1982–2006 95Tuberous Sclerosis 1979–2006 32Rett 1985–2006 31Down 1979–2006 16Phenylketonuria 1969–2003 9CHARGE 1998–2006 7Angelman 1996–2004 6Neurofibromatosis 1998–2007 4Joubert 1991–2005 4Williams 1985–2006 2Goldenhar 1992–2002 2Hypomelanosis of Ito 1991–2002 2Noonan 1983–1994 2Sotos 1990–2001 2VCF 1998–2006 2Leber’s amaurosis 1989–2007 2Cohen syndrome 2001–2005 1Cornelia de Lange syndrome 2006 1Ehlers-Danlos 1992 1Lujan-Fryns 2005 1Moebius 1989 1
854Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

less attention in the literature, but where at leastfive published papers on the association with ASDare described. These include: Down syndrome,CHARGE syndrome, Angelman syndrome andPhenylketonuria (PKU).
Fragile X syndrome
Fragile X syndrome (FXS) is the most commoncause of inherited ID, occurring in 1 in 3600 malesand 1 in 8000 females (Cornish et al. 2008). Itresults from an excess of CGG trinucleotide repeatson the FMR1 (Fragile X Mental Retardation-1)gene at location Xq27-3 (Dykens et al. 2000). InFXS males, the degree of ID is usually reported tobe within the mild to severe range while FXSfemales usually demonstrate a mild degree of learn-ing disability, although this can be more severe in asmall percentage of females (approximately 25%;Cornish et al. 2008).
Reported prevalence rates of ASD in FXS varywidely from 0 to 60%, although the most recentestimates from studies conducted between 2001 todate are more consistent, ranging from 21% to50%. The percentage of ASD in females with FXSis lower, between 1% and 3% (see Table 2). Thevariation in estimates of ASD among the earlierstudies is likely to result from the use of differentmethodologies and diagnostic criteria; the moreconsistent findings in recent years are likely toreflect an increased reliability in both ASD diagno-sis and genetic testing for FXS. Recent studiesreport a strong correlation between the associateddegree of ID and, in particular, impairments inverbal skills and the presence of ASD characteristicsin FXS (Demark et al. 2003; Kaufmann et al. 2004;Lewis et al. 2006; Loesch et al. 2007). This seems tosupport Skuse’s suggestion that the severity of IDincreases the risk of ASD symptomatology ingenetic syndromes. However, ASD has also beenidentified in individuals with the pre-mutation FXSwith mild cognitive impairments or IQ in thenormal range (Hagerman et al. 2005). Dissanayakeet al. (2009) report that while individuals with FXSand ASD demonstrate a similar profile of scores onthe Autism Diagnostic Observation Schedule(ADOS) (Lord et al. 2000) to individuals with idio-pathic ASD, individuals with FXS score signifi-cantly lower on tests of performance and verbal IQ.
The authors suggest that the common pathwayunderlying the shared characteristics of FXS andASD is likely to be neural rather than genetic, inwhich diverse biological pathways may lead to acommon cognitive and behavioural outcome.
Studies that have focused on the specific phenom-enology of ASD in FXS have raised doubts aboutthe strength of association Bailey et al. (2001). Baileyet al. (1998) and Demark et al. (2003) suggest thatsevere autism is relatively rare and that a milder pre-sentation of ASD symptomatology is more charac-teristic of individuals with FXS. Fine-grainedanalysis has identified specific areas of behaviourthat, although they may appear initially to be ASD-related, seem to be qualitatively different from thecharacteristics identified in idiopathic autism. Indi-viduals with FXS are more likely to demonstratesocial anxiety, extreme shyness and gaze avoidancealongside seemingly preserved emotion sensitivityand willingness to interact (Turk & Cornish 1998;Lesniak-Karpiak et al. 2003; Hall et al. 2006;Cornish et al. 2007; Roberts et al. 2007).This profileis somewhat different to the social impairments thatare characteristic of idiopathic autism. Moreover, thegaze avoidance and perseverative speech described inFXS are reported to be unrelated to verbal ability orage (in contrast to the autism population) and aremore marked in FXS than they are in autism or‘non-specific’ ID (Sudhalter et al. 1990). Recentresearch suggests that in FXS it is the impairmentsin social interaction that are most likely to contributeto an individual meeting criteria for ASD (Kauf-mann et al. 2004; Budimirovic et al. 2006).Thedevelopmental trajectory of ASD in FXS is alsoreported to differ from idiopathic autism and,according to some studies, the rate of autism andsocial avoidance behaviours increases with age inmales with full-mutation FXS (Hatton et al. 2006;Roberts et al. 2007).These findings suggest thateven when individuals with FXS meet criteria forASD on autism-specific assessments, they may do sofor somewhat different reasons from those withidiopathic ASD.
Recent findings also suggest that in addition tosubtle differences at the behavioural level regardingapparently shared ASD characteristics in FXS, dif-ferences between these two populations may beobserved at the level of social-cognition (Cornishet al. 2008). For example, detailed analysis of
855Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

Theory of Mind (ToM) skills in individuals withFXS with and without ASD and individuals withID indicates that, while all three groups seem toperform at a similar level on ToM tasks, differencesin error patterns suggest that the underlying bases
for these deficits are syndrome-specific. Grant et al.(2007) reported that impaired false belief reasoningin FXS was downstream of a more primary impair-ment in working memory in those with and withoutASD characteristics. In contrast to individuals with
Table 2 Prevalence studies of autism spectrum disorder (ASD) in Fragile X syndrome (FXS)
AuthorNumber ofparticipants with FXS
Autism diagnosticassessment/criteria n (%) meeting autism/ASD criteria
Levitas et al. (1983) 10 males DSM-III† 6 (60%)Brown et al. (1986) 150 males DSM-III† 26 (17%)Hagerman et al. (1986) 50 males DSM-III† 16 (32%); 15 (30%) additional participants
met criteria in early childhood but not oncurrent behaviourABC‡
15 (31%) met ABC criteria; ‘Autistic traits’identified in almost all cases
Reiss & Freund (1990) 17 males DSM-III-R† 3 (18%); 3 additional cases met criteria in earlychildhood; 7 (41%) met PDD-NOS criteria
Cohen et al. (1991) 13 multiplex families(total n = 35)
DSM-III† 11 (31%); 3 of 7 probands (43%); 4 of 28(15%) remaining males in family met currentcriteria
Kerby & Dawson (1994) 9 males DSM-III-R† FXS significantly more autistic characteristicsthan controls with ID9 ID controls
Turk & Graham (1997) 49 males HBS§; 14 (29%) FXS45 Down syndrome males (DS) DSM-III-R† 5 DS (11%)42 males with ‘idiopathic
intellectual disability’ (ID)18 ID (43%)
Mazzocco et al. (1997) 30 females NDI¶; 1(3%) FXS31 age/IQ-matched controls. DSM-III-R† 1 (3%) control
5 (17%) FXS vs. 2 (6% ) controls met PDDcriteria
FXS more autistic characteristics thancontrols on NDI
Bailey et al. (2001) 55 males CARS** 14 (25%) ‘autistic behaviour’; 12 (22%)‘mildly-moderately autistic’; 1 (2%) ‘severelyautistic’
Demark et al. (2003) 15 males CARS** 6 (40%) FXS vs. 8 (38%) PDD‘mildly-moderately autistic’;21 children with pervasive
developmental disorder(PDD)
1 (7%) FXS vs. 11 (52%) PDD ‘severelyautistic’
Sabaratnam et al. (2003) 18 males DSM-III-R† NoneKau et al. (2004) 55 males ADI-R†† 14 (26%) FXS vs. 7 (32%) DLD met autism
criteria22 males with developmental
language delay (DLD).DSM-IV† 18 (33%) FXS vs. 3 (14%) DLD met PDD
criteriaHatton et al. (2006) 142 males & 32 females CARS** 38 (21%; 36 males, 2 females)
† Diagnostic and Statistical Manual (American Psychiatric Association 1980, 1987, 1994).‡ Autism Behavior Checklist (Krug et al. 1980).§ The Schedule of Handicaps, Behaviour and Skills ( Wing 1980).¶ Neuropsychiatric Developmental Interview (Reiss & Freund 1990).** Childhood Autism Rating Scale (Schopler & Renner 1988).†† Autism diagnostic interview, revised (Rutter et al. 2003b)
856Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

ASD, emotion perception in FXS is reported to becommensurate with overall level of ability (Turk &Cornish 1998; Wishart et al. 2007).
It is clear that while the association between ASDand FXS is considered to be reasonably robust,this may only be evident at the level of overtsymptomatology/diagnostic cut-off scores. When thespecific profile of behaviours is considered in moredetail, those characteristics that initially appear tobe autism-related in fact demonstrate qualitativedifferences with idiopathic autism at both thebehavioural and socio-cognitive levels. Thus,although individuals with FXS may appear to sharea number of core characteristics with individualswith ASD, the underlying aetiological pathwaysinvolved may differ between these two disorders(Cornish et al. 2008). The study of ASD character-istics in FXS provides a good example of whycareful, detailed assessment and identification ofASD-related characteristics is important in order toavoid erroneous conclusions concerning the associa-tion between ASD and genetic syndromes.
Summary
FXS is a genetic syndrome associated with mild tosevere intellectual impairments. Current estimatessuggest that ASD occurs in 21–50% of males withFXS, with ASD being more likely to be identified inindividuals with a greater degree of ID. Studies thathave considered the phenomenology of ASD inFXS in more detail have identified differences inthe nature, quality and development of ASD char-acteristics in FXS that raise questions regardingthe strength of association between these twodisorders.
Rett syndrome
Rett syndrome (RS) is a neurological disorder, pre-dominantly affecting females, occurring in between1 in 15 000–22 800 live female births (Kozinetzet al. 1993). It is caused by mutations on theX-linked MECP2 gene (Amir et al. 1999). In theclassic form of RS, development often appears rela-tively normal for the 6–18 months. This is followedby a period of regression resulting in a reduction inhead circumference growth, onset of seizures andloss of language and motor skills, leading to severe
or profound intellectual and physical disabilities(Nomura & Segawa 2005). However, there is arange of severity of RS, and some individuals havebeen reported to retain and develop their languageskills further (Kerr et al. 2001; Smeets et al. 2005).These milder cases of RS are more likely to beassociated with a slightly different type and locationof genetic mutation on the MECP2 gene than thosewith classic RS (Kerr et al. 2001; Smeets et al.2005; Neul et al. 2008).
In Rett’s initial account of the syndrome (Rett1966; cited in Van Acker 1997), ‘autistic-like’ behav-iour was noted as being characteristic of the disor-der. Subsequently, estimates of rates of ASD in RSrange from 25% to 40% and up to 97% in individu-als with the preserved speech variant of RS (seeTable 3). ASD is also the most common initial mis-diagnosis in children with RS, with 18% of indi-viduals being diagnosed with ASD before receivinga diagnosis of RS (Young et al. 2008).
The overlap between RS and ASD has previouslybeen considered to be so robust that RS is currentlyclassified as a PDD alongside autism, according toboth the DSM-IV-TR (APA 2000) and the ICD-10
(WHO 1992) diagnostic criteria. However, theinclusion of RS within the PDD category is nowconsidered inappropriate by many (Tsai 1992),because of distinct differences in phenomenology.For example, many (although not all) individualswith RS develop simple speech before regressionand despite the marked deterioration in social skills,eye contact is often maintained; social impairmentsand autistic characteristics also tend to improvewith age (Nomura & Segawa 2005). Furthermore,the characteristic repetitive hand movements in RSare very different from the motor stereotypesobserved in individuals with ASD (Howlin 2002). Itis important to ensure that unique syndrome char-acteristics such as these are not misclassified inassessments of ASD symptomatology. Even whendiagnostic criteria for autism are met, individualswith RS demonstrate an atypical profile of phenom-enology. They manifest fewer of the core features ofautism and are more likely to score on non-autism-specific items, such as ‘sleeps too much’, ‘underactive’ and ‘unhappy’ (Mount et al. 2003a).
The severity of ID typically associated with RSalso confounds the distinction between ASD andRS. The ability reliably to identify ASD-specific
857Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

impairments in the areas of communication, socialinteraction and repetitive behaviours becomes farmore difficult as the degree of ID increases (Howlin2000). However, Mount et al. (2003b) reported thatindividuals with RS scored significantly higher onthe Autism Behavior Checklist (Krug et al. 1980)than individuals with a matched level of ID, indicat-ing that ASD characteristics in RS are not solelyaccounted for by the degree of ID. Moreover, esti-mated prevalence rates of ASD characteristics areactually higher in more mildly affected individualswith RS (up to 97%; Zappella et al. 1998, 2001)although other studies report that these individualsdemonstrate good social interaction skills (Kerret al. 2006).
Summary
Early studies indicated an increased prevalence ofASD in RS and this led to the inclusion of RSunder the PDD category within DSM and ICDcriteria. Recently, more fine-grained assessmentssuggest that the inclusion of RS in the PDD cat-egory is inappropriate. Although the prevalence ofASD in RS is heightened when compared with indi-viduals matched for degree of ID, and individualswith RS who are more mildly affected have beenreported to demonstrate a higher prevalence ofASD characteristics, individuals with RS demon-strate an atypical profile of characteristics comparedwith those with idiopathic autism.
Tuberous Sclerosis Complex
Tuberous Sclerosis Complex (TSC) occurs in 1 in6000 live births (O’Callaghan 1999) and is causedby a mutation in the TSC1 (9q34) or TSC2 genes(16p13; Povey et al. 1994). Mutations in either generesult in dysregulated cell development, giving riseto abnormal tissue growth or benign tumours in thebrain, skin, kidneys and heart (Crino et al. 2006).The TSC phenotype is extremely variable withsome individuals having only superficial skinproblems or mild seizures; others show severephysical effects and profound ID (de Vries &Howe 2007).
Autistic-type symptoms in TSC were first notedby Critchley & Earl (1932) who described 29 indi-viduals with impaired social contact, stereotypedbehaviours, absent or abnormal speech and socialwithdrawal. However, it was only after Kanner’sdescription of autism in 1943 (Kanner 1943) thatthe behaviours noted by Critchley & Earl were rec-ognised as being characteristic of ASD. Despitethese early descriptions, the association betweenASD and TSC has only recently been systematicallyexplored. Reported rates of ASD in TSC rangefrom 5% to 89%, although the more consistentlyreported prevalence figures range from 24% to 60%(see Table 4). Although it has been suggested thatcomorbidity of ASD in TSC is associated with thepresence of temporal-lobe tubers (Bolton et al.2002), not all individuals with temporal-lobe
Table 3 Prevalence of autism spectrum disorder (ASD) in Rett syndrome (RS)
AuthorNumber of girlswith RS
Autism diagnosticassessment/criteria
n (%) meetingautism/ASD criteria
Witt-Engerstrom &Gillberg (1987)
47 DSM-III† 18 (38%) autism diagnosis & 19 (40%)autistic-like behaviours reportedbefore diagnosis of RS
Naidu et al. (1990) 22 ABC‡ NoneZappella et al. (1998) 30 (with preserved
speech variant)DSM-IV† 29 (97%)
Sandberg et al. (2000) 8 DSM-IV† 2 (25%)Mount et al. (2003b) 15 ABC‡ 6 (40%) RS vs. 1 (7%) ID scored above
autism cut-off14 females withsevere/profound ID
† Diagnostic and Statistical Manual (American Psychiatric Association 1980, 1994).‡ Autism Behavior Checklist (Krug et al. 1980).
858Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd
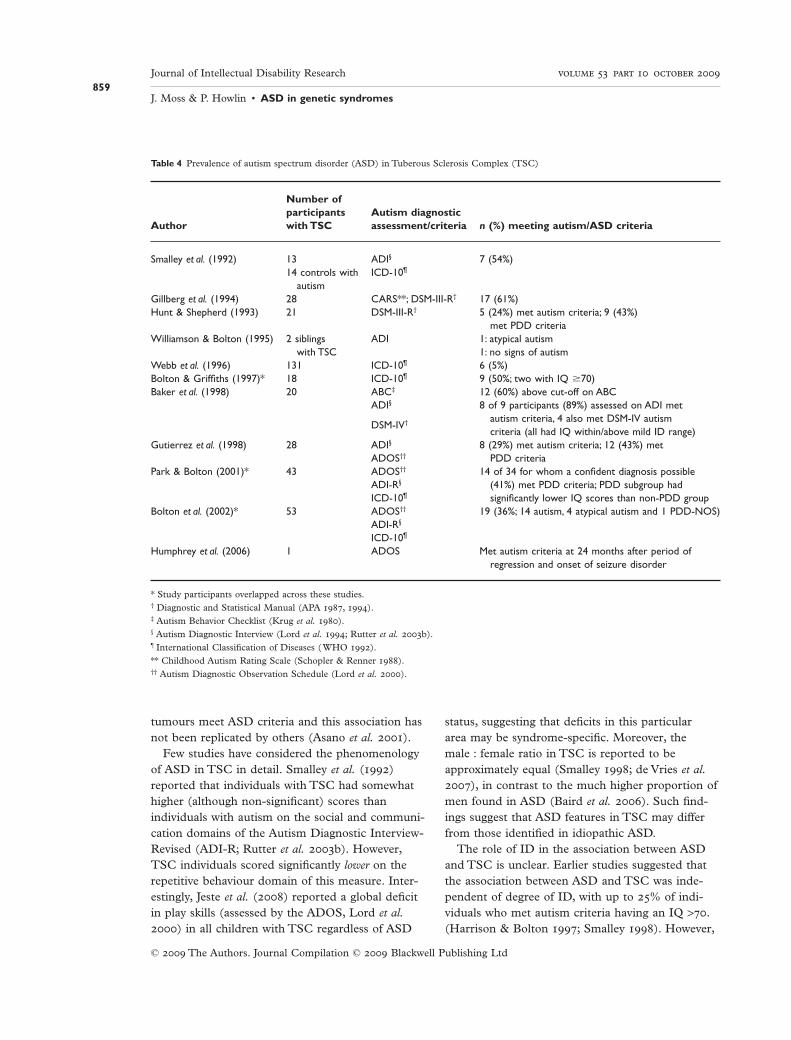
tumours meet ASD criteria and this association hasnot been replicated by others (Asano et al. 2001).
Few studies have considered the phenomenologyof ASD in TSC in detail. Smalley et al. (1992)reported that individuals with TSC had somewhathigher (although non-significant) scores thanindividuals with autism on the social and communi-cation domains of the Autism Diagnostic Interview-Revised (ADI-R; Rutter et al. 2003b). However,TSC individuals scored significantly lower on therepetitive behaviour domain of this measure. Inter-estingly, Jeste et al. (2008) reported a global deficitin play skills (assessed by the ADOS, Lord et al.2000) in all children with TSC regardless of ASD
status, suggesting that deficits in this particulararea may be syndrome-specific. Moreover, themale : female ratio in TSC is reported to beapproximately equal (Smalley 1998; de Vries et al.2007), in contrast to the much higher proportion ofmen found in ASD (Baird et al. 2006). Such find-ings suggest that ASD features in TSC may differfrom those identified in idiopathic ASD.
The role of ID in the association between ASDand TSC is unclear. Earlier studies suggested thatthe association between ASD and TSC was inde-pendent of degree of ID, with up to 25% of indi-viduals who met autism criteria having an IQ >70.(Harrison & Bolton 1997; Smalley 1998). However,
Table 4 Prevalence of autism spectrum disorder (ASD) in Tuberous Sclerosis Complex (TSC)
Author
Number ofparticipantswith TSC
Autism diagnosticassessment/criteria n (%) meeting autism/ASD criteria
Smalley et al. (1992) 13 ADI§ 7 (54%)14 controls with
autismICD-10¶
Gillberg et al. (1994) 28 CARS**; DSM-III-R† 17 (61%)Hunt & Shepherd (1993) 21 DSM-III-R† 5 (24%) met autism criteria; 9 (43%)
met PDD criteriaWilliamson & Bolton (1995) 2 siblings
with TSCADI 1: atypical autism
1: no signs of autismWebb et al. (1996) 131 ICD-10¶ 6 (5%)Bolton & Griffiths (1997)* 18 ICD-10¶ 9 (50%; two with IQ �70)Baker et al. (1998) 20 ABC‡ 12 (60%) above cut-off on ABC
ADI§ 8 of 9 participants (89%) assessed on ADI metautism criteria, 4 also met DSM-IV autismcriteria (all had IQ within/above mild ID range)
DSM-IV†
Gutierrez et al. (1998) 28 ADI§ 8 (29%) met autism criteria; 12 (43%) metPDD criteriaADOS††
Park & Bolton (2001)* 43 ADOS†† 14 of 34 for whom a confident diagnosis possible(41%) met PDD criteria; PDD subgroup hadsignificantly lower IQ scores than non-PDD group
ADI-R§
ICD-10¶
Bolton et al. (2002)* 53 ADOS†† 19 (36%; 14 autism, 4 atypical autism and 1 PDD-NOS)ADI-R§
ICD-10¶
Humphrey et al. (2006) 1 ADOS Met autism criteria at 24 months after period ofregression and onset of seizure disorder
* Study participants overlapped across these studies.† Diagnostic and Statistical Manual (APA 1987, 1994).‡ Autism Behavior Checklist (Krug et al. 1980).§ Autism Diagnostic Interview (Lord et al. 1994; Rutter et al. 2003b).¶ International Classification of Diseases ( WHO 1992).** Childhood Autism Rating Scale (Schopler & Renner 1988).†† Autism Diagnostic Observation Schedule (Lord et al. 2000).
859Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

more recent studies have identified a greater risk ofautism and ASD with increased degree of ID inTSC (Wong 2006; de Vries et al. 2007; Jeste et al.2008). The latter findings are consistent withSkuse’s model of overall increased risk of ASD withincreased degree of ID. Nevertheless, currentresearch indicates that up to 17% of individualswith TSC with an IQ in the normal range arereported to meet criteria for ASD (Prather & deVries 2004; de Vries et al. 2007). This is still aheightened rate in comparison with the prevalenceof ASD in the general population, suggesting thatthe degree of ID associated with TSC cannot solelyaccount for the raised prevalence of ASD in TSC.
Summary
Although research suggests a strong associationbetween ASD and TSC at the diagnostic level, fewstudies have considered the precise nature of ASDphenomenology in this condition. The degree towhich the associated ID contributes to the associa-tion between ASD and TSC is unclear, but recentstudies indicate that, as is the case with FXS, theprevalence of ASD increases with the degree of ID.
In the final part of this section, we consider fourgenetic disorders where the association with ASDhas received comparatively less attention within theliterature, but where at least five published paperson the association with ASD have been identified.As the evidence concerning their association withASD is limited, the discussion here includes casereports and studies that have either investigated theprevalence of ASD or have described ASD-likebehaviours within the syndrome. Only studies usingstandardised assessments and diagnostic criteria areincluded within the tables.
Down syndrome
Down syndrome (DS) is the most common chro-mosomal cause of ID, occurring in approximately10.3 in 10 000 live births (Bell et al. 2003). Typi-cally, DS is caused by the presence of a full orpartial trisomy of chromosome 21, although occa-sionally an unbalanced translocation involving chro-mosome 21 has been identified (Dykens et al.2000). ID in DS ranges from mild to severe(Capone et al. 2005).
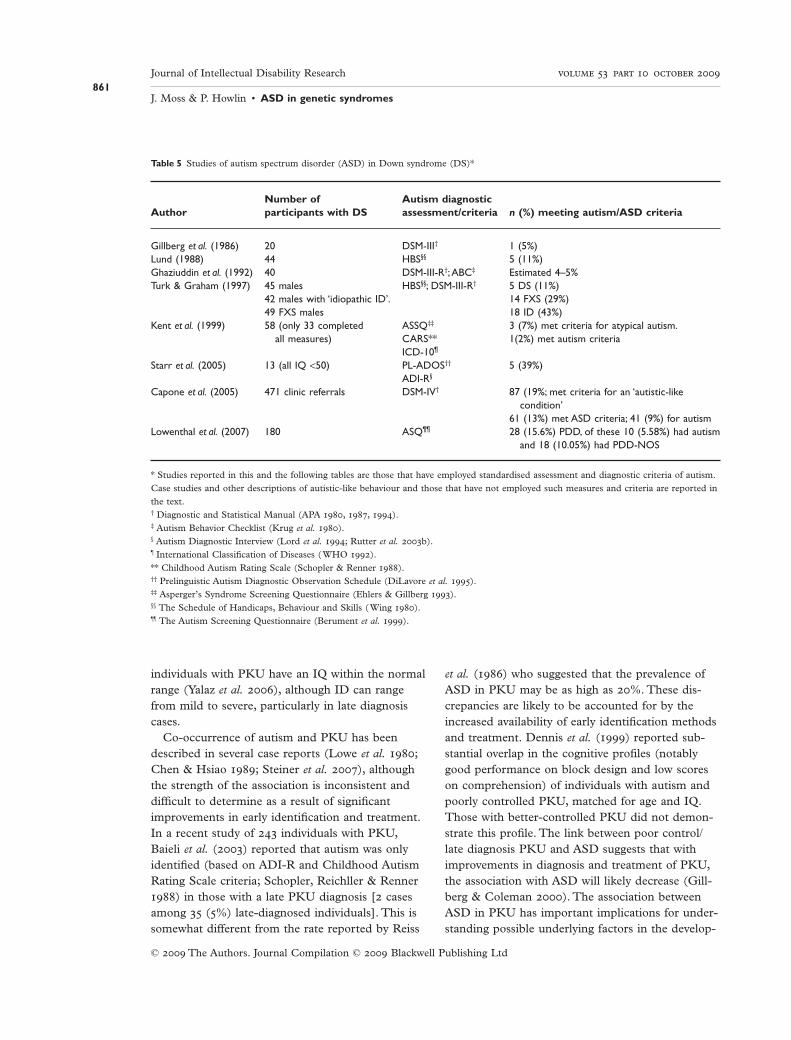
Previously, the association between ASD and DSwas considered to be relatively rare; indeed, therewere suggestions that DS might actually be protec-tive against autistic-like behaviours (Turk 1992).However, several case studies have describedindividuals with DS who also met ASD criteria(Wakabayashi 1979; Bregman & Volkmar 1988;Ghaziuddin et al. 1992; Howlin et al. 1995) andrecent research indicates that comorbidity may bemore common than previously thought with preva-lence rates ranging from 5% to 39% (see Table 5).Difficulties in social-cognition, notably in areasrelated to ToM and emotion perception, have alsobeen reported in some children with DS (Zelazoet al. 1996; Wishart 2007; Wishart et al. 2007; Hip-polyte et al. 2008). Higher rates of impaired socialskills have also been reported in family members ofindividuals with DS and ASD in comparison withindividuals with DS without ASD (Lowenthal et al.2007).
Individuals with DS and ASD are reported tohave a greater degree of ID and higher rates of ste-reotyped behaviours, hyperactivity and inappropri-ate speech than those with DS without ASD(Capone et al. 2005). However, it remains unclearhow far the increased severity of intellectual impair-ment can explain the increased prevalence of ASDsymptomatology in this subgroup. Further researchis required to investigate the phenomenology ofthese characteristics in DS more carefully, in orderto clarify whether these characteristics are indeedshared, are superficially similar to that of idiopathicASD or perhaps associated with different underly-ing aetiologies.
Phenylketonuria
Phenylketonuria (PKU) is a genetic disorder associ-ated with defects in protein metabolism, resulting inan inability to break down the amino acid phenyla-lanine. PKU occurs in approximately 1 in 10 000
live births (Scriver et al. 1994). Pre/post-natalscreening has significantly reduced PKU in devel-oped countries and with early diagnosis and acontrolled diet the effects of PKU are minimal.However, in cases of late diagnosis, high levels ofprotein in the diet can produce toxic levels of phe-nylalanine hydroxylase, resulting in ID, seizuresand many physical difficulties. The majority of
860Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd
individuals with PKU have an IQ within the normalrange (Yalaz et al. 2006), although ID can rangefrom mild to severe, particularly in late diagnosiscases.
Co-occurrence of autism and PKU has beendescribed in several case reports (Lowe et al. 1980;Chen & Hsiao 1989; Steiner et al. 2007), althoughthe strength of the association is inconsistent anddifficult to determine as a result of significantimprovements in early identification and treatment.In a recent study of 243 individuals with PKU,Baieli et al. (2003) reported that autism was onlyidentified (based on ADI-R and Childhood AutismRating Scale criteria; Schopler, Reichller & Renner1988) in those with a late PKU diagnosis [2 casesamong 35 (5%) late-diagnosed individuals]. This issomewhat different from the rate reported by Reiss
et al. (1986) who suggested that the prevalence ofASD in PKU may be as high as 20%. These dis-crepancies are likely to be accounted for by theincreased availability of early identification methodsand treatment. Dennis et al. (1999) reported sub-stantial overlap in the cognitive profiles (notablygood performance on block design and low scoreson comprehension) of individuals with autism andpoorly controlled PKU, matched for age and IQ.Those with better-controlled PKU did not demon-strate this profile. The link between poor control/late diagnosis PKU and ASD suggests that withimprovements in diagnosis and treatment of PKU,the association with ASD will likely decrease (Gill-berg & Coleman 2000). The association betweenASD in PKU has important implications for under-standing possible underlying factors in the develop-
Table 5 Studies of autism spectrum disorder (ASD) in Down syndrome (DS)*
AuthorNumber ofparticipants with DS
Autism diagnosticassessment/criteria n (%) meeting autism/ASD criteria
Gillberg et al. (1986) 20 DSM-III† 1 (5%)Lund (1988) 44 HBS§§ 5 (11%)Ghaziuddin et al. (1992) 40 DSM-III-R†;ABC‡ Estimated 4–5%Turk & Graham (1997) 45 males HBS§§; DSM-III-R† 5 DS (11%)
42 males with ‘idiopathic ID’. 14 FXS (29%)49 FXS males 18 ID (43%)
Kent et al. (1999) 58 (only 33 completedall measures)
ASSQ‡‡ 3 (7%) met criteria for atypical autism.CARS** 1(2%) met autism criteriaICD-10¶
Starr et al. (2005) 13 (all IQ <50) PL-ADOS†† 5 (39%)ADI-R§
Capone et al. (2005) 471 clinic referrals DSM-IV† 87 (19%; met criteria for an ‘autistic-likecondition’
61 (13%) met ASD criteria; 41 (9%) for autismLowenthal et al. (2007) 180 ASQ¶¶ 28 (15.6%) PDD, of these 10 (5.58%) had autism
and 18 (10.05%) had PDD-NOS
* Studies reported in this and the following tables are those that have employed standardised assessment and diagnostic criteria of autism.Case studies and other descriptions of autistic-like behaviour and those that have not employed such measures and criteria are reported inthe text.† Diagnostic and Statistical Manual (APA 1980, 1987, 1994).‡ Autism Behavior Checklist (Krug et al. 1980).§ Autism Diagnostic Interview (Lord et al. 1994; Rutter et al. 2003b).¶ International Classification of Diseases ( WHO 1992).** Childhood Autism Rating Scale (Schopler & Renner 1988).†† Prelinguistic Autism Diagnostic Observation Schedule (DiLavore et al. 1995).‡‡ Asperger’s Syndrome Screening Questionnaire (Ehlers & Gillberg 1993).§§ The Schedule of Handicaps, Behaviour and Skills ( Wing 1980).¶¶ The Autism Screening Questionnaire (Berument et al. 1999).
861Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

ment of ASD. In the case of PKU, the toxic levelsof phenylalanine hydroxylase appear to play a sig-nificant role in the development of ASD symptoma-tology. In the wider ASD population, this is unlikelyto be a common underlying factor. This suggeststhat the presence of ASD characteristics may be acommon end state of a number of different aetio-logical pathways.
CHARGE syndrome
CHARGE syndrome occurs in approximately 1 in10 000–12 000 live births (Issekutz et al. 2005). Theunderlying genetic cause has yet to be established,although recent studies have identified mutations onthe CHD7 gene (Vissers et al. 2004). The syn-drome’s acronym, CHARGE, refers to the charac-teristic physical deficits: Coloboma of the eye,Heart defects, Atresia of the choanae, Retardationof growth and/or development, Genital and/orurinary abnormalities, and Ear abnormalities anddeafness. There is great variability in the presenceand severity of these abnormalities. Many childrenwith CHARGE syndrome have IQs in the normalrange although ID can occur.
The behavioural phenotype of CHARGE has notbeen widely studied, but hyperactivity, obsessions,compulsions and tic disorders have been noted(Wachtel & Hartshorne 2006; Kuijpers et al. 2007).Autistic-like behaviours have been described inseveral case reports (Davenport et al. 1986; Fernellet al. 1999; Sabaratnam et al. 2000; Wachtel &
Hartshorne 2006; Kuijpers et al. 2007). Larger-scalestudies suggest that the prevalence of ASD rangesfrom 15% to 50% (see Table 6).
Information is limited regarding the degree of IDand sensory deficits associated with CHARGE–ASD comorbidity. The two cases described bySmith et al. (2005) suggest that ASD is more likelyin non-verbal individuals with severe to profoundID. In a larger study, Hartshorne et al. (2005)found some variability in the severity of autisticsymptomatology in comparison with individualswith ASD, but the results indicated that the pres-ence of autism characteristics in CHARGE couldnot be wholly accounted for by the visual andhearing impairments typically associated with thesyndrome.
Angelman syndrome
Angelman syndrome (AS) occurs in approximately1 in 12 000–15 000 live births (Clayton-Smith &Pembrey 1992; Kyllerman 1995) and is caused bymaternally inherited anomalies on chromosome 15.Approximately 70% of cases of AS are due tomaternal deletions; between 2% and 5% are causedby paternal uni-parental disomy. Approximately2–3% of cases have imprinting defects, includingdeletions of the imprinting centre, and a further 1%have other unusual mutations on chromosome 15.The remaining 22–25% of individuals with AS havemutations in the UBE3A critical region (Dykenset al. 2000). AS is associated with a severe to
Table 6 Studies of autism spectrum disorder (ASD) in CHARGE syndrome
AuthorNumber of participantswith CHARGE
Autism diagnosticassessment/criteria
n (%) meetingautism/ASD criteria
Smith et al. (2005) 13 SCQ¶ 2 (15 %) autism3 (23%) ASD
Hartshorne et al. (2005) 160 ABC‡ 44 (28%)Johansson et al. (2006) 18 ABC‡ 9 (50%)
ADI-R§
DSM-IV†
† Diagnostic and Statistical Manual (APA 1994).‡ Autism Behavior Checklist (Krug et al. 1980).§ Autism Diagnostic Interview (Lord et al. 1994; Rutter et al. 2003b).¶ Social Communication Questionnaire (Rutter et al. 2003a).
862Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd
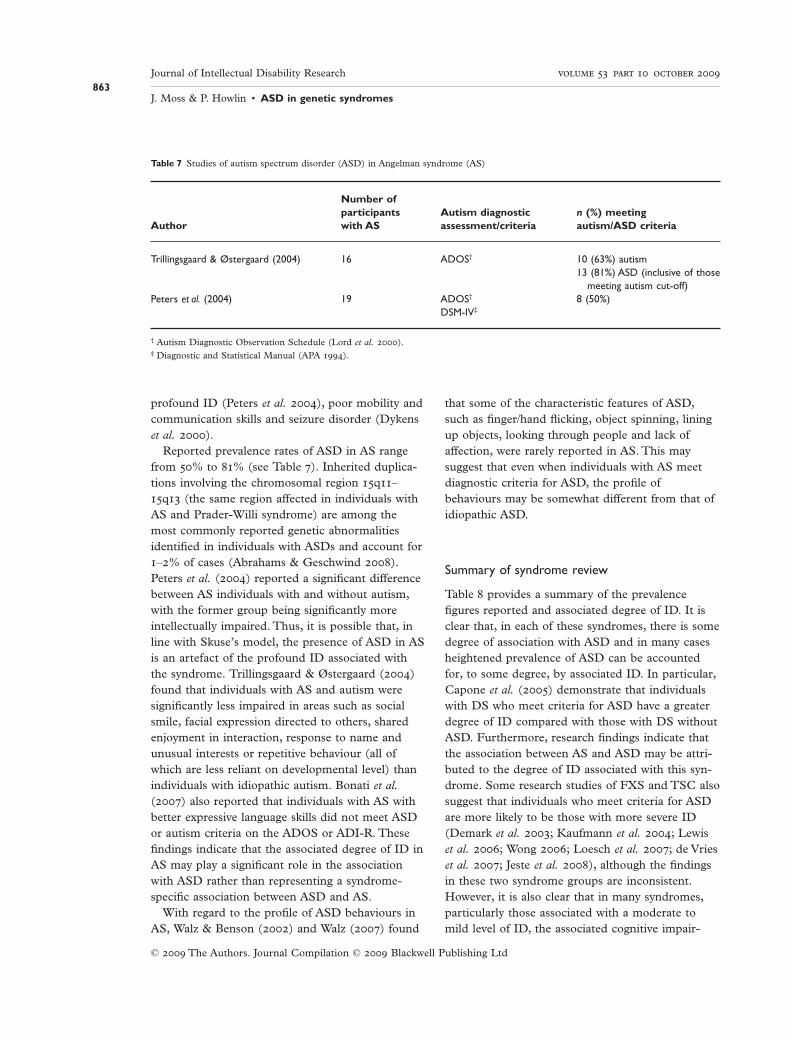
profound ID (Peters et al. 2004), poor mobility andcommunication skills and seizure disorder (Dykenset al. 2000).
Reported prevalence rates of ASD in AS rangefrom 50% to 81% (see Table 7). Inherited duplica-tions involving the chromosomal region 15q11–15q13 (the same region affected in individuals withAS and Prader-Willi syndrome) are among themost commonly reported genetic abnormalitiesidentified in individuals with ASDs and account for1–2% of cases (Abrahams & Geschwind 2008).Peters et al. (2004) reported a significant differencebetween AS individuals with and without autism,with the former group being significantly moreintellectually impaired. Thus, it is possible that, inline with Skuse’s model, the presence of ASD in ASis an artefact of the profound ID associated withthe syndrome. Trillingsgaard & Østergaard (2004)found that individuals with AS and autism weresignificantly less impaired in areas such as socialsmile, facial expression directed to others, sharedenjoyment in interaction, response to name andunusual interests or repetitive behaviour (all ofwhich are less reliant on developmental level) thanindividuals with idiopathic autism. Bonati et al.(2007) also reported that individuals with AS withbetter expressive language skills did not meet ASDor autism criteria on the ADOS or ADI-R. Thesefindings indicate that the associated degree of ID inAS may play a significant role in the associationwith ASD rather than representing a syndrome-specific association between ASD and AS.
With regard to the profile of ASD behaviours inAS, Walz & Benson (2002) and Walz (2007) found
that some of the characteristic features of ASD,such as finger/hand flicking, object spinning, liningup objects, looking through people and lack ofaffection, were rarely reported in AS. This maysuggest that even when individuals with AS meetdiagnostic criteria for ASD, the profile ofbehaviours may be somewhat different from that ofidiopathic ASD.
Summary of syndrome review
Table 8 provides a summary of the prevalencefigures reported and associated degree of ID. It isclear that, in each of these syndromes, there is somedegree of association with ASD and in many casesheightened prevalence of ASD can be accountedfor, to some degree, by associated ID. In particular,Capone et al. (2005) demonstrate that individualswith DS who meet criteria for ASD have a greaterdegree of ID compared with those with DS withoutASD. Furthermore, research findings indicate thatthe association between AS and ASD may be attri-buted to the degree of ID associated with this syn-drome. Some research studies of FXS and TSC alsosuggest that individuals who meet criteria for ASDare more likely to be those with more severe ID(Demark et al. 2003; Kaufmann et al. 2004; Lewiset al. 2006; Wong 2006; Loesch et al. 2007; de Vrieset al. 2007; Jeste et al. 2008), although the findingsin these two syndrome groups are inconsistent.However, it is also clear that in many syndromes,particularly those associated with a moderate tomild level of ID, the associated cognitive impair-
Table 7 Studies of autism spectrum disorder (ASD) in Angelman syndrome (AS)
Author
Number ofparticipantswith AS
Autism diagnosticassessment/criteria
n (%) meetingautism/ASD criteria
Trillingsgaard & Østergaard (2004) 16 ADOS† 10 (63%) autism13 (81%) ASD (inclusive of those
meeting autism cut-off)Peters et al. (2004) 19 ADOS† 8 (50%)
DSM-IV‡
† Autism Diagnostic Observation Schedule (Lord et al. 2000).‡ Diagnostic and Statistical Manual (APA 1994).
863Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

ment cannot solely account for the raised preva-lence of ASD. Of the three most commonlyresearched syndromes, with regard to theirassociation with ASD (i.e. FXS, RS and TSC), onlyRS is characterised by severe and profound ID.TSC and FXS are both associated with a milderdegree of ID and yet the reported prevalence rate ofASD in all three groups is upwards of 15%. Therole that the degree of ID plays in the manifestationof ASD in these syndrome groups is, therefore,unclear and further work is required, particularly inAS and TSC, in order to establish further thespecificity of the syndrome–ASD association. It isclearly important that individuals’ degree ofID be taken into account when consideringwhether or not they meet diagnostic criteria. Thisis relevant to both research and clinical assessmentsof ASD.
A final point to note is that within each of thesyndrome groups reviewed above, clinicaldiagnosis or formal, algorithm-based cut-off crite-ria have been used to determine the prevalence orrate of ASD. However, further detailed examina-tion of the specific ASD profile in these syn-dromes reveals a range of similarities anddifferences in the specific behavioural pattern ofASD within each group. It seems that each syn-drome group may have their own, unique,syndrome-specific ‘signature’ of ASD characteris-tics and impairments that are different from thoseobserved in idiopathic ASD. It is these atypicalprofiles that may prove to be of most importancein further understanding the aetiology of ASD andthe conceptualisation of the triad of impairmentsand the spectrum of autism.
Section II: diagnostic considerations ofdifferential diagnosis in genetic syndromesand implications for intervention,conceptual and theoretical frameworks
Studies identifying ASD symptomatology in specificgenetic conditions have provided valuable informa-tion on the behavioural phenotypes of the syn-dromes described in this review. However, researchin this area has also highlighted some importantdiagnostic, intervention-related and conceptualissues.
Diagnostic considerations
Recent research regarding the boundaries of theautism spectrum has tended to support a continu-ous severity gradient (Spiker et al. 2002; Constan-tino et al. 2004; Ring et al. 2008), rather than aclear distinction between ‘affected’ and ‘non-affected’ individuals. Family genetic studies clearlyshow that among first-degree relatives of probandswith ASD, up to 20% show difficulties associatedwith social functioning, communication or rigidbehaviours/beliefs (Bolton et al. 1994; Fombonneet al. 1997). Indeed, none of the core characteristicsof ASD are unique to individuals with ASD. Mostpeople have fixed patterns of doing certain things,sociability varies widely and few people are fullycompetent in all aspects of verbal and non-verbalcommunication. In the absence of any genetic testfor ASD, diagnosis is based on clinical judgement ofwhen such problems extend beyond the normalrange. However, as yet, there is no definition ofwhere the boundaries of the ‘normal range’ lie and
Table 8 Summary of prevalence figures and associated degree of ID within syndrome groups
Genetic syndrome Associated degree of IDEstimated prevalence ofautism spectrum disorder
Fragile X syndrome Moderate to severe 21–50%Rett syndrome Severe to profound 25–40% (classic), 97% (mild)Tuberous Sclerosis Complex Normal to profound 15–89%; 17% (normal IQ)Down syndrome Moderate to severe 5–39%Phenylketonuria Normal to severe 5%CHARGE Normal to severe 15–50%Angelman syndrome Severe to profound 50–80%
864Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

it should be remembered that even when standard-ised instruments, such as the ADI-R or ADOS(both of which are becoming increasingly consid-ered as the ‘gold standard’ instruments for assess-ment of ASD), are used, cut-off scores aredetermined by statistically significant group differ-ences. This is why, for reliable diagnosis, suchassessments must be used in conjunction withexpert clinical judgement (Lord 1995; Lord et al.2006). Similarly, caution should be taken whenrelying on clinical judgement alone without the useof standardised measures to guide diagnosis. Thenature of the ICD-10 and DSM-IV-TR diagnosticmanuals is such that, inevitably, diagnoses usingthese descriptive criteria alone are based on a sub-jective judgement only and this may lead to pro-blems of validity and with reliability, even betweenexpert clinicians.
The diagnosis of ASD and identification of ASDsymptomatology are particularly problematic inindividuals affected by genetic disorders in whichsocial, communication and behavioural difficultiesare also present, and particularly in those syn-dromes associated with a severe to profound degreeof ID. As noted in section I, it is extremely difficultto identify ASD-specific behaviours and impair-ments in individuals with such complex difficulties.Many of the diagnostic criteria outlined in theDSM-IV-TR and ICD-10 manuals are heavilyreliant upon the individual reaching a certain levelof development. Thus, individuals with a moresevere degree of intellectual impairment may appearto fulfil certain criteria for ASD purely because theyhave not yet reached the developmental levelrequired to demonstrate these behaviours. More-over, recent studies that have investigated the valid-ity of assessments, such as the ADOS and ADI-R,in children with ID have indicated poor to moder-ate agreement between the ADI-R and clinicaljudgement and between the ADI-R and ADOS.There are also indications that sensitivity and speci-ficity of both the ADI-R and the ADOS arereduced in very young children and in individualswith low developmental age (Ventola et al. 2006;Chawarska et al. 2007; Gray et al. 2008). Otherstudies have reported validity and reliability to begood in individuals with severe ID (de Bildt et al.2004). It must also be recognised thatstandardised assessments, such as the ADI-R
(Rutter et al. 2003b) or ADOS (Lord et al. 2000),were not designed to distinguish between neurode-velopmental conditions in which social-communication impairments are common butcomplex and somewhat different in nature fromthose that are typical of idiopathic autism, nor werethey designed to be sensitive to often subtle differ-ences between groups.
The importance of employing a detailed and fine-grained analysis of the relationship between ASDand other conditions is well illustrated in theexamples of FXS and RS (see section I). Initialdescriptions at a superficial behavioural level sug-gested a significant, even causal, relationship withASD. However, further systematic and standardisedinvestigation of the specific phenomenology of ASDcharacteristics within these groups revealed verydifferent developmental, behavioural and cognitiveprofiles from those found in individuals with idio-pathic ASD. For example, eye gaze avoidance inFXS and ASD was initially considered to be ashared characteristic in both populations. However,it is now suggested that in FXS eye gaze avoidanceoccurs in response to hypersensitivity to sensorystimuli, hyperarousal and social anxiety, while inASD the same behaviour is reported to result froma more general impairment in understanding socialinteraction (Cornish et al. 2007, 2008). Theseexamples highlight the need for caution in drawingconclusions about the relationship between ASDand a given syndrome group. The complex andoften unusual behavioural and cognitive patternsthat are characteristic of many genetic syndromesmay result in individuals obtaining scores above theautism cut-off on a standard assessment, even whenthe underlying mechanisms of these characteristicsare different from those of individuals with idio-pathic ASD. It is therefore important that investiga-tions of the association between ASD and a geneticdisorder be conducted meticulously, at both theclassification/diagnostic and behavioural level.
Implications for intervention in individuals withdifferential diagnosis
There is sometimes a tendency within clinical andeducational settings to attribute all the behavioursand difficulties shown by an individual directly tothe specific genetic syndrome from which he/she
865Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd
suffers, rather than considering the possibility ofother additional or differential diagnoses. ‘Diagnos-tic overshadowing’ (Reiss et al. 1982; Dykens 2007)of this kind can be a particular problem in the caseof rare genetic syndromes, with the result that othercauses and, more importantly, possible interven-tions, may not be considered by parents orprofessionals.
For example, Jeremy2 was an 18-year-old withCornelia de Lange syndrome. In his teens hebecame progressively more withdrawn and uncom-municative and was diagnosed as being selectivelymute. However, his eye contact had always beenpoor and since childhood he had a keen preferencefor routine and engaged in various repetitive andstereotyped behaviours. The possibility of ASD wasnot considered until he was 17 years old, despite hisparents’ previous requests for assessment. The moveto college, where the emphasis was on flexibilityand student choice, rather than the structure androutine he needed, led to significant deterioration inhis mood and behaviour. The college were unwillingto modify their programme, insisting that Jeremyneeded to ‘learn to be more flexible and cope withthe changes’. Jeremy became increasingly tearfuland withdrawn, stopped taking part in his usualdaily activities and refused to go to college.Although he has since received a formal diagnosisof ASD, Jeremy still remains at home, with no edu-cational provision. His outcome contrasts markedlywith that of David, another 18-year-old with Corne-lia de Lange syndrome for whom, following aperiod of regression in his late teens, the recogni-tion that he showed many characteristics of ASDled to his being transferred to specialist autism pro-vision, resulting in significant improvements in hismood and behaviour.
Leber’s congenital amaurosis is another conditionthat has been linked to ASD (Rogers & Newhart-Larson 1989). Ivan was an 11-year-old boy with thisdisorder, attending a school for visually impairedchildren. Although he had some very specific areasof skill, especially in music, he showed no interestin other children, had very stereotyped and repeti-tive language and very fixed routines. The headmas-
ter did not agree with the possibility that he mighthave ASD and therefore did not support hisparents’ request for transfer to a specialist ASDunit. Ivan became increasingly isolated, self-injurious behaviours increased and his parentsfound it more and more difficult to cope. He even-tually required placement in a residential school.
In another case, Jake, an 8-year-old boy with DS,showed a typical ASD profile of repetitive, non-communicative speech, poor eye contact, limitedinteraction with other people and a host of repeti-tive and restricted interests. Although his parentshad become increasingly concerned about his lackof progress, school staff interpreted his behavioursas being ‘difficult’ or ‘naughty’ and again rejectedthe possibility of comorbid ASD. Over time, Jake’sbehaviour became steadily more disruptive andaggressive. Diagnostic assessment for ASD indicatedthat he met all the criteria for this disorder andtransfer to a specialist autism unit was recom-mended (see Howlin et al. 1995 for furtherexamples).
Such vignettes illustrate how failure to recognisethe possibility of ASD or the implications of ASDsymptomatology can have negative and long-lastingeffects. However, while clinically it is important torecognise that individuals with a given genetic syn-drome may have similar educational and supportneeds to those with idiopathic autism (Rutter et al.1994), there is a need to be cautious about over-inclusive use of the term ‘autistic’. Mathew, forexample, was a young man with Williams syndromewho, unusually for this condition, also had pro-found learning disabilities. His limited communica-tion skills, lack of sociability and highly stereotypedbehaviours resulted in his being given the additionaldiagnosis of ASD, despite the fact that these diffi-culties were explicable in terms of his very low IQ.His parents, having read about various ‘cures’ forASD, believed that enrolment in an intensive behav-ioural autism unit would solve all his difficulties,and were bitterly disappointed when the unit wouldnot accept him because of his severe intellectualimpairment.
While recognition of shared ASD characteristicsmay be extremely important for appropriate behav-iour management and school placement, we are notaware of any research to date that has consideredthe suitability and effectiveness of ASD-specific
2 Please note that each of the case studies reported here use indi-vidual cases that have been observed/assessed by the authors inclinical or research settings, and all cases are reported usingpseudonyms.
866Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

interventions for use in children and adults withgenetic syndromes who have a differential diagnosisof ASD or ASD-related characteristics. Childrenwith genetic syndromes may not receive a differen-tial diagnosis of ASD until much later than indi-viduals in the wider ASD population. Given the latediagnosis and considering the complex behavioural,communication and intellectual impairments thatare often associated with genetic syndromes, adap-tation to current autism-specific interventions maybe required in order to be effective in such cases.Additionally, better dissemination of information toprofessionals and care workers, regarding the asso-ciation between ASD symptomatology and geneti-cally determined syndromes, may be important forincreasing recognition of these shared characteris-tics. Future research to consider the effectiveness ofvarious autism-specific interventions may be helpfulin guiding appropriate management and educationalplacement of individuals with genetic syndromesand ASD.
Implications for understanding the wider ASDpopulation
Unsubstantiated claims that X % of children withcondition Y have ASD, or conversely that X % ofchildren with ASD have condition Y, are not helpfulfor advancing research or clinical practice. Many ofthe earlier claims about the association betweenFXS and ASD, for example, were made in theabsence of reliable genetic testing or standardiseddiagnostic assessments. When standardised diagnos-tic and behavioural assessments of ASD began to beused, a far weaker association was identified andstudies have since identified specific differences thatmay distinguish the two disorders (see section I fordetails).
Rutter et al. (1994) made the point that in anumber of conditions that are claimed to have ahigh association with autism (e.g. PKU, Rubella),the ASD profile tends to be atypical. The fact thatso many different syndromes are associated withcommunication and social deficits and stereotypedbehaviours raises the issue of how unique this ‘triadof impairments’ is to ASD. Moreover, even thoseindividuals who clearly fall within the ‘broader’autism spectrum and show a number of ASD-related characteristics do not always demonstrate
the full triad of impairments (Charman & Swetten-ham 2001). The fact that the phenomenology ofASD appears to differ, not only across genetic syn-dromes but also between individuals with an ASDdiagnosis, has particular implications for the debateconcerning the boundaries of the autism spectrum.
The apparent heterogeneity of autism spectrumphenomenology across different syndrome groups isalso relevant at the level of aetiology. Traditionally,it has been considered that the three core character-istics of ASD share a single underlying aetiologicalpathway (Morton & Frith 1994). However, there isnow some evidence that the components of thetriad are in fact fractionated at the level of aetiol-ogy. Thus, the different domains have differentdevelopmental trajectories (Charman & Swetten-ham 2001; Charman et al. 2005). Repetitive behav-iours, in particular, may become evident later thansocial and communication impairments; they arealso less likely to improve over time (Fecteau et al.2003; Piven et al. 1996; Charman et al. 2005).Genetic studies of the general population (Ronaldet al. 2006) also suggest that the three domains areonly moderately associated with one another andthat there may be different aetiological explanationsunderlying each domain. This observed divergenceat the aetiological level might account for the differ-ent types of profiles observed across genetic syn-dromes, particularly in conditions where one or twocomponents of the triad of impairments are moreevident than others.
Summary of diagnostic considerations andimplications for intervention andconceptual and theoretical frameworks
There is sometimes a tendency, when working withindividuals with genetic syndromes, to attribute allbehavioural and emotional difficulties to the pres-ence of the syndrome itself, rather than to considerthat there may be shared characteristics with otherdisorders and that in many cases a comorbid diag-nosis might be appropriate. As indicated in thevignettes described above, recognition of shared fea-tures between specific genetic syndromes and ASDmay be crucial in ensuring that individuals receiveappropriate and effective behaviour managementand educational placement. However, it is also
867Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

important to apply the differential diagnosis of ASDappropriately and cautiously. The review of ASDand associated characteristics in the specific syn-drome groups outlined above highlights the impor-tance of conducting fine-grained assessment of ASDin these syndromes. Subtle differences in the qualityand nature of specific ASD-like impairments mayonly be revealed when conducting detailed analysesof behavioural characteristics, and may be maskedat the broader level of clinical or algorithm-baseddiagnoses. Recognition of atypicalities in the profileand phenomenology of ASD in genetic syndromesmay be crucial for developing appropriate, individu-ally tailored, interventions. Continued research inthis area is also important in further understandingthe aetiology or underlying mechanisms andnetwork structures involved in idiopathic ASD andin further unravelling the structure of the triad ofimpairments.
Acknowledgements
The authors would like to thank Professor JamesHarris for his insightful comments and ideasregarding the association between ASD and geneticsyndromes, which stimulated the author’s conceptu-alisation and review of this area of study.
References
Abrahams B. S. & Geschwind D. H. (2008) Advances inautism genetics: on the threshold of a new neurobiol-ogy. Nature Reviews Genetics 9, 341–55.
American Psychiatric Association (1980) Diagnostic andStatistical Manual of Mental Disorders. Third Edition(DSM-III). American Psychiatric Association:Washington D.C.
American Psychiatric Association (1987) Diagnostic andStatistical Manual of Mental Disorders,Third EditionRevised (DSM-III-R). American Psychiatric Association:Washington DC.
American Psychiatric Association (1994) Diagnostic andStatistical Manual of Mental Disorders. Fourth Edition(DSM-IV). American Psychiatric Association:Washington D.C.
American Psychiatric Association (2000) Diagnostic andStatistical Manual of Mental Disorders: DSM-IV-Text Revi-sion. American Psychiatric Association: Washington DC.
Amir R. E., van den Veyber I. B., Wan M., Tran C. Q.,Francke U. & Zoghbi H.Y. (1999) Rett syndrome is
caused by mutations in X-linked MECP2, encodingmethyl-CpG binding protein 2. Nature Genetics 23,185–8.
Asano E., Chugani D. C., Muzik O., Behen M., Janisse J.,Rothermel R. et al. (2001) Autism in tuberous sclerosiscomplex is related to both cortical and subcortical dys-function. Neurology 57, 1269–77.
Baieli S., Pavone L., Meli C., Fiumara A. & Coleman M.(2003) Autism and phenylketonuria. Journal of Autismand Developmental Disorders 33, 201–4.
Bailey D. B., Mesibov G. B., Hatton D. D., Clark R. D.,Roberts J. E. & Mayhew L. (1998) Autistic behavior inyoung boys with Fragile X syndrome. Journal of Autismand Developmental Disorders 28, 499–508.
Bailey D. B., Hatton D. D., Skinner M. & Mesibov G.(2001) Autistic behavior, FMR1 protein, and develop-mental trajectories in young males with fragile X syn-drome. Journal of Autism and Developmental Disorders 31,165–74.
Baird G., Simonoff E., Pickles A., Chandler S., Loucas T.,Meldrum D. et al. (2006) Prevalence of disorders of theautism spectrum in a population cohort of children inSouth Thames: the Special Needs and Autism Project(SNAP). Lancet 368, 210–15.
Baker P., Piven J. & Sato Y. (1998) Autism and TuberousSclerosis Complex: prevalence and clinical features.Journal of Autism and Developmental Disorders 28, 279–85.
Bell R., Rankin J. & Donaldson L. J. (2003) Down’s syn-drome: occurrence and outcome in the north ofEngland, 1985–99. Paediatric and Perinatal Epidemiology17, 33–9.
Belmonte M. K. & Bourgeron T. (2006) Fragile Xsyndrome and autism at the intersection of geneticand neural networks. Nature Neuroscience 9,1221–5.
Berument S., Rutter M., Lord C., Pickles A. & Bailey A.(1999) Autism screening questionnaire: diagnostic valid-ity. British Journal of Psychiatry 175, 444–51.
de Bildt A., Sytema S., Ketelaars C., Kraijer D., MulderE., Volkmar F. et al. (2004) Interrelationship betweenAutism Diagnostic Observation Schedule-Generic(ADOS-G), Autism Diagnostic Interview-Revised (ADI-R), and the Diagnostic and Statistical Manual of MentalDisorders (DSM-IV-TR) classification in children andadolescents with mental retardation. Journal of Autismand Developmental Disorders 34, 129–37.
Bolton P. & Griffiths P. D. (1997) Association of tuberoussclerosis of temporal lobes with autism and atypicalautism. The Lancet 349, 392–5.
Bolton P., Macdonald H., Pickles A., Rios P., Goode S.,Crowson M. et al. (1994) A case–control family historystudy of autism. Journal of Child Psychology and Psychia-try and Allied Disciplines 35, 877–900.
868Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

Bolton P. F., Park R. J., Higgins J. N. P., Griffiths P. D. &Pickles A. (2002) Neuro-epileptic determinants ofautism spectrum disorders in tuberous sclerosiscomplex. Brain 125, 1247–55.
Bonati M. T., Russo S., Finelli P., Valsecchi M. R.,Cogliati F., Cavalleri F. et al. (2007) Evaluation ofautism traits in Angelman syndrome: a resource tounfold autism genes. Neurogenetics 8, 169–78.
Bregman J. D. & Volkmar F. R. (1988) Case study autisticsocial dysfunction and Down syndrome. Journal of theAmerican Academy of Child and Adolescent Psychiatry 27,440–1.
Brown W. T., Jenkins E. C., Cohen I. L., Fisch G. S.,Wolf-Schein E. G., Gross A. et al. (1986) Fragile X andautism: a multicenter survey. American Journal ofMedical Genetics 23, 341–52.
Budimirovic D. B., Bukelis I., Cox C., Gray R. M.,Tierney E. & Kaufmann W. E. (2006) Autism spectrumdisorder in Fragile X syndrome: differential contributionof adaptive socialization and social withdrawal. AmericanJournal of Medical Genetics 140A, 1814–26.
Capone G. T., Grados M. A., Kaufmann W. E., Bernad-Ripoll S. & Jewell A. (2005) Down Syndrome andComorbid Autism-Spectrum Disorder: characterizationusing the aberrant behavior checklist. American Journalof Medical Genetics 134A, 373–80.
Charman T. & Swettenham J. (2001) Repetitive behaviorsand social-communicative impairments in autism: impli-cations for developmental theory and diagnosis. In: TheDevelopment of Autism: Perspectives from Theory andResearch (eds J. A. Burack, T. Charman, N. Yirmiya &P. R. Zelazo), pp. 325–45. Lawrence Erlbaum Associates,New Jersey.
Charman T., Taylor E., Drew A., Cockerill H., Brown J.& Baird G. (2005) Outcome at 7 years of children diag-nosed with autism at age 2: predictive validity of assess-ments conducted at 2 and 3 years of age and pattern ofsymptom change over time. Journal of Child Psychologyand Psychiatry 46, 500–13.
Chawarska K., Klin A., Paul R. & Volkmar F. (2007)Autism spectrum disorder in the second year: stabilityand change in syndrome expression. Journal of ChildPsychology and Psychiatry 48, 128–38.
Chen C. H. & Hsiao K. J. (1989) A Chinese classic phe-nylketonuria manifested as autism. British Journal ofPsychiatry 155, 251–3.
Clayton-Smith J. & Pembrey M. E. (1992) Angelman syn-drome. Journal of Medical Genetics 29, 412–15.
Cohen I. L., Sudhalter V., Pfadt A., Jenkins E. C., BrownW. T. & Vietze P. M. (1991) Why are autism and theFragile X syndrome associated? Conceptual and meth-odological issues. American Journal of Human Genetics48, 195–202.
Constantino J. N., Gruber C. P., Davis S., Hayes S., Pas-sanante N. & Przybeck T. (2004) The factor structureof autistic traits. Journal of Child Psychology and Psychia-try 45, 719–26.
Cornish K., Turk J. & Levitas A. (2007) Fragile X Syn-drome and autism: common developmental pathways?Current Pediatric Reviews 3, 61–8.
Cornish K., Turk J. & Hagerman R. (2008) The fragile Xcontinuum: new advances and perspectives. Journal ofIntellectual Disability Research 52, 469–82.
Crino P. B., Nathanson K. L. & Henske E. P. (2006) TheTuberous Sclerosis complex. New England Journal ofMedicine 355, 1345–56.
Critchley M. & Earl C. J. (1932) Tuberouse Sclerosis andallied conditions. Brain 55, 311–46.
Davenport S. L. H., Hefner M. A. & Mitchell J. A. (1986)The spectrum of clinical features in CHARGE syn-drome. Clinical Genetics 29, 298–310.
Demark J. L., Feldman M. A. & Holden J. A. (2003)Behavioral relationship between autism and Fragile Xsyndrome. American Journal on Mental Retardation 108,314–26.
Dennis M., Lockyer L., Lazenby A. L., Donnelly R. E.,Wilkinson M. & Schoonheyt W. (1999) Intelligence pat-terns among children with high-functioning autism, phe-nylketonuria, and childhood head injury. Journal ofAutism and Developmental Disorders 29, 5–17.
DiLavore P. C., Lord C. & Rutter M. (1995) The pre-linguistic autism diagnostic observation schedule. Journalof Autism and Developmental Disorders 25, 353–79.
Dissanayake C., Bui Q., Bulhak-Paterson D., Huggins R.& Loesch D. (2009) Behavioural and cognitive pheno-types in idiopathic autism versus autism associated withfragile X syndrome. Journal of Child and Adolescent Psy-chology and Psychiatry 50, 290–9.
Dykens E. M. (2007) Psychiatric and behavioral disordersin persons with Down syndrome. Mental Retardation andDevelopmental Disabilities Research Reviews 13, 272–8.
Dykens E. M., Hodapp R. M. & Finucane B. M. (2000)Genetics and Mental Retardation Syndromes. Paul HBrookes Publishing Co, Baltimore.
Ehlers S. & Gillberg C. (1993) The epidemiology ofAsperger’s Syndrome: a total population study. Journalof Child Psychology and Psychiatry 34, 1327–80.
Fecteau S., Mottron L., Berthiaume C. & Burack J.(2003) Developmental changes of autistic symptoms.Autism: International Journal of Research and Practice 7,255–68.
Fernell E., Olsson V. A., Karlgren-Leitner C., Norlin B.,Hagber B. & Gillberg C. (1999) Autistic disorders inchildren with CHARGE association. DevelopmentalMedicine and Child Neurology 41, 270–2.
Fombonne E. (1999) The epidemiology of autism: areview. Psychological Medicine 29, 769–86.
Fombonne E., Du Mazaubrun C., Cans C. & GrandjeanH. (1997) Autism and associated medical disorders in aFrench epidemiological survey. Journal of the AmericanAcademy of Child and Adolescent Psychiatry 36, 1561–9.
869Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

Ghaziuddin M., Tsai L.Y. & Ghaziuddin N. (1992)Autism in Down’s syndrome: presentation and diagno-sis. Journal of Intellectual Disability Research 36, 449–56.
Gillberg C. & Coleman M. (2000) The Biology of theAutistic Syndromes, 3rd edn. McKeith Press, London.
Gillberg C., Pearson E., Grufman M. & Themner U.(1986) Psychiatric disorders in mildly and severely men-tally retarded urban children and adolescents: epidemio-logical aspects. British Journal of Psychiatry 149, 68–74.
Gillberg C., Gillberg I. C. & Ahlsen G. (1994) Autisticbehavior and attention deficits in tuberous sclerosis: apopulation-based study. Developmental Medicine andChild Neurology 36, 50–6.
Grant C. M., Apperly I. & Oliver C. (2007) Is Theory ofMind understanding impaired in males with Fragile Xsyndrome? Journal of Abnormal Child Psychology 35,17–28.
Gray K. M., Tongue B. & Sweeney D. J. (2008) Using theAutism Diagnostic Interview-Revised and the AutismDiagnostic Observation Schedule with young childrenwith developmental delay: evaluating diagnostic validity.Journal of Autism and Developmental Disorders 38, 657–67.
Gutierrez G., Smalley S. L. & Tanguay P. E. (1998)Autism in tuberous sclerosis complex. Journal of Autismand Developmental Disorders 28, 97–103.
Hagerman J., Jackson A. W., Levitas A., Rimland B. &Braden M. (1986) An analysis of autism in fifty maleswith the fragile x syndrome. American Journal of MedicalGenetics 23, 359–74.
Hagerman R. J., Ono M.Y. & Hagerman P. J. (2005)Recent advances in fragile X: a model for autism andneurodegeneration. Current Opinion in Psychiatry 18,490–6.
Hall S., de Bernardis M. & Reiss A. (2006) Social EscapeBehaviours in Individuals with Fragile X Syndrome.Journal of Autism and Developmental Disorders 36, 935–47.
Harrison J. E. & Bolton P. F. (1997) Annotation: TuberousSclerosis. Journal of Child Psychology and Psychiatry andAllied Disciplines 38, 603–14.
Hartshorne T. S., Grialou T. L. & Parker K. R. (2005)Autistic-like behavior in CHARGE syndrome. AmericanJournal of Medical Genetics 133A, 248–56.
Hatton D. D., Sideris J., Skinner M., Mankowski J., BaileyD. B., Roberts J. et al. (2006) Autistic behavior in chil-dren with fragile X syndrome: prevalence, stability, andthe impact of FMRP. American Journal of MedicalGenetics 140A, 1804–13.
Hippolyte L., Barisnikov K. & van der Linden M. (2008)Face processing and facial emotion recognition in adultswith Down syndrome. American Journal on MentalRetardation 113, 292–306.
Howlin P. (2000) Autism and intellectual disability: diag-nostic and treatment issues. Journal of the Royal Societyof Medicine 93, 351–5.
Howlin P. (2002) Autism related disorders. In: BehaviouralPhenotypes in Clinical Practice, 2nd edn. (ed. G.O’Brien), pp. 31–43. Cambridge University Press,Cambridge.
Howlin P., Wing L. & Gould J. (1995) The recognition ofautism in children with Down syndrome: implicationsfor intervention and some speculations about pathology.Developmental Medicine and Child Neurology 37,398–414.
Humphrey A., Neville B. G. R., Clarke A. & Bolton P. F.(2006) Autistic regression associated with seizure onsetin an infant with tuberous sclerosis. Developmental Medi-cine and Child Neurology 48, 609–11.
Hunt A. & Shepherd C. (1993) A prevalence study ofautism in Tuberous Sclerosis. Journal of Autism andDevelopmental Disorders 23, 323–39.
Issekutz K. A., Graham J. M., Prasad C., Smith I. M. &Blake K. D. (2005) An epidemiological analysis ofCHARGE syndrome: preliminary results from a Cana-dian study. American Journal of Medical Genetics 133A,309–17.
Jambaque I., Cusmai R., Curatolo P., Cortesi F., Perrot C.& Dulac O. (1991) Neuropsychological aspects ofTuberous Sclerosis in relation to epilepsy and MRI find-ings. Developmental Medicine and Child Neurology 33,698–705.
Jeste S. S., Sahin M., Bolton P., Ploubidis G. B. & Hum-phrey A. (2008) Characterization of autism in youngchildren with tuberous sclerosis complex. Journal ofChild Neurology 23, 520–5.
Johansson M., Rastam M., Billstedt E., Danielsson S.,Stromland K., Miller M. et al. (2006) Autism spectrumdisorders and underlying brain pathology in CHARGEassociation. Developmental Medicine and Child Neurology48, 40–50.
Kanner L. (1943) Autistic disturbances of affectivecontact. Nervous Child 2, 217–50.
Kau A. S. M., Tierney E., Bukelis I., Stump M. H., KatesW. R., Trescher W. H. et al. (2004) Social behaviorprofile in young males with Fragile X syndrome: charac-teristics and specificity. American Journal of MedicalGenetics 126, 9–17.
Kaufmann W. E., Cortell R., Kau A. S. M., Bukelis I.,Tierney E., Gray R. M. et al. (2004) Autism spectrumdisorder in Fragile X syndrome: communication, socialinteraction and specific behaviors. American Journal ofMedical Genetics 129, 225–34.
Kent L., Evans J., Paul M. & Sharp M. (1999) Comorbid-ity of autistic spectrum disorder in children with Downsyndrome. Developmental Medicine and Child Neurology41, 158.
Kerby D. S. & Dawson B. L. (1994) Autistic features,personality, and adaptive-behavior in males with thefragile-x syndrome and no autism. American Journal onMental Retardation 98, 455–62.
870Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

Kerr A. M., Belichenko P., Woodcock T. & Woodcock M.(2001) Mind and brain in Rett disorder. Brain andDevelopment S1, 44–9.
Kerr A. M., Archer H. L., Evans J. C., Prescott R. J. &Gibbon F. (2006) People with MECP2 mutation-positive Rett disorder who converse. Journal of Intellec-tual Disability Research 50, 386–94.
Kozinetz C. A., Skender M. L., MacNaughton N., AlmesM. J., Schultz R. J., Percy A. K. et al. (1993) Epidemiol-ogy of Rett syndrome: a population-based registry. Pedi-atrics 91, 445–50.
Krug D. A., Arick J. & Almond P. (1980) Behavior check-list for identifying severely handicapped individuals withhigh levels of autistic behaviour. Journal of Child Psychol-ogy and Psychiatry 21, 221–9.
Kuijpers H. J. H., van der Heijden F. M. M. A., Tuinier S.& Verhoeven W. M. A. (2007) Hereditary hemorrhagictelangiectasia and psychopathology. Journal of Neuropsy-chiatry and Clinical Neurosciences 19, 199–200.
Kyllerman M. (1995) On the prevalence of Angelman syn-drome. American Journal of Medical Genetics 59, 405.
La Malfa G., Lassi S., Bertelli M., Salvini R. & PlacidiG. F. (2004) Autism and intellectual disability: a studyof prevalence on a sample of the Italian population.Journal of Intellectual Disability Research 48,262–7.
Lesniak-Karpiak K., Mazzocco M. M. M. & Ross J. L.(2003) Behavioral assessment of social anxiety infemales with Turner or fragile X syndrome. Journal ofAutism and Developmental Disorders 33, 55–67.
Levitas A., Hagerman R. J., Braden M., Rimland B.,Mcbogg P. & Matus I. (1983) Autism and the Fragile-Xsyndrome. Journal of Developmental and BehavioralPediatrics 4, 151–8.
Lewis P., Abbeduto L., Richmond E., Giles N., Bruno L.& Schroeder S. (2006) Cognitive, language and social-cognitive skills of individuals with fragile X syndromewith and without autism. Journal of Intellectual DisabilityResearch 50, 532–42.
Loesch D. Z., Bui Q. M., Dissanayake C., Clifford S.,Gould E. et al. (2007) Molecular and cognitive predic-tors of the continuum of autistic behaviours in FragileX. Neuroscience and Biobehavioral Reviews 31, 315–26.
Lord C. (1995) Follow-up of two-year-olds referred forpossible autism. Journal of Child Psychology and Psychia-try 36, 1365–82.
Lord C., Rutter M. & Le Couteur A. (1994) AutismDiagnostic Interview-Revised: a revised version of adiagnostic interview for caregivers of individuals withpossible pervasive developmental disorders. Journal ofAutism and Developmental Disorders 24, 359–85.
Lord C., Rutter M., DiLavore P. C. & Risi S. (2000) TheAutism Diagnostic Observation Schedule (ADOS).Western Psychological Services, Los Angeles.
Lord C., Risi S., DiLavore P., Shulman C., Thurm A. &Pickles A. (2006) Autism from 2 to 9 years of age.Archives of General Psychiatry 63, 694–701.
Lowe T. L., Tanaka K., Seashore M. R., Young J. G. &Cohen D. J. (1980) Detection of phenylketonuria inautistic and psychotic children. Journal of the AmericanMedical Association 243, 126–8.
Lowenthal R., Paula C. S., Schwartzman J. S., Brunoni D.& Mercadante M. T. (2007) Prevalence of pervasivedevelopmental disorders in Down’s syndrome. Journal ofAutism and Developmental Disorders 37, 1394–5.
Lund J. (1988) Psychiatric aspects of Down’s syndrome.Acta Psychiatrica Scandinavica 78, 369–74.
Mazzocco M. M., Kates W. R., Baumgardener T. L.,Freund L. S. & Reiss A. L. (1997) Autistic behaviorsamong girls with Fragile X syndrome. Journal of Autismand Developmental Disorders 27, 415–33.
Morton J. & Frith U. (1994) Causal modeling: a structuralapproach to developmental psychopathology. In:Manual of Developmental Psychopathology (eds D.Cicchetti & D. J. Cohen), pp. 357–89. John Wiley, NewYork.
Mount R. H., Hastings R. P., Reilly S., Cass H. &Charman T. (2003a) Towards a behavioral phenotypefor Rett syndrome. American Journal on Mental Retarda-tion 1, 1–12.
Mount R. H., Charman T., Hastings R. P., Reilly S. &Cass H. (2003b) Features of autism in Rett syndromeand severe mental retardation. Journal of Autism andDevelopmental Disorders 33, 435–42.
Naidu S., Hyman S., Piazza K., Savedra J., Perman J.,Wenk G. et al. (1990) The Rett syndrome: progressreport on studies at the Kennedy-Institute. Brain &Development 12, 5–7.
Neul J. L., Fang P., Barrish J., Lane J., Caeg E. B., SmithE. O. et al. (2008) Specific mutations in Methyl-CpG-Binding Protein 2 confer different severity in Rett syn-drome. Neurology 70, 1313–21.
Nomura Y. & Segawa M. (2005) Natural history of Rettsyndrome. Journal of Child Neurology 20, 764–8.
O’Callaghan F. J. K. (1999) Tuberous sclerosis. BritishMedical Journal 318, 1019–20.
Park R. J. & Bolton P. F. (2001) Pervasive developmentaldisorder and obstetric complications in children andadolescents with tuberous sclerosis. Autism: InternationalJournal of Research and Practice 5, 237–48.
Persico A. M. & Bourgeron T. (2006) Searching for waysout of the autism maze: genetic, epigenetic and environ-mental clues. Trends in Neuroscience 29, 349–58.
Peters S. U., Beaudit A. L., Madduri N. & Bacino C. A.(2004) Autism in Angelman syndrome: implications forautism research. Clinical Genetics 66, 530–6.
Piven J., Harper J., Palmer P. & Arndt S. (1996) Course ofbehavioral change in autism: a retrospective study of
871Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

high-IQ adolescents and adults. Journal of the AmericanAcademy of Child and Adolescent Psychiatry 35, 523–9.
Povey S., Burley M. W., Attwood J., Benham F., Hunt D.,Jeremiah S. J. et al. (1994) Two loci for Tuberous Scle-rosis – one on 9q34 and one on 16p13. Annals of HumanGenetics 58, 107–27.
Prather P. & de Vries J. P. (2004) Behavioral and cognitiveaspects of tuberous sclerosis complex. Journal of ChildNeurology 19, 666–74.
Reiss A. L. & Freund L. S. (1990) Fragile X syndrome,DSM-III-R and autism. Journal of the American Academyof Child and Adolescent Psychiatry 29, 885–91.
Reiss A. L., Feinstein C. & Rosenbaum K. N. (1986)Autism and genetic disorders. Schizophrenia Bulletin 12,724–38.
Reiss S. S., Levitan G. W. & Szyszko J. (1982) Emotionaldisturbance and mental retardation: diagnostic over-shadowing. American Journal on Mental Deficiency 86,567–74.
Rett A. (1966) Uber ein eigenartiges hirnatrophischessyndrom bei Hyperammonamie im Kindesalter. WeinMedWochenschr 116, 723–38.
Ring H., Woodbury-Smith M., Watson P., Wheelwright S.& Baron-Cohen S. (2008) Clinical heterogeneity amongpeople with high functioning autism spectrum condi-tions: evidence favouring a continuous severity gradient.Behavioral and Brain Functions 4, 1744–9081.
Roberts J. E., Weisenfeld L. A. H., Hatton D. D.,Heath, M. & Kaufmann W. E. (2007) Social approachand autistic behavior in children with fragile x syndrome.Journal of Autism and Developmental Disorders 37, 1748–60.
Rogers S. J. & Newhart-Larson S. (1989) Characteristicsof infantile autism in five children with Leber’s congeni-tal amaurosis. Developmental Medicine and Child Neurol-ogy 31, 598–608.
Ronald A., Happe F., Price T. S., Baron-Cohen S. &Plomin R. (2006) Phenotypic and genetic overlapbetween autistic traits at the extremes of the generalpopulation. Journal of the American Academy of Child andAdolescent Psychiatry 45, 1206–14.
Rutter M., Bailey A., Bolton P. & LeCouteur A. (1994)Autism and known medical conditions: myth and sub-stance. Journal of Child Psychology and Psychiatry 35,311–22.
Rutter M., Bailey A., Lord C. & Berument S. K. (2003a)The Social Communication Questionnaire. Western Psy-chological Services, Los Angeles.
Rutter M., LeCouteur A. & Lord C. (2003b) AutismDiagnostic Interview- Revised (ADI-R). Western Psycho-logical Services, Los Angeles.
Sabaratnam M., Turk J. & Vroegop P. (2000) Case report:autistic disorder and chromosomal abnormality 46, XXduplication (4) p12-p13. European Child & AdolescentPsychiatry 9, 307–11.
Sabaratnam M., Murthy N. V., Wijeratne A., BuckinghamA. & Payne S. (2003) Autistic-like behaviour profile andpsychiatric morbidity in Fragile X Syndrome: a prospec-tive ten-year follow-up study. European Child & Adoles-cent Psychiatry 12, 172–7.
Sandberg A. D., Ehlers S., Hagberg B. & Gillberg C.(2000) The Rett syndrome complex: communicativefunctions in relation to developmental level. Autism:TheInternational Journal of Research and Practice 4,249–67.
Schopler E., Reichller R. & Renner B. R. (1988) TheChildhood Autism Rating Scale (CARS). Western Psycho-logical, Los Angeles.
Scriver C. R., Eisensmith R. C., Woo S. L. C. & Kauf-mann S. (1994) The hyperphenylalaninemias of manand mouse. Annual Review of Genetics 28, 141–65.
Skuse D. H. (2007) Rethinking the nature of genetic vul-nerability to autistic spectrum disorders. Trends in Genet-ics 23, 387–95.
Smalley S. L. (1998) Autism and Tuberous Sclerosis.Journal of Autism and Developmental Disorders 28, 407–14.
Smalley S. L., Tanguay P. E., Smith M. & Gutierrez G.(1992) Autism and Tuberous Sclerosis. Journal of Autismand Developmental Disorders 22, 339–55.
Smeets E., Terhal P., Casaer P., Peters A., Midro A.,Schollen E. et al. (2005) Rett syndrome in females withCTS hot spot deletions: a disorder profile. AmericanJournal of Medical Genetics 132, 117–20.
Smith I. M., Nichols S. L., Issekutz K. & Blake K. (2005)Behavioral profiles and symptoms of autism inCHARGE syndrome: preliminary Canadian epidemio-logical data. American Journal of Medical Genetics 133A,248–56.
Spiker D., Lotspeich L. J., Dimiceli S., Myers R. M. &Risch N. (2002) Behavioral phenotypic variation inautism multiplex families: evidence for a continuousseverity gradient. American Journal of Medical Genetics114, 129–36.
Starr E. M., Berument S. K., Tomlins M., PapanikolaouK. & Rutter M. (2005) Brief report: autism in individu-als with Down syndrome. Journal of Autism and Develop-mental Disorders 35, 665–73.
Steiner C. E., Acosta A. X., Guerreiro M. M. & Marques-De-Faria A. P. (2007) Genotype and natural history inunrelated individuals with phenylketonuria and autisticbehaviour. Arquivos de Neuro-Psiquiatria 65, 202–5.
Sudhalter V., Cohen I. L., Silverman W. & WolfscheinE. G. (1990) Conversational analyses of males withfragile X, Down syndrome, and autism: comparison ofthe emergence of deviant language. American Journal onMental Retardation 94, 431–41.
Trillingsgaard A. & Østergaard J. R. (2004) Autism inAngelman syndrome: an exploration of comorbidity.Autism: International Journal of Research and Practice 8,163–74.
872Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd

Tsai L.Y. (1992) Is Rett syndrome a subtype of pervasivedevelopmental disorders. Journal of Autism and Develop-mental Disorders 22, 551–61.
Turk J. (1992) The Fragile X syndrome: on the way to abehavioural phenotype. British Journal of Psychiatry 160,24–35.
Turk J. & Cornish K. (1998) Face recognition andemotion perception in boys with fragile-X syndrome.Journal of Intellectual Disability Research 42, 490–9.
Turk J. & Graham P. (1997) Fragile X syndrome andautistic features. Autism: International Journal of Researchand Practice 1, 199–214.
Van Acker R. (1997) Rett syndrome: a pervasive develop-mental disorder. In: Handbook of Autism and PervasiveDevelopmental Disorders (eds D. J. Cohen & F. R.Volkmar), pp. 60–93. John Wiley & Sons, Inc, New York.
Ventola P. E., Kleinman J., Pandey J., Barton M., Allen S.,Green J.et al. (2006) Agreement among four diagnosticinstruments for autism spectrum disorders in toddlers.Journal of Autism and Developmental Disorders 36, 839–47.
Vissers L. E. L. M., van Ravenswaaij C. M. A., AdmiraalR., Hurst J. A., de Vries B. B. A., Janssen I. M. et al.(2004) Mutations in a new member of the chromo-domain gene family cause CHARGE syndrome. NatureGenetics 36, 955–7.
de Vries P. J. & Howe C. J. (2007) The tuberous sclerosiscomplex proteins – a GRIPP on cognition and neurode-velopment. Trends in Molecular Medicine 13, 319–26.
de Vries P. J., Hunt A. & Bolton P. (2007) The psycho-pathologies of children and adolescents with tuberoussclerosis complex (TSC): a postal survey of UK fami-lies. European Child and Adolescent Psychiatry 16, 16–24.
Wachtel L. E. & Hartshorne T. S. (2006) Portraits inCHARGE: similarities and variability in the CHARGEsyndrome behavioural phenotype as exemplified by eightindividuals. Journal of Intellectual Disability Research 50,799.
Wakabayashi S. (1979) Case of infantile-autism associatedwith Down’s syndrome. Journal of Autism and Develop-mental Disorders 9, 31–6.
Walz N. C. (2007) Parent report of stereotyped behaviors,social interaction, and developmental disturbances inindividuals with Angelman Syndrome. Journal of Autismand Developmental Disorders 37, 940–7.
Walz N. C. & Benson B. A. (2002) Behavioral phenotypesin children with Down syndrome, Prader-Willi syn-drome, or Angelman syndrome. Journal of Developmentaland Physical Disabilities 14, 307–21.
Webb D. W., Clarke A., Fryer A. & Osborne J. P. (1996)The cutaneous features of tuberous sclerosis: a popula-tion study. British Journal of Dermatology 135, 1–5.
Williamson D. A. & Bolton P. (1995) Brief report: atypicalautism and tuberous sclerosis in a sibling pair. Journal ofAutism and Developmental Disorders 25, 435–42.
Wing L. (1980) Schedule of Handicaps, Behaviour andSkills. Medical Research Council, London.
Wishart J. G. (2007) Socio-cognitive understanding: astrength or a weakness in Down’s syndrome? Journal ofIntellectual Disability Research 51, 996–1005.
Wishart J. G., Cebula K. R., Willis D. S. & Pitcairn T. K.(2007) Understanding of facial expressions of emotionby children with intellectual disabilities of differing aeti-ology Journal of Intellectual Disability Research 51, 551–63.
Witt-Engerstrom I. & Gillberg C. (1987) Rett Syndromein Sweden. Journal of Autism and Developmental Disorders17, 149–50.
Wong V. (2006) Study of the relationship between tuber-ous sclerosis complex and autistic disorder. Journal ofChild Neurology 21, 199–204.
World Health Organisation (1992) The ICD-10 Classifica-tion of Mental and Behavioral Disorders: Clinical Descrip-tions and Diagnostic Guidelines. World HealthOrganisation, Geneva.
Yalaz K., Vanli L., Yilmaz E., Tokatli A. & Anlar B.(2006) Phenylketonuria in pediatric neurology practice:a series of 146 cases. Journal of Child Neurology 21, 987–90.
Young D. J., Bebbington A., Anderson A., Ravine D.,Ellaway C., Kulkarni A. et al. (2008) The diagnosis ofautism in a female: could it be Rett Syndrome? Euro-pean Journal of Pediatrics 167, 661–9.
Zappella M., Gillberg C. & Ehlers S. (1998) The pre-served speech variant: a subgroup of the Rett complex:a clinical report of 30 cases. Journal of Autism and Devel-opmental Disorders 28, 519–26.
Zappella M., Meloni I., Longo I., Hayek G. & Renieri A.(2001) Preserved speech variants of the Rett syndrome:molecular and clinical analysis. American Journal ofMedical Genetics 104, 14–22.
Zelazo P. D., Burack J., Benedetto E. & Frye D. (1996)Theory of Mind and rule use in individuals withDown’s syndrome: a test of the uniqueness and specific-ity claims. Journal of Child Psychology and Psychiatry andAllied Disciplines 37, 479–84.
Zhao X., Leotta A., Kustanovich V., Lajonchere C. &Geschwind D. H. et al. (2007) A unified genetic theoryfor sporadic and inherited autism. Proceedings of theNational Academy for Sciences of the United States ofAmerica 104, 12831–6.
Accepted 8 July 2009
873Journal of Intellectual Disability Research volume 53 part 10 october 2009
J. Moss & P. Howlin • ASD in genetic syndromes
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd



















