Embed Size (px)
Citation preview

Autism: Integrating a Personal Perspective with Music Therapy Practice
DIANE A. TOIGO Wassaic Developmental Center, Wassaic, New York
ABSTRACT: This article seeks to combine the insights of Dr. Temple Grandin with current music therapy practice. Dr. Grandin was diagnosed as having autism as a child but went on to earn a doctorate in Animal Science. She has been a member of the Board of Directors of the Autism Society of America and has written and lectured extensively. She is supportive of music therapy and recommends it in her writings. Dr. Grandin’s views about the experience of autism, the causes of autism, and the treatment of autism are summarized. Ways in which these insights can be applied to music therapy practice are then discussed.
As therapists, we are engaged in the process of trying to
understand our clients’ inner worlds. This has been particu
larly difficult for people with autism because their experience
is so different from ours and because the limitations imposed
by the disability itself prevent the sharing of the experience
of autism. Because the world of the person with autism has
been so inaccessible, the insights of Dr. Temple Grandin, a
woman who was diagnosed as having autism, are particularly
valuable.
Grandin was a featured speaker at a seminar on autism at
tended by the author in 1989 (Grandin, 1989b). This presen
tation and her many writings provide a comprehensive picture
of her experiences as a person with autism. She was able to
overcome her disability, earned a doctorate in Animal Sci
ence, and has successfully designed livestock handling facil
ities worldwide (Grandin & Scariano, 1986). Grandin has been
on the Board of Directors of the Autism Society of America,
has toured facilities for individuals with autism throughout
the world, and has written and lectured extensively about
autism. Her articles have been published in numerous pro
fessional journals. Although her experience cannot be con
strued as being representative of the experiences of every
person with autism, she does provide a fascinating look into
the world of an individual with autism. In describing her child
hood Grandin (1988b) wrote:
At the age of 11/2 to 3 I had many of the standard autistic behaviors such as fixation an spinning objects, refusing to be touched or held, preferring to be alone, destructive behavior, temper tantrums, inability to speak, sensitivity to sudden noises, appearance of deafness, and an intense interest in odors. (p. 144)
She had many of the symptoms of autism found on the Rim
land checklist and would have scored +9 at the age of 11/2
(Rimland, 1971; Grandin, 19886). She had trouble with face
recognition and feared physical contact: “As a child I wanted
to feel the comfort of being held, but then I would shrink
away for fear of losing control and being engulfed when peo
ple hugged me” (Grandin, 1988b, p. 151). Avoidance of con
tact was caused by overstimulation, not anger or fear. Activ
ities such as having her hair combed or her teeth brushed
could be excruciatingly painful (Grandin, 1990). As is true with
many people with tactile defensiveness, Grandin has always
craved deep pressure. She noted, “I liked intense stimulation
when I was young. Maybe the desire for intense stimulation
is what causes some autistic children to self-mutilate” (Gran
din, 1988b, p. 166). In contrast, light touch and clothing could
be extremely painful.
Grandin (1988a) also had significant problems handling au
ditory stimuli:
The most common sensory difficulties occur with the auditory and tactile senses. Noise was a major problem for me. When I was confronted with loud or confusing noise, I could not modulate it. I either had to shut it all out and withdraw, or let it all in like a freight train. To avoid its onslaught, I would often withdraw and shut the world out. (p. 3)
Motoric noises were particularly painful, and screening
background noises was so difficult that she was functionally
deaf in noisy situations. Overresponsiveness to auditory and
tactile stimuli was frequently the cause of violent behavior,
and high levels of arousal also increased her tendency to fixate
(Grandin, 1988b).
Language presented great problems. She understood ev
erything that people said to her but could respond only by
screaming and flapping her hands (Grandin, 1988b). The fol
lowing remarks illuminate the nature of her language prob
lem: “Sometimes I heard and understood and other times
sounds or speech reached my brain like the unbearable noise
of an onrushing freight train” (Grandin & Scariano, 1986, p.
149) and “I had the words I wanted to say in my mind, but I
just could not get them out; it was like a big stutter” (Grandin,
1988a, p. 2). Interestingly, in times of emotional stress or fever
she could sometimes speak normally (1988b).
Grandin (1988a) also reported specific learning difficulties.
Describing herself as a visual thinker she wrote:
I do not remember non-visual information. Abstract concepts such as Betting along with people have to have a visual image. For example, my visual image for relationships with people is a sliding glass door. If you push on it too hard it will break. To make the abstract concept more real, I would
13
at Colum
bia University L
ibraries on Novem
ber 27, 2014http://m
tp.oxfordjournals.org/D
ownloaded from

14
sometimes act it out-for example, by walking through a real sliding door. (p. 7)
Music Therapy Perspectives (1992), Vol. 10
sensory receptors, and insist on an unchanging environment”
(Kootz, Marineuin, & Cohen cited in Grandin, 1988b, p. 156).
Grandin (1988b) believed that damage to the central ner
vous system can create a deprived environment. In describing
her own experience, she (1989a) noted that pulling away from
her environment kept her from receiving stimulation which
was required for normal development. This presents the in
triguing idea that brain damage may be both cause and effect
of autism as the child with autism avoids the very stimulation
that is necessary for normal development. In describing the
effect this could have on relationships with people Grandin
& Scariano (1986) wrote:
The original fetal defect in brain development is probably responsible for the baby’s avoidance of being touched and comforted. The longer a baby lives without experiencing the feeling of being comforted, the more likely the brain circuits involved in the development of emotional contact with people will be damaged. (p. 177)
She noted that many studies have confirmed the visual spatial
nature of theautistic mind (Hermelin, and Lockyer and Rutter,
cited in Grandin 1988a). Memorizing nonvisual material was
impossible for her, and melodies were the only things she
could memorize without a visual image (Grandin, 19886). Be
cause her mind was completely visual, Grandin had difficulty
with sequential tasks, such as math, which cannot easily be
visualized.
In summarizing how a person with autism might think Gran
din (1988b) wrote:
There may be two basic kinds of thinking, visual and sequential. Society needs to recognize the value of people who think visually. Misinterpretation of psychological test results could label a brilliant visual thinker as below average in intelligence. Einstein was a visual thinker who failed his high school language requirement and relied on visual methods of study. (p. 147)
Additional learning difficulties occurred because she had sig
nificant gaps in attention, analogous to reality fading in and
out as if controlled by an on/off switch (19896).
Both as a child and as an adult, Grandin was tested exten
sively with very interesting results. The Weschler IQ test, ad
ministered at ages 9 and 12, yielded scores of 120 and 137
respectively (Grandin, 19886). On other tests her scores ranged
from the 6th percentile to the 95th percentile and from the
second-grade level to above the ceiling of the test (for visual
spatial ability). In summarizing the test results, Grandin (1988b)
wrote, “My difficulties on many of the subtests stemmed from
the inability to hold one piece of information in my mind
while I manipulated another piece of information” (p. 147).
She suffered a setback when she reached puberty and had
bouts of impulsive behavior and severe “stage fright.” She
attributes this to the increase in norepinephrine activity in
the brain which occurs at puberty (Grandin, 1988b).
Grandin (1986) managed, in large part, to overcome these
deficits. For this recovery she credited early intervention,
structured programs, a mechanical device she invented to
lessen tactile defensiveness (discussed further in this article),
loving parents, teachers, and friends, and the antidepressant
drug, Tofranil.
The Causes of Autism
Grandin & Scariano (1986) believed that autism may be caused
by many different kinds of brain damage and said, “It may be
like a TV with a poor picture. Damage to any one of many
parts in the tuning circuit would ruin the picture quality” (p.
174). Many instances of autism might be due to a hyperex
citable central nervous system which cannot integrate incom
ing stimuli effectively (Grandin, 1988b). There is an overre
sponsiveness to some stimuli and an undersensitivity to other
stimuli (Ayres, 1979). Faced with a constantly changing world
that cannot be understood, the child with autism avoids stim
ulation and might resort to self-stimulatory behavior to “flood
Grandin (1988b) noted that institutionalized babies develop
many autistic characteristics as they strive to adapt to their
state of sensory and emotional deprivation and that excessive
self-stimulation often occurs. Studies by Prescott (cited in
Grandin, 1988b) found that absence of tactile stimulation will
cause hyperactivity, autistic behavior, violence, and aggression
and concluded that these behaviors may be related to inad
equate sensory stimulation. Grandin (1989a) also referred to
the work of Dr. Fein who believed that the lack of sensory
input early in the lives of children with autism deprives them
of the perceptual experiences necessary to form the building
blocks for higher skills such as language.
Grandin & Scariano (1986, 1989b) aIso has delved extensively
into the kinds of brain damage that might cause autism. In
summarizing her views, she has hypothesized that the original
brain damage is compounded as the child with autism fails to
receive adequate stimulation due to a failure to pay attention,
or due to withdrawal to block out an onslaught of painful or
confusing stimuli. Continuing hyperactivity and stereotypic
behaviors could damage the brain further and have been shown
to alter the brain at the dendritic level.
Specific brain abnormalities have also been identified. The
cerebellum acts as a sensory modulator, and Grandin’s cer
ebellum is 20% smaller than normal (Grandin, 1989b). Cere
bella abnormalities could explain overreaction to touch,
nervousness, and overarousal problems (Grandin, 1989a;
Grandin & Scariano, 1986).
Damage to the reticular activating system could account for
overresponsiveness to stimuli, and problems with sensory in
tegration could be partially responsible for damaging the hip
pocampus or other brain areas (Luria, cited in Grandin, 1988b).
Reisman (cited by Grandin, 1988b) found that since the hip
pocampus receives input from all sensory systems, lesions in
this area might cause distractability, immediate response to a
stimulus, or fixation on a stimulus. Grandin (1989b) also be
lieved that autism could be caused by damage to the amygdala
or the lymbic system, which regulates emotional responses.
at Colum
bia University L
ibraries on Novem
ber 27, 2014http://m
tp.oxfordjournals.org/D
ownloaded from

Autism and Music Therapy
Abnormalities in brain chemistry such as excessive amounts
of endorphins (Panksepp, cited in Grandin, 1988b) also may
play a role. Stereotyped behavior might serve initially to calm
the individual by producing endorphins but persists because
it is pleasurable and produces an endorphin “high.”
In summary, there is considerable evidence that autism may
be caused by diverse kinds of brain damage which, in turn,
lead to problems handling sensory input. This could cause the
child with autism to withdraw, and brain damage could be
compounded as the brain is denied the stimulation necessary
for normal development.
The Treatment of Autism
In their fascinating book, Emergence: Labeled Autistic, Gran
din concluded, “A good program should have flexible non
aversive behavior modification, sensory treatment, speech
therapy, exercise, and music therapy” (Grandin & Scariano,
1986, p. 184). She has visited treatment program worldwide
and has seen many diverse treatment approaches work ef
fectively. In summarizing her views she wrote, “In many in
stances the real magic that makes a program effective is early
intense intervention in a structured environment, meaningful
contact with normal children, and plenty of structured phys
ical activity” (Grandin, 1988a, p. 1). Most of her treatment
recommendations involve structured educational programs,
sensory treatment, and selective use of medication.
Grandin & Scariano (1986) favors trying other approaches
before resorting to medication and said, “Giving a child med
ication often just masks a symptom, but finding the right drug
which actually corrects or compensates for faulty biochem
istry is very useful” (p. 149). She also noted, “There are many
different autism subtypes, and the brain abnormalities that
cause each subtype may be different. A medicine that works
for one subtype may be useless for another” (Grandin, 1990,
p. 11).
Grandin (19896) was helped significantly by the anti-de
pressant drug Tofranil (Imipramine), which she believes acted
to calm the nervous circuit and elevate the mood circuit. She
received some relief immediately after starting on the drug,
while other changes, such as development of a sense of hu
mor, took years. Grandin (1988b) cited a study by Campbell
et al. which examined the effects of lmipramine in children
with autism or schizophrenia. The drug affected five children
negatively while three children markedly improved, leading
Campbell to conclude that the drug merited further study in
children who are mute and who have autism, developmental
disabilities, and little psychotic symptomatology.
Dr. Paul Hardy successfully treated adolescents with autism
with different types of antidepressant drugs (Grandin & Scari
ano, 1986). In his presentation, “The Use of Alternative Med
ication to Treat Aggression and Self Injury,” Dr. Ratey (1989),
Assistant Director of Psychiatry at Harvard, spoke of his suc
cess using beta-blockers for aggression and self-injury. He
noted that a state of hyperarousal often leads to social isola
tion, reliance on repetition, violent behavior, self-injurious
behavior, and impulsive acts. Beta-blockers, developed to treat
15
high blood pressure, do not have the many negative side
effects, such as drowsiness and cognitive problems, associated
with neuroleptics, major tranquilizers, and benzodiazepines.
A study by Ratey (cited in Grandin, 1988b) concluded that
beta-blockers greatly reduced aggressive behavior in some
adults with autism. In addition, positive behaviors such as lan
guage skills, social skills, and sense of humor have increased
(Ratey, 1989). Ratey (1989) hypothesized that beta-blockers
may create a “pharmacological holding environment,” and
that they may also create “an optimal level of arousal for
learning.”
Grandin (1988a) also strongly supported sensory treatment
which is an area that is often overlooked:
Sensory methods of reducing nervous system arousal and physical activity should be used before a child is Put on drugs.. Prescribing drugs for young children should be avoided if possible. Sensory treatment in conjunction with traditional behavioral approaches is probably more effective than behavioral methods alone. (p. 5)
She particularly emphasized the importance of vestibular, tac
tile, and kinesthetic stimulation because these systems start
to develop first after birth (Moore, cited in Grandin, 19886).
and their dysfunction may be responsible for strange senso
riomotor behavior in children with autism (Ornitz, cited in
Grandin, 1988b). Grandin supported the sensory integration
theory developed by Ayres (1979) and noted, “Sensory inte
gration therapy is based on the concept that stimulation of
the vestibular system and other sense modalities will help the
immature or damaged nervous system to develop” (Grandin,
1988b, p. 160). Both human and animal studies have found
that deep pressure is calming (Grandin, 1989a), and vestibular
and tactile stimulation are used very naturally by parents in
soothing their children.
Grandin (1989a) grew up with animals and believed that the
reaction of an untamed animal to touch is similar to the re
action of a child with autism. She saw good results through
sensory treatment achieved in less than an hour of treatment
per day (Grandin, 1989a), and gives the following advice:
Therapists have helped many autistic children by gently applying tactile and vestibular stimulation (Ayres, 1979; King, cited in Grandin, 1989a). One effect of this stimulation is to desensitize the tactile system. This is not a cure, but it has increased speech, affection, and eye contact in some children. It also helps to decrease stereotypical and self-injurious behavior. The sensory activities are done gently as fun games and are never forced. Strong encouragement and some intrusiveness may be used but a good therapist knows how far she can intrude before the stimulation becomes so overwhelming that the child starts crying. (Grandin, 19094 p. 75)
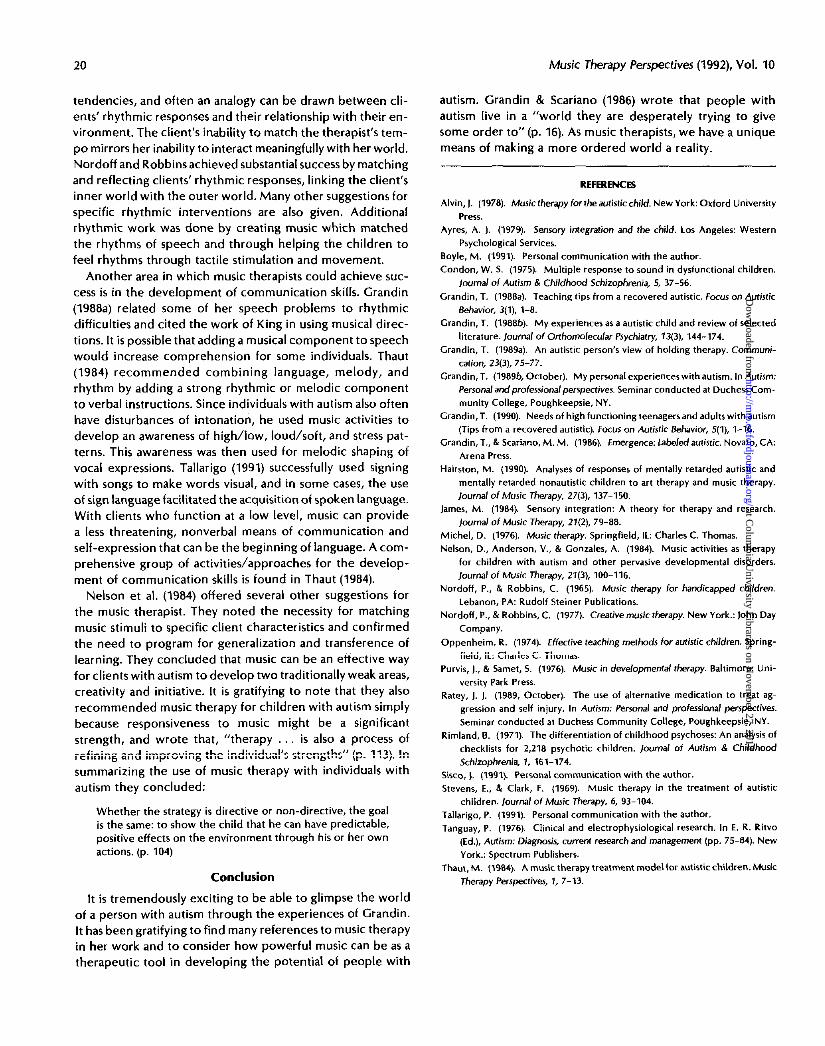
A unique form of sensory treatment Grandin (19886) de
vised is the squeeze machine. She came upon this idea by
spending time at an aunt’s ranch where she observed that
“the cattle sometimesappeared to relax when they were held
in the squeeze chute, a device for holding cattle for veterinary
procedures.. After a horrible bout of the ‘nerves’ I got in
the squeeze chute”(p. 5). She designed the squeeze machine,
later describing it as:
at Colum
bia University L
ibraries on Novem
ber 27, 2014http://m
tp.oxfordjournals.org/D
ownloaded from

Music Therapy Perspectives (1992), Vol. 10
Figure 1. Squeeze machine
completely lined with foam rubber. It squeezer the user very firmly, yet it is soothing and comforting.. The machine is also equipped with an automatic pulsator so that the squeeze pressure can be rhythmically applied.. It is stimulating and relaxing at the same time. Pressure applied by the machine activates the pressure receptors from nearly every nerve branch which originated from the spinal cord. The machine was powered by a small air compressor which operates the squeeze sides by pulling them together with an air cylinder. (p. 151)
Grandin (1988b) hypothesized “Regular use of the squeeze
machine may help maintain an adequate number of endor
phin and other receptor sites in the brain” (p. 153). She also
conducted a study in which 62% of college students liked
the squeeze machine and found it to be relaxing. In describing
its effect, she wrote:
When I was in the chute, I felt closer to people. Although the squeeze chute was just a mechanical device, it broke through my barrier of tactile defensiveness, and I felt the love and concern of there people and war able to express my feelings about myself and others. It war as if an accordion folding door had been shoved back revealing my emotions. (Grandin & Scariano, 1986, p. 96)
Grandin (1988a) also made a number of more general treatment recommendations. She suggested avoiding noisy environments and recommended:
Autistics must be protected from noises that disturb them.. All the behavior modification in the world will not teach a child to tolerate a noise that is overloading a damaged nervous system. The classroom should be quiet and free from distracting noises, such as a high-pitched fan. Some teachers have found that disturbing noises can be blocked out with headphones and music. When a child has to make a trip to a bury shopping center, a headset with a favorite tape can help make the trip more peaceful. (p. 3)
Grandin & Scariano (1986) also recommended watching food
intake and testing for common allergies such as milk, wheat,
corn, tomatoes, chocolate, sugar, and mushrooms; also rec
ommended was testing for zinc deficiency and excessive cop
per. She noted that megavitamin therapy and vitamin B6 and
magnesium supplements might be beneficial.
In regard to developing language skills, Grandin (1988a) sug
gested stimulating the vestibular system prior to or during
speech activities by having the child swing slowly on a swing.
Using pictures and written language to communicate (Gran
din, 1988b) as well as a visualized reading method developed
by Miller and Miller (cited in Grandin, 19896) was also rec
ommended.
Grandin (1988a) also addressed the issue of stereotyped be
haviors and fixations:
at Colum
bia University L
ibraries on Novem
ber 27, 2014http://m
tp.oxfordjournals.org/D
ownloaded from

‘Autism and Music Therapy
I have made a successful career bared on my fixation with cattle squeeze chutes. ..... .If my fixation had been taken away, I could have ended up in an institution. Do not confuse fixations with stereotyped behavior, such as hand flapping or rocking. A fixation is an interest in something external that should be directed and used to motivate. (p. 6)
She noted that fixations are tremendous motivators, fulfill a
need to reduce arousal in an overactive nervous system, and
should not be eliminated (Grandin, 1986, 1990). Instead of
eliminating fixations, she recommended using them, i.e., teach
concepts such as reading or counting in relation to vacuum
cleaners if that is the fixation. If possible, direct the fixation
into a career:
A high-functioning autistic woman who works doing graphic arts may never be able to fit in with the social whirl, but if they can develop an interesting career they will make social contacts.. People respect talent, even though they might think you are “weird.” Weirdness is more tolerable because other people like the good music or art an autistic person produces. (Grandin, 1988a. p. 7)
Since some people with autism are musically or artistically
gifted, these talents should be nurtured along with more tra
ditional vocational skills. She strongly recommended that peo
ple with autism have career mentors to deal with job-related
social complexities because it is very difficult for a person with
autism to understand how others might think and feel (Gran
din, 1990).
In dealing with stereotype behavior, Grandin (1989b) rec
ommended joining in the stereotype then broadening it into
an activity. This is an approach with which the music therapists
at the author’s facility have had considerable success, and it
is discussed further in the last section.
Grandin & Scariano (1986) was also supportive of behavior
modification but believed that “behavior modification may
be more effective if it is combined with calming sensory input
and exercise to reduce arousal” (p. 183). She recommended
a stable, ordered, secure environment, and giving individuals
with autism a private place to be themselves. She was partic
ularly thankful for creative, unconventional teachers and
friends, people like a teacher who” didn’t see any of the labels,
just the underlying talents.. lie seemed to sense my search
for acceptance on my own level” (p. 86).
17
Grandin’s References to Music
Throughout Grandin’s writings there are many positive ref
erences to music therapy and to the value of music experi
ences. As a child, she was enrolled in an intensive speech
therapy nursery school in which “two or three hours a day
were spent doing physical and musical activities. A strong
emphasis on these types of activities is an important part of a
successful autism program” (Grandin, 1988a, p. 1). She also
described her own musical abilities and deficits. As was pre
viously noted, melodies are the only nonverbal material she
can memorize; however, rhythmic activities are more difficult:
Throughout Grandin’s writings there are many positive references to music therapy and to the value of music experiences
Both as a child and as an adult I have difficulty keeping in time with a rhythm. At a concert where people are clapping in time with the music I have to follow another person sitting beside me. I can keep rhythm moderately well by myself, but itis extremely difficult to synchronize my rhythmic motions with other people or with a musical accompaniment. (Grandin, 1988b p. 165)
She also dicussed possible impacts this might have:
Rhythmic activities with musical instruments can be very helpful. Many amistics have problems with rhythm. The rhythm prablems some autistics have may be related to speech problems. Research has shown that normal babies move in synchronization with adult speech. Autistics fail to do this.. I cannot fallow the rhythmic give and take of conversation. (Grandin, 1988a, p.2)
This implies that rhythm is an integral part of many life activ
ities not usually thought of in this context. Rhythm is essen
tially a sequential task, occurring over time, the kind of task
that Grandin and many individuals with autism find very dif
ficult.
Rhythmic music, particularly when integrated with the tac
tile and vestibular stimulation Grandin emphasizes, can have
a calming effect. Grandin was supportive of combining music
and movement and wrote, “Encourage the autistic child to
use his kinesthetic senses as in motor learning and educating
the musculature of the body.. Musical and rhythmic activ
ities are highly recommended for autistic children” (Grandin
& Scariano, 1986, p. 147). Readers interested in further infor
mation about rhythm are referred to the article, “My Expe
rience as an Autistic Child and Review of Selected Literature,”
in which Grandin devoted several sections to advanced the
ories of body rhythms.
Music also has value for many children with autism because
it is something that is inherently pleasurable, perhaps because
it is an absolutely predictable phenomenon in an unpredict
able world. Grandin (19886) confirmed that responsiveness to
music and wrote:
Music also has value for many children with autism because it is something that is inherently pleasurable, perhaps because it is an absolutely predictable phenomenon in an Unpredictable world.
As a young child I hummed constantly to myself and made little peeping noises. Even as an adult I often hum. Eight-year old autistic children have a tendency to prefer music., Autistic children preferred to turn on a speaker playing sung lyrics instead of turning on a speaker playing spoken lyrics
at Colum
bia University L
ibraries on Novem
ber 27, 2014http://m
tp.oxfordjournals.org/D
ownloaded from

18
of the same song (Blackstock, cited in Grandin, 19886). I can hear a song once or twice and reproduce the melody and pitch accurately. Autistic children can imitate tones as well as or better than normal children. (Applebaum, Egel, Koegel, & Imhoff, cited in Grandin, 19886, p. 148)
Grandin found that music can also play a role in developing
communication skills. She wrote that “some autistic children
can sing a response when they are unable to speak it” (Gran
din, 1988a, p. 2)and that “Lorna King (1981) found that singing
instructions to a 12.-year-old autistic boy resulted in better
communication and obeying of the instructions” (Grandin,
1988b, p. 48).
Grandin(l986a) has known individuals with autism who have
made successful careers in the arts and wrote, “If an autistic
student shows a talent for art or music, the talent must be
nurtured like a delicate flower” (p. 6). She noted that some
people with autism have succeeded at piano tuning because
they have perfect pitch (Grandin, 1990), and that even some
very visual thinkers are able to succeed musically-“Discus
sions with other people with autism have revealed visual
methods of thinking on tasks that are often considered se
quential and nonvisual. A gifted autistic composer told me
that he made ‘sound pictures”’ (Grandin, 1990, p. 6). Musical
successes often lead to significant gains in self-esteem and
social acceptance.
Implications for Music Therapy Practice
The applications of Grandin’s insights to music therapy
practice are many and varied. Within the music therapy lit
erature, there is support for the musical responsiveness of
people with autism which she noted. Thaut (1984). for ex
ample, found that children with autism chose musical time
involvement significantly longer than control groups of nor
mal children. Several studies(Applebaum et al., cited in Gran
din, 19886; DeLong, cited in Thaut (1984); Tanguay, 1976) con
cluded that children with autism process musical stimuli
despite other deficits. Nelson, Anderson, and Gonzales(1984)
found that children with autism can respond very positively
to music or to sound vibrations, such as from a radio. Purvis
and Samet (1976) found music to be a highly effective means
of developing the social-emotional skills of children with au
tism. Positive response to music has also been confirmed by
Alvin (1978), Hairston (1990), Michel(1976), Nordoff and Rob
bins (1977,1965), and Oppenheim (1974). King (cited in Gran
din, 1988b)found that slow rhythmic movements are soothing
tochildren with autism, although the rate which was preferred
was faster than the rate which was quieting to them.
The three basic treatment recommendations Grandin
(1988a) makes can provide a foundation for music therapy
programs. Her emphasis on structure is easily carried over
into the music therapy setting, where there is both the struc
ture of the session and the structure provided by the music
itself. Structure can be provided through a consistent greeting
and goodbye song, and through familiar songs and activities
done in a consistent manner. Thaut (1984) referred to the
Music Therapy Perspectives (1992), Vol. 10
microstructure of activities within sessions and the macro
structure provided by music therapy goals and learning steps
implemented over time. That also found that adding rhyth
mic or melodic structure to verbal instructions aided com
prehension. Nelson et al. (1984) emphasized the importance
of structuring for a high rate of success and noted that music
is inherently a highly structured stimulus due to its repetitive,
concrete nature. They identified two specific ways to struc
ture a session for success: a firm, directive approach with
frequent, clear expectations, or a more open-ended approach
with many opportunities for success without many demands.
The latter approach was mentioned by Alvin (1978)and could
be implemented through the improvisational approach dis
cussed later in this section.
Grandin (1988a) also has advocated exposure to normal chil
dren noting that a person with autism who has skills could be
integrated into a group of individuals who are nonautistic,
providing him with a more normal music experience and ex
posure to behavioral norms.
Structure also could be achieved through a behavioral ap
proach, and it was previously noted that Grandin supported
flexible, non-aversive behavior modification. The use of music
as a reinforcer certainly meets this criterion. Boyle (1991) suc
cessfully trained a girl with autism to come when called by
using access to a music box as a contingent reinforcer. Michel
(1976) reported success by using the playing of instruments
as a contingent reinforcer in teaching a boy with autism to
button his shirt. Music therapists using a behavioral approach
could consult with family or treatment team members about
the use of music as a reinforcer in the classroom or home.
Since many individuals with autism do not respond to tradi
tional reinforcers such as praise or affection, contingent music
could become an important motivator. When employed at a
community residence for male adolescents with autism, the
author noted that two of the eight residents enjoyed recorded
music deeply and were themselves musically gifted. With in
dividuals such as these, live music experiences or recorded
music would provide a powerful motivational tool.
Grandin has been a strong supporter of physical activity,
exercise, and sensory treatment, all of which expose the in
dividual to sensory and motor stimulation in order to develop
his ability to process and learn from this input. Music therapy
can provide the client with a rich variety of sensory and motor
experiences including the vestibular, tactile, and kinesthetic
experiences which Grandin emphasized.
In attempting to provide these experiences, the music ther
apist should be knowledgeable about sensory integration the
ory (Ayres, 1979). James (1984) discussed the application of
sensory integration theory to music therapy practice and con
cluded that an inability to process information from the en
vironment leads to withdrawal from that environment. The
music therapist, using a sensory integration approach, would
work less on teaching a specific skill, such as shape discrimi
nation, but would work at a more basic level of enhancing
the brain’s capacity to integrate and organize the sensory
at Colum
bia University L
ibraries on Novem
ber 27, 2014http://m
tp.oxfordjournals.org/D
ownloaded from

Autism and Music Therapy
stimuli necessary before the development of shape discrim
ination. Results, though possibly slower initially, would be
more generalized (James, 1984). Use of sensory integration
techniques by the music therapist would be done most ef
fectively with a thorough knowledge of the field and through
consultation with an occupational therapist. Music therapists
also need to be aware of the possibilities of abnormal re
sponses to sound due to auditory input not being processed
normally. Nelson et al. (1964) confirmed that individuals with
autism could be hyporesponsive or hyperresponsive to sound,
and Condon (1975) found that persons with autism might ex
perience echoes of auditory stimuli, leading him to recom
mend the consideration of short, separate stimuli. Children
with autism can be particularly responsive to resonant instru
ments (Thaut, 1984), and it has been the author’s experience
that this can become a fixation. A woman with pronounced
withdrawal and self-stimulatory tendencies became totally ab
sorbed in loud, compulsive drum beating and could not be
reached when so engaged. Helping her to feel rhythms and
tempi by tapping on her body and the use of quieter melodic
instruments was a much more effective therapeuticapproach.
When dealing with hyperresponsiveness to sound, the rnu
sic therapist must provide auditory stimulation in such a way
that it is pleasurable to the client with autism. Sisco (1991), in
her work with a very withdrawn, tactilely defensive woman,
found that initially the woman could only tolerate a single
melodic line. A very gentle, nondemanding approach was
used, and the woman gradually became more tolerant of open
fifths and then more complex harmonies. Her social responses
improved, she made eye contact, she vocalized in tonality,
and she began to tolerate touch.
Music therapy activities can serve to integrate auditory,
proprioceptive, tactile, and vestibular stimulation in many ways.
The act of playing an instrument combines the motoric input
from moving muscles with the sound these movements pro
duce. Nelson et al. (1984) believed that “. learning to control
and predict the timing of sounds will improve the child’s
ability to integrate sequences of sounds” (p. 110). Similar re
sults could be achieved through movement to music and
through action songs. The use of action songs was supported
by Alvin (1978) and Stevens and Clark (1969). Thaut (1984)
found that “movement to music also aids the integration of
tactile/kinesthetic and auditory perception and the differ
entiation of self/non-self” (p. 12). By using sounds in syn
chrony with movement or by using body percussion (Thaut,
1984), the music therapist can facilitate the process of sensory
integration.
Music therapy could also provide opportunities for the in
tegration of auditory and visual stimuli. Auditory experiences
can become visual through many means. That (1984) rec
ommended the use of graphic notations to visually represent
the elements of music. In the author’s experience, visually
representing the concepts “same” and “different” with no
tation cards showing different numbers of beats immediately
allowed a client who functioned at a high level but who had
19
poor conceptual skills to grasp these concepts which had
given him great difficulty when presented auditorily.
Computer music programs also would add a visual com
ponent to sound, make auditory experiences more meaning
ful, and facilitate successful experiences. Movement activities
would combine auditory, motor, and visual input effectively.
By addressing these basic levels of sensory integration, the
music therapist could be laying the foundation for successful
learning experiences at higher levels.
Music also could be used to the calm the hyperresponsive
central nervous system to which Grandin referred. Music could
have a soothing effect on a hyperexcitable nervous system,
helping the client to become more receptive to the learning
environment or providing him with respite from a world which
is difficult to understand. Tallarigo (1991) reported a very pos
itive response to the soothing sound of a guitar among ado
lescents with autism.
Music therapy also can play a significant role for individuals
who are autistic with low functioning abilities. Grandin rec
ommended joining in a stereotype behavior (such as hand
flapping or rocking) then broadening this into an activity. At
the author’s facility, this approach has been used with sub
stantial success with people with autistic characteristics and
developmental disabilities. This approach is based on the cre
ative music therapy approach originated by Nordoff and Rob
bins (1977), in which individualized music is improvised to
reflect the client’s motoric, vocal, and instrumental behaviors
and responses. For instance, music might be improvised vo
cally or instrumentally to reflect the rhythm of the client’s
rocking or the pitches or emotional quality of their sounds.
It is an approach in which the music comes from the client,
allowing them considerable control over the amount and kind
of auditory stimulation they receive. Combinations of impro
vised music and movement, i.e., moving with the client while
music is improvised instrumentally or vocally to reflect the
client’s rhythms and moods, also have been used. This im
provisational approach may be successful because it conveys
the acceptance and understanding that Grandin indicated is
so important to a person with autism.
The creative music therapy approach to working with an
autistic child is described in Nordoff and Robbins’ book, Cre
ative Music Therapy (1977). Additional case studies are docu
mented in their book, Music Therapy for Handicapped Children
(1965). Music is used as a powerful means of nonverbal com
munication, a means of gently entering the client’s world
before demanding that he enter ours.
Nordoff and Robbins also analyzed the rhythmic responses
of many developmentally disabled children and identified
specific categories of rhythmic response such as compulsive,
impulsive, and chaotic creative. These categories provide an
interesting framework through which to analyze rhythmic re
sponses and confirm the rhythmic disturbances that Grandin
noted in some individuals with autism. The author has noted
compulsive rhythmic responses, a tendency to become fix
ated in one tempo or rhythm, in several clients with autistic
at Colum
bia University L
ibraries on Novem
ber 27, 2014http://m
tp.oxfordjournals.org/D
ownloaded from
20 Music Therapy Perspectives (1992), Vol. 10
tendencies, and often an analogy can be drawn between clients’ rhythmic responses and their relationship with their environment. The client’s inability to match the therapist’s tempo mirrors her inability to interact meaningfully with her world. Nordoff and Robbins achieved substantial success by matching and reflecting clients’ rhythmic responses, linking the client’s inner world with the outer world. Many other suggestions for specific rhythmic interventions are also given. Additional rhythmic work was done by creating music which matched the rhythms of speech and through helping the children to feel rhythms through tactile stimulation and movement.
Another area in which music therapists could achieve success is in the development of communication skills. Grandin (1988a) related some of her speech problems to rhythmic difficulties and cited the work of King in using musical directions. It is possible that adding a musical component to speech would increase comprehension for some individuals. Thaut (1984) recommended combining language, melody, and rhythm by adding a strong rhythmic or melodic component to verbal instructions. Since individuals with autism also often have disturbances of intonation, he used music activities to develop an awareness of high/low, loud/soft, and stress patterns. This awareness was then used for melodic shaping of vocal expressions. Tallarigo (1991) successfully used signing with songs to make words visual, and in some cases, the use of sign language facilitated the acquisition of spoken language. With clients who function at a low level, music can provide a less threatening, nonverbal means of communication and self-expression that can be the beginning of language. A comprehensive group of activities/approaches for the development of communication skills is found in Thaut (1984).
Nelson et al. (1984) offered several other suggestions for the music therapist. They noted the necessity for matching music stimuli to specific client characteristics and confirmed the need to program for generalization and transference of learning. They concluded that music can be an effective way for clients with autism to develop two traditionally weak areas, creativity and initiative. It is gratifying to note that they also recommended music therapy for children with autism simply because responsiveness to music might be a significant strength, and wrote that, “therapy ... is also a process of refining and improving the individual’s strengths” (p. 113). In summarizing the use of music therapy with individuals with autism they concluded:
Whether the strategy is directive or non-directive, the goal is the same: to show the child that he can have predictable, positive effects on the environment through his or her own actions, (p. 104)
Conclusion
It is tremendously exciting to be able to glimpse the world of a person with autism through the experiences of Grandin. It has been gratifying to find many references to music therapy in her work and to consider how powerful music can be as a therapeutic tool in developing the potential of people with
autism. Grandin & Scariano (1986) wrote that people with autism live in a “world they are desperately trying to give some order to” (p. 16). As music therapists, we have a unique means of making a more ordered world a reality.
REFERENCES
Alvin, J. (1978). Music therapy for the autistic child. New York: Oxford University
Press. Ayres, A. I. (1979). Sensory integration and the child. Los Angeles: Western
Psychological Services. Boyle, M. (1991). Personal communication with the author.
Condon, W. S. (1975). Multiple response to sound in dysfunctional children. Journal of Autism & Childhood Schizophrenia, 5, 37-56.
Grandin, T. (1988a). Teaching tips from a recovered autistic. Focus on Autistic Behavior, 3(l), 1-8.
Grandin, T. (1988b). My experiences as a autistic child and review of selected literature. Journal of Orthomolecular Psychiatry, 13(3), 144-174.
Grandin, T. (1989a). An autistic person’s view of holding therapy. Communi
cation, 23(3), 75-77. Grandin, T. (19896, October). My personal experienceswith autism. In Autism:
Personal and professional perspectives. Seminar conducted at Duchess Community College, Poughkeepsie, NY.
Grandin, T. (1990). Needs of high functioning teenagers and adults with autism (Tips from a recovered autistic). Focus on Autistic Behavior, 5(1), 1-16.
Grandin, T., & Scariano, M. M. (1986). Emergence: Labeled autistic. Novato, CA: Arena Press.
Hairston, M. (1990). Analyses of responses of mentally retarded autistic and
mentally retarded nonautistic children to art therapy and music therapy. Journal of Music Therapy, 27(3), 137-150.
lames, M. (1984). Sensory integration: A theory for therapy and research. Journal of Music Therapy, 21(2), 79-88.
Michel, D. (1976). Music therapy. Springfield, IL: Charles C. Thomas. Nelson, D., Anderson, V., & Gonzales, A. (1984). Music activities as therapy
for children with autism and other pervasive developmental disorders.
Journal of Music Therapy, 21(3), 100-116. Nordoff, P., & Robbins, C. (1965). Music therapy for handicapped children.
Lebanon, PA: Rudolf Steiner Publications. Nordoff, P., & Robbins, C. (1977). Creative music therapy. New York.: John Day
Company.
Oppenheim, R. (1974). Effective teaching methods for autistic children. Spring
field, IL: Charles C. Thomas. Purvis, J., & Samet, S. (1976). Music in developmental therapy. Baltimore: Uni
versity Park Press. Ratey, J. J. (1989, October). The use of alternative medication to treat ag
gression and self injury. In Autism: Personal and professional perspectives.
Seminar conducted at Duchess Community College, Poughkeepsie, NY. Rimland, B. (1971). The differentiation of childhood psychoses: An analysis of
checklists for 2,218 psychotic children. Journal of Autism & Childhood
Schizophrenia, 1, 161-174. Sisco, J, (1991). Personal communication with the author. Stevens, E., & Clark, F. (1969). Music therapy in the treatment of autistic
children. Journal of Music Therapy, 6, 93-104. Tallarigo, P. (1991). Personal communication with the author. Tanguay, P. (1976). Clinical and electrophysiological research. In E. R. Ritvo
(Ed.), Autism: Diagnosis, current research and management (pp. 75-84). New York.: Spectrum Publishers.
Thaut, M. (1984). A music therapy treatment model for autisticchildren. Music
Therapy Perspectives, 1, 7-13.
at Colum
bia University L
ibraries on Novem
ber 27, 2014http://m
tp.oxfordjournals.org/D
ownloaded from





























