Embed Size (px)
Citation preview

ATS Basel
Sekundärprophylaxe nach Schlaganfall
Stefan Engelter 26. April 2012

Stroke- RezidivpräventionPrinzipien
ANTITROMBOTIKA

Übersicht
OAK versus ASS/Clopidogrel
Neue Orale Antikoagulatien
Antikoagulationsbeginn
Aetiologie und „Number needed to treat“

NASCET
Guidelines for Management of Ischemic Stroke and Transient Ischemic Attack 2008 Cerebrovasc Dis 2008;25:457-507

Guidelines for Management of Ischemic Stroke and Transient Ischemic Attack 2008 Cerebrovasc Dis 2008;25:457-507

Vorhofflimmern: Antikoagulation vs. Placebo
AFASAK I SPAF BAATAF CAFA SPINAF
Alle Studien RRR = 62 %
Relative Risikoreduktion 95% CI
0 -50% -100% 100% 50% Hart RG et al. Ann Intern Med 1999;131:492-501

OAK versus ASS/Clopidogrel

Lit.: EAFT Study Group, Lancet 1993;342:1255-62
100%
80%
60%
1 J 2 J 3 J
Placebo
Aspirin
Antikoagulation
Primäre Outcomes
Ereignisse 17%/J 8%/J
Schlaganfälle 12%/J 4%/J

Lit.: EAFT Study Group, Lancet 1993;342:1255-62
100%
80%
60%
1 J 2 J 3 J
Placebo
Aspirin
Antikoagulation
Primäre Outcomes
Ereignisse 17%/J 8%/J
Schlaganfälle 12%/J 4%/J
Probleme der OAK:
• Langsamer Wirkungseintritt
• Interaktionen (Medi, Diät)
• Enges therap. Fenster (INR 2-3)
• Engmaschiges Monitoring (Labor)
• Effekt individuell unbestimmt

ACTIVE W: Orale Antikoagulation ist einer Tc-Aggregationshemmer-Kombination überlegen!
Atrial Fibrillation Clopidogrel Trial with Irbesartan for Prevention of Vascular Events - Warfarin
Studie gestoppt nach medianem Verlauf 1.28 Jahre
ACTIVE Writing Group of the ACTIVE Investigators Lancet 2006;367:1903-12
-30% p=0.0003
-77% p=0.005
(Primary outcome+major bleed)
Primary outcome: composite endpoint of stroke, non-CNS systemic embolus, MI or vascular death
Einschlusskriterien : dokumentiertes VHF + mind 1 RF für Hirnschlag:
Alter >75, Hypertonie, LVEF <45%, PAVK, D.mell (55-74j.), Anamnese mit Stroke, TIA
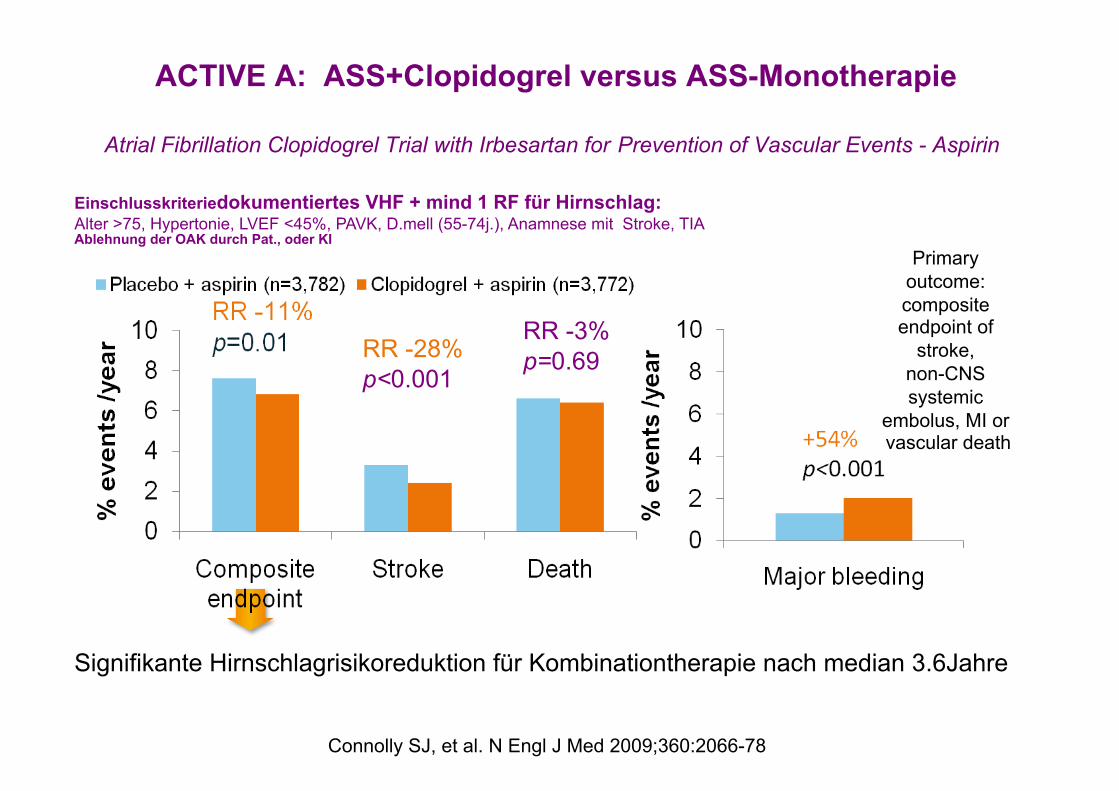
ACTIVE A: ASS+Clopidogrel versus ASS-Monotherapie
Atrial Fibrillation Clopidogrel Trial with Irbesartan for Prevention of Vascular Events - Aspirin
Signifikante Hirnschlagrisikoreduktion für Kombinationtherapie nach median 3.6Jahre
Connolly SJ, et al. N Engl J Med 2009;360:2066-78
RR -28% p<0.001
RR -3% p=0.69
Einschlusskriteriedokumentiertes VHF + mind 1 RF für Hirnschlag: Alter >75, Hypertonie, LVEF <45%, PAVK, D.mell (55-74j.), Anamnese mit Stroke, TIA Ablehnung der OAK durch Pat., oder KI
Primary outcome: composite endpoint of
stroke, non-CNS systemic
embolus, MI or vascular death

Rel
ativ
es R
isik
o Risiko für Blutung
INR
0 . 0
2 . 0
4 . 0
6 . 0
8 . 0
1 0 . 0
0 . 0 1 . 0 2 . 0 3 . 0 4 . 0 5 . 0 6 . 0
(Lit: EM Hylek, NEJM 1996;335:540)
Optimaler INR-Bereich bei nicht-valvulärem Vorhofflimmern
Risiko für Stroke

Warfarin in AF: Time in therapeutic range

Warfarin in AF: SUBGROUPS

Neue Orale Antikoagulatien
Warum neue Antikoagulantien zur Prävention des Hirnschlages bei Vorhofflimmern
• Vitamin K Antagonisten sind wirksam • Werden noch immer zu wenig eingesetzt • „Time in therapeutic range“ unzureichend(?) • Einsatz durch Nebenwirkungen eingeschränkt: intrakranielle
Hämorrhagien, enges therapeutisches Fenster, Nahrungsmittel und Medikamenteninteraktionen, individuelle Wirksamkeit/Dosis nicht voraussehbar (CyP-Polymorphismen)
• Alternativsubstanzen müssen mindestens die gleiche Wirksamkeit mit einem tieferen Blutungsrisiko aufweisen und eine einfache Behandlung gewährleisten
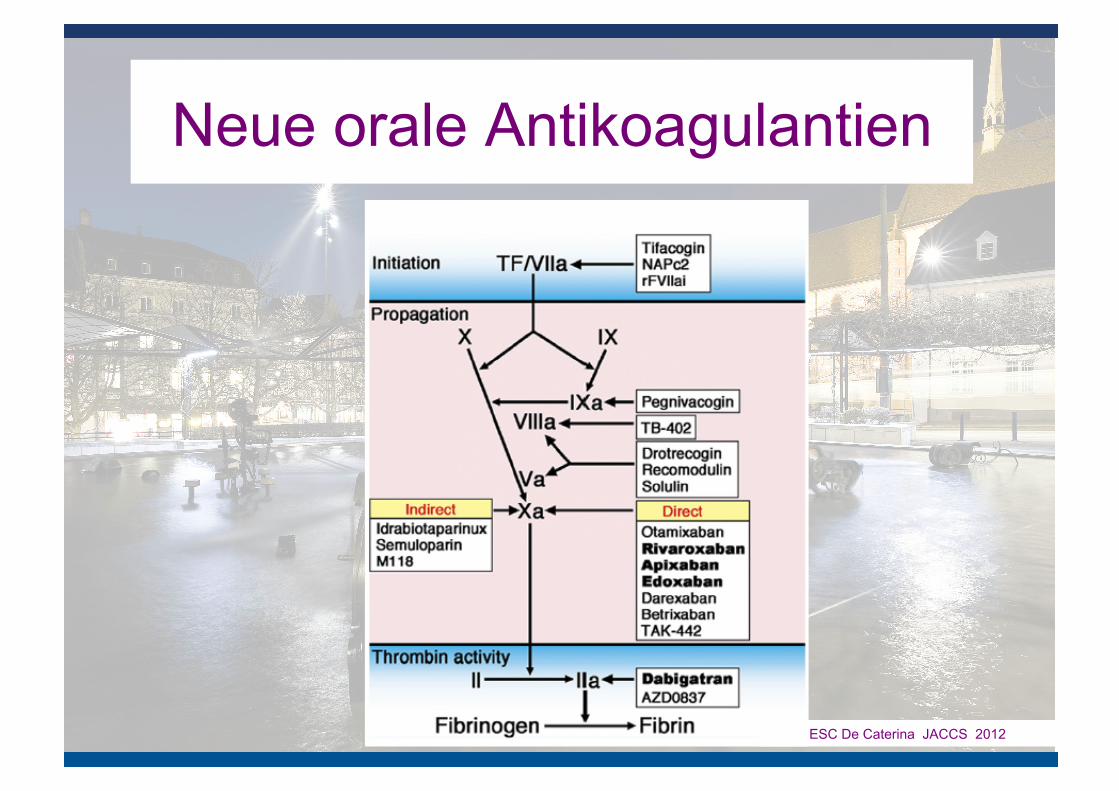
Neue orale Antikoagulantien
ESC De Caterina JACCS 2012

Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation
(ROCKET AF) • double-blind trial, • 14,264 patients with nonvalvular atrial • fibrillation at increased risk for stroke • rivaroxaban (at a daily dose of 20 mg) or dose-adjusted warfarin • designed to determine whether rivaroxaban was non-inferior to warfarin • primary end point of stroke or systemic embolism
published on August 10, 2011, at NEJM.org.

Rocket Results: Primary efficacy endpoint
Per protocol population, on-treatment
Kaplan–Meier survival curve showing time to the primary endpoint (stroke or systemic embolism)
Months from randomization
Cum
ulat
ive
even
t rat
e –
stro
ke o
r sy
stem
ic e
mbo
lism
(%)
0
1
2
3
0
4
5
6
7
No prior stroke/TIA, warfarin
30
Prior stroke/TIA, warfarin
6 12 18 24
No prior stroke/TIA, rivaroxaban
Prior stroke/TIA, rivaroxaban
Event rates:
1.7% vs. 2.2%/yr
RR 0.79

Rivaroxaban Events/100 pt-
yrs
Warfarin Events/100 pt-
yrs Interaction
p-value Stroke or systemic embolism
1.09 2.26
1.69 2.60
0.15
Any stroke 1.06 2.21
1.53 2.37
0.16
Haemorrhagic stroke
0.17 0.35
0.41 0.47
0.22
Ischaemic or unknown stroke
0.89 1.86
1.11 1.92
0.41
Disabling or fatal stroke
0.45 1.15
0.88 1.31
0.07
Non-CNS systemic embolism
0.04 0.05
0.16 0.23
0.99
Any cause death 2.00 1.74
2.35 2.07
0.94
Vascular death 1.61 1.44
1.70 1.71
0.60
Rocket:Efficacy analysis
0.1 10 1 Favours rivaroxaban
Favours warfarin
No prior stroke or TIA Prior stroke or TIA
Per protocol population, on-treatment

Rocket-AF Subgroup: Stroke/TIA

Rocket-AF Subgroup: Stroke/TIA-Pts SAFETY

Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY)
• noninferiority trial • 18,113 patients with fibrillation and a risk of stroke • blinded , fixed doses of dabigatran — 110 mg or 150 mg twice daily
— or, in an unblinded fashion, adjusted-dose warfarin • follow-up period 2.0 years • primary outcome: stroke or systemic embolism

24
Results: Time to first stroke or systemic embolism
BID = twice daily; NI = non-inferiority; RR = relative risk; RRR = relative risk reduction; Sup = superiority
Years 0.0 0.5 1.0 1.5 2.0 2.5
0.01
0.02
0.03
0.05
0.04
Cum
ulat
ive
haza
rd r
ates
0.00
Warfarin Dabigatran 110 mg BID Dabigatran 150 mg BID
RR 0.90 (95% CI: 0.74–1.10) P<0.001 (NI) P=0.30 (Sup)
RR 0.65 (95% CI: 0.52–0.81) P<0.001 (NI) P<0.001 (Sup)
RRR 35%
Connolly SJ et al. N Engl J Med 2010;363:1875–6
Event rates:
1.69% vs. 1.53% vs. 1.11%
RR 0.91 resp. 0.66

Stroke or systemic embolism
Ischaemic or unspecified stroke
Hemorrhagic stroke
Relative risk 0.5 2.0 1.0 1.5
Favours dabigatran 110 mg BID
Favours warfarin
Non-disabling stroke
Stroke
Disabling or fatal stroke
25
Error bars = 95% CI; BID = twice daily
Dabigatran etexilate 110 mg BID compared with warfarin for stroke prevention in AF
Connolly SJ et al. N Engl J Med 2009;361:1139–51; Connolly SJ et al. N Engl J Med 2010;363:1875–6

26 Connolly SJ et al. N Engl J Med 2010;363:1875–6
Error bars = 95% CI; BID = twice daily
Risk of stroke or systemic embolism
Dabigatran 110 mg BID vs. warfarin
Dabigatran 150 mg BID vs. warfarin
0.50 0.75 1.00 1.25 1.50
<0.001
<0.001
Superiority P-value
0.30
<0.001
Non-inferiority P-value
Hazard ratio M
argi
n =
1.4
6

RE-LY: subgroup with prior stroke or TIA
• Diener HC et al: www.thelancet.com/neurology online November 8, 2010 DOI:10.1016/S1474-4422(10)70274-X
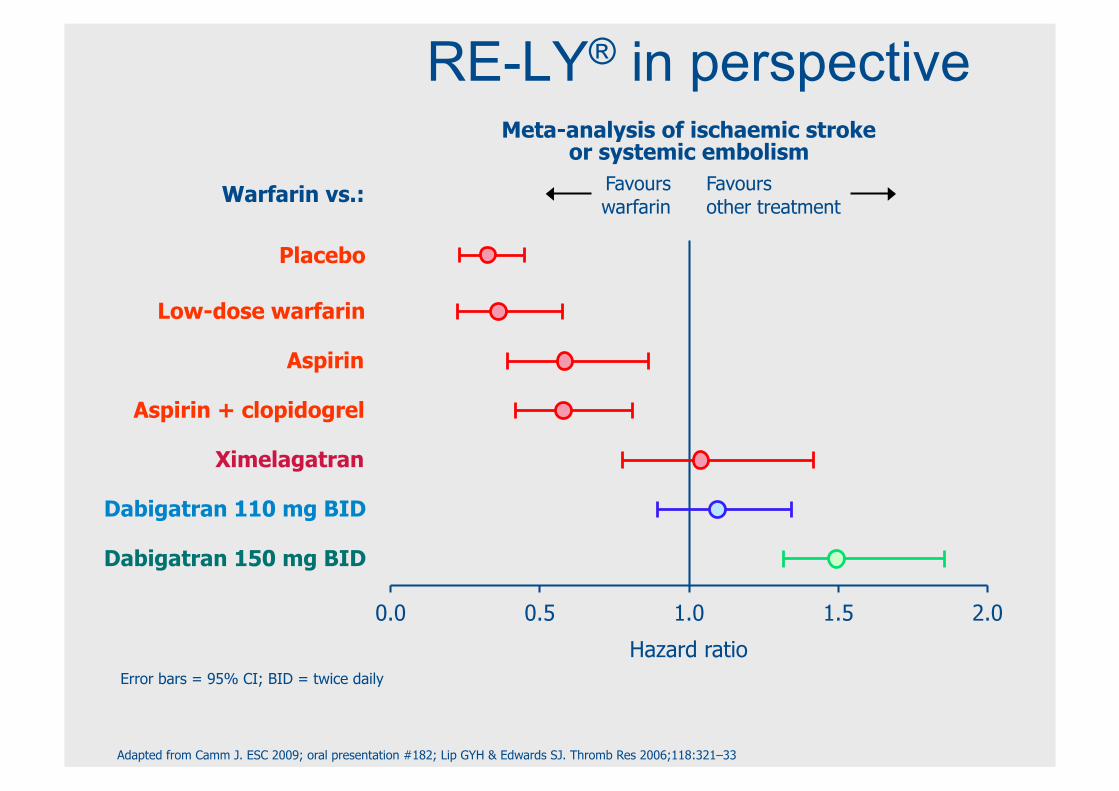
0.0
Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolism
Favours warfarin
Favours other treatment
Warfarin vs.:
Placebo
2.0
Low-dose warfarin
0.5 1.0 1.5
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY® in perspective
Error bars = 95% CI; BID = twice daily
Adapted from Camm J. ESC 2009; oral presentation #182; Lip GYH & Edwards SJ. Thromb Res 2006;118:321–33

• apixaban 5 mg twice daily) compared to warfarin (target international normalized ratio, 2.0 to 3.0)
• 18,201 patients with atrial fibrillation and at least one additional risk factor for stroke.
• primary outcome: ischemic or hemorrhagic stroke or systemic embolism.
• test for noninferiority, with key secondary objectives of testing for superiority with respect to the primary outcome and to the rates of major bleeding and death from any cause.
published online August 28, 2011
Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE)

Granger CB et al. N Engl J Med 2011. DOI: 10.1056/NEJMoa1107039
Kaplan–Meier Curves for the Primary Efficacy and Safety Outcomes.
Apixaban versus Warfarin in Patients with Atrial Fibrillation
Event rates:
1.27%vs.1.60% /yr
RR: 0.66

Efficacy Outcomes.
Granger CB et al. N Engl J Med 2011. DOI: 10.1056/NEJMoa1107039

Relative Risks of the Primary Efficacy and Safety Outcomes, According to Major Prespecified Subgroups
Granger CB et al. N Engl J Med 2011. DOI: 10.1056/NEJMoa1107039

Antikoagulationsbeginn

Efficacy and Safety of Anticoagulant Treatment in Acute Cardioembolic Stroke A Meta-Analysis of Randomized Controlled Trials Maurizio Paciaroni et al. Stroke 2007;38;423-430
significant in symptomatic intracranial bleedings: 2.5% vs 0.7% odds ratio 2.89; 95% CI: 1.19 to 7.01, P=0.02 no sig. differences in recurrent ischem. stroke, death, disability
N = 4642 pts
<48 h

„In patients with AF and acute TIA, anticoagulation treatment should begin as soon as possible in the absence of cerebral infarction or haemorrhage.
ESC-Guideleines 2010; European Heart Journal (2010) 31, 2369–2429

Purroy Stroke 2007 38(12):3225

Apixaban: Excl. criteria: • „stroke within the previous 7 days“
N Engl J Med 2011;365:981-92
Dabigatran: Excl. criteria: • „stroke within 14 days or severe stroke within 6 months before screening “
N Engl J Med 2009;361:1139-51
Rivaroxaban: Excl. criteria: • Severe, disabling stroke (modified Rankin score of 4 to 5, inclusive) within 3 months or any stroke within 14 days before the randomization visit • Transient ischemic attack within 3 days before the randomization visit“ • Fibrinolytics within 10 days before randomization
N Engl J Med 2011;365:883-91 (suppl. Material)
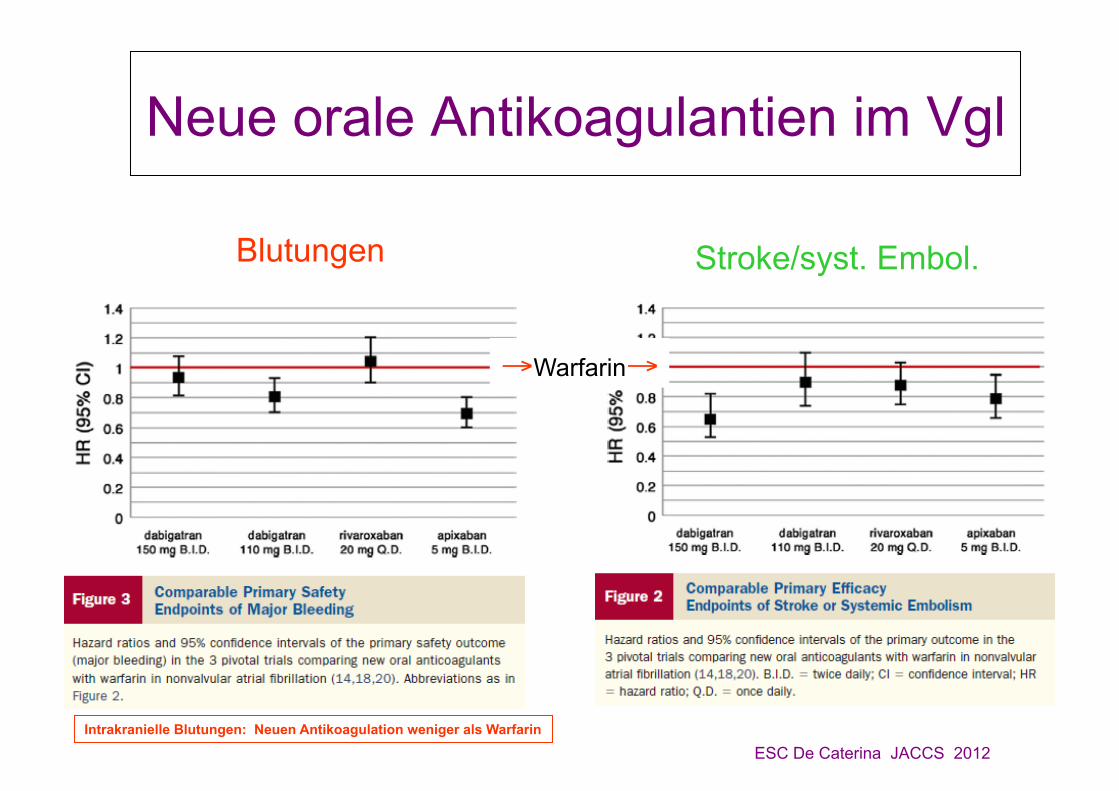
Neue orale Antikoagulantien im Vgl
Blutungen Stroke/syst. Embol.
→Warfarin→
ESC De Caterina JACCS 2012 Intrakranielle Blutungen: Neuen Antikoagulation weniger als Warfarin

Zusammenfassung • Tc-Hemmer Standard nach atherothrombotischen Hirninfarkt
• Bei Vorhofflimmern und Hirninfarkt/TIA: OAK • 3 neue Antithrombotika zur Hirnschlagprävention bei VHF
• Effekt gegenüber WF (Coumarine) jeweils vergleichbar bis besser
• Im Vergleich zu WF (Coumarinen) weniger zerebrale Hämorrhagien • Dabigatran 2 x tgl., 2 mögliche Dosen (110, 150mg), Zulassung wird
unmittelbar erwartet
• Rivaroxaban 1x tgl., eingeführt als Thromboseprophylaxe für chir. Eingriffe, erweiterte Zulassung demnächst
• Apixaban 2 Gaben tgl., Zulassungen CH pendent





























