Embed Size (px)
Citation preview
Atrial Fibrillation - ED Electrical and Pharmacologic Cardioversion Protocol
1
General Measures:
If unstable: proceed more urgently – see emergent cardioversion protocol
Ensure atrial fibrillation of recent onset (<48 hours) and not recurrent
NPO for at least 3-4 hrs, bedrest, IV, monitor Work up:
Troponin, electrolytes, TSH, CMP, PT/INR, PTT, BNP
Echocardiogram to be arranged if not previously obtained
TEE in selected cases for rapid cardioversion if unknown duration or AFib > 48hrs
Assess CHADVASC score and document in chart
Management: Control rate; consider rhythm cardioversion, and anticoagulate as shown below, according to Category: 1, 2 or 3 Category 1. Normal EF
Rate control: Ca-blocker or beta-blocker.
Cardiovert: o If onset < 48 hours, consider DC cardioversion OR with one of the following agents: amiodarone, ibutilide,
procainamide, (flecainide, propafenone), sotalol. o If onset > 48 hours: avoid drugs that may cardiovert (e.g. amiodarone). Either:
Delayed Cardioversion: anticoagulate adequately x 3 weeks, then cardioversion, then anticoagulate x 4 weeks
Early Cardioversion: admission, iv heparin, then TEE, then cardioversion within 24 hours, then anticoagulate x 4 weeks
Anticoagulate if not contraindicated, if A fib > 48 hrs
Category 2. EF< 40% or CHF
Rate control: o digoxin, diltiazem, amiodarone (avoid if onset of AF > 48 hours). o avoid verapamil, beta-blockers, ibutilide, procainamide (and propafenone/flecainide)
Cardiovert: same as Category 1, except the only conversion agent allowed is amiodarone.
Anticoagulate, if A fib > 48 hr.
Category 3. WPW A fib
Suggested by: delta wave on resting EKG, very young patient, HR>300
Avoid adenosine, beta-blocker, Ca-blocker, or Digoxin
If < 48 hour: o If EF normal: one of the following for both rate control and cardioversion: amiodarone, procainamide,
propafenone, sotalol, flecainide o If EF abnormal or CHF: amiodarone or cardioversion
If > 48 hour o Medication listed above may be associated with risk of emboli o Anticoagulate and DC cardioversion as in Category 1.
Note: new ALCS does not allow mixing antiarrhythmics for AFib/flutter.
Atrial Fibrillation - ED Electrical and Pharmacologic Cardioversion Protocol
2
Electrical Cardioversion
[stable pt with a tachydysrhythmia (rapid atrial fibrillation, supraventricular tachycardia/SVT, ventricular tachycardia/VT with a
pulse)]:
1. Properly place on monitor/defibrillation that is capable of providing synchronization. Apply patches anteroposterior.
2. RE-assess cardiac rhythm for appropriateness of cardioversion
3. Have equipment available /prepared for possible worsening of patient’s condition
4. Anesthesia present if possible and non-urgent/IV sedation/Airway management
5. Ensure all personnel are clear of patient before initiating chock
6. Apply synchronization –assure sensing or R wave (and not T wave)
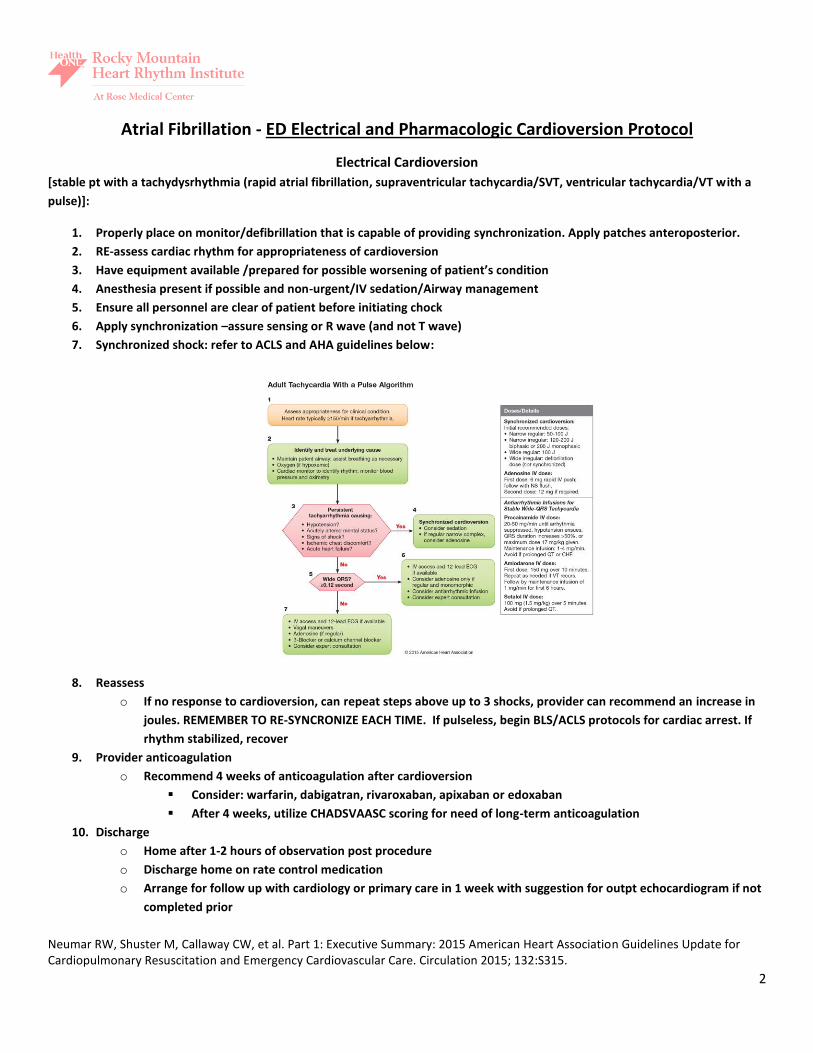
7. Synchronized shock: refer to ACLS and AHA guidelines below:
8. Reassess
o If no response to cardioversion, can repeat steps above up to 3 shocks, provider can recommend an increase in
joules. REMEMBER TO RE-SYNCRONIZE EACH TIME. If pulseless, begin BLS/ACLS protocols for cardiac arrest. If
rhythm stabilized, recover
9. Provider anticoagulation
o Recommend 4 weeks of anticoagulation after cardioversion
Consider: warfarin, dabigatran, rivaroxaban, apixaban or edoxaban
After 4 weeks, utilize CHADSVAASC scoring for need of long-term anticoagulation
10. Discharge
o Home after 1-2 hours of observation post procedure
o Discharge home on rate control medication
o Arrange for follow up with cardiology or primary care in 1 week with suggestion for outpt echocardiogram if not
completed prior
Neumar RW, Shuster M, Callaway CW, et al. Part 1: Executive Summary: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015; 132:S315.





















