Embed Size (px)
Citation preview
Provider Respiratory Inservice
2
Welcome
Opening Remarks
3
We will cover:
• Definition of Asthma & COPD
• Evidence based guidelines for diagnosis, evaluation, and management of asthma
• Evidence based guidelines for diagnosis, evaluation, and management of adult with COPD
• Coding
• BC/BS services available to assist your practices
4
What is Asthma?
• Obstructive lung disease with characteristics of:
– Airway obstruction; reversible in most patients
– Chronic airway inflammation (eosinophils)
– Increased airway responsiveness
• Onset of symptoms can occur at any age
Asthma
• 34 million people in the U.S. currently diagnosed with asthma
• 7.1 million children are diagnosed with asthma
• 1.3 million visits to hospital outpatient departments with asthma as a primary diagnosis
• Asthma costs exceed $30 billion/year
• Asthma in the U.S. is growing every year
5 U.S Department of Health and Human Resources Center for CDC: 12/2012
6
What is COPD?
• A common, preventable, and treatable disease:
– Characterized by persistent airflow limitation
• Usually progressive
– Associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases.
– Exacerbations and comorbidities contribute to the overall severity in individual patients.
COPD
• 16 million U.S. adults have been diagnosed with COPD
• 15 million or more U.S. adults have COPD that have not been diagnosed
• 4th leading cause of death in the U.S.
• Annual direct & indirect COPD Medical Costs $42.6 billion
7 U.S Department of Health and Human Resources Center for CDC: 2007
8
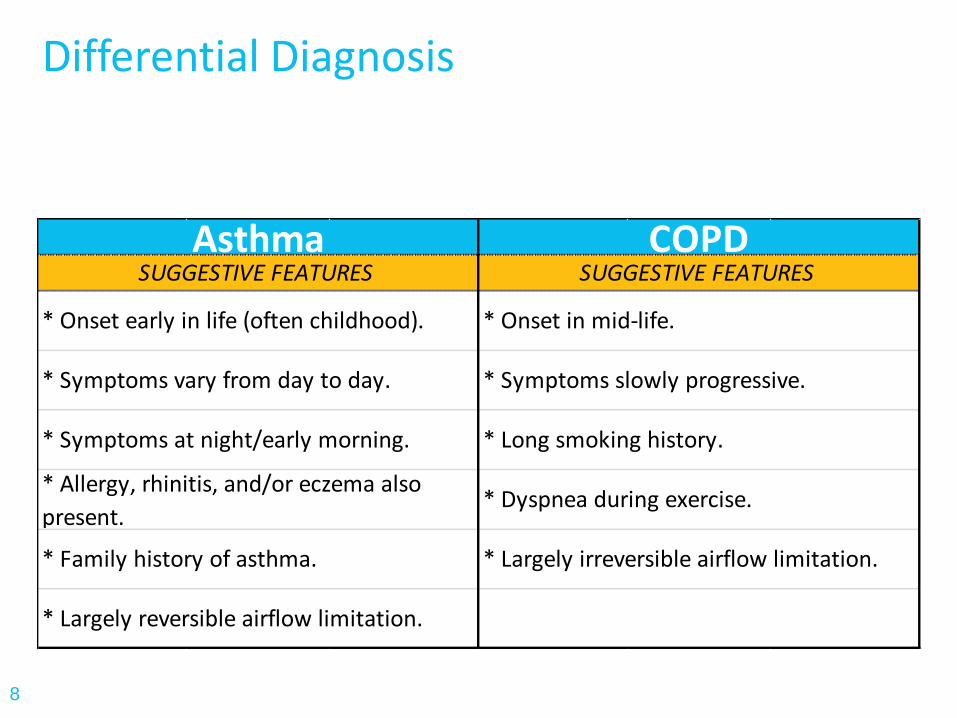
Differential Diagnosis
* Onset early in life (often childhood).
* Symptoms vary from day to day.
SUGGESTIVE FEATURES
* Onset in mid-life.
* Symptoms slowly progressive.
* Largely irreversible airflow limitation.
COPDSUGGESTIVE FEATURES
Asthma
* Symptoms at night/early morning.
* Allergy, rhinitis, and/or eczema also
present.
* Family history of asthma.
* Largely reversible airflow limitation.
* Long smoking history.
* Dyspnea during exercise.
Asthma vs. COPD
• Spirometry is required pre- and post- bronchodilator to help differentiate between Asthma and COPD
– Asthma = Reversibility
– COPD = No/partial reversibility
• Chest Xray – to order or not?
• Vaccinate for flu and pneumonia
9
Case Study
• 45 year old female presents to the office with complaints of shortness of breath and wheezing. She has a history of asthma.
10
History – Questions to ask • Symptoms (wheezing, dyspnea, cough)
• Timing and Frequency
• Triggers
– Work environment: dust, fumes, chemicals
– Home environment: heating, mold, pets, dust, roaches, cigarette/cigar smoke
– Exercise
– Upper Respiratory Infections
• Medications – inhalers, steroids and other medications
• Smoking history
• Family history 11
Findings
• Smoker – 1 ppd X 10 years, quit age 30
• SOB and wheezing – daily
• Uses albuterol inhaler 1x per day
• Wakes at least 1 night per week with a cough
• Becomes SOB with exercise
• Works at Chevy plant Monday – Friday
• 2 courses of oral systemic corticosteroids last 6 months
12
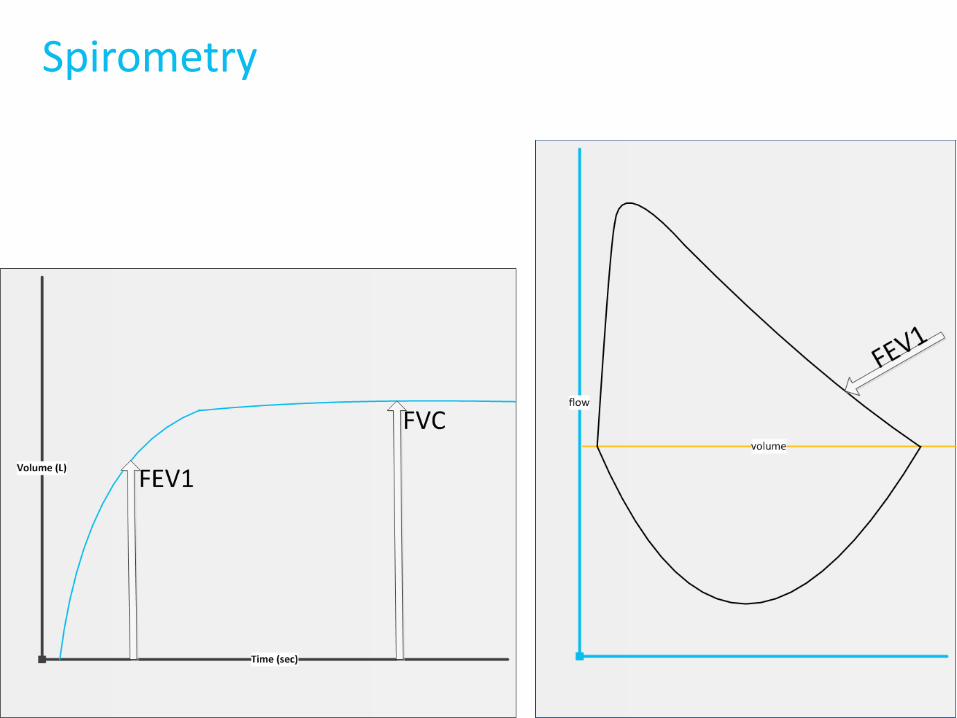
Spirometry
13
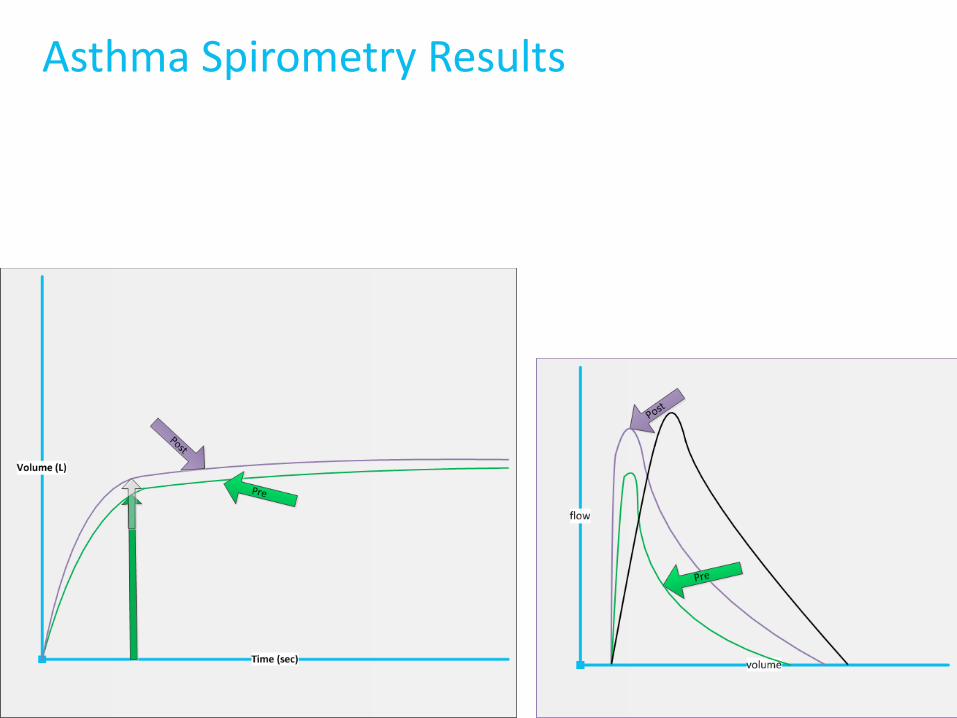
Asthma Spirometry Results
14
15
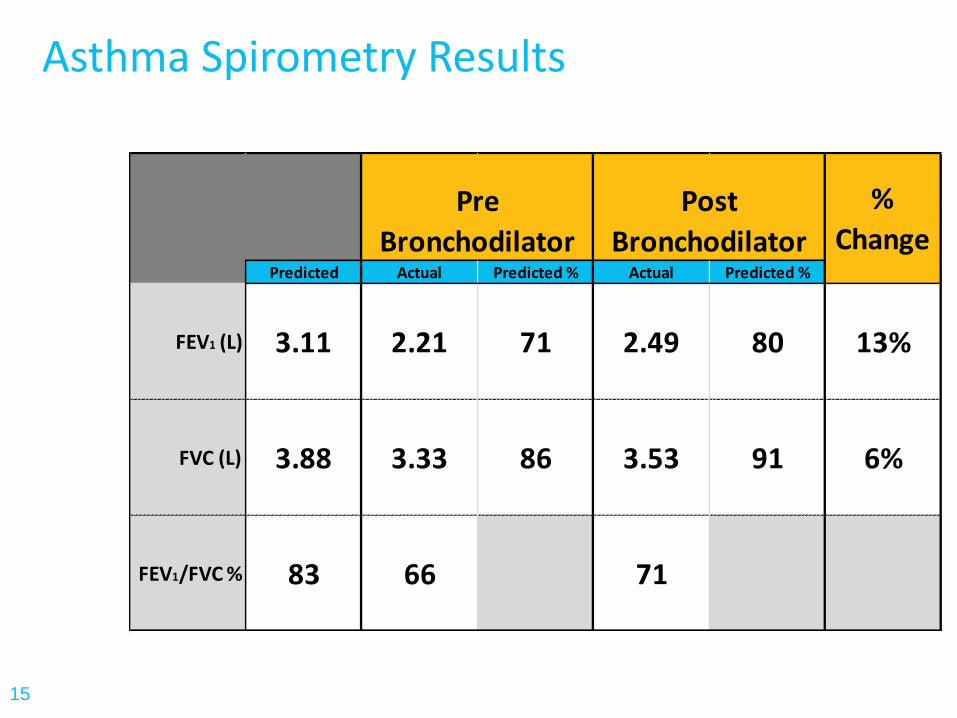
Asthma Spirometry Results
Predicted Actual Predicted % Actual Predicted %
FEV1 (L) 3.11 2.21 71 2.49 80 13%
FVC (L) 3.88 3.33 86 3.53 91 6%
FEV1/FVC % 83 66 71
%
ChangePre
Bronchodilator
Post
Bronchodilator
16
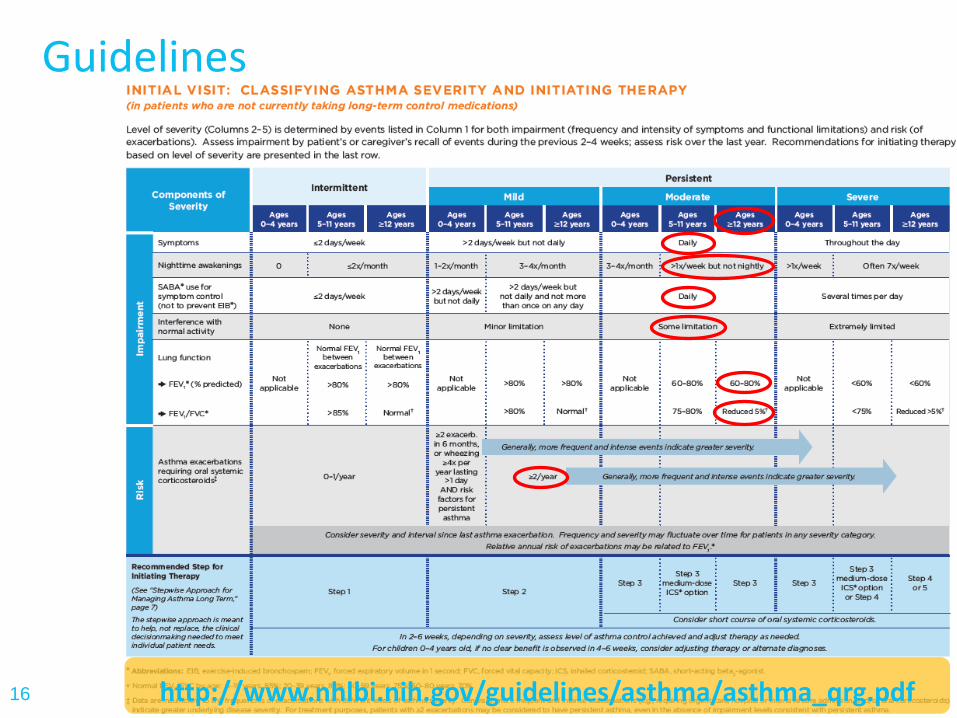
Guidelines
http://www.nhlbi.nih.gov/guidelines/asthma/asthma_qrg.pdf
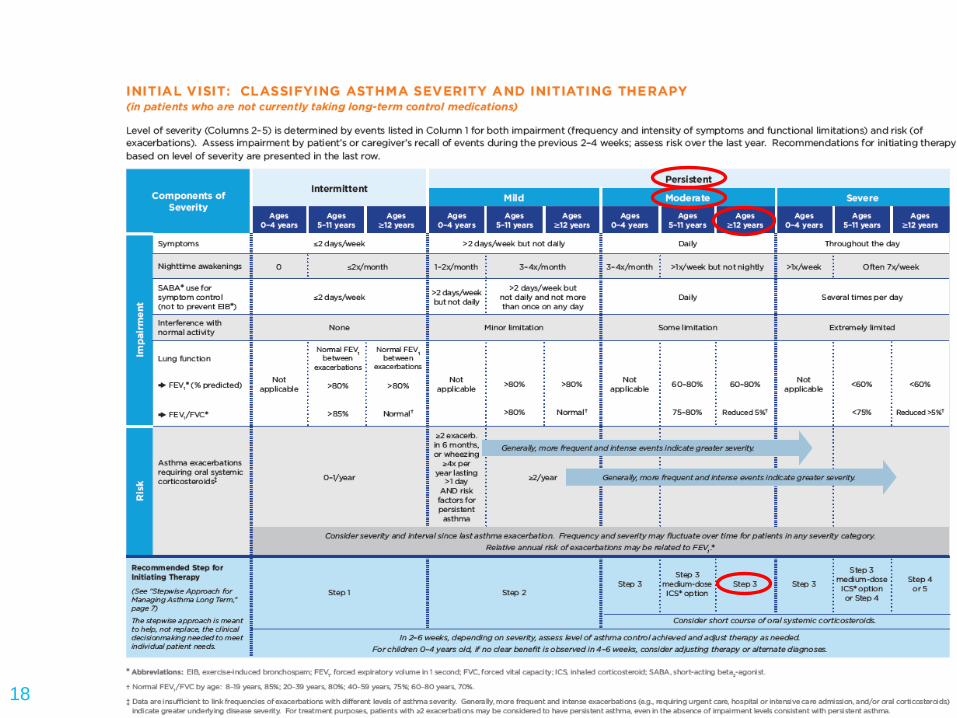
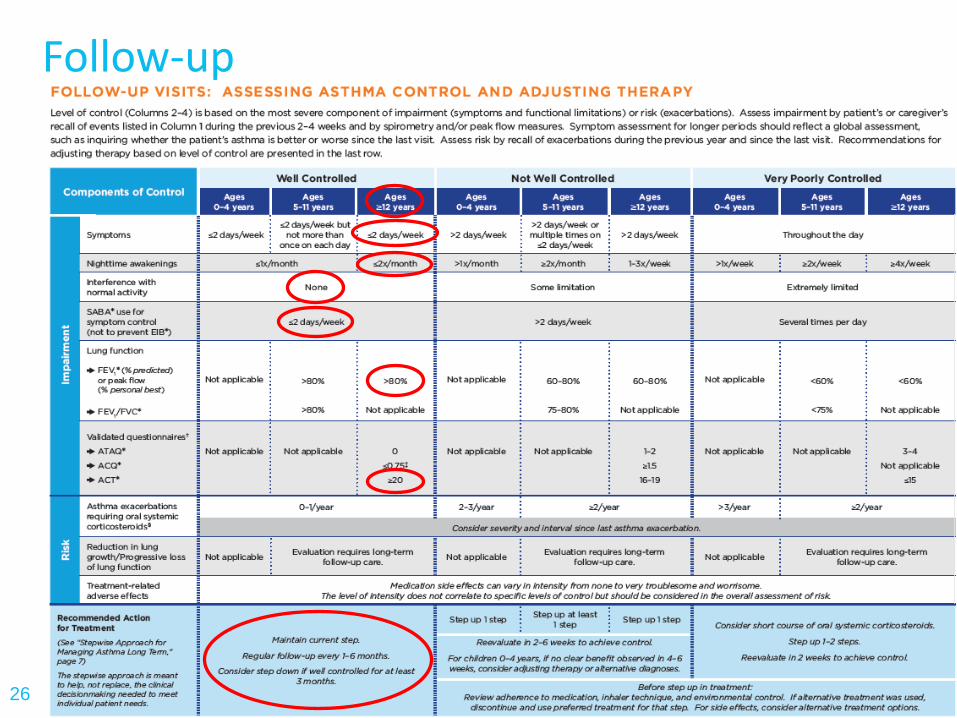
Classifying Asthma Severity
• According to EPR-3 guidelines, the member is classified as having moderate persistent asthma
• Diagnosis = moderate persistent asthma
– Next - therapy
17
18
19
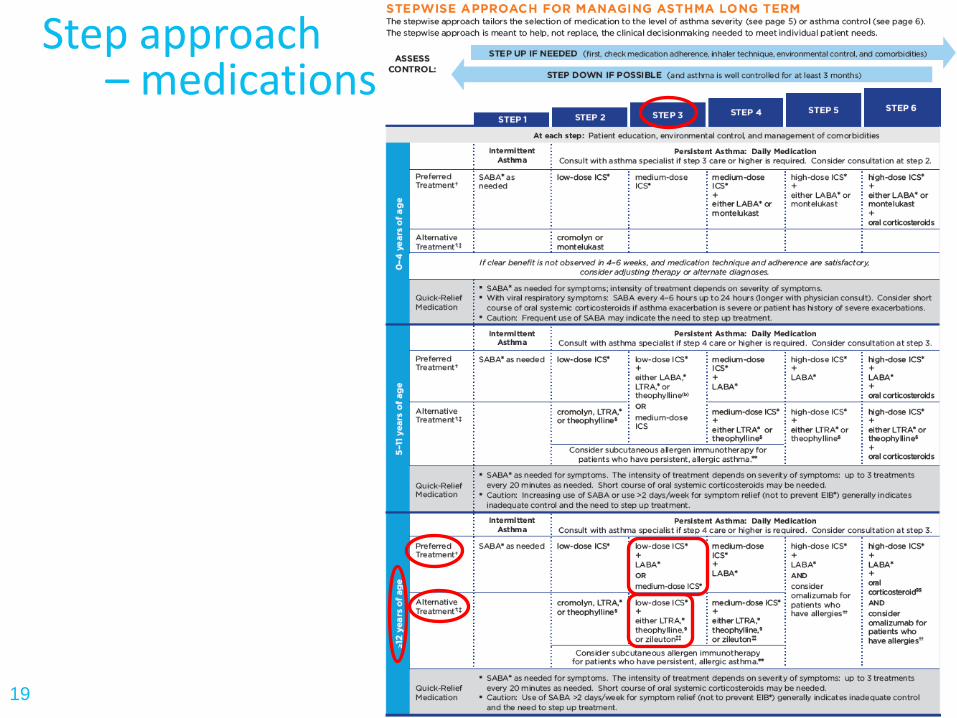
Step approach – medications
Asthma Medications
Quick-Relief medication: • SABA (Short-Acting Beta Agonists)
Controller medications:
• ICS (Inhaled Corticosteroids)
• LABA (Long-Acting Beta Agonists)
• LABA/ICS Combinations
• LEUKOTRIENE MODIFIERS
• Miscellaneous (theophylline, cromolyn)
20
Next Steps
Education: • Review Medications
• Review inhaler technique + compliance at each visit
• Reducing exposure to triggers
• Review asthma action plan each follow-up visit
• Smoking cessation assistance
• Vaccinate for flu and pneumonia
21
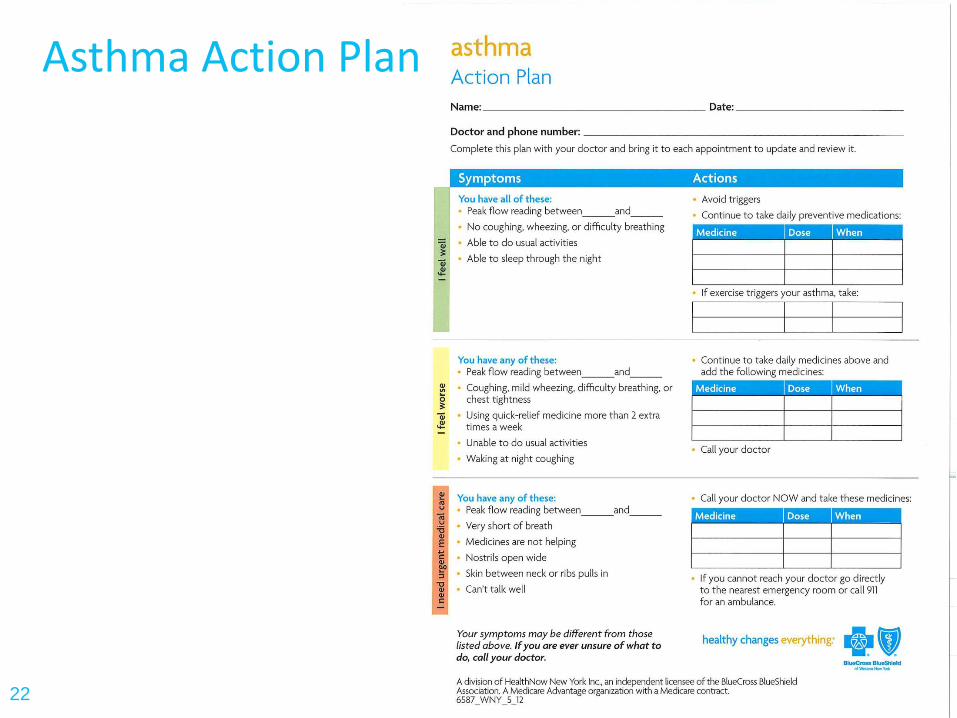
Asthma Action Plan
22
Follow-up: 2-6 weeks after initial visit
23
• ACT test – patient completes
• Assess level of symptom control with current medication regime
• Medication compliance and technique
• Step up or step down, according to signs and symptoms
• Patient education
• Referral to pulmonologist or allergist, if needed
• Review and update Asthma action plan
• Encourage compliance
24
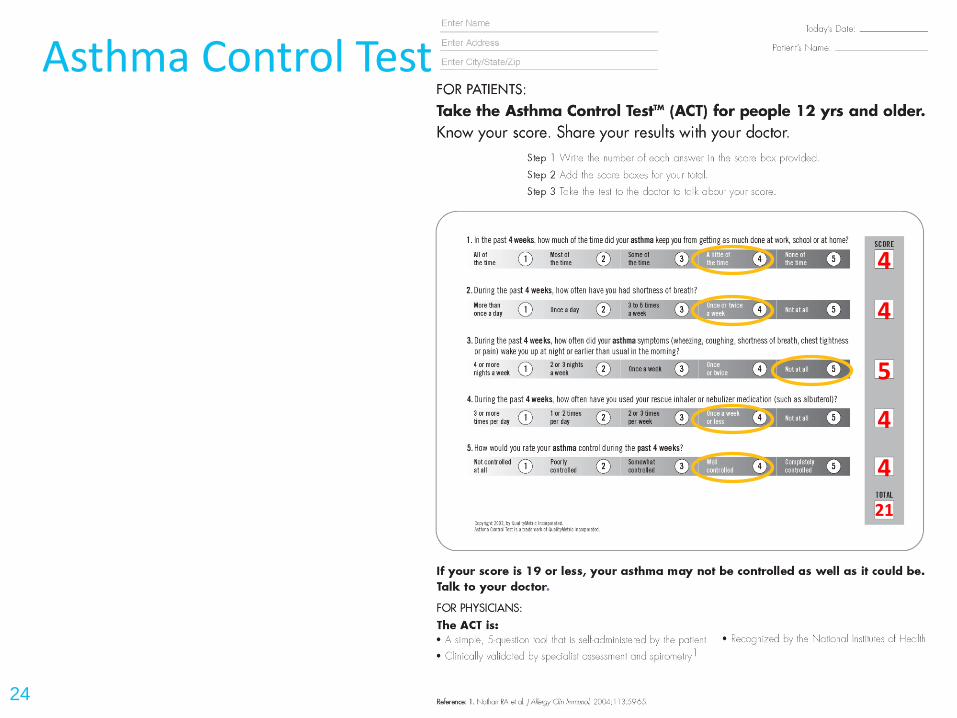
Asthma Control Test
4
4
5
4
4
21
Case study follow-up • ACT test – review
• SOB 1X in 3 weeks
• No nighttime awakening
• No SOB while exercising
• Use albuterol inhaler 1X in 3 weeks
• Repeat spirometry showed FEV1 > 80% predicted
• Next follow up appointment in 1-6 months
• Well controlled
• Consider step down if well controlled for at least 3 months
25
26
Follow-up
Case Study
• 45 year old female presents to the office with complaints of shortness of breath and wheezing.
27
History – Questions to ask
• Symptoms (SOB, cough, wheezing, phlegm production, color, amount)
• Timing and Frequency
• Smoking history
• Medications – inhalers, steroids, other medications
• Family history
28
Findings
• Smoker 2ppd since age 20
• Dyspnea and wheezing
• Uses albuterol inhaler 1x per day
• Experiences cough and some dyspnea with exercise
• Productive cough with white sputum
• Works at Chevy plant Monday – Friday
• Has been treated with 2 courses of Prednisone in the past 6 months
29
Is this COPD?
Spirometry MUST be performed! Within 180 days from initial diagnosis
• Pulse oximetry – to do or not?
• Chest Xray – to do or not?
30
31
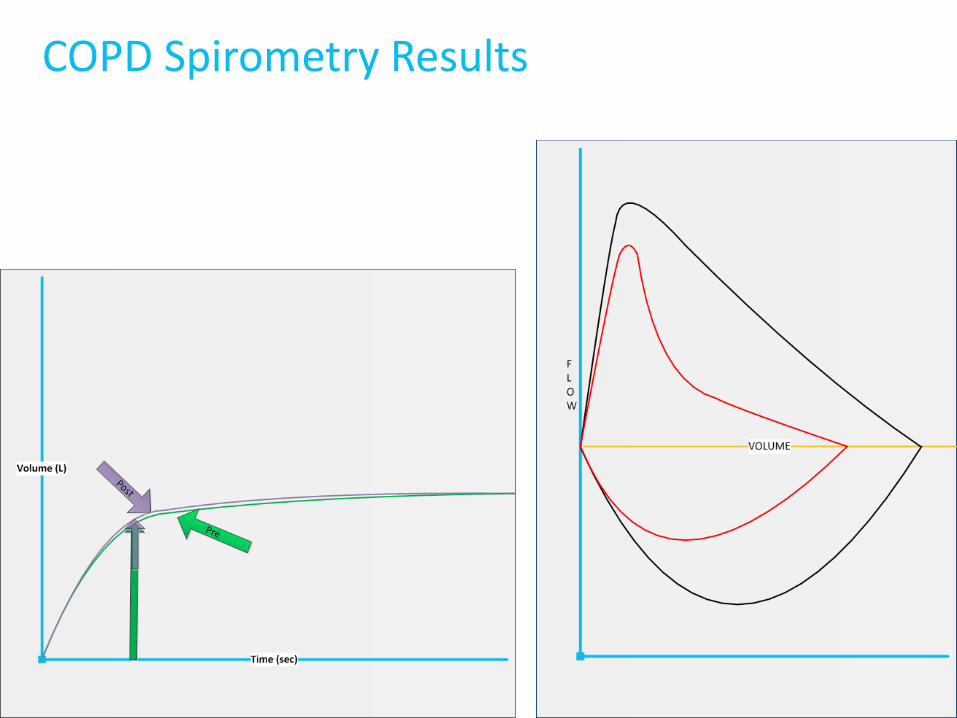
COPD Spirometry Results
32
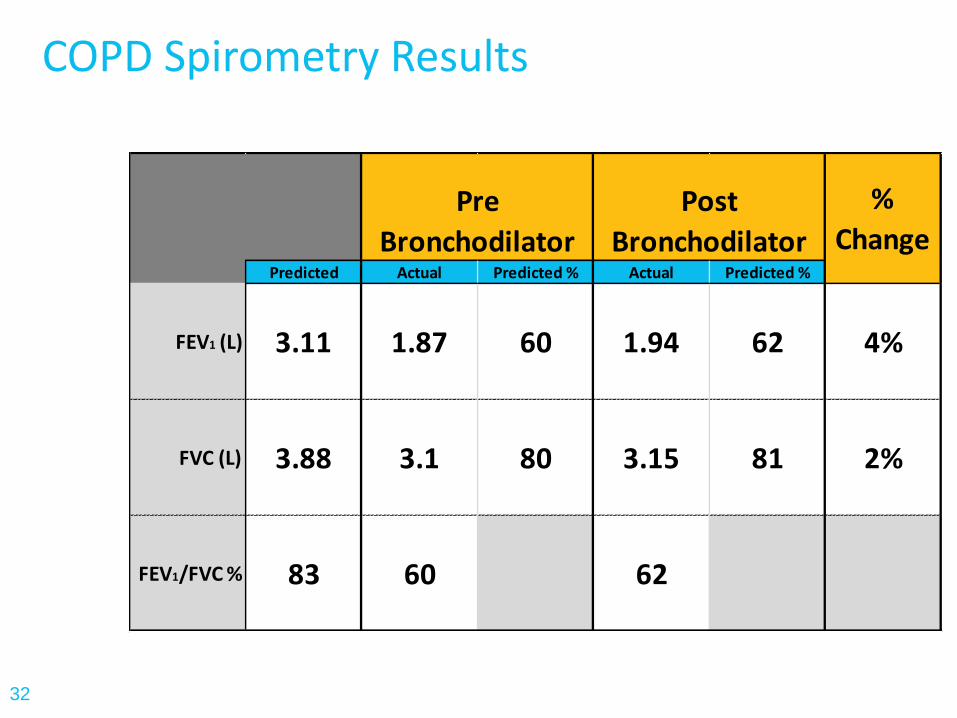
COPD Spirometry Results
Predicted Actual Predicted % Actual Predicted %
FEV1 (L) 3.11 1.87 60 1.94 62 4%
FVC (L) 3.88 3.1 80 3.15 81 2%
FEV1/FVC % 83 60 62
%
ChangePre
Bronchodilator
Post
Bronchodilator
COPD Medications
• SABA (Short-Acting Beta Agonists)
• ICS (Inhaled Corticosteroids)
• LABA (Long-Acting Beta Agonists)
• LABA/ICS Combinations
• Anticholinergics
• Miscellaneous (theophylline, roflumilast, combivent)
33
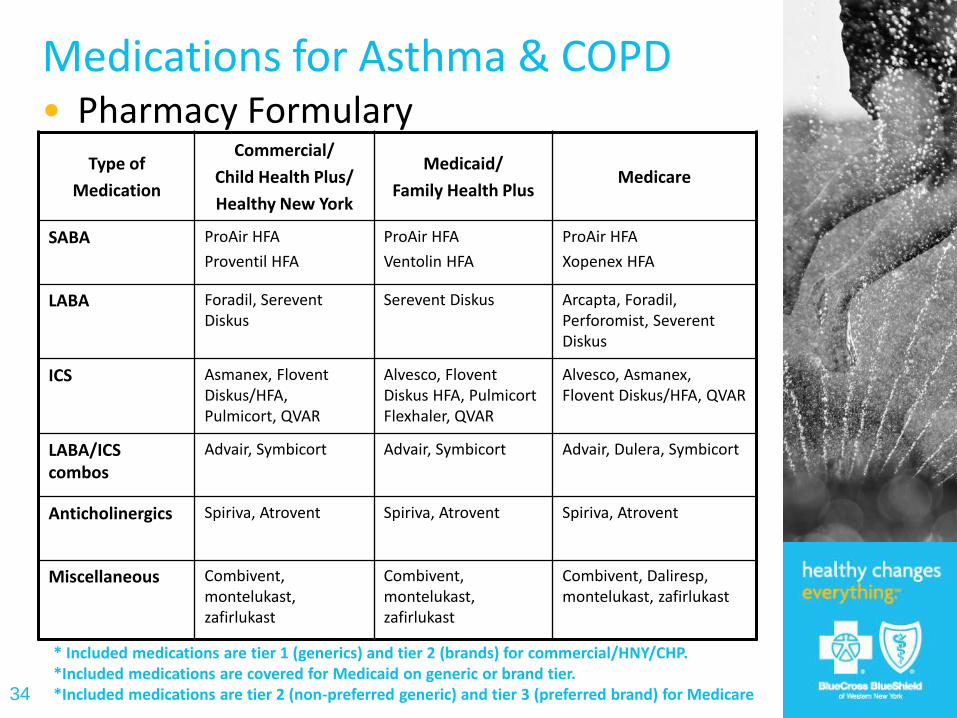
Medications for Asthma & COPD • Pharmacy Formulary
34
Type of
Medication
Commercial/
Child Health Plus/
Healthy New York
Medicaid/
Family Health Plus Medicare
SABA ProAir HFA
Proventil HFA
ProAir HFA
Ventolin HFA
ProAir HFA
Xopenex HFA
LABA Foradil, Serevent Diskus
Serevent Diskus Arcapta, Foradil, Perforomist, Severent Diskus
ICS Asmanex, Flovent Diskus/HFA, Pulmicort, QVAR
Alvesco, Flovent Diskus HFA, Pulmicort Flexhaler, QVAR
Alvesco, Asmanex, Flovent Diskus/HFA, QVAR
LABA/ICS combos
Advair, Symbicort Advair, Symbicort Advair, Dulera, Symbicort
Anticholinergics Spiriva, Atrovent Spiriva, Atrovent Spiriva, Atrovent
Miscellaneous Combivent, montelukast, zafirlukast
Combivent, montelukast, zafirlukast
Combivent, Daliresp, montelukast, zafirlukast
* Included medications are tier 1 (generics) and tier 2 (brands) for commercial/HNY/CHP. *Included medications are covered for Medicaid on generic or brand tier. *Included medications are tier 2 (non-preferred generic) and tier 3 (preferred brand) for Medicare
Next Steps
• Review medications
• Review inhaler technique & compliance at each visit
• Review care plan each follow up visit
• Smoking cessation assistance
• Vaccinate for flu and pneumonia
35
Follow up
• Follow up Q 6 months or sooner if hospitalized or in ED for COPD
• Review symptoms at each visit
• Review Medications
• Spirometry every year
36
37
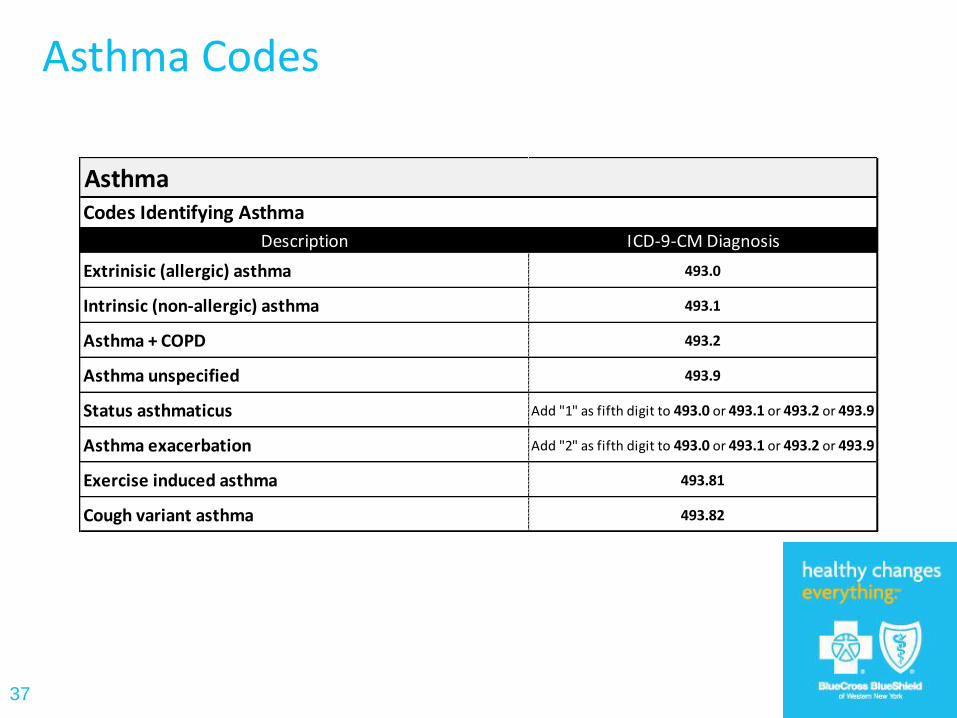
Asthma Codes
Description ICD-9-CM Diagnosis
Extrinisic (allergic) asthma 493.0
Intrinsic (non-allergic) asthma 493.1
Asthma + COPD 493.2
Asthma unspecified 493.9
Status asthmaticus Add "1" as fifth digit to 493.0 or 493.1 or 493.2 or 493.9
Asthma exacerbation Add "2" as fifth digit to 493.0 or 493.1 or 493.2 or 493.9
Exercise induced asthma 493.81
Cough variant asthma 493.82
Codes Identifying Asthma
Asthma

38
39
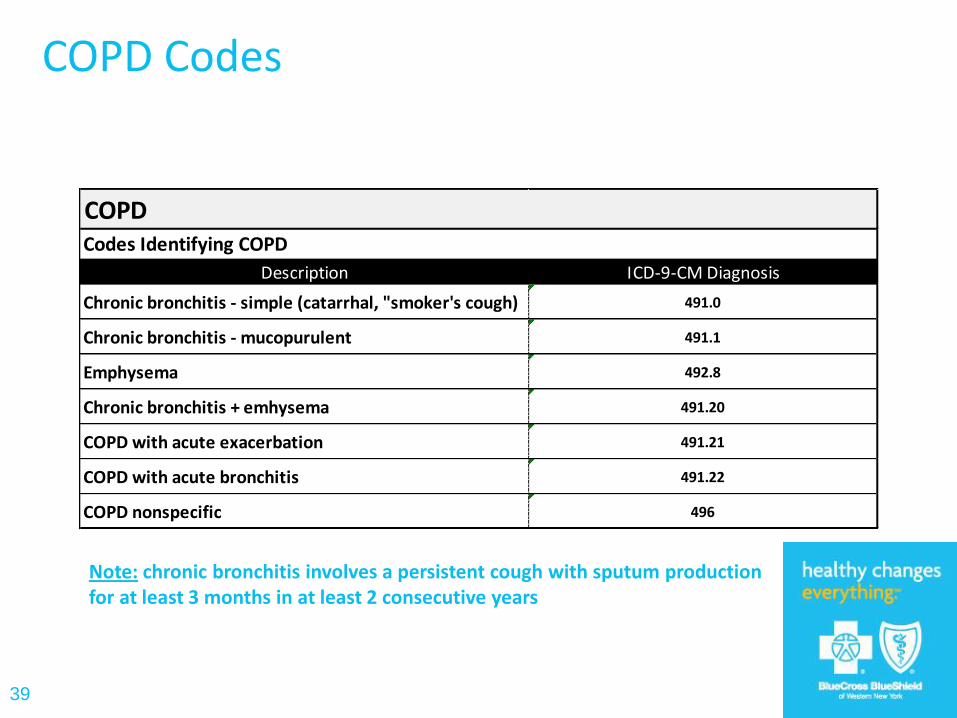
COPD Codes
Note: chronic bronchitis involves a persistent cough with sputum production for at least 3 months in at least 2 consecutive years
Description ICD-9-CM Diagnosis
Chronic bronchitis - simple (catarrhal, "smoker's cough) 491.0
Chronic bronchitis - mucopurulent 491.1
Emphysema 492.8
Chronic bronchitis + emhysema 491.20
COPD with acute exacerbation 491.21
COPD with acute bronchitis 491.22
COPD nonspecific 496
COPDCodes Identifying COPD
40
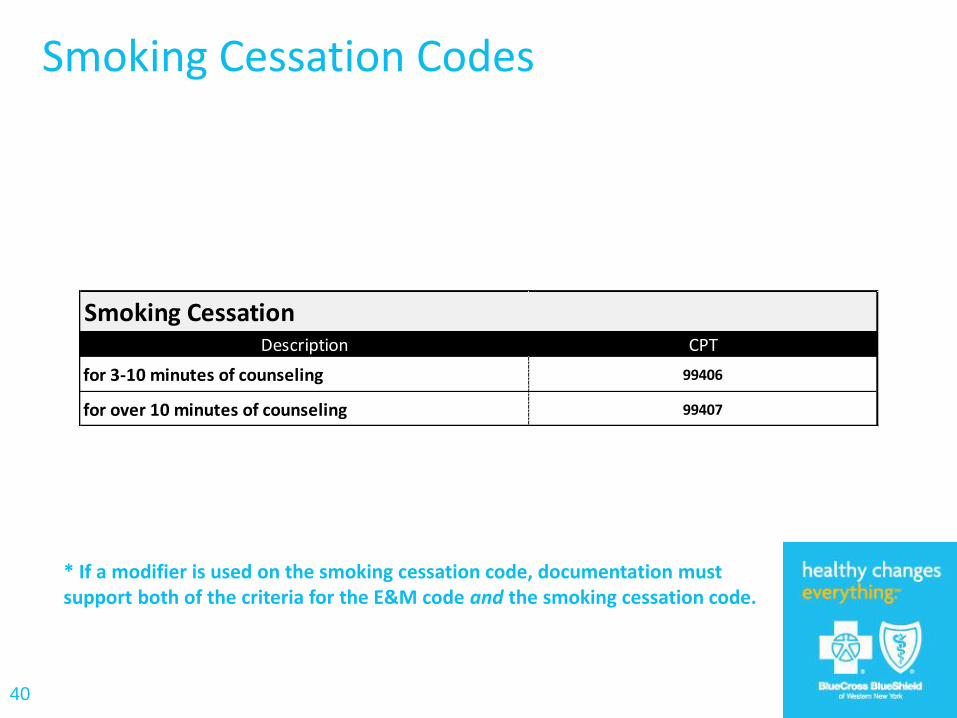
Smoking Cessation Codes
Description CPT
for 3-10 minutes of counseling 99406
for over 10 minutes of counseling 99407
Smoking Cessation
* If a modifier is used on the smoking cessation code, documentation must support both of the criteria for the E&M code and the smoking cessation code.
41
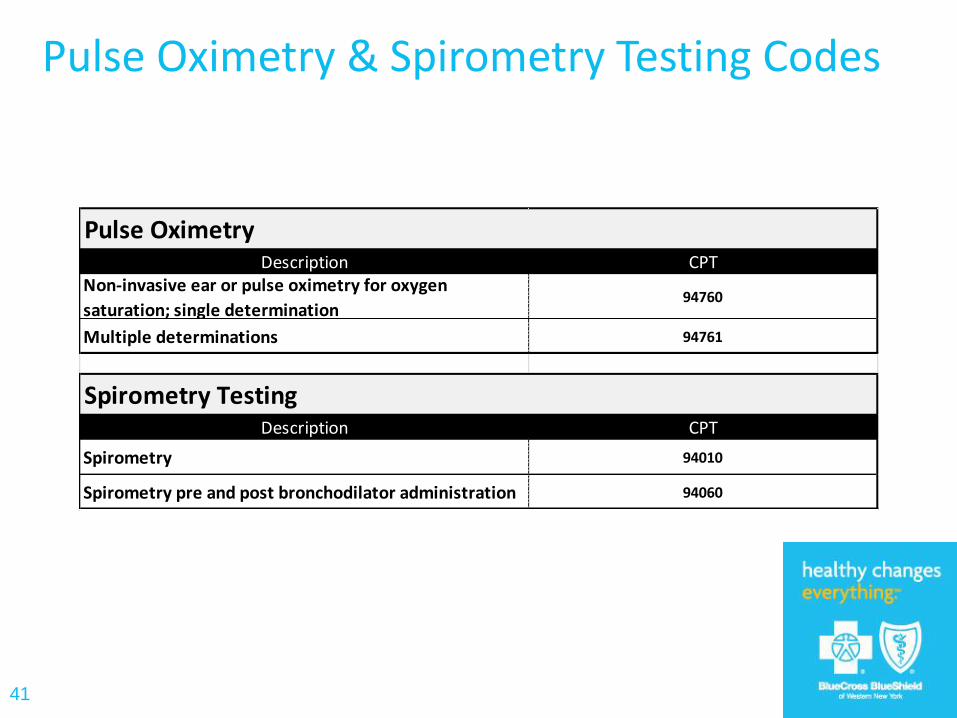
Pulse Oximetry & Spirometry Testing Codes
Description CPTNon-invasive ear or pulse oximetry for oxygen
saturation; single determination94760
Multiple determinations 94761
Description CPT
Spirometry 94010
Spirometry pre and post bronchodilator administration 94060
Spirometry Testing
Pulse Oximetry
42
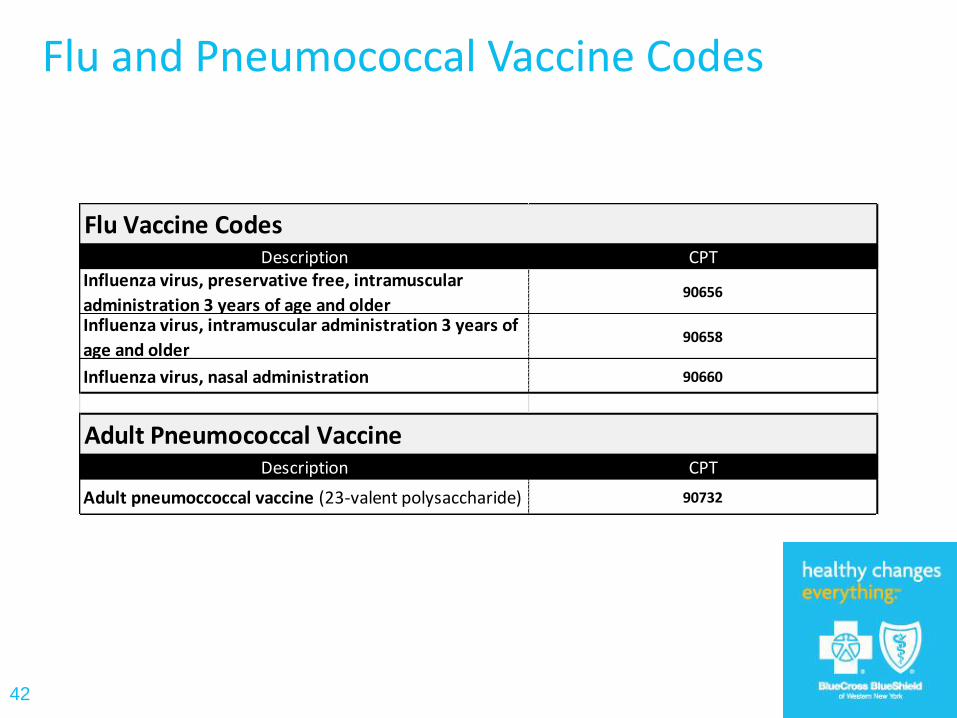
Flu and Pneumococcal Vaccine Codes
Description CPTInfluenza virus, preservative free, intramuscular
administration 3 years of age and older90656
Influenza virus, intramuscular administration 3 years of
age and older90658
Influenza virus, nasal administration 90660
Description CPT
Adult pneumoccoccal vaccine (23-valent polysaccharide) 90732
Flu Vaccine Codes
Adult Pneumococcal Vaccine
43
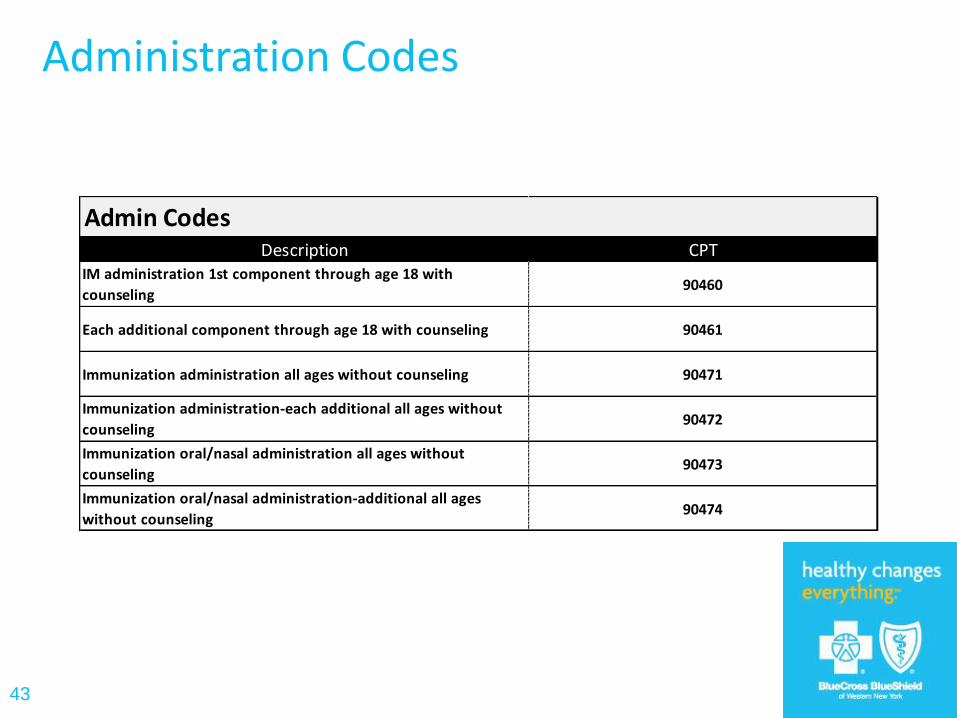
Administration Codes
Description CPTIM administration 1st component through age 18 with
counseling90460
Each additional component through age 18 with counseling 90461
Immunization administration all ages without counseling 90471
Immunization administration-each additional all ages without
counseling90472
Immunization oral/nasal administration all ages without
counseling90473
Immunization oral/nasal administration-additional all ages
without counseling90474
Admin Codes

How we can help you
• One on one health coaching with a registered nurse available to assist our BCBS members
– Educate about disease process
– Medication management
– Address gaps in care
– Coordinate services
– Reinforce treatment plan
44
How we can help you
• We also have a team of social workers, dieticians and outreach workers
• Community classes:
– Smoking cessation
– Nutrition
– Weight management
– Exercise programs
– Stress management
45
www.bcbswny.com
How to access DM/CM services
• Fax referral form to 716-887-7913
• Phone – call 1-877-878-8785, option 2
• Member self referral online at
DM = “Disease mangement”
CM = “Case management”
46
www.bcbswny.com

47
Questions

Thank You!