Embed Size (px)
Citation preview
1
Assessing The Patient Robert Harwood, MHA, RRT-NPS
Objectives At the end of this presentation the student should be able to:
• Assess general appearance of a patient’s head, neck and face, including venous distention, edema, accessory muscle activity, chest wall movement, diaphoresis, clubbing, cyanosis and breathing pattern
• Assess the patient’s airway, including macroglassia and neck range of motion
• Collect and evaluate clinical information concerning cough, sputum, and the character and amount of sputum
• Evaluate a patient’s condition using Apgar score, gestational age, and transillumination of the chest

2
General Appearance • General appearance characteristics:
Facial expression- pain Body position- tripod (COPD) Distress, diaphoresis- short of breath Look of anxiousness- hypoxia Malnutrition, emaciated, generally ill (cachexia)- COPD
• Questions with these characteristics, you would want to treat and stabilize the patient
Examination of Head and Neck Respiratory disease signs:
• Nasal flaring-increased flow rate • Cyanosis: Central vs. Peripheral
§ Central Need: requires oxygen Location: lips, nose, ears, neck region, tongue Darker pigmentation more difficult to see Look at palm of hands, oral cavity, tongue
§ Peripheral or acrocyanosis Poor circulation to extremities- cool
• Pursed-lip breathing

3
Sample Question
A patient is receiving oxygen by nasal cannula at 3 L/minute. Upon inspection you notice the patient to have central cyanosis. This would indicate the presence of cyanosis to be: a. In the feet and ankles b. In the neck region and lips c. In the hands, fingers and wrists d. From the knees to the ankles
Sample Question Answers b. Correct answer-Neck region, lips, tongue, ears
4
Examination of Head and Neck
• EYES • Normal- pupils equal, round, reactive to light PERRLA • Dilated and fixed pupils- brain death - Miadriasis • Pinpoint pupils - Miosis (opiates) • Double vision - Diplopia • Neuromuscular disease, e.g. Myasthenia gravis
Examination of Head and Neck • NECK
• Normal tracheal position: midline Assess: palpation of suprasternal notch
• Abnormal tracheal position Shift toward affected lung - pull
Shift away from affected lung - push
Severe Atelectasis
Pneumothorax, pleural effusion
Opposite Lung
5
Examination of Head and Neck • Jugular Venous Pressure
• Level of column of blood in jugular vein reflects:
• Abnormal conditions Right sided heart failure from:
Head elevated 45° degrees-distention 3-4 cm above sternal angle to angle of the jaw is abnormal
Volume Pressure Right Heart
Chronic hypoxemia-COPD Secondary to left-sided heart failure-CHF
Sample Question A male COPD patient is being assessed in the ICU following admission for acute exacerbation of his condition. The patient is lying in bed with the head of the bed at a 45° angle. Upon inspection, it is noticed that the jugular vein is distended to the jaw line. This finding would indicate the presence of which of the following? a. Anemia b. Polycythemia c. Kidney failure d. Right-sided heart failure

6
Sample Question Answer d. Correct answer. Right sided heart failure can occur from
chronic hypoxemia or 2nd to CHF.
Examination of Thorax • Inspection to determine
Normal thorax: Anterior Posterior (AP) diameter < transverse diameter Abnormal AP diameter = barrel chest
Common in COPD (emphysema), CF Ribs loose normal 45º angle = horizontal
• Other Abnormal Thorax Inspection Pectus carinatum - chest characterized by a protrusion of the sternum and ribs Pectus excavatum - a caved-in or sunken appearance of the chest Kyphosis - over-curvature of the thoracic vertebrae (upper back) Scoliosis - person's spine is curved from side to side Kyphoscoliosis - combination of kyphosis and scoliosis Flail chest - detachment of the rib cage from the chest wall causing the flail segment to move in the opposite direction as the rest of the chest 2-2 rule: two ribs broken in 2 adjacent places
7
Accessory Muscle Activity • Indicates need for greater air flow • Patient has an increased work of breathing • Associated with diaphoresis, increased heart rate, desaturation • Cardiopulmonary disease increased use of accessory muscles of
inspiration and expiration • Retractions- increased airway resistance and decreased lung
compliance Substernal retractions Intercostal retractions
Sample Question Upon inspection of the head, neck and thorax, you notice the patient has respiratory distress and increased work of breathing. Which of the following would be present to indicate this finding?
I. Nasal flaring II. Pitting edema III. Jugular vein distention IV. Intercostal retractions a. I, II b. I, IV c. I, II, III d. I, II, III, IV
8
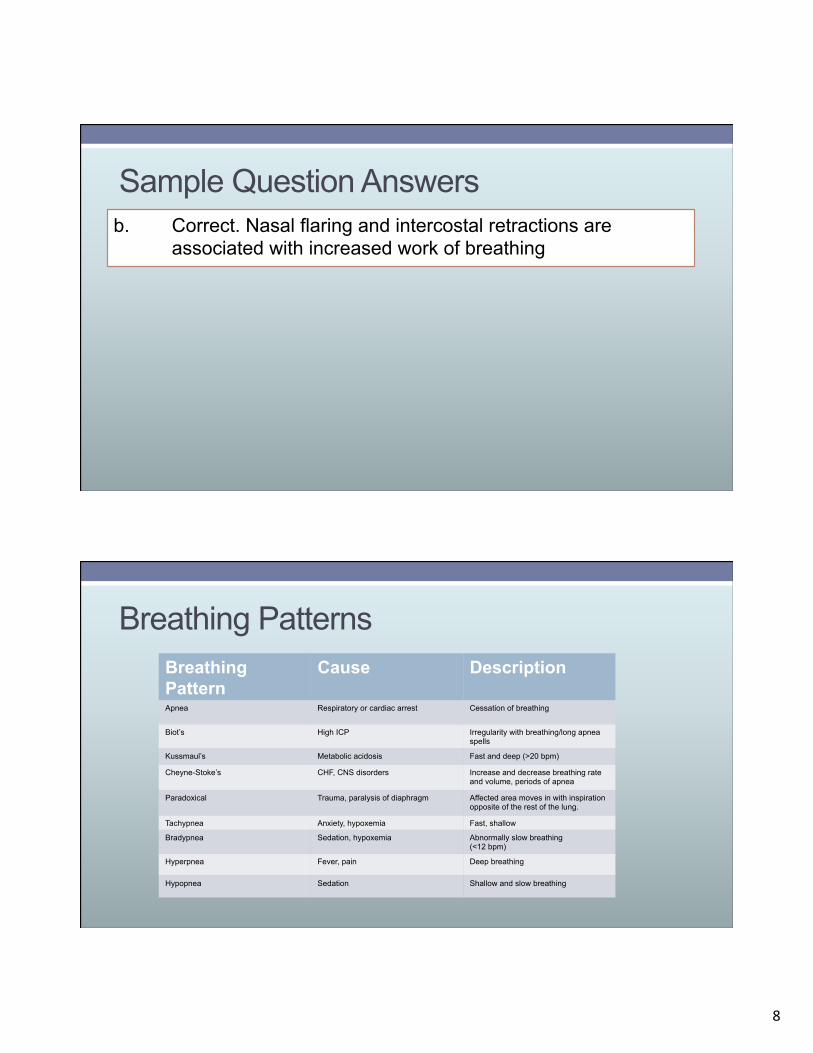
Sample Question Answers b. Correct. Nasal flaring and intercostal retractions are
associated with increased work of breathing
Breathing Patterns Breathing Pattern
Cause Description
Apnea Respiratory or cardiac arrest Cessation of breathing
Biot’s High ICP Irregularity with breathing/long apnea spells
Kussmaul’s Metabolic acidosis Fast and deep (>20 bpm)
Cheyne-Stoke’s CHF, CNS disorders Increase and decrease breathing rate and volume, periods of apnea
Paradoxical Trauma, paralysis of diaphragm Affected area moves in with inspiration opposite of the rest of the lung.
Tachypnea Anxiety, hypoxemia Fast, shallow
Bradypnea Sedation, hypoxemia Abnormally slow breathing (<12 bpm)
Hyperpnea Fever, pain Deep breathing
Hypopnea Sedation Shallow and slow breathing
9
Sample Question A patient has returned from a procedure requiring administration of a sedative. After evaluating the patient, the respiratory therapist charts that the patient has hypopnea. This type of breathing pattern would be associated with which of the following? a. Fast and shallow b. Irregular breathing with periods of apnea c. Shallow and slow breathing d. Deep breathing with snoring
Sample Question Answer c. Correct. Hypopnea is shallow and slow breathing.
10
Sample Question A 23-year-old male is in the ED for contusions sustained from a fall while pruning a tree. He is receiving 40% oxygen by air-entrainment mask. Upon inspection, it is noticed that the patient’s right chest sinks in during inspiration while the rest of the chest rises. This type of breathing pattern would be referred to as which of the following? a. Kussmaul’s b. Paradoxical c. Cheyne-Stoke’s d. Pneumonic
Sample Question Answers
b. Correct- affected area moves in with inspiration opposite to the rest of the lung
a. Not correct- fast, deep breathing c. Incorrect- Increased and decreased breathing rate and
volume, periods of apnea d. Incorrect- no such breathing pattern
11
Inspection of Extremities • Digital Clubbing
Manifestation of chronic cardiopulmonary disease seen in Cystic Fibrosis, bronchiectasis, COPD Enlargement of the phalanges of the fingers and toes Angle of the nail advances past 180 degrees
• Edema Soft-tissue swelling. Pitting edema is present. Localized or generalized (anasarca) Associated with kidney, liver, cardiac, pulmonary disease, and venous or lymphatic drainage obstruction Unilateral peripheral edema- may be from venous obstruction
Inspection of Extremities • Bilateral peripheral (dependent) edema
Cause: Cor pulmonale - right heart failure • Progression: feet and ankles = abdominal organs = hepatomegaly
= jugular vein distension • Pitting edema scale
Normal: Pitting returns rapidly Severe: >2 minutes
• 1+ trace (around ankles) to 4+ severe (well above knee)
12
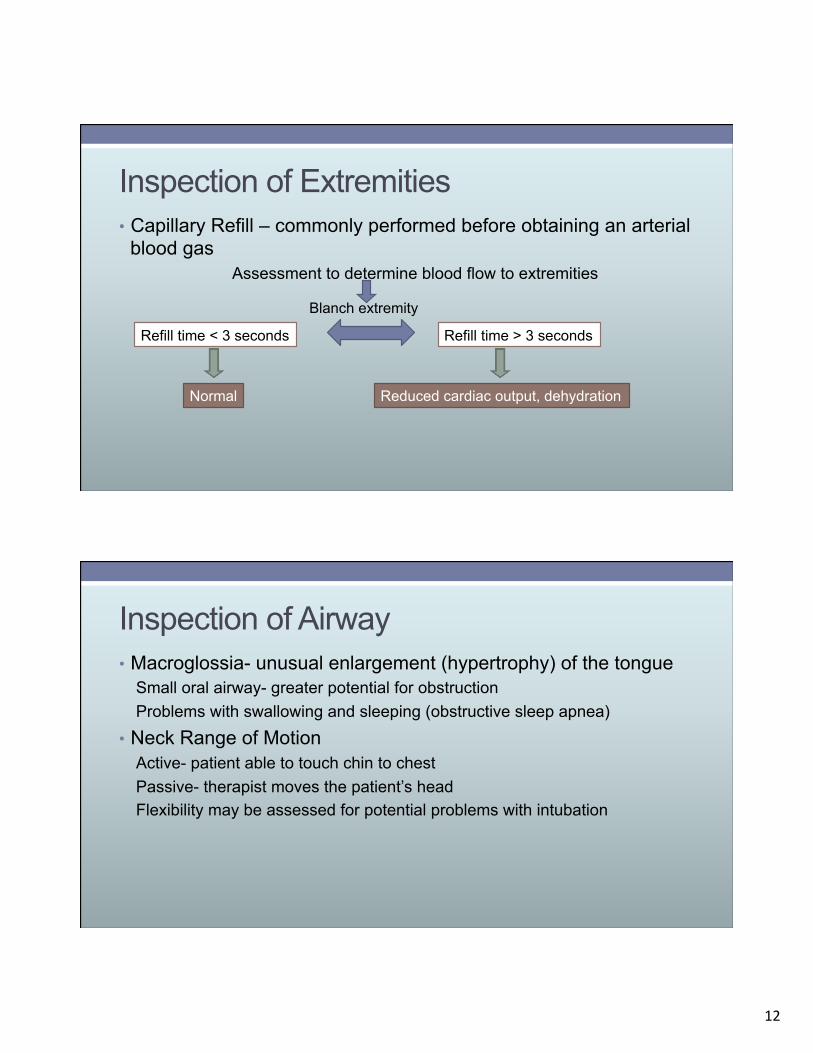
Inspection of Extremities • Capillary Refill – commonly performed before obtaining an arterial
blood gas Assessment to determine blood flow to extremities
Blanch extremity
Refill time < 3 seconds
Normal
Refill time > 3 seconds
Reduced cardiac output, dehydration
Inspection of Airway • Macroglossia- unusual enlargement (hypertrophy) of the tongue
Small oral airway- greater potential for obstruction Problems with swallowing and sleeping (obstructive sleep apnea)
• Neck Range of Motion Active- patient able to touch chin to chest Passive- therapist moves the patient’s head Flexibility may be assessed for potential problems with intubation
13
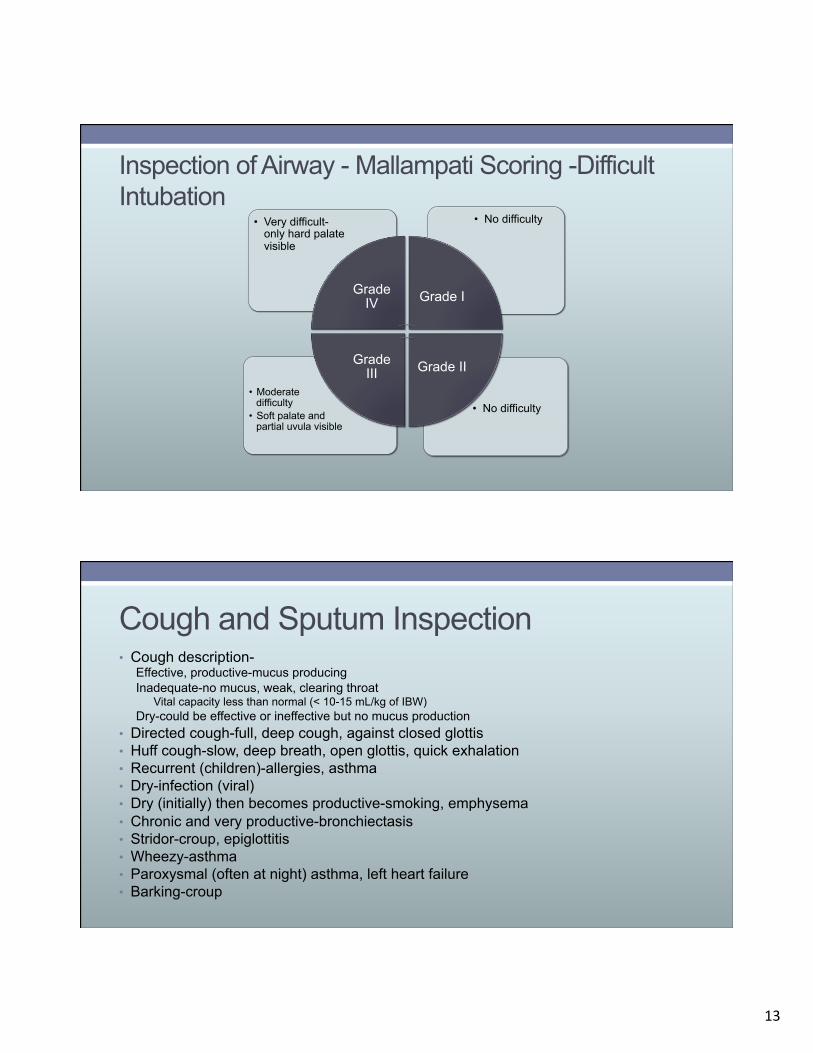
Inspection of Airway - Mallampati Scoring -Difficult Intubation
• No difficulty • Moderate
difficulty • Soft palate and
partial uvula visible
• No difficulty • Very difficult-only hard palate visible
Grade IV Grade I
Grade II Grade III
Cough and Sputum Inspection • Cough description-
Effective, productive-mucus producing Inadequate-no mucus, weak, clearing throat
Vital capacity less than normal (< 10-15 mL/kg of IBW) Dry-could be effective or ineffective but no mucus production
• Directed cough-full, deep cough, against closed glottis • Huff cough-slow, deep breath, open glottis, quick exhalation • Recurrent (children)-allergies, asthma • Dry-infection (viral) • Dry (initially) then becomes productive-smoking, emphysema • Chronic and very productive-bronchiectasis • Stridor-croup, epiglottitis • Wheezy-asthma • Paroxysmal (often at night) asthma, left heart failure • Barking-croup
14
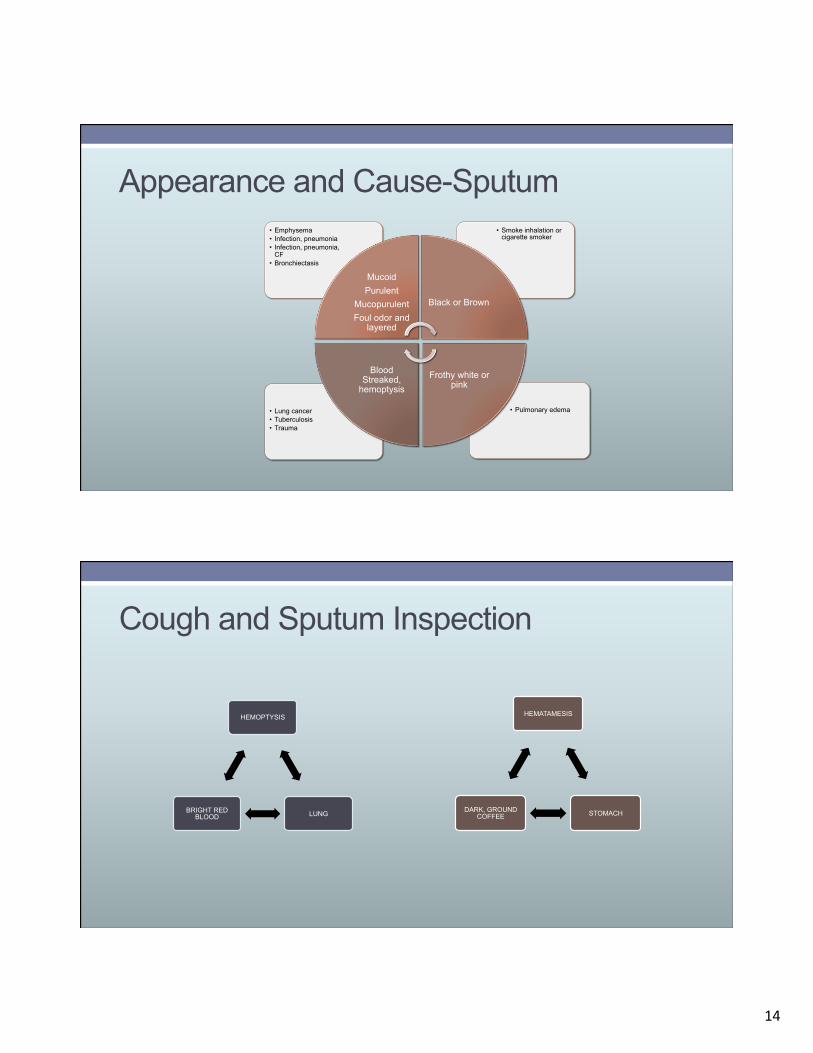
Appearance and Cause-Sputum
• Pulmonary edema • Lung cancer • Tuberculosis • Trauma
• Smoke inhalation or cigarette smoker
• Emphysema • Infection, pneumonia • Infection, pneumonia,
CF • Bronchiectasis
Mucoid Purulent
Mucopurulent Foul odor and
layered
Black or Brown
Frothy white or pink
Blood Streaked,
hemoptysis
Cough and Sputum Inspection
HEMOPTYSIS
LUNG BRIGHT RED BLOOD
HEMATAMESIS
STOMACH DARK, GROUND COFFEE
15
Cough and Sputum Inspection
TYPES OF COUGH
ACUTE < 3 weeks
Common Cold
SUBACUTE 3-8 weeks
Respiratory Tract Infection CHRONIC
> 8 WEEKS Asthma GERD
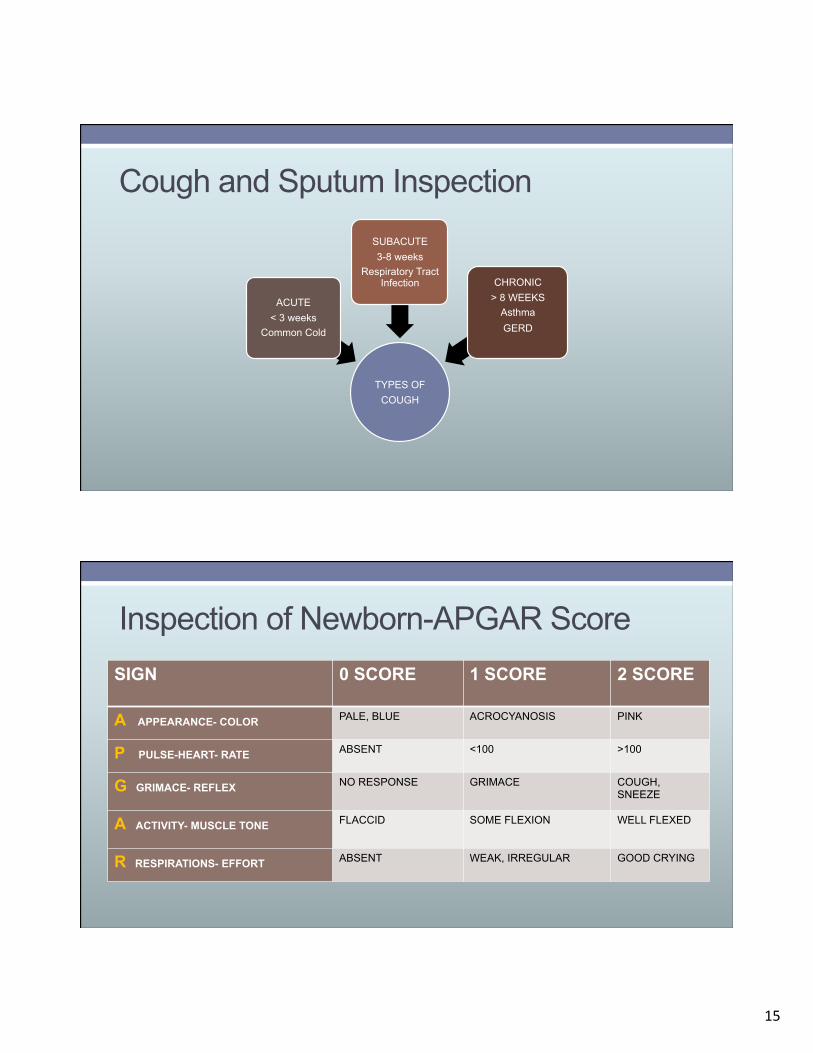
Inspection of Newborn-APGAR Score SIGN 0 SCORE 1 SCORE 2 SCORE
A APPEARANCE- COLOR PALE, BLUE ACROCYANOSIS PINK
P PULSE-HEART- RATE ABSENT <100 >100
G GRIMACE- REFLEX NO RESPONSE GRIMACE COUGH, SNEEZE
A ACTIVITY- MUSCLE TONE FLACCID SOME FLEXION WELL FLEXED
R RESPIRATIONS- EFFORT ABSENT WEAK, IRREGULAR GOOD CRYING
16
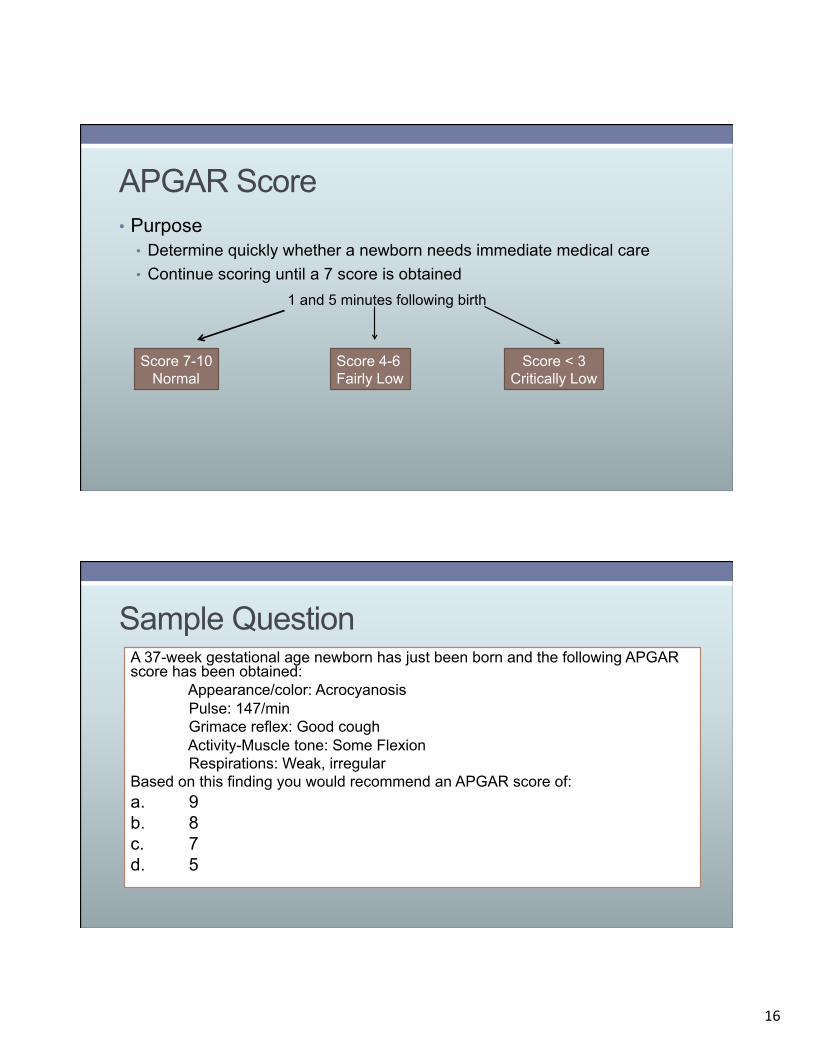
APGAR Score • Purpose
• Determine quickly whether a newborn needs immediate medical care • Continue scoring until a 7 score is obtained
1 and 5 minutes following birth
Score 7-10 Normal
Score 4-6 Fairly Low
Score < 3 Critically Low
Sample Question A 37-week gestational age newborn has just been born and the following APGAR score has been obtained:
Appearance/color: Acrocyanosis Pulse: 147/min Grimace reflex: Good cough Activity-Muscle tone: Some Flexion Respirations: Weak, irregular
Based on this finding you would recommend an APGAR score of: a. 9 b. 8 c. 7 d. 5
17
Sample Question Answer c. Correct: Score of 7
Appearance/color: Acrocyanosis – 1 point Pulse: 147/min – 2 points Grimace reflex: Good cough – 2 points Activity-Muscle tone: Some Flexion – 1 point Respirations: Weak, irregular – 1 point
Gestational Age Assessment
GESTATIONAL AGE
ASSESSMENT
Maternal Dates
Fetal Ultrasound
Ballard Scoring
Dubowitz Scoring
18
Inspection of Newborn Chest
Transillumination of Chest
Normal Findings: Halo appearance on chest
Abnormal Findings: Area under light “lights up” from air or fluid
References Clinical Assessment in Respiratory Care, Sixth Edition, Robert L. Wilkins, James R.
Dexter, Albert J. Heuer, (2009), The Mosby/Elsevier Company, St. Louis, MO. Egan’s Fundamentals of Respiratory Care, Ninth Edition, Robert L. Wilkins, James K.
Stoller, Robert M. Kacmarek, (2009), Mosby/Elsevier Company, St. Louis, MO Respiratory Care Principles and Practice, Second Edition, Dean R. Hess, Neil R.
MacIntyre, Shelley C. Mishoe, William F. Galvin, Alexander B. Adams, (2011), Jones and Bartlett Learning, Sudbury, MA
The Essentials of Respiratory Care. Robert M. Kacmarek, Steven Dimas, Craig W. Mack (2005). Fourth Edition. Mosby/Elsevier, St. Louis, MO
Perinatal and Pediatric Respiratory Care. Brian K. Walsh, Michael P Czervinske, Robert M. DiBlasi (2010). Saunders Elsevier, St. Louis, MO





























