Embed Size (px)
Citation preview
Aspirin and paracetamol tolerance in patientswith nimesulide-induced urticariaRiccardo Asero, MD
Background: The administration of aspirin and other nonsteroidal anti-inflam-matory drugs in patients sensitive to nimesulide might be hazardous.Objective: To assess the tolerance to both acetaminophen (paracetamol) and
aspirin in patients with a history of urticaria induced by nimesulide.Methods: Nine patients with a history of nimesulide intolerance were submitted
to single-blind, placebo-controlled peroral challenges with increasing doses ofacetaminophen and aspirin.Results: Acetaminophen was tolerated by all patients, whereas two experienced
immediate systemic urticaria after the administration of 125 mg of aspirin.Conclusion: Acetaminophen and aspirin are well tolerated by most nimesulide-
sensitive patients. Since a minority of patients show aspirin sensitivity, tolerance ofthis agent should always be ascertained by properly performed peroral challenges.
Ann Allergy Asthma Immunol 1998;81:237–238.
INTRODUCTIONIn most patients with pseudo-allergicreactions induced by aspirin or relatednonsteroidal anti-inflammatory drugs,nimesulide (4-nitro-2-phenoxymeth-anesulfanilide), along with acetamino-phen (paracetamol), represents a well-tolerated alternative drug.1–3 This factis probably associated with its weakinhibitory effect on cyclooxygenase,4an enzyme generally considered of cru-cial importance in the pathogenesis ofadverse reactions induced by anti-in-flammatory drugs. Nimesulide’s anti-in-flammatory effects are most probablyrelated to its oxygen radical-scaveng-ing activity and to the inhibition ofsuperoxide anion production.2,5 Nime-sulide intolerance is rare3; nonetheless,some patients experience their first ep-isode of drug-induced urticaria afterthe ingestion of this agent. In thesesubjects, the administration of fulldose aspirin or other nonsteroidal anti-inflammatory drugs might be hazard-ous since nimesulide intolerance mightrepresent the first sign of a more gen-
eral intolerance to anti-inflammatorydrugs. It is generally accepted that withmost drugs, the only way to rule outintolerance is to administer a test dose,followed by increments up to thescheduled therapeutical dose, by theroute used in treatment.3,6 In this study,tolerance to both acetaminophen andaspirin was assessed in nimesulide-sensitive subjects.
PATIENTS AND METHODSNine patients (two men and sevenwomen; mean age 39 years, range 22to 65 years) seen at this allergy centerbetween January 1993 and December1997 were studied. All had an un-equivocal clinical history of recentepisodes of systemic urticaria/angio-edema following nimesulide adminis-tration. One of them had experiencedtwo episodes of urticaria. In two otherpatients nimesulide-induced urticarialrash was associated with Stevens-Johnson syndrome and with laryngealedema, respectively. Three patientssuffered from respiratory allergies andtwo had a history of intolerance todrugs other than nimesulide (sulfame-thoxazole-trimethoprim and penicil-lins, respectively). Tolerance to bothacetaminophen and aspirin was as-sessed by single-blind, placebo-con-
trolled peroral challenges. Doses givenwere (1) paracetamol: day 1 � 125mg, 250 mg, 500 mg; and (2) aspirin:day 1 � 50 mg, 125 mg; day 2 � 250mg, and 500 mg. Placebo capsuleswere given at the beginning of eachsession. Doses were given one hourapart and patients were controlled forat least one hour after the last provoc-ative dose. Patients were also seen onday 2 (paracetamol) or 3 (aspirin) inorder to detect possible late reactions.The two study drugs were challengedat least 1 week apart. All patients gavean informed written consent beforeeach challenge session.
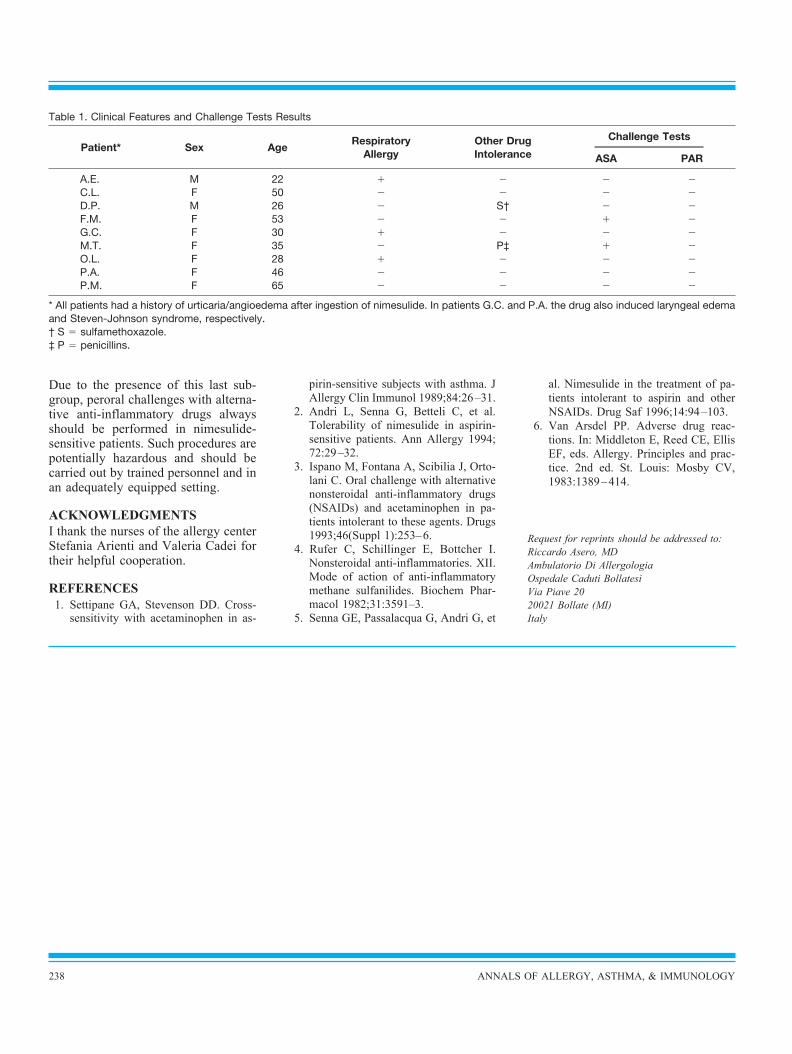
RESULTSAll patients tolerated paracetamol.Two of nine (22%) patients had urti-caria 45 to 60 minutes after the admin-istration of 125 mg of aspirin; rash waseasily controlled by conventional ther-apy. These subjects did not suffer fromrespiratory allergy; one had a historyof drug intolerance (penicillins). Clin-ical findings and challenge tests resultsare summarized in Table 1.
DISCUSSIONThis study aimed to assess acetamino-phen and aspirin tolerance in patientswho experienced the first episode ofurticaria induced by anti-inflammatorydrugs after the ingestion of nimesulide.The results of peroral challengesclearly show that seldomly does nime-sulide sensitivity represent the firstclinical sign of a more generalized in-tolerance to nonsteroidal anti-inflam-matory drugs. Most patients withnimesulide intolerance seem to have atrue allergic (IgE-mediated ?) sensitiv-ity. By contrast, in a minority of nime-sulide intolerant patients, cyclooxy-genase inhibition seems to representthe relevant pathogenetic mechanism.
From the Ambulatorio di Allergologia, Os-pedale Caduti Bollatesi, Bollate (MI), Italy.Received for publication September 12,
1997.Accepted for publication in revised form
April 8, 1998.
VOLUME 81, SEPTEMBER, 1998 237
Due to the presence of this last sub-group, peroral challenges with alterna-tive anti-inflammatory drugs alwaysshould be performed in nimesulide-sensitive patients. Such procedures arepotentially hazardous and should becarried out by trained personnel and inan adequately equipped setting.
ACKNOWLEDGMENTSI thank the nurses of the allergy centerStefania Arienti and Valeria Cadei fortheir helpful cooperation.
REFERENCES1. Settipane GA, Stevenson DD. Cross-sensitivity with acetaminophen in as-
pirin-sensitive subjects with asthma. JAllergy Clin Immunol 1989;84:26–31.
2. Andri L, Senna G, Betteli C, et al.Tolerability of nimesulide in aspirin-sensitive patients. Ann Allergy 1994;72:29–32.
3. Ispano M, Fontana A, Scibilia J, Orto-lani C. Oral challenge with alternativenonsteroidal anti-inflammatory drugs(NSAIDs) and acetaminophen in pa-tients intolerant to these agents. Drugs1993;46(Suppl 1):253–6.
4. Rufer C, Schillinger E, Bottcher I.Nonsteroidal anti-inflammatories. XII.Mode of action of anti-inflammatorymethane sulfanilides. Biochem Phar-macol 1982;31:3591–3.
5. Senna GE, Passalacqua G, Andri G, et
al. Nimesulide in the treatment of pa-tients intolerant to aspirin and otherNSAIDs. Drug Saf 1996;14:94–103.
6. Van Arsdel PP. Adverse drug reac-tions. In: Middleton E, Reed CE, EllisEF, eds. Allergy. Principles and prac-tice. 2nd ed. St. Louis: Mosby CV,1983:1389–414.
Request for reprints should be addressed to:Riccardo Asero, MDAmbulatorio Di AllergologiaOspedale Caduti BollatesiVia Piave 2020021 Bollate (MI)Italy
Table 1. Clinical Features and Challenge Tests Results
Patient* Sex AgeRespiratory
AllergyOther DrugIntolerance
Challenge Tests
ASA PAR
A.E. M 22 � � � �C.L. F 50 � � � �D.P. M 26 � S† � �F.M. F 53 � � � �G.C. F 30 � � � �M.T. F 35 � P‡ � �O.L. F 28 � � � �P.A. F 46 � � � �P.M. F 65 � � � �
* All patients had a history of urticaria/angioedema after ingestion of nimesulide. In patients G.C. and P.A. the drug also induced laryngeal edemaand Steven-Johnson syndrome, respectively.† S � sulfamethoxazole.‡ P � penicillins.
238 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY