Embed Size (px)
Citation preview

8/7/2019 artikel orto
http://slidepdf.com/reader/full/artikel-orto 1/6
8/7/2019 artikel orto
http://slidepdf.com/reader/full/artikel-orto 2/6
J. Lingual Ortho.Th. Vol.2 No.1 Jan.-Jun 20028
Anchorage management : Space obtained
from extraction one bicuspid is utilized for cor-
rection of protrusion by maximum retraction of the
anterior segment (Type A anchorage), retractionof the anterior segment and protraction of the
posterior segment (Type B anchorage) or pro-
traction of the posterior segment (Type C anchor-
age)(2). In lingual orthodontics, management of
anchorage is depended upon configuration of the
archwire and the amount of force.
Biomechanics : Asymmetric retraction of
the anterior segment should be a treatment of
choice if the dental protrusion cannot be
corrected by alteration of jaw relationship.
The objective of the article was to present
the Class II division 1 case treated with
asymmetric extraction by lingual orthodontic
mechanics.
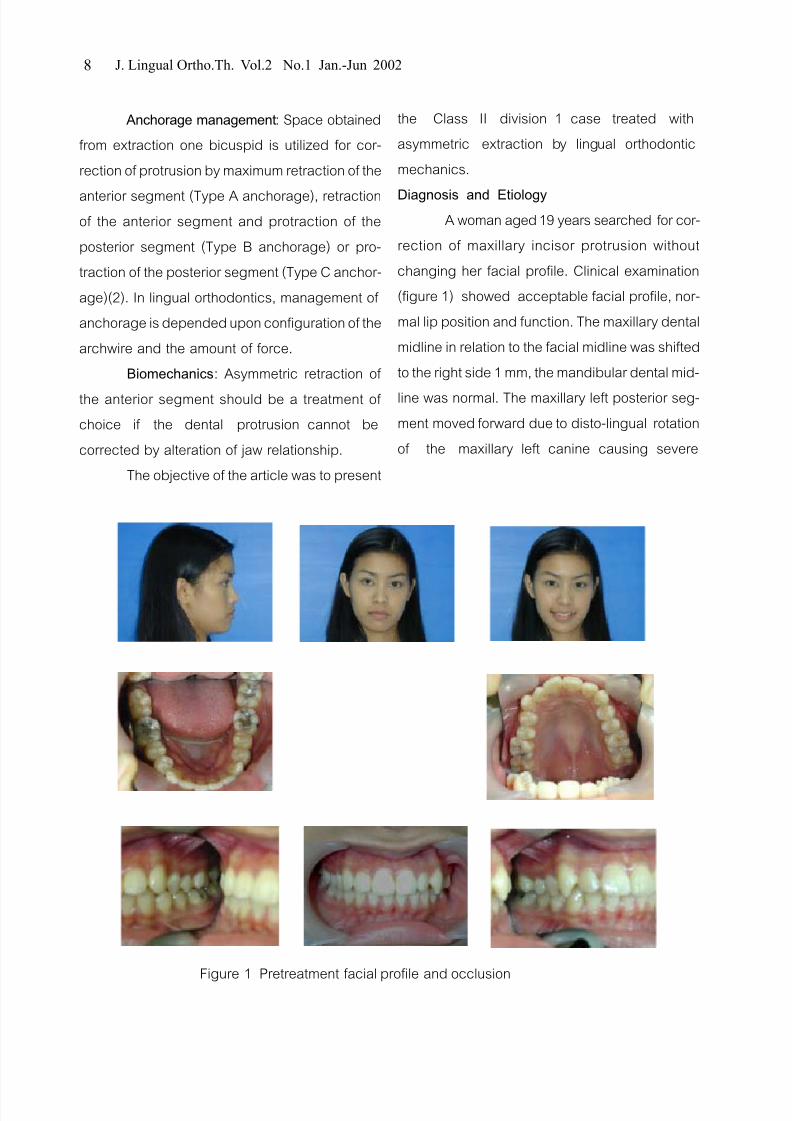
Diagnosis and EtiologyA woman aged 19 years searched for cor-
rection of maxillary incisor protrusion without
changing her facial profile. Clinical examination
(figure 1) showed acceptable facial profile, nor-
mal lip position and function. The maxillary dental
midline in relation to the facial midline was shifted
to the right side 1 mm, the mandibular dental mid-
line was normal. The maxillary left posterior seg-
ment moved forward due to disto-lingual rotation
of the maxillary left canine causing severe
Figure 1 Pretreatment facial profile and occlusion

8/7/2019 artikel orto
http://slidepdf.com/reader/full/artikel-orto 3/6
. . . . 2 1 . .-- . . 2545 9
Figure 2 Pretreatment cephalometric analysis
Figure 3 Oral features during treatment
8/7/2019 artikel orto
http://slidepdf.com/reader/full/artikel-orto 4/6
J. Lingual Ortho.Th. Vol.2 No.1 Jan.-Jun 200210
Class II molar and canine relationship around 4
mm. The maxillary right segment was slightly
Class II molar and canine relation 2 mm. The
overbite was normal while the overjet was 6 mm.The Bolton analysis showed maxillary
anterior teeth excess 2 mm.
Panoramic radiograph showed normal
development dentition.
Cephalometric analysis showed skeletal
Class I normal bite with maxillary incisor
protrusion and proclination, normal facial profile
(figure 2).
Hereditary factor should be a major
etiological factor.
Treatment Objectives
To correct maxillary incisor protrusion
while maintaining the facial profile.
To obtain Class I molar (right side), Class
II molar (left side) and Class I canine (both sides)
with normal overbite and overjet.
Extraction of the maxillary left first bicus-
pid was recommended to obtain space available
8 mm for correction of the maxillary left canine
rotation and incisor protrusion. Type B anchor-
age was selected to achieve the aforemen-
tioned occlusion.
Treatment Progress (figure 3)Edgewise lingual appliance was used for
the maxillary teeth and labial appliance was used
for the mandibular teeth. The .022x.028" Roth
vertical slot edgewise appliance (Ortho Organizer)
were placed. The treatment sequences were as
follows:
Upper Arch
1. Band #16, #26 Impression for bracket align-ment with TARG system
2. Indirect bonding #15, #12, #11, #21, #22, #25
leveling with .014"TMA
3. Insert .016"TMA after extraction #24,
direct bonding #23 Labial brackets and retract#23 with elastic chain 150 grams
4.Insert .016x.016" Blue elgiloy L loop closing loop
5. Insert .016" NiTi after complete space closure.
6. Insert .017x.025" TMA archwire
Lower Arch
1 Band #36, #46 direct bonding all remaining teeth
leveling with .0175" Superflex
2. Insert .014" stainless steel archwire
3. Insert .016" stainless steel archwire
4. Insert .018" stainless steel archwire
5. Insert .016x.022" stainless steel archwire
6. Insert .017x.025" TMA archwire
Final adjustment of occlusion with Class
II traction 4 oz. 1/4”
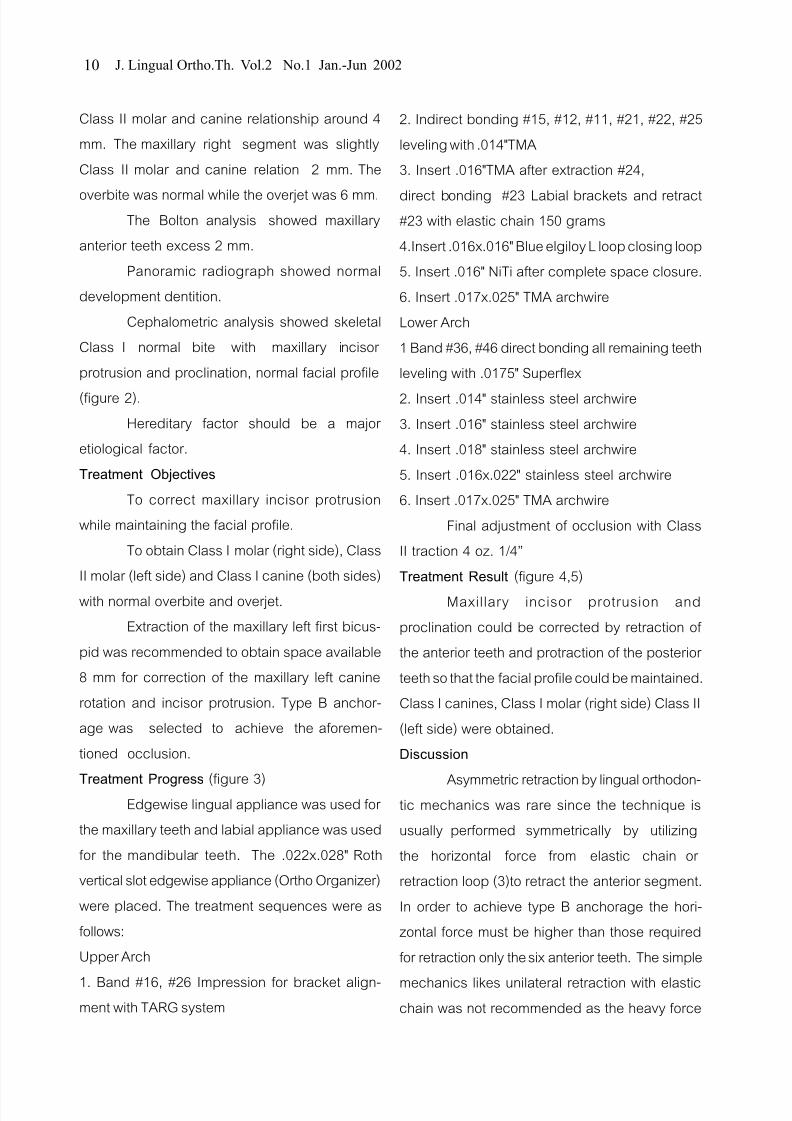
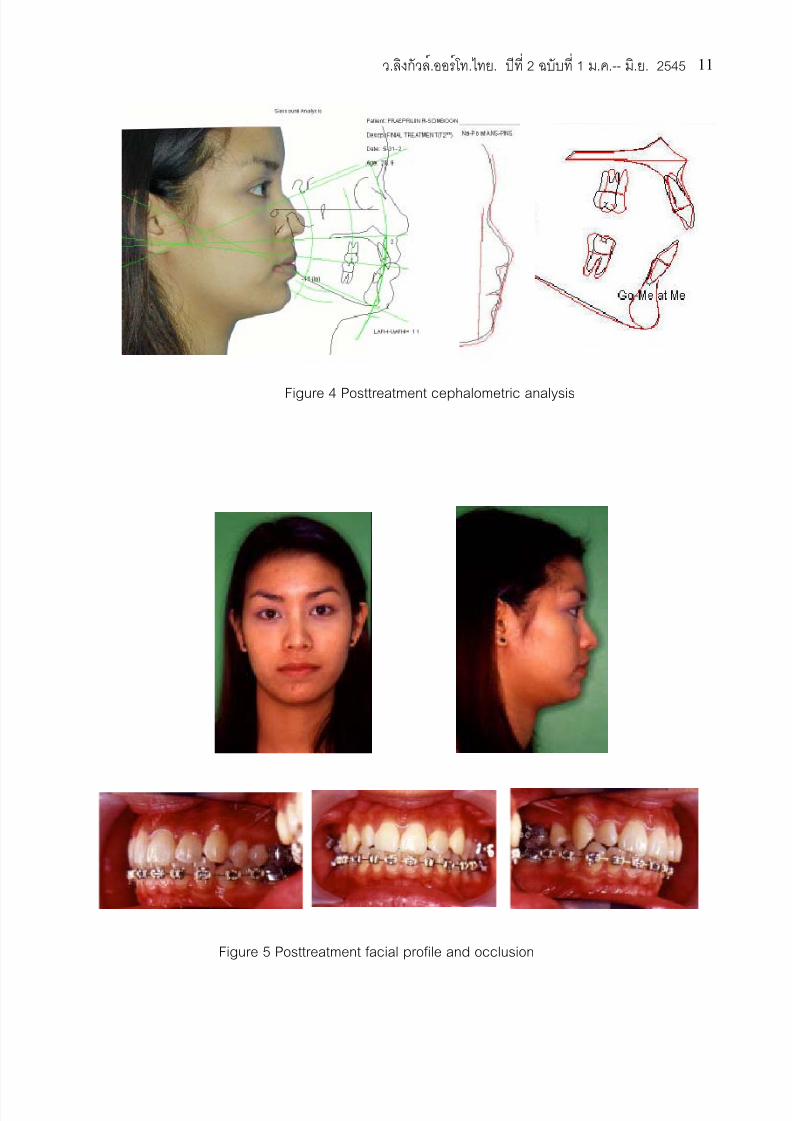
Treatment Result (figure 4,5)
Maxillary incisor protrusion and
proclination could be corrected by retraction of
the anterior teeth and protraction of the posterior
teeth so that the facial profile could be maintained.
Class I canines, Class I molar (right side) Class II
(left side) were obtained.
Discussion
Asymmetric retraction by lingual orthodon-tic mechanics was rare since the technique is
usually performed symmetrically by utilizing
the horizontal force from elastic chain or
retraction loop (3)to retract the anterior segment.
In order to achieve type B anchorage the hori-
zontal force must be higher than those required
for retraction only the six anterior teeth. The simple
mechanics likes unilateral retraction with elasticchain was not recommended as the heavy force
8/7/2019 artikel orto
http://slidepdf.com/reader/full/artikel-orto 5/6
. . . . 2 1 . .-- . . 2545 11
Figure 4 Posttreatment cephalometric analysis
Figure 5 Posttreatment facial profile and occlusion

8/7/2019 artikel orto
http://slidepdf.com/reader/full/artikel-orto 6/6
J. Lingual Ortho.Th. Vol.2 No.1 Jan.-Jun 200212
References
1. Marcotte MR. The use of occlusogram in
planning orthodontic treatment. Am J Orthod.
1976;69:655-67.2. Burstone CJ. The segmented arch approach
to space closure. Am J Orthod.1982;82:361-78.
3. Alexander CM., Alexander RG., Gorman JC.
et al. Lingual orthodontics: A status report part
5 lingual mechanotherapy. J Clin Orthod
1983;17:99-115.
might cause distortion of the archwire thus ended
up with asymmetric arch form. In order to mini-
mize this side effect the L loop retraction archwire
was used with minimal attachment to the teeth of the nonextraction side. Initial retraction of the
maxillary left canine with both labial and lingual
mechanics was necessary for controlling rotation
of the canine and enabling the perfect engage-
ment of the canine slot to the retraction archwire.
Acknowledgement The authors would like to express our sincerely thanks to the patient for
her contributions as the subject of the presentation.