Embed Size (px)
Citation preview
(p�.004). Risk factors that did not correlate with low BMD included sex,type of IBD, disease location, cumulative lifetime steroid dose, diseaseduration, history of surgical resections, and family history of osteoporosis.Two of 45 (4%) patients had asymptomatic compression fractures seen onradiographs.Conclusions: A significant proportion of a cohort of IBD patients living inthe southeastern United States have low BMD. African-American race,advanced age, low BMI, and severe disease are identified as risk factors forlow BMD in this group of patients.
776
ARE LABORATORY TESTS EFFECTIVE IN ASSESSINGDISEASE ACTIVITY IN INFLAMMATORY BOWEL DISEASE(IBD)?Michelle V. Smedley, M.D., Carol Bodian, Dr., P.H.,James H. Boone, M.S., Daniel H. Present, M.D.*. Mount Sinai SOM,New York, NY and TechLab, Inc., Blacksburg, VA.
Purpose: Fecal lactoferrin, a heat stable neutrophil derived protein, hasbeen shown to differentiate IBD from irritable bowel syndrome. This is apilot study to assess the correlation of a quantitative ELISA specific forhuman lactoferrin in feces (fL), C-reactive protein (CRP), ErythrocyteSedimentation Rate (ESR), and platelet count (plt) with clinical diseaseactivity in CD and UC.Methods: We calculated Crohn’s Disease Activity Index (CDAI) and aClinician’s Global Assessment (CGA) for CD and a modified Mayo Indexfor UC. Patients then provided blood and a spot stool sample.Results: We enrolled 47 patients, 25 females and 22 males. Thirty patientshad CD (11 ileal, 14 ileocolonic, and 5 colonic). The disease pattern waspenetrating in 13, fibrostenotic in 4, and inflammatory in 13. We proposeda cut-off value for fL at 50ug/g for active CD. This level of fL had asensitivity of 88.9% and specificity of 76 % in differentiating remissionfrom active disease via the CDAI (ROC area .899). The Kappa agreementbetween active disease, defined as CDAI �150, and fL � 50ug/g was 0.62in isolated ileal disease (n�11) and 0.49 in colonic disease (n�19).Seventeen patients had UC (extensive 10, left sided 3, and proctosigmoid-itis 4). We proposed a cut-off value for fL at 15 ug/g for active UC. Thislevel of fL had a sensitivity of 72.7% and specificity of 100% in differ-entiating remission from active disease via the Mayo Index (ROC area.985). The Kappa agreement between active disease in UC and fL � 15ug/g was 1.0 when disease was confined to the left colon (n�7) and 0.4 inextensive disease (n�10).
Spearman Correlation Coefficients for Disease Activity and Laboratory Tests
CDAI CGA (CD) Mayo Index
Fecal Lactoferrin 0.66 (p�0.0001) 0.46 (p�0.01) 0.89 (p�0.0001)ESR 0.46 (p�0.01) 0.28 (p�0.14) 0.04 (p�0.87)Platelets 0.32 (p�0.08) 0.16 (p�0.41) 0.68 (p�0.003)CRP 0.38 (p�0.08) 0.07 (p�0.75) 0.65 (p�0.005)
Conclusions: Of the laboratory tests we studied stool lactoferrin had thestrongest correlation with IBD activity. CRP and plts did not correlate withwith CD activity while ESR did not correlate with UC activity. Fecallactoferrin may be the best laboratory test to measure inflammation in IBD.
777
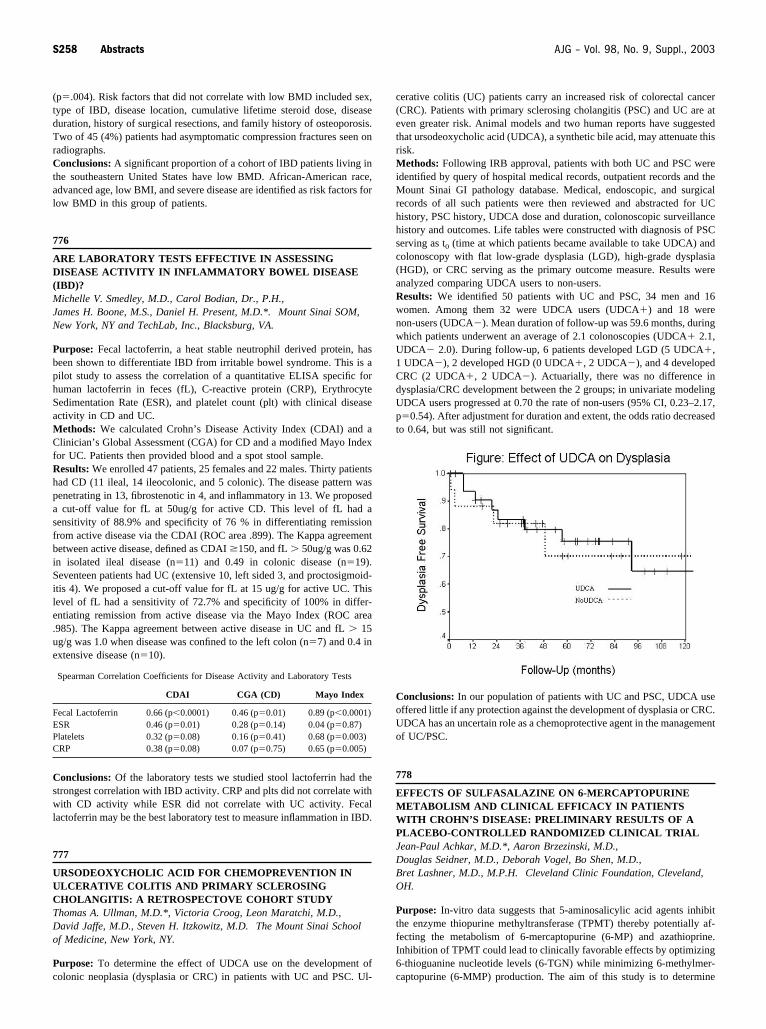
URSODEOXYCHOLIC ACID FOR CHEMOPREVENTION INULCERATIVE COLITIS AND PRIMARY SCLEROSINGCHOLANGITIS: A RETROSPECTOVE COHORT STUDYThomas A. Ullman, M.D.*, Victoria Croog, Leon Maratchi, M.D.,David Jaffe, M.D., Steven H. Itzkowitz, M.D. The Mount Sinai Schoolof Medicine, New York, NY.
Purpose: To determine the effect of UDCA use on the development ofcolonic neoplasia (dysplasia or CRC) in patients with UC and PSC. Ul-
cerative colitis (UC) patients carry an increased risk of colorectal cancer(CRC). Patients with primary sclerosing cholangitis (PSC) and UC are ateven greater risk. Animal models and two human reports have suggestedthat ursodeoxycholic acid (UDCA), a synthetic bile acid, may attenuate thisrisk.Methods: Following IRB approval, patients with both UC and PSC wereidentified by query of hospital medical records, outpatient records and theMount Sinai GI pathology database. Medical, endoscopic, and surgicalrecords of all such patients were then reviewed and abstracted for UChistory, PSC history, UDCA dose and duration, colonoscopic surveillancehistory and outcomes. Life tables were constructed with diagnosis of PSCserving as t0 (time at which patients became available to take UDCA) andcolonoscopy with flat low-grade dysplasia (LGD), high-grade dysplasia(HGD), or CRC serving as the primary outcome measure. Results wereanalyzed comparing UDCA users to non-users.Results: We identified 50 patients with UC and PSC, 34 men and 16women. Among them 32 were UDCA users (UDCA�) and 18 werenon-users (UDCA�). Mean duration of follow-up was 59.6 months, duringwhich patients underwent an average of 2.1 colonoscopies (UDCA� 2.1,UDCA� 2.0). During follow-up, 6 patients developed LGD (5 UDCA�,1 UDCA�), 2 developed HGD (0 UDCA�, 2 UDCA�), and 4 developedCRC (2 UDCA�, 2 UDCA�). Actuarially, there was no difference indysplasia/CRC development between the 2 groups; in univariate modelingUDCA users progressed at 0.70 the rate of non-users (95% CI, 0.23–2.17,p�0.54). After adjustment for duration and extent, the odds ratio decreasedto 0.64, but was still not significant.
Conclusions: In our population of patients with UC and PSC, UDCA useoffered little if any protection against the development of dysplasia or CRC.UDCA has an uncertain role as a chemoprotective agent in the managementof UC/PSC.
778
EFFECTS OF SULFASALAZINE ON 6-MERCAPTOPURINEMETABOLISM AND CLINICAL EFFICACY IN PATIENTSWITH CROHN’S DISEASE: PRELIMINARY RESULTS OF APLACEBO-CONTROLLED RANDOMIZED CLINICAL TRIALJean-Paul Achkar, M.D.*, Aaron Brzezinski, M.D.,Douglas Seidner, M.D., Deborah Vogel, Bo Shen, M.D.,Bret Lashner, M.D., M.P.H. Cleveland Clinic Foundation, Cleveland,OH.
Purpose: In-vitro data suggests that 5-aminosalicylic acid agents inhibitthe enzyme thiopurine methyltransferase (TPMT) thereby potentially af-fecting the metabolism of 6-mercaptopurine (6-MP) and azathioprine.Inhibition of TPMT could lead to clinically favorable effects by optimizing6-thioguanine nucleotide levels (6-TGN) while minimizing 6-methylmer-captopurine (6-MMP) production. The aim of this study is to determine
S258 Abstracts AJG – Vol. 98, No. 9, Suppl., 2003







![Inflammatory Bowel Disease - BSWHealth.med · Inflammatory Bowel Disease: ... • Infectious colitis: Salmonella, E. coli, ... IBD Path Pitfalls Handout.ppt [Compatibility Mode]](https://img.dokumen.tips/doc/110x75/5cc8e3e088c9937c048b644f/inflammatory-bowel-disease-inflammatory-bowel-disease-infectious.jpg)





















