Embed Size (px)
Citation preview

Approach to patients with malignancies
Semmelweis University
Internal medicine II. Department
2017.10.17
Approach?Treatment? Cure?
• Stigma
• Fear
• Symptoms not well definite
• Multidisciplinary
• Emotions ?
• Stigma
• Fear
• Symptoms not well definite
• Multidisciplinary
• Emotions ?
Threatening data
WHO information concerning EU states
2000-2010: mortality rates Cardiovascular disease 9,7% ↓ Respiratory disease 5,8% ↓ Malignant disease 7,2% ↑
2008-2010 incidence:
EU28 average 273,6
Hu 1. place 375,4
Cancer: death sentence or chronic
disease?
Of all the common medical diagnoses, cancer probably carries the greatest stigma and is associated with the
most fear.
Why is so agressiv
Six steps to become a cancer ’
1. Grow without a trigger (selfsufficiency in growth stimuli).
2. Don ’ t stop growing (insensitivity to inhibitory stimuli)..
3. Don ’ t die (evasion of apoptosis).
4. Don ’ t age (immortalization).
5. Feed themselves (neoangiogenesis).
6. Spread (invasion and metastasis)
Etiology : DNA level
Cancer :
-genetic disease,caused by the accumulation over time of changes to the normal DNA sequence alterations, loss, or amplification
- question to be answered:
monoclonal or polyclonal
changes are present in one progenitor cell ??
Etiology (???)
RNA viruses
Human T - cell leukaemia virus Leukaemia
HIV (and Epstein – Barr virus) Non - Hodgkin ’ s lymphoma
HIV (and human herpesvirus 8) Kaposi ’ s sarcoma
Hepatitis C virus Hepatocellular cancer
DNA viruses
Human papillomavirus Cervical cancer
Hepatitis B virus Hepatocellular cancer
Epstein – Barr virus Burkitt lymphoma,
Hodgkin ’ s disease,
nasopharyngeal cancer
Bacteria
Helicobacter pylori Gastric cancer, gastric lymphoma
Known genetic alteration
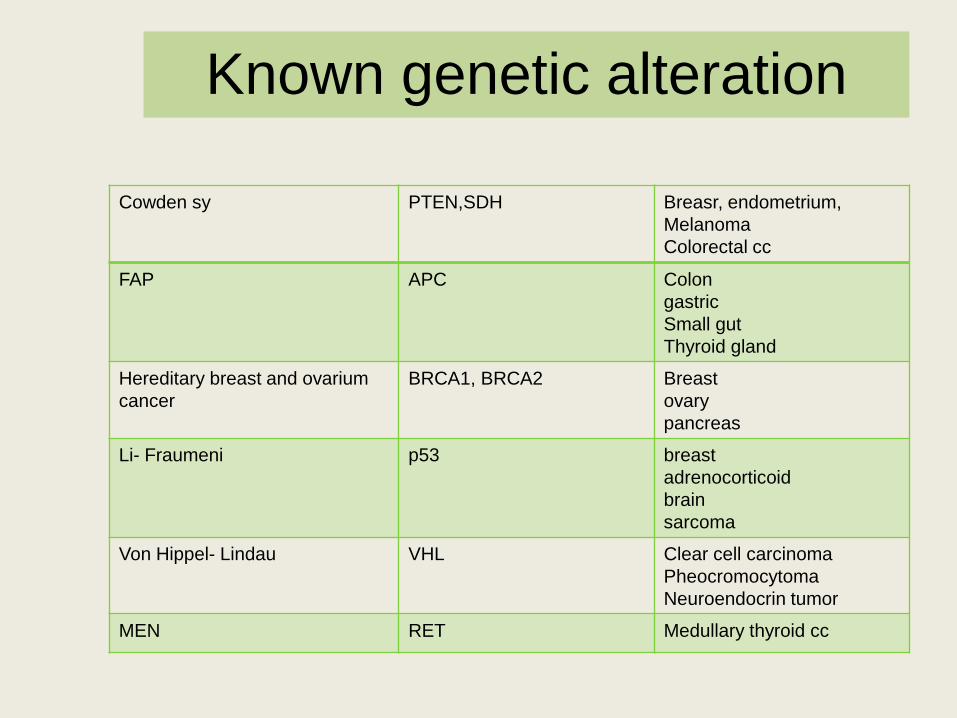
Cowden sy PTEN,SDH Breasr, endometrium,
Melanoma
Colorectal cc
FAP APC Colon
gastric
Small gut
Thyroid gland
Hereditary breast and ovarium
cancer
BRCA1, BRCA2 Breast
ovary
pancreas
Li- Fraumeni p53 breast
adrenocorticoid
brain
sarcoma
Von Hippel- Lindau VHL Clear cell carcinoma
Pheocromocytoma
Neuroendocrin tumor
MEN RET Medullary thyroid cc
When should we think at hereditary disease
Several organs effected
In body doublets both organs effected
Young patient
Tumor not used in that gender (ex.breast cancer in men)
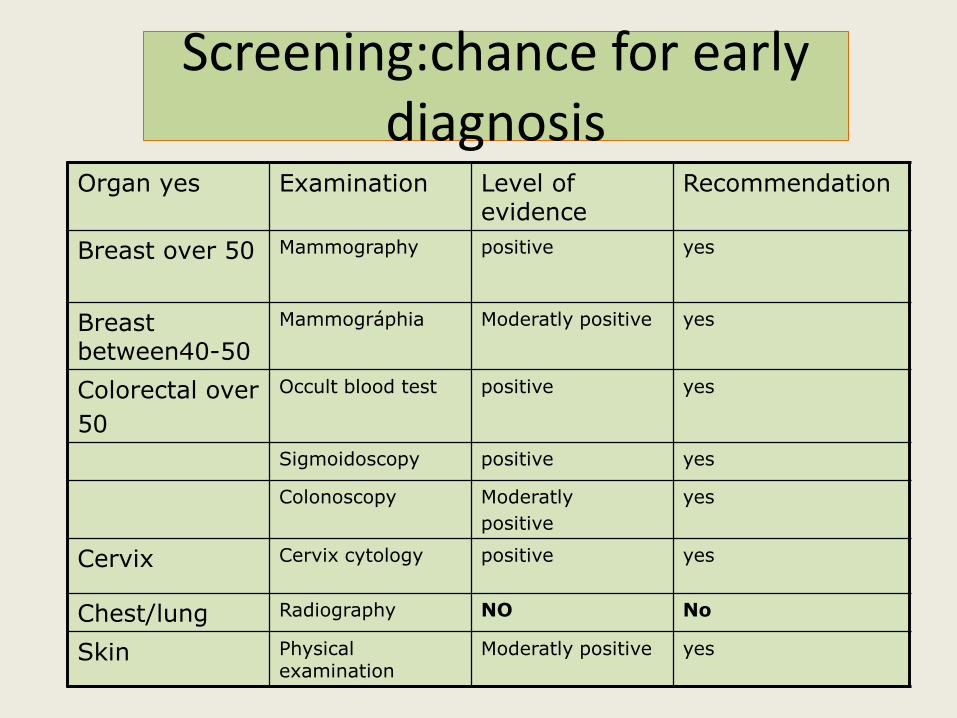
Screening:chance for early diagnosis
Organ yes Examination Level of evidence
Recommendation
Breast over 50 Mammography positive yes
Breast between40-50
Mammográphia Moderatly positive yes
Colorectal over
50
Occult blood test positive yes
Sigmoidoscopy positive yes
Colonoscopy Moderatly
positive
yes
Cervix Cervix cytology positive yes
Chest/lung Radiography NO No
Skin Physical examination
Moderatly positive yes
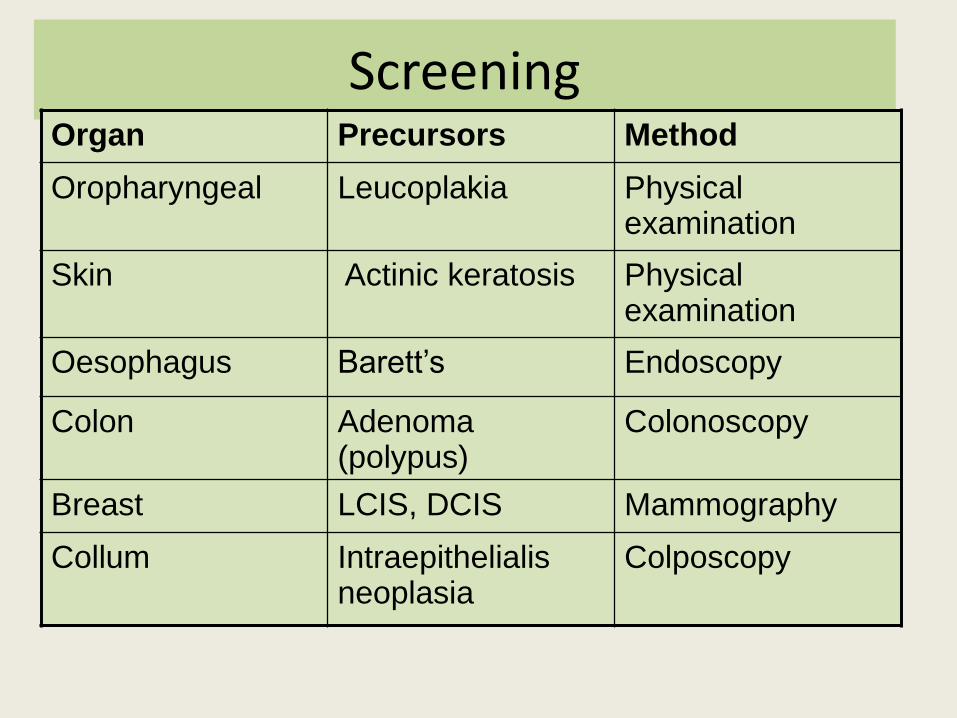
Screening Organ Precursors Method
Oropharyngeal Leucoplakia Physical examination
Skin Actinic keratosis Physical examination
Oesophagus Barett’s Endoscopy
Colon Adenoma (polypus)
Colonoscopy
Breast LCIS, DCIS Mammography
Collum Intraepithelialis neoplasia
Colposcopy
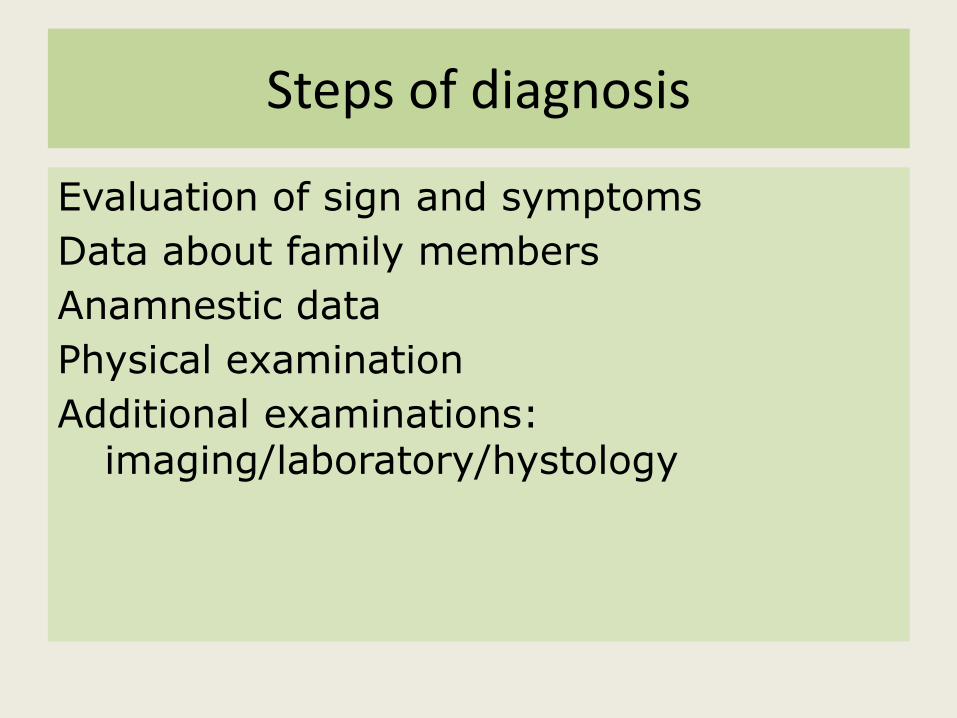
Steps of diagnosis
Evaluation of sign and symptoms
Data about family members
Anamnestic data
Physical examination
Additional examinations: imaging/laboratory/hystology
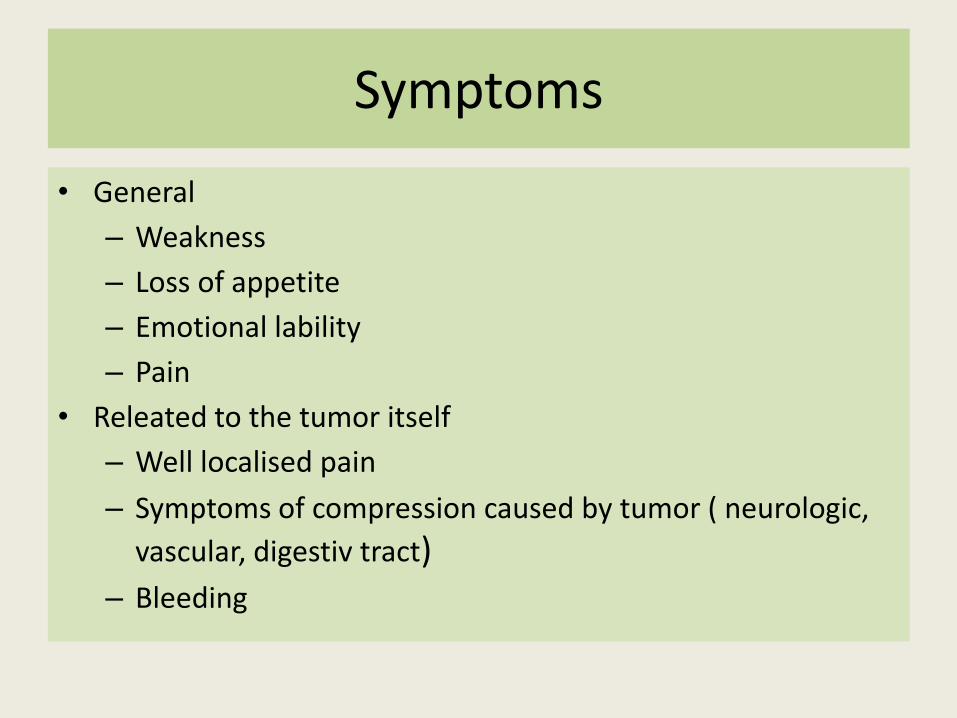
Symptoms
• General
– Weakness
– Loss of appetite
– Emotional lability
– Pain
• Releated to the tumor itself
– Well localised pain
– Symptoms of compression caused by tumor ( neurologic,
vascular, digestiv tract) – Bleeding
Evaluation of symptoms
Cause
Need for differential diagnosis
Importance of anamnestic data
• Family history
– Malignant disease among family members
• Data concerning lifestyle
– smoking
– Liquor consumption
– obesity
• Previous disease
– Pl: viral infection, inflammatory bowel disease, chronic pancreatic inflammation
Physical examination
• Colour of the skin: pale, icteric, cyanotic...
• Palpable tumor: abdominal, in the breast
• Digital rectal examination
• Examination of lymph node areas ( axillary, supraclavicular, inguinal.. )
Additional examinations
• Laboratory findings
• Imaging
• Endoscopy
• Biopsy ( FNB- cytologic, core biopsy-histology)
Tumor marker????
• No evidence in screening
• Importance:
– Follow up
– Effectiveness of therapy
– Differencial diagnosis
Prognostic concerns
• In which stage is diagnosed
• Histology: type, invasion, receptor status, genetic findings, molecular pathology exam.
• Resecability
• Age
• Operability
• Comorbidities
Therapeutic options
• Surgery
• Systemic treatment
• Radiotherapy
• Invasive radiological intervention ( chemo-embolisation, radiofrequency ablation…)
Therapeutic options after surgery
Wait and see
Systemic treatment
Radiotherapy
Other procedures/ second look surgery
Legislativ decree
2012/
Every cancer patient must be consulted by the onco-team before each treatment
The quideline, the recommended therapy should be the same, independently in wich center the patient is treated
Members of the team
Medical oncologist
Surgical oncologist
Radiation oncologist
If possible:
Pathologist
Radiologist
Oncology social worker and other health care team members
The onco-team function
Decision making
To give therapeutic options
Evaluate the results ( imaging, histology, new laesion, regression, progression )
Efficacy of therapy
• Progression free survival
• Overall survival
• Complet remission
• Partial remission
• Stable disease
• Progression – More than 25% , new lesion
Supportiv treatment
• What does it mean: – Treatment of side effects caused by active treatment
• Which symptoms generally appears – Vomiting, diarrhea, mucositis, hand-food syndroma,
anaemia, leucopenia, bleeding, hypertension
• What is the goal – To make possible to treat as planned : with the right dose,
in right time , in metastatic setting as long as needed
Palliative treatment
• What does it mean:
– The release of symptoms due to metastatic disease
• Symptoms
– Cahexia, anorexia, nausea,vomiting
– Dyspnoe
– Weakness(fatigue)
– Pain
– Secondary neurologic problems (polyneuropathy)
The importance of palliative treatment
• Targeting the quality of life:
– Focused on patients need and not on illness
• Helps the caregivers, the relatives
• Ensure a better compliance
Progressive loss of body weight with depletion of
both adipose tissue and skeletal muscle mass. At the time of diagnosis :between 15% and 20% In advanced disease : between 80% to 90% of patients are malnourished
Different origine: pain,malabsorbtion, depression
Characteristics: – Mostly loss of skeletal muscle mass
– Loss of appetite is present
– Complex process: role of enzymes ( cachectin), inflammatory cytokines..
Cachexia
Nausea/vomiting
Gastric outlet obstruction/intestinal obstruction Delayed gastric emptying Raised intracranial pressure :brain tumor or metastasis, Gastroesophageal reflux disease/gastritis/peptic ulcer Gross ascites Drugs : opioids,antibiotics, digoxin Metabolic disorders e.g., hypercalcemia, hyponatremia, liver failure, renal failure Psychological factors/ anxiety/anticipatory (conditioned) Chemotherapy/radiotherapy
Nausea/vomiting
• One of leading symptoms in advanced disease
• Freqvency : 40-70 %
• New drugs available:
– HT3 antagonist ( setron ) for chemotherapy induced vomiting 70-80% decrease
– For nausea less effectiv, other drugs reccomended metoclopramid , steroid, anxiolytics
Weakness (fatigue)
• Cause
– The primary tumor
– Treatment’s side effect
– Treatment induced anaemia.
– Physiological changes (cachexia, erőnlét csökkenése, cytokinek magas szintje)
– Psychosocial tényezők (anxiety, depression , insomnia)
Pain
• Importance – Connected to cancer, main cause of fear
Pain caused by: Tumor itself Treatment Pain not related to tumor
Influenced by Psychologic problems Social difficulties Cultural habits
Total pain
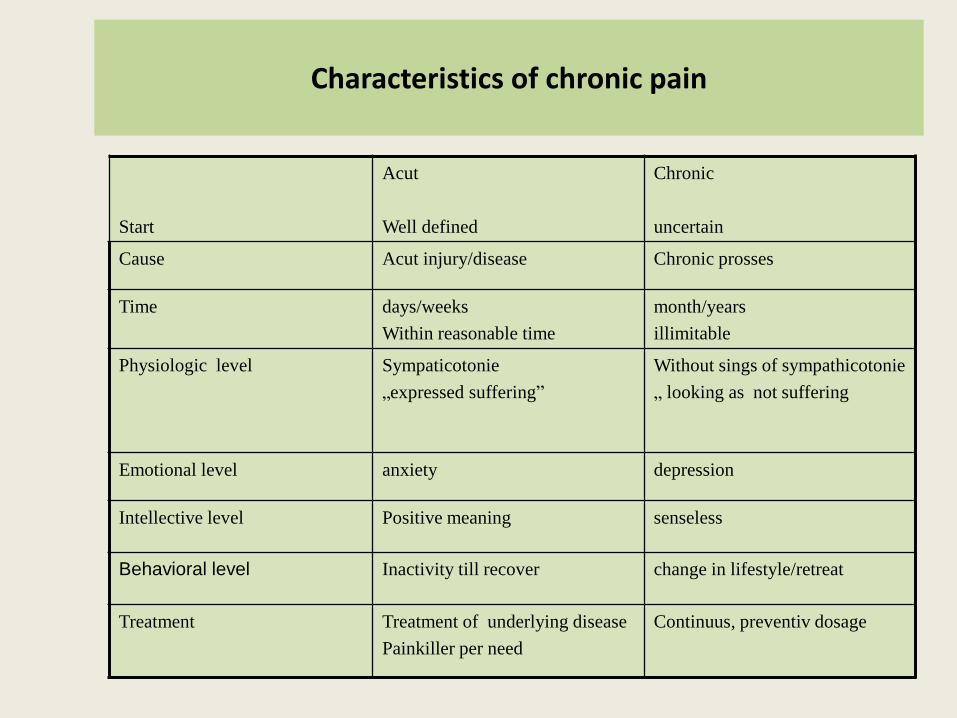
Characteristics of chronic pain
Start
Acut
Well defined
Chronic
uncertain
Cause Acut injury/disease Chronic prosses
Time days/weeks
Within reasonable time
month/years
illimitable
Physiologic level Sympaticotonie
„expressed suffering”
Without sings of sympathicotonie
„ looking as not suffering
Emotional level anxiety depression
Intellective level Positive meaning senseless
Behavioral level Inactivity till recover change in lifestyle/retreat
Treatment Treatment of underlying disease
Painkiller per need
Continuus, preventiv dosage
The goal of pain-killing
To provide the rest, to increase the number of sleeping hours To minimise the pain at rest Restore the patient's physical function, mental status, ability to work
Principles of pain-killing treatment
• Right time
• Right dose
• Right combination
• Individualized
• NOT AS NEEDED !!!!!
Importance of communication
• Breaking the bad news
• Therapeutic decision
• Side effects
• End of active treatment
• Difficulties in the terminal phase
Breaking bad news
First shock for the patient
How to be empathic enough, without crying with the patient
Subconcious present- patient doesn’t hear the reality: need for a relative around if it’s possible
Communication about treatment
Good patient-doctor relation
Give time for decision
Give more options
Give information about new drugs , side effects, alternativ treatments
Case of elderly patients
What age is considered old
Importance of commorbidity
Consider biological age
Importance of dose modification
Communication about end of treatment
Wait and see
Treatment holiday
Progressive disease
Best supportive care



























