Embed Size (px)
Citation preview
ANTONIO SOCIETY OF PATHOLOGISTS SAN ANTONIO, TEXAS
Twenty-Thhcl Annual
TUMOR SEMINAR December 3, 1966
BROOKE GENERAL HOSPITAL Brooke Army medical Center
fort Sam Houston, Texas
CONDUCTED BY
S A UL KA Y, M, V,
Professor of Surgical Pathology Medical College of Virgini a
Richmond , Virginia
This Tumor Seminar is supported in part by
THE AMERICAN CANCER SOCIETY
TEXAS DIVISI ON
The meeting will be held in the Auditorium, Building 1026 (behi nd the ~~n Hospital) , at Brooke General Hospital on December 3, 1966 , beginning at 9:00 a.m.
0 00 0 0 00 0 00 00 00
The San Anton.i.o Soci.ay o6 Pa.tltol.cg.(..6u .<.nv.UU a.U con6eJLee.6 and the.Ur. wivu
noll c.ocktai~ and bu66U 6oUowhtg .the Senli.natt, time and p!ac.e.
to be anno!Litced.
0000 00000 0 0000
Please f ill in your diagnoses on the form provided on the last page , det aqa, and mail to the Olief of Pathology Service , Brooke C.eneral llospital, Fort Sam Houston, Texas , at your ear liest convenience , so that diagnoses may be summarized prior to the meeting for presentation at t he Seminar .
CASE 1
Contributed by Dr. Kay
A 30-year-old 1~hite woman noted enlargement of the right nipple for about one year prior to admission. This was associated with bl eeding and drainage from t he surface of the nipple , Examination showed an enlarged nipple which was hard and noncyst i c , No discharge was noted, The nipple was partiall y excised under local anesthesi a.
My diagnosis : --------------------------------------
Dr. Kay's diagnosis:~-------------------------------
Comment: -------------------------------------------
CASE 2
Contr i buted by Dr . Kay
A 30-year-old colored man ~~as admitted follo1~ing a gunshot 1vound of the abdomen. Free ai r 1vas f ound under the diaphra!.'ll and the patient was explored, Three perforations of the small b01vel 1o~ere closed. An i ncidental golf-ball-sized tumor was found in the s J!'G!ll intestine which was resected. Examination of the specimen showed a segment of sma ll b01vel 8. 5 em. in l ength, Three em, from the end there was a firm , irregul ar mass approximately 2. 5 by 2 by 1.5 em. constricting the lumen. I t seemed to involve mainly the wall of the bowe l 1vith an area of mucosal u lceration,
t1y diagnosis : --------------------·---
Dr. Kay ' s diagnosis : --------------------------------
Comment : ----------------------------------------
CASt: 3
Contributed by Dr. Kay
II 50-vear-old 1~hite man was admitted in 1949 Nith a tumor in the right parot id region, first noted in 1941 as a small lump behind the ear. It gradually i ncreased in size and a f acial paralysis sl01dy developed. A large , sliw1tly movable, smooth , t ense, firm , and tender mass extended to the pre- and postauricular regions. It 1~as excised and t he entire facia l nerve 1~as found to be i nfiltrated, The tumor recurred and cervical node metastases were suspected in 1953. A biopsy was foll01~ed by radical neck dissection. The slide is from the parotid area.
My diagnosis:
Dr, Kay's diagnosis:
Comment:
CASE 4
Contributed by Dr. Kay
II 41-year-old colored 1o~oman had a left mastectomy in 1961 and a hard, 3-by-2-inch nontender mass in the U0Q of the riw1t breast in 1964. After rjght simple mastectomy a circumscribed mass, 4. S by 3. 8 by 3. 7 em., of soft to slightly firm, red-br01m tiss ue , Nas found deep in the specimen , It contained small, irregular cavities lojith ragged linings containing blood and c lotted material. Two other similar nodules k<ere adjacent to the main mass, and in the more inferior portion of the breast. Slides are identical to those of the left mastectomy,
l·ly diagnosis: -------------- --- --
Dr, Kay's diagnosis: --------------- --------
Comment: ----------- ------------- -------
CASE 5
Contributed by Dr. Norman H, Jacob Santa Rosa Medical Center , San Antonio , Texas
A 69-year-old wanan had a right parotid gland tumor removed, It weighed 6 grams, measured Z. S em. in maximum dimension, and had a lobular cyst ic pattern.
My diagnosis : - ------------ - ---- -
Dr; Kay l s ciiagnos:i.s i - ---------------
Comment:
CASE 6
Contribut ed by Drs. A. M, Ri chmond, C. J. Farinacci, and H. c. Ford , Nix Clinical Labor atory, San Antonio, Texas
The patient, an 85-year-old spinster, was brought to a physician by her neice, A mass of unknOiofD durat ion was found in the right breast, lateral to the nipple, Because of her poor physical condition a simple mastectany was performed, The specimen consisted of an ellipse of skin 14 by 7 by 6 on. with a bulging mass l ateral to the nipple covered with reddish blue dusky skin. On cut section the mass was 4 on. in diameter with a gritty, granular • dirty gray-1~hite surface flecked with small cysts fi lled 1~ith bloody fluid and/or friable yellowish gray material.
l~y diagnosis :
Dr, Kay' s diagnosis: ----- --------- ----------
Comment : ----------------- ------------------
CASE 7
Contributed by Col, Hugh B. Hoeffler and Capt . A. E. Roth Brooke General Hospital , Fort Sam Houston , Texas
A nodule was discovered on the left lobe of thyroid of an asymptomatic 52-yef~·old white f emale oo routine physical examination. I 1 uptake was normal . The no· dule was inactive to scan. The specimen 1~as a left lobe of thyroid tissue wei ghi ng 10 grams, I t contained a cen· tral nodule 1.4 em. i n diameter, Areas of the nodule were quit e firm and cut with gritty sensation ; other small nodular areas had a soft gelat i nous consistency.
~ diagnosis: -----------------------------------------------
Dr. Kay 's diagnosis: --------- - - - --- ---- -
Comment: - ------------- -------- --------
------------------------------------~
CP$E 8
Contributed by Dr. George c. Mani Santa Rosa ~~dical Center, San Antonio, Texas
A 12-year -old girl 1rith a benign hemangiooa of the left neck had striking regional adenopathy, ller admis-sion laboratory work 1~as unremarkable ,
My diagnos Js :
Dr. Kay's dia&nosis: ------ - ------------
Comrr~nt : ----------------------------------
CASE 9
Contr ibuted by Dr, A. 0 . Severance and Associates Baptist Memorial Hospital, San Antonio, Texas
A 30-year- old white female 1~as aclrnitted to the hospital for removal of a nonfunctional left kidney. She had experienced pain in the left costovertebral angle beginning one year previously and had been said to have pyuria at that time, whi'ch had been treated intermittently, She was pregnant at the time of admission and it was elected to follow her through the pregnancy before attempting surgery, A l arge 348-gram , 15-by-7,5-by-5, 3-cm. kidney containing a staghorn calculus was removed, There seemed to be essentially no normal renal parenchyma, but there ~~re multiple ragged abscesses scattered throughout the t issue. Coliform organisms were cultured fran this kidney at time of operation.
~ diagnosis: --------------------------------------
Dr. Kay's diagnosis: -------------------------
Comment : ------------------------------------
CASE 10
Contributed by Dr , James K, Lowry Santa Rosa t~edical Center, San Antonio , Texas
A 22-year-old woman had papillary tumor masses of both ovaries. One mass weighed 135 grams and measured 9 em. ; the second mass \4eighed 270 grams and measured 11 em,
My diagnosis : --------------------------------
Dr, Kay's di'a gnosis: ___________________________ _
Comment : -----------------------------------------
CASE 11
Contributed by Col. I! ugh 8 . Hoeffler and Capt . A, E. Roth Brooke General Hospital, fort Sam Houston , Texas
A 20-year-C)Jd male 1~ith a 3-month history of abdominal fullness hall a rC'tropcri toneal mass removed from the left upper quadrant. "The 560- gram, partially encapsulated specimen was composed of firm tissue in 1~hich there were large areas of cystic degeneration adjacent to soft yel-101~ tissue. Along one margi n of the mass there was distinct nodul arity, with a small, 1,5-cm, nodule raised slightly above the adjacent capsul e. Also submitted ~~ere additional encapsulated soft tissue masses measuring as much as 0,8 em. in maximum dimension,
My d iagnosis : --------------------------------------
Dr. Kay's diagnosis:
Comment :
CASE 12
~"'on l r i butAd by 01". H, J , Schattenberv. , Sr. Medical Arts Building , San Antonio , Texas
A 53-year-old female who had left upper quadrant abdominal pain was found to have a mass in the left retroperitoneal area. At surgery a mass was removed from the retroperitoneum, It 1~as located primarily to the left of the 4th lumbar vertebra . Grossly it measured 4 by 5 em. , was well encapsulated, and presented outer surfaces 1~ith many small nodules , The cut surface revealed solid tumor.
fly diagnosis: --------------------------------------
Dr. Kay's diagnosis : --------------------
Comment: --- - ---------------------
CASE 13
Contributed by Lt . Col. Robert w. Morrissey Wilford Hall USAF Hospital, Lackland Air Force Base
A 19-year-old white male had had a "conmon cold" for 1-1/2 wee ks when he developed pain in his r i ght eye . This pain 1~as follrn~ed by blurring of vision and finally diplopia, He was fo\md to have a right nasal tumor "<ith extension into the right ant rum , ethmoid sinus , and orbit.
My diagnosis : ---------------------------------------------
Dr. Kay's diagnosis :
Comment: -----------------------------------------------
CASE 14
Contributed by Dr, A. 0. Severance and Associates Bapt ist Memorial Hospital , San Antonio, Texas
Under local anesthesia a soft tissue mass from the left elb~ 1~as excised f ran a 77-year-old white female. This mass appeared grossly to be encapsulated and measured 2, 5 em, in greatest dimension. The cut surface had a gray mucoid appearance .
My diagnosis : -----------------------------------------------
Dr, Kay's diagnosis: --------------------------------------
Comment :
- - - -------·--------
CASE 15
Contributed by Dr. Charles T. Br ierty Santa Rosa Medical Center, San Antonio , Texas
A 75-year-old woman was admitted for a large tumor in the l01~er medial portion of the right leg. Several years before she had had a chondrosarcoma of a finger .
Hy diagnosis : ----------------------------------------
Dr. Kay ' ~ diagnosis: _______________________________ ___
Comment : ---------------------------------------------
CA'.>E 16
Contributed by Dr, A, 0, Severance and Associates Baptist Memorial Hospital, San Antonio. Texas
A 44-year-old male deve loped an intrascapular mass on the back slightly to the left. lt hau r.•·otm :; l01dy over a two-year period, This mass had appeared at the site of removal of a sebaceous cys t ten years earlier, A piece of skin t~ith underlying tissue t~as exci~cd . There was a lunpy mass 4, 3 by 3, 3 by 2 em, over which the skin appeared bosselated, The cut surface was dense and fibrous; separate fran the main mass was a s11'.all 6-mn. satellite nodule. Another 4-mn, satellite nodule was found a lso adjacent to the main mass. Tumor did not seem to invade the underlying muscle.
My di agnosis : ---------------------------------
Dr. Kay's diagnosis: -------------------------------
Comment: ----------------------~----------------
CASE 17
Contributed by Or, Horman H. Jacob Santa Rosa Medical Center, San Antonio, Texas
A 29-year-old man had a huge t umor of the left hip area l ocated be low the iliac crest and extending to the greater trochanter, The tumor was not painful. It weighed 1750 grams and measured 22 by 18 hy 8 em.
~1y di agnosis 1
Dr. Kay ' s diagnosis:
Comment : ----------------------------------
CASE 18
Cont ributed by Lt. Col. Robert w. Morrissey Wilford Hall USAf Hospital , Lackland Air Force Base
I n a 30-year-old whi t e mal e a 2- cm. left l ower lung mass was identified by routine x-ray. lie had a smoking hi story of 18 pack years. He had also noted a productive cough for 18 years. He had never 1~orked indoors or with a protect ive mask.
My diagnosis :
Dr. Kay ' s diagnosis :
Comment : --------------------------------------------------
DIAGNOSES:
1WEN1Y-'IHl RD ANNUAL TtJI.OR SEMINAR
SIIN ANTONIO SOCIETY OF PATHOLOGISTS
BROOKE GENERAL HOSPITAL BROOKE AJU.IY ~EDICAL CEN1ER
Fort Sam Houston , Texas OecembeT 3, 1966
C~E 1 ----------------------------------
C/ISt 2 ------------------~E 3 _________________________ _
C~E 4-----------------------------------C'.ASE 5
CASE 6
CASE 7
CASE 8
CASE 9
CASE 10
('.ASE 11
CASE 12
C~E 13
C/I.SE 14
CASE 15---------------------------------~ 16 ___________________________ __
C~E 17 --------------------------C~E 18-----------------------------------
Tlt.U. page. ma.y be. Jt.eta.bte.d 601t. yol.lll own Jt.e.6eJtence.,
DI AGNffiES:
TII'EN1Y-TIHRD ANNUAL TtJI.OR SEMINAR SAN ANTCl'liO SOCIE1Y OF PATI-IOUX>I STS
BROOKE GENERAJ. HffiPI TAL IIROO<E ARMY ~EDICAL CEiffl!R
ror t Sam lioust on, Texas December 3, 1966
C~E 1----------------------------------CASE 2
C~E 3-----------------------------------C~E 4---------------------------------C~E 5-----------------------------------C~E 6------------------------------------
CASE 7 ------------------------------------
C~E 8---------------------------------C~E 9---------------------------------C~E 10---------------------------------C~E 11-----------------------------------CASE 12------------------------------------OOE13 ----------------------------------OOE 14 -----------------------------------
C~E 15-----------------------------------C~E 16---------------------------------C~E 17-----------------------------------C~E 18 ------------------------------------
P te;u. e 6.i..U in yoWL c:Ua.gnoa u on .tit.U. 6oJtm, de,ta.ch, a.nd ma.U to .the Chief of Pathology Service , Brooke General llospi tal , Fort Sam llouston , Texas, ct.t yoWL eaJLU.ut convenience, :60 thct.t c:Uagno6U may be 6wnrmM.zed pJUOit. ;to the meeting oOJr. pJr.Uen;f.at.(.on ct.t the SeminM. Th.<.l> 6oJUn need not be 6.igneci ,
,
Case 1 (S-65 6164}
Diagnosis: Adenoma; of the Nipple
Description: The section s hm<s essentially a "mega.>urple" with multi p le proliferating ducts beneath 'the surface epithelium. Most <lucts are t ubular ·and lined by- simple cuboidal epi thelium. Others show the usual double l ayer wi th myoepithelial proliferation . A few are dilated t~J~d tortuous, with papillary infolding . The epith.elial changes are consistent with a benign proliferati.ng proces·s.
Discussion: 'It is difficult to attach a satisfactory- n.ame to this condition. It i s not an intraductal papilloma in the usual ~;lanse , since no simple dilatation of a major duct with intracystic papillary proliferation is seen. It appears that there llas been proliferatio.n and budding of all the ducts of the nipple with only occasional papillary formation. In Cutler's "Tumor of the Breas·t", no reference to this unique entity: is made. The closest resemblance to our case is a description by Ha.agensen in his text of an int're(luent form of intraductal papilloma that grows wi.thin the ducts of the nipple itself. A recent a:rticle, h owever, appeared i n Cancer Aug. 1965, under the title of "Adenomas of the Nipple". This paper reports 29 cases and furnishes clinical dat a, some of which ·will be pre·sented here. None of the cases showed .evidence o.i' malignancy, and local excision was a perfectly satisfactory method of handling the problem. Even more recently reported is a similar· case in a male p.atient.
rlP.ferences: Ha~gensen, C. D. Diseases of the Breast, pg. 253, w. B. Saunders Co., Phila ., Pa.
ShSpix:o, L . & Karpas , C. t·l. Fl orid papillo)llatosis of t he nippl e. First reported case in a male . Am.J. of Clin . Path. 411:155-159, 1965.
Taylor, H.B., & Robertson, A.G. 1002, 1965.
Adenomas of the ~iipnle . Cancer 18,995-.. -
.. Case 2 {S-62 5217) ·.
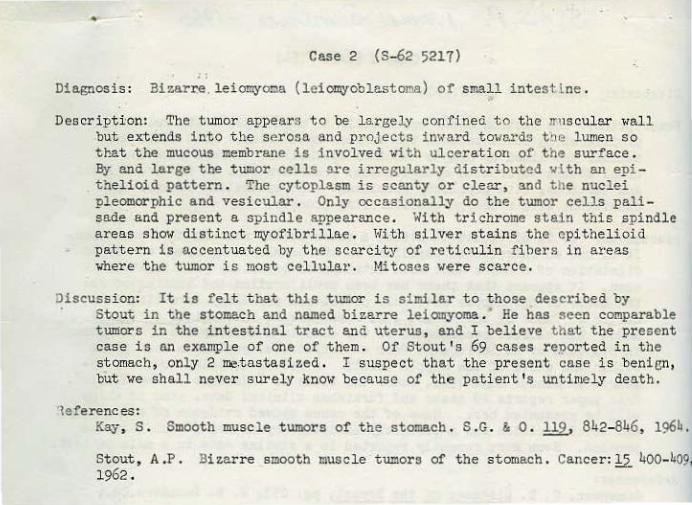
Diagnosis : Ei~arre.leiomyoma (leio~oblastoma) of smal l intestine .
Descr i pti:on: 'l'he t umor appears to be l arge1_v con fineci to thC! ll'\lSCuler wal l but ext ends into the se rosa and projects inward tmre.rds t he lumen so tr~t the mucous membrane is involved wi th ulcerati on of the surface. ay and large the tumor cells src irregularly distributed with an epi thelioid pattern. The cytoplasm is scanty or clear, and the nuclei pleomorphic and vesicular . Only occasionally do the tumor cells palisade and present a spindle appearance . With trichr ome stain this spindle a reas show distinct ~ofibrillae . \•lith silver stai ns the epithel ioid pattern is accentuated by the scarci ty of reticulin fibers in areas where t he tumor i s most cellular. Mitoses were scarce.
Discussion: It is felt that this tumor is similar to those described by Stout in the stomach and named biza..l'Te leiomyoma . He has seen comparable tumors in the intestinal tract and uterus, and I believe that the present case i s an example of one of them . Of Stout's 69 cases reported i n the stomach, only 2 me.tast a sized . I s uspect that the present case is benisn, but we shall neve r surely know because of the pat i ent's untin~ly death .
'leferences: Kay , S . Smooth muscle tumors of the stomach . S .G. & 0 . 119, 842-846, 196b.
Stout, A .P. !li~arre smooth muscle tumors of the s tomach . Cancer: J:2. 400-409, 1962 .
•
Case 3 (S-53 2491)
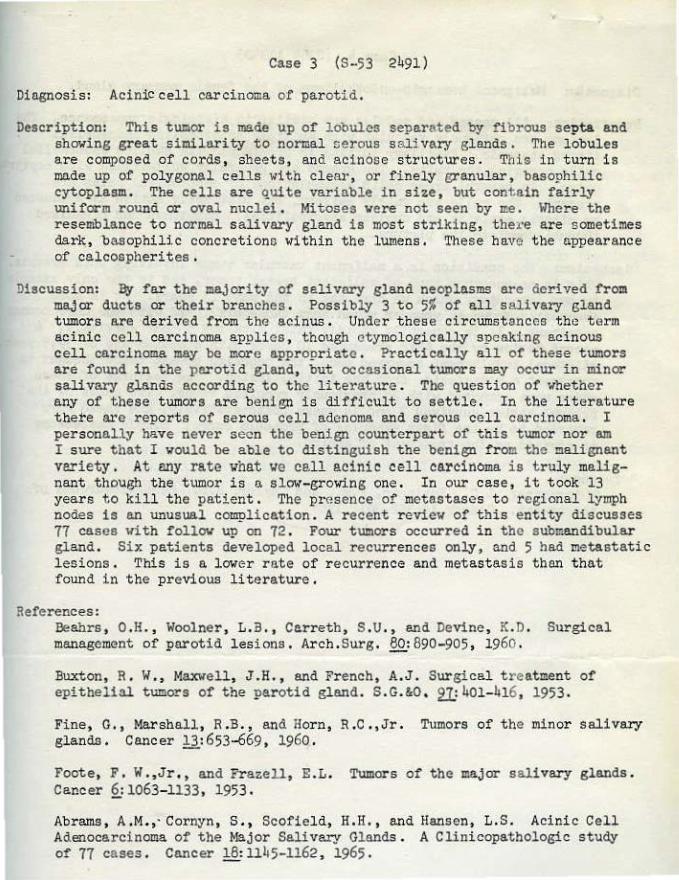
Die.enosis: Acinic cell carcinoma of par otid.
Description: This tumor is made up of lobules separated by fibrous septa and showing great s imilarity to normal cercus salivary glands. The lobules a re composed of cords, sheets, and acinose structures. This in turn is made up of po~ygonal cells with clear, or fine ly granular, basophilic cytoplasm. The cells are quite variable in size, but contain fairly uniform round or oval nuclei. Mitoses were not seen by me. Where the resemblance to normal s alivary gland is most striking, the1·e are sometimes dark, basophilic concretionG within the lumens. These have the appearance of calcoepher ites .
Discussion: By fa.r the majority of salivary gland neoplasms are dcriYed from major ducts or their br anches . Possibly 3 to 5% of all s alivary gland tumors are derived from the acinus. Under these circumstances th•~ t erm acinic cell carcinoma. applies , though etymologically speaking acinous cell carcinoma may be more appropriate . Practically all ot' these tumors are found in the perotid gland, but occasional tumors may occur in minor salivary glands according to the literature . The question of whether any of these tumors are benign is difficult to se ttle . In the liter ature t here are reports of serous cell adenoma and serous cell carcinoma. I personally have never seen the benign counterpart of this tumor nor am I sure that I would be able to distinguish the benign from the malignant variety . At MY rate vhat ve ce.ll acinic cell carcinoma is truly malignant though the tumor is a slow-growing one . In our case, it took 13 years to kill the patient. The presence of metastases to r egional lymph nodes is an unusual complication . A recent r eview of this entity discusses 77 cases with follow up on 72 . Four tumors occurred in the submandibular gland. Six patients developed local r ecurrences only, and 5 had metastatic lesions. This is a lower rate of r ecurrence and metastasis than that found in the pre'fious literature .
References: Beahrs , 0. H. , Woolner, L. il. , Cerreth, S . U. , and DeVine , K. D. Surgical management of parotid lesions. Arcb.Surg. 80:890-905 , 1960 .
Buxton, R. W., ~laxwell , J.H ., and French, A.J. Surgical t reatment of epithelial tumors of the parotid gland. S.G.&O , tl= 401- 1!16, 1953 .
Fine, G., ~~shall, R.B., and Horn, R.C .,Jr . Tumors of the minor salivary glands. Cancer 13 :653-669, 1960 .
Foote, F. W .,Jr,, and Frazell, E .L. Tumors of the major s a livary glands . Cane er §..: 1063-1133, 195 3 •
Abrams, A.M.,· Cornyn , S., Scofield, H.H., and Hansen, L.S. Acinic Cell Adenocarcinoma of the Major Salivary Gl ands . A Clinicopathologic stuey of 77 cases. Cancer 18: 1145-1162, 1965.
Case 4 (S-6b 11340)
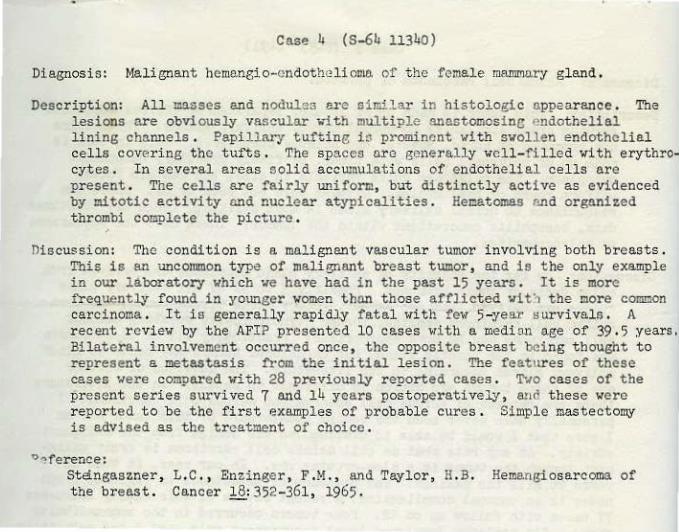
Diagnosis: Malignant hemangio-cndotheli on~ of the female mammary gland.
Description: All masses and nodula:> are similar in histol ogic appearance . The l esi ons are obviously vascular -~th multiple anestomosinc endothelial lining channels . Papi llary tufting ir. prominent wi t h swollen endothelial cells covering t he tufts . The spaces ar e generally well-fi l led wi t h erythr ocytes . In several areas solid accuJnulations of endothelial cel l s are pr esent . The cells are fairly uniform, but dist inct ly active as evidenced by znitotic activity and nuclear atypica.lities . Heoatomas and or ganized thrombi complete the picture .
Oiscussion: The condition i s a malignant vascul ar tumor i nvol ving both breasts . Thi s is an uncommon t ype of malignant br east tumor, and is the only example in our labor atory which we have bad in the past 15 years . It is more fr equently found in younger women than those afflict ed vit'1 the more connnon carcinoma . It is generalllf r apidly fatal vith fev 5-year aurvival a . A recent r eview by t he AFIP presented 10 cases with a median age of 39 .5 years. Bilateral involvement occurred once , the opposite breast being t hought to represent e. metastasis from the i nitial lesion . The features of these cases •.tere compared vi th 28 previously r eported cases. ~.10 cases of the present series survived 7 and 14 years postoperatively, Wld these were reported to be the first examples of probable cures . Simple mas t ectomy i s advised as the treatment of choice .
0~ference :
Stangaszner, tbe bree.s t .
L. C., Enz.inger , F.H., and Taylor, H.B. Cancer 18: 352- 361, 1965 .
Hemangiosarcoma of
Case 5 S-435-66
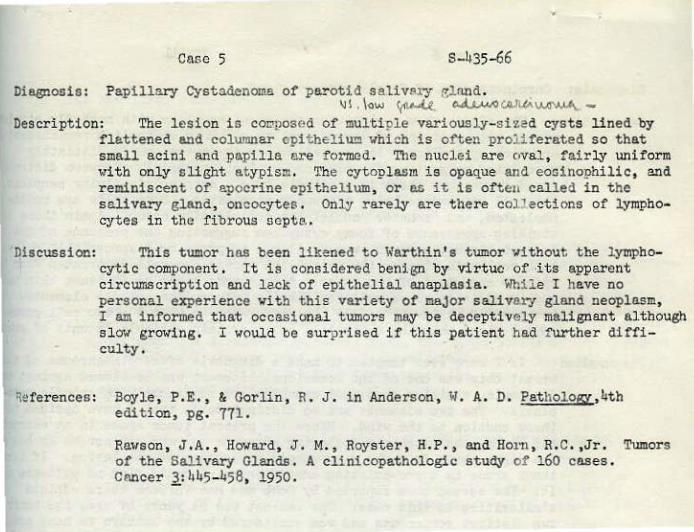
Diagnosis: Papillary Cyst adenoma of parotid sali very ela.nd. \JI . low ~...U. c..ll.,wo W\.(A~M~WA., -
Description: The l esion i s cOJ:'l?OSed of multiple variously- siZed cysts lined by flattened and columnar cpit heliuo which is often proliferated so that small acini and papilla are formed . The nuclei are oval, fairly uniform with only slight atypism. The cytopla.szn is opaque and eosinophilic, and reminiscent of apocrine epithelium, or as it is often called in the s alivary gland, oncocytes . Only rarely ar e there col l ections of lymphocytes in the f i brous septe ..
Discussion: This tumor bas been likened to Warthin's tumor without the lympho-cytic component . It is considered benign by virtue of ·its apparent circumscription and la.ck of epithelia! anaplasia. WMle I have no personal experience with this variety of major salivary gland neoplasm, I am i nformed that occasional tumors may be deceptively malignant although slow growing. I would be sur prised if this patfent had further diffi-~~. .
~eferences : Boyle, P.E., & Gorlin, R. J. in Anderson , W. A. D. PathologY,4th edit ion, pg. 771 .
Rawson, J .A., Howard, J, M., Royster, H.P., and Ho1n , R.C. ,Jr. Tumor s of the Salivar¥ Glands . A clinicopathologic study of 160 cases . Cancer 1_: 1145-1!58, 1950 .
•
Case 6
Diagnosis: Ca r cinosarcoma of :remale ma.mzr.aJ.-.f gland.
Descripti on: The slides s how a gl.anc1ular malignant neoplasm ~rith markedly atypical glands with a lining. of large, swollen columnar epithelium reminiscent of apocrine epithelium. In several places the cytoplasm is distinctly vacuolated suggesting the presence of lipid me.terial. Between distinct gland formations there is a spindle-type , extre~ly cellular neoplasm, the cell components being extremely anaplastic . Some cells are multinucleated, and "monster" nuclei are occasionally noted . Again there is a s t riking o.ppearance of foamy cytoplasm suggesting the presence of fat. No wet tissue, however, was available to prove 01' disprove this point. Wi th reticulin stains, the epithelial masses are well.-demarcated fro:n the spindle· component of the tumor . A trichrome :>tain again bears this out, and in addition shows collagen fibrils between the spindle elements. A mucicarmine stain emphasizes the difference between t he t wo cell components , since only the epithelia! cells contain variable amounts of mucin.
~iscussion : I f I were ever t empted to make a diagnosis of carc inosarcoma of the breast this was one of the occasi ons . Stewart has cnutioned against this diagnosis, claiming that most examples are carcinoma with spi ndle metaplasia. The two elements are so distinct here, that I have decided to throw caution to the wind. Since the present tumor P.rose in an extreme}1 old woman, the prognosis following adequate therapy may not be as bad as one mi5ht think from the microscopic appearance of the lesion . If this tumor arose in a ~re-existing adenofibroma , I could find no evidence ot it. The second case reported by Robb and Mac Farlane bears certain s imilarities to this case . The patient was 91 years of age , the tumor h two distinct components and ••as considered by the authors to have arisen in a fibroadenoma . Incidentally this patient was well 5 years after simple mastectomy .
~.:: ferences : Robb , P.~! ., & l•1acFarlane , A. Tl~o rare br east t umouro. J .Path . & Bact . l2,: 293-298, 1958.
-stewart, F. W.., Tumors of the Breast . Atlas of Tumor Pathology, AF!P Washington, D. C. , 1950 .
Case 7
·~~- c .• ;.L ·AJ•V' '""' l\A •• "
S-775-66
Diagnosis: Medullary carcinoma •'i tb ~loid stroma of the thyroi d .
Description: The tumor nodule is composed of solid accUl!IUlct~ons of small,
•
r ounded, dArkly-staining cella aeparatt?d end s ubdivi,1ed by an intens el y IflJI~eJ;JlJ.ning stroma. The s troma was po:; i t .ive for l!.l:oyl oid with the Congo
'flllile the cell accumulations o.re generall;r solid , there o.re distinct follicular arrangements without colloid in s o'!lie o.reas . Calcification is present in the s t roma i n one s mall :f'ocua.
riscussion: This is a malignant tU.lllor, less malignant than the anaplastic thyroid tumors, but more malignant than the papiJ.larJ varieties . Accordi ng to Hazcrd, metast ases to r egional lymph noder. occur in about 50% of
' cases. I have seen one case where two malignant nodules vc re present, one i n each thyroid lobe . Radical neck dissection i s distinctly wort.h while when dealing 1~itb these tumors. 'tlhile the t erm "medullary or s olid carcinoma" is a. relatively r ecent term, the tumor itseli' is not a recent discovery. I susp~ct t hat the old classi fication of '<arren and Meiss ner published in 1941 i~cluded this t~or under the n ame of small cell carcinoma (compact type) .
ll'!ferences : Freeman, D. , and Li nd:l91f , S . Medu.lla.ry Carcinoma of the Thyroid Gland, Arch.Path. 80: 575-582, 1965.
Hazar d, J . B. , HeM!~ , W. A. , and Cri 1e , G. ,Jr . Medullary (soli d carcinoma of the thyroid): A c linicopathologic entit y . J .Clln. Endocr. ~:152-161 , 1959.
1-lilliam:;, E.D., Bro·nn, C. L. and Doniach, I. Pathological and Clinical finciings in a series of 67 cases of medul l 3r'f carcinoma of th<:! thyroid. J . Clin. Pat h. ,19: J.03-ll3 , 1966.
williams , E .D. Histogenesis of medullary carcinoma of thyroid. J .Cli n. Path . , !2_: 114-116, 1966.
Case 8 S-7642-65
Diagnosis: Hamartomatous ~hadenitis of ce rvical lymph nodes.
Description: The striking appe6rllllce of t-his node or grou!' of nodes is the lacl; of the normal architecture, absence of the sinusoidal pattern, and the almost thymomatous appearonce as exemplified by the thin bands of fibrOU$ septa separating t he lymphoid strome into follicular masses . Germinal centers are small and indistinct, and in some areas Hassa.ll ' s corpuscles are mimicked . A linear arr angement of lymphocytes concentrically J surrounds t hese s mal l germinal centers . I could f i nd no anaplastic eel or Reed··Sternberg cells .
Uiscussion: Castleman first called attention to these benign l esions i n tbe me~a.stinum in the AFIP fascicle dealing with the thymus . Be Clllled the condition hyperplasia of mediastinal lymph nodes. A recent paper by Lattes and Pachter reported 12 cases with silllilar changes in different sites . Four cases involved the cervical region . The criteria for diagnosis were tebulated as follO\(S: 1. Follicular architecture throll8h· out . 2. lack of s inusoidal pattern . 3. unusuBl follicular and interfol licular vascularity. 4 . Hassall ' s corpuscle- like follicle centers . 5. absence of anaplastic cells .
~oferencea: Ce.stleman , B. Atlas of Tumor Pathology, Tumors of.!!~ Thymus Gland, AFIP, Washington, D. C. ,l955 .
Lattes, R. and Pachter, H. R. Benign lymplioi d masses of' probable hamartomatous nature . Ano.l,vs i s of l2 cases . Cance r !2_:197-214, 1962.
Case 9 7899 A-65
Diagnosis: Xanthogranulomatous pyeloneph:!'i tis.
D~scription: The kidney is largely destroyed by an inflammatory process of which the striking feature consists of muJ.tl.ple abscesses with a lining of multinucleated giant cells, lymphocytes , plasma cells , polymorphs, and histiocytic foam cell s . It is the presence of the l atter cells in large accumulations that has given ·the name of xanthogranuloma to this kidney lesion.
Discussion: The presence of large masses of to~ bistiocytes serves to dis-tinguish this l e Gion from tqe usual variety of pyelonephritis. Admittedly a number of inflammatory nephritides may contain small collections of lipid-containing phagocytes in addition to the usual inflammatory infiltrate. The real importance of recognizing thts lesion ia to distinguish it from clear cell carcinoma of the kidney. I have seen some cases of xanthogranulomatous pyelonephritis that were almost indistinguishable grossly from hypernephroid carcinoma. The presence of staghorn ce.lcull indeed ~v be helpful. Microscopically the differential diagnosis is e&aier. As to the etiology of t his disease infection, derangement in lipid metabolism, and urinary obstruction may all play a role. It would be interesting to have blood lipid data on this patient .
neferences : Mitchell, R. E., Jr . , Dodson, A. I., and Key , S. Xanthogranulome.tous pyelonephritis. Am . Pract. & Digest Treat . 10:2150-2155 , 1959.
Saeed, S.M. & Fine , G. Xanthogranulomatous pyelonephritis . Am J. of Clin . Path. ~:616-625 , 1963.
Case 10 7737-65
Di agnosis : Benign mesot helioma of the ova:ry . 'J ~ ~~~Ju.. ..
Description: In the mat erial. which I had to study, it appear ed to me t hat the tumor was on the surface of t he ovary, and no actual i.nvosion of the stroma was pre sent . The tumor is largely a papil~ary a.lveo~ar growth with many irregular end tortuous tubules presenting the most striking feature . The t ubules are c1·owded toget he r, but are often separat ed by a peculiar hyalin-like stroma. In one ar ea there• is dis tinct connection with t he surf ace mesothelium of t he ovary , and it llll\V not be t oo f anciful to imagine that the t UIIlor is growing f r om these cells . The epithelium lining t he tubules ar e not particular bizarre, but t he cells do vary i n size and shape end lie flat against the str oma. Hi toses were not s een by me . Huc i carmine stains were entirely negative .
~iscussion: The re semblance of this tumor t o mesonephr ic t ubules i s so s triking that one is reminded of Tei l um' s contention that t he so-call ed adenomatold tumors of the genital sphere is of mesonephric o.dgin . The present tumor does indeed show a superficial resemblance to the mesonephr ic carcinomas of the ovary, but al.l of t he l at t er which I have seen have a distinctly malignant appearance with bi zarre, "peg" cells , and invasive characterist i cs. The mesothelioma or adenamatoid tumor of the ovary is distinctly uncommon . I n a revie~ by t he Mayo Clini c in 1950 of geni tal tract mesotheliomas , 35 we r e studied , and only one wae found in t he ovar1 1-lhile I have seen about 6 cases of t hese t umor s involving the uterus , th! present case represents the only one I have encounter ed in the ovary . r believe t he les i on i s benign , s t rikingly s imilar to mesonephric ovarian t umors , and supports Teilum ' s wor k concerni ng the mesonephri c origin of e.ll of these tumors .
References: Kay , S . and Hoge , R.H. Mesonephric carcinomas of t he ovary . S . G.& 0. 107: 61!-94, 1958.
Lee, H.J., Dockerty , ~1.B . , Thompson, G .• J ., ~ Waugh 1 J .M. Beni gn mesotheliomas (a.d.eno®toid t umors ) of the geni t al. tract . S ,G.& 0 , 21,:221-231 1950 .
Teilum, G. Histogenesis and cl aseificatioq of mesonephric tumors or tp~ female and male genital system and relati on$hip to beni gn so-cnlled adenomatoid t umors (mesot bellanas), A oomparati ve histologica l study Acta Path .et r.jicro.Scand. ~~ ~31-481, 1954. · . ' •
Case 11 S-863-66
Diagnosis: Neurilemoma of retroperitoneum.
Descript ion: Thi s tumor ShO'wS l'emarkabl e :paJ.i na.ding or the nucL:i ,' s o character -istic of Antoni A tissue· in neurilemoma.s . 'l'he Antoni ll tissue is also well represented by the presence of the loos~-texturec.: and cystic areas of deseneration . Tbe vessels show hyalin sheaths .• another typical feature of these tumors .
Discussi on: Neurilemomas are uncommon in the retroperitoneum, end I personally have never seen a case i n this location . I pres~ that the tumor vas encapsulated . Very often it is associated with a major nerve , and may pr otrude from the spinal cll.llal in dumbbell fashi on . 'l'hc bona !'ide neurilemoma is always benign and malignant change does not occur-; in contradis tincti on to the neurofibroma. vhe1·e malignancy may occur in about 13% o f cases .
~~rerence: Acberman, L.V. Tumors of the retroperitoneum, mesentery and peritoneum. Atlas of Tumor Pathology , AFIP, 'das hington, D. C. 1954 .
Stout , A .P . Neurofibroma and Heurilel1!0J218 . Clinical Proceedings 2_: 1-12, 19116.
Case 12 277
Diagnosis: Leiom,yose.rcoma (vascular type) of r etroperitoneum.
Description: This tumor is made up of compact whorls of spindle cells reminiscent of smooth muscle cells . The nuclei are distinctly atypical, and I could find mitoses rather easily . The st:-iking feature is i he vascularity vbie is prominent in most fields , and one therefore bas to decide whether the tumor cells are in reality of smooth muscle origin(vescular lei~~osarc~ or whether they are indeed nodified smooth muscle elements or pericytes . A trichrome and PTA stain were not particul arly helpful , but intracellula f ibrils were seen though they stained poorly. Reticulin stains show cell i ndividually wrapped by silver-stained fibrils which in many areas were distinctly parallel.
!::.scussion: This is a fairly common neopl'!.Sm in the retro~ritoneum, and in our l aboratory has been the most f requent type of lllaligne.nt tumor . At Columbia University the liposarcoma headed the list , and since many more neopl asms of the retroperitoneum are seen there , this may be the true state of affairs.
:lererence: Golden, T., and Stout, A.P. Smooth muscle tumors of the gastroint estine: tract and retroperitoneal tissues . S.O . &0. 73:784-810 , 1941.
Case 13 HPS·-7180-65
Diagn~sis: Rhe.bdomyos'a!'coma ( e.lveolar type) of orbit and ethmoi <l. sinus. )
Description: ~JVtumor ,is largel y necrotic Hith the viable nreas ·showing a dense fibrovascular stroma support-ing tumor cells in l-arge clusters, nests, and alveolar groupings. The tumor celJ.s are. quite bizarre, \lith abundant mitoses, and darkly-staining nuclei with coro·s e chromr.tin. In general the cells are rounded with distinct rims of eosinophilic cytoplasm. Some cells shO'-' eccentric .nuclei w"i th abundant cytoplasm. · Rare nuclei show large, well-defined eosin-staining inclusion bocJ.i ·es, such a.s ntay often be seen in malignant melanoma cells . lnth reticulin stains the compartmentalization of t he tumor cel ls is well shmn1. A trichrome stain did not particularly color the cytoplasm, and was disappointingly non- revealing . I wish to emphasize, however, that no fibri l s are seen between. the tumor cells which seem merely to floaii in an empty space. The lack of fiorils was z:.lso noted with the Bodian, Ht,lmes and the PTA stain . 'rhe latter, however, did not reveal any cross -·striations to me. A striking feature, sometimes noted, is the presence of gland-like configurations by the tumor celJ.s. This may be artifactual but stil l quite definitive.
) 5 scussion: It seems to me that there. are. only two diagnostic possibilities for this case. This is either an olf!!.Ctory neuroepithelioma or an alveolar rhabdomyosarcoma. The patient bas a long history of r:aso.l obstruction, but ~e are not told hc;JW long is long. If "long" is a matter of years, then olfactory neuroepi theliome. is -a. more logical dia:gnosis . From the pure morphological point of vie~, I >Tish to call attention to a paper from the Mayo Clinic pub:).ished, in J.960, and I quote: 111-le have come ·to the conclusion· that, in the absence of fibrils, a nasal tumor cannot be classified as a neuroblastoma with certa.inty11• I do not know the fixative employed in this case, and p.erhaps ltzy' special stain result.s are not vaJ.id. The same previously-referred-to paper states that "Bodian silver impregnation failed to stain the fibrils". Another pertinllllt quotation states that " ..• mitotic figures are alillost never seen".
On morphological grounds therefore, there is little to support a diagnosis of olfactory neuroepithelioma unless it is a rare example of a highly malignant one with many mitoses and no cytoplasmic fibrils . On the other hand the alveolar rhabdomy·osarcoma has much to commend it . The anaplastic rounded forms with gland- like structures are quite typical, and the diagnosis would be certain if the trichrome and PTA stains colored the cytoplasm appropriately which unfortunately it did not.
,.~ferences: Enterline, H.T., and Horn, ll.C . ,Jr. Alveolar rhabdomyosarcoma. A distinctive tumor type . Azner .J. of Clin. Path. ~: 356-366, 1958.
Obert, G.J., Devine, K. D., and McDonald, J.R, Olfactory Neuroblastomas. Cancer 13:205-215, 1960.
Mendcloff, J . The olfactory neuroepithelial tumors. A review of the 1i terature and report of six .additional cases. Cancer .tO: 9114-956, 1957.
Case 14
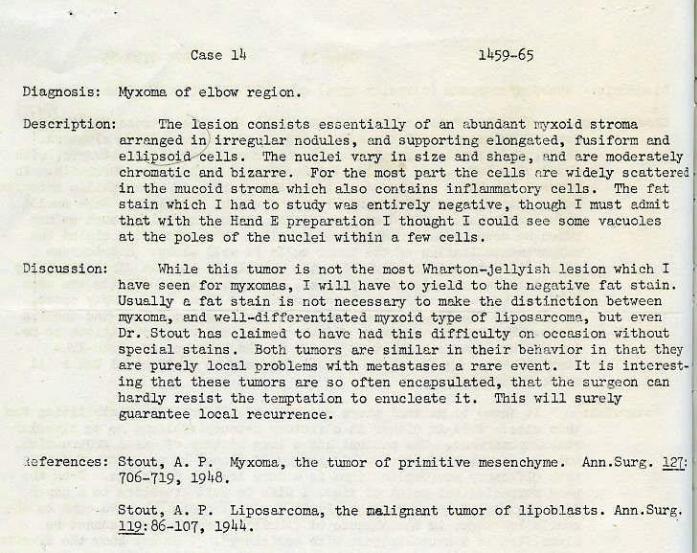
D:j.agnosis.: Myxoma of elbow region.
Description: The lefion consists e soeptially of an abundant Jli>'Xoid stroma arranged in; irregular nodules, and supporting elongated, fusiform and eUUl~--iells . The nuclei vary in size and shape, and are moderat ely chromatic and bizarre. ·For t he most part the cells Are widely scattered
·in the mucoid stroma which als·o contains inflammat ory cel ls. The fat stain which I had t o study was entirely negat ive , thou~p I must admit that with the Hand E preparation I thought I coul d see some vacuoles at the poles of the nuclei within a f ew cells .
Discussion: WM.le this tumor is not the most Wharton-jellyish lesion which. I have seen for myxomas, I will have to yie l d to the negative fat stain . Usual ly a fat stain is not necessary to make . the disti.nction between myxoma~ and well-differentiate d nwxoid type of liposa rcoma, but e':en Dr • . Stout has clai med to have had this difficulty on occasion without special stains. Both tUl'!lcrs are similar in their be!\avior i n that they are purely local p roblems with metastases ·a r ar e event. I t is interesting that these tumors are so often encapsulated, the.t the surgeon can hard!y resist the t emptation to enucleate it . This will surely guarantee local recurrence •
. le ferences: Stout, A. P. Myxoma, t he t umor of primitive mesenchyme. Ann.Surg . 127: 706-719 ' 19lf8.
Stout, A. P. Liposarcoma, the mali gnant tumor of lipoblasts . Ann.Surg_. 119:86-107, 1944 .
Case 15 1067-66
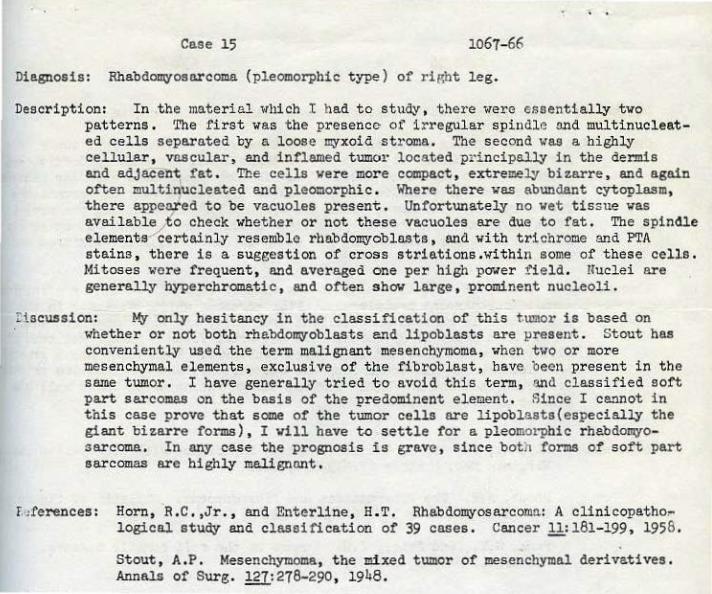
Diagnosis: Rhabdomyosarcoma (pleomorphic type) of riRht leg.
Description: In .the materia l which I had to study , there were essentially two patterns. 'l'he first. was the presence of i rregular spindl~ and multinucl eated cells separated by a loose myxoid st1·oma. The second was a highly celluJ.ar, va.scular, and inflamed tumo1· l ocated principally in the der:mis and adJacent fat . The cells were more compact , extremely bizarre, and again often multinucleated and pleomorphic . llhere there vas abundant cytopla.sm, there appealed to be vacuoles present. Unfortunately no wet tissue was availabl~to check whether or not these vacuoles are due to fat. The spindle elements certainly resemble rhabdomyoblasts , and with t richrome and PTA stains , there is a suggestion of cross striations.within some of these cells. lolitoses wore frequent , and averaged one per high p<To~er field . nuclei ar e generally hypercbrO!llatic, and often sh011 large , prominent nucleoli .
t iscW!sion: My only hesitancy in the classification of t his tumo1· is based on whether or not both rhabdomyoblasts end lipoblasts are present . Stout has conveniently used the term malignant mesench,ymoma, when two or more mesenchymal elements, exclusive of tne fibroblast ,. have been present in the same tumor . I have generally tried to avoid this term, and classified soft part sarcomas on the basis of the predominant element. Since I cannot in this case prove that some of the t~or cells are lipobl asts(especially the giant bizarre forms) , I vill have to settle for a pleomorphic rhebdomyosarcoma, In any case the prognosis is grave , since both forms of soft part sarcomas are highly malignant,
r."ferences : Horn, R . C. ,Jr. , and Enterline, H . T. Rhabdomyosarcomn: A clinicopatho,.. logical study and classification of 39 cases . Cancer 11:181-199, 1958 .
Stout , A.P. Mesencbymoma, the mixed tumor of mesenchymal derivatives. Annals of Surg. 127:278-290, 1948.
Case 16
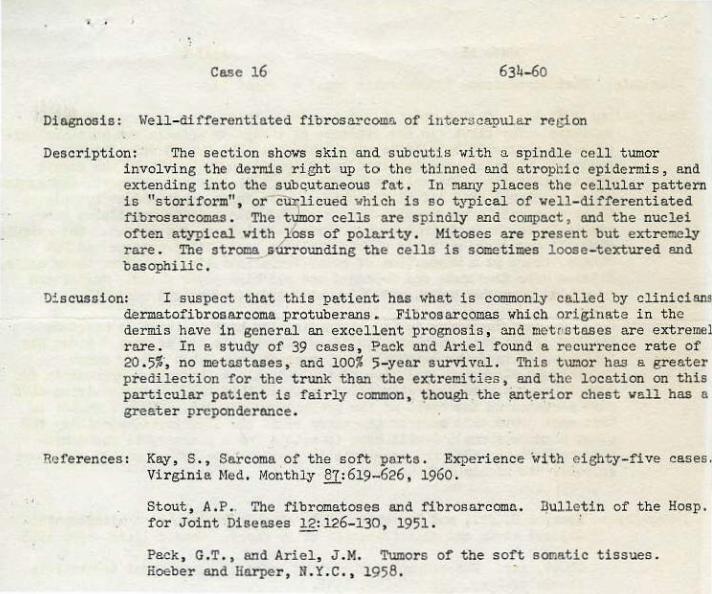
Dingnosis: \-/ell-differentiated fibrosarcoma of interscapular r et;ion
Description: The section shows skin and subcutJ.s with a spindle cell tumor involving the dermis right up to the thinned and atrophic epidermis, and extending into the sube,utaneous fat. In many places the cellular pattern is "storiform", or~licued which is so typical of well-differentiated fibrosarcomas. The tumor cells are spindly and compact, and the nuclei often atypical wi tb lbss of pola.ri ty . Mitoses are present but extremely rare. The stroma surrounding the cells is sometimes loose-textured and basophilic.
Discussion: I suspect that this patient has what is commonly called by clinicians dermatofibrosarcoma protuberans. Fibrosarcomas which originate in the dermis have in general an excellent prognosis, 31ld metr•.etases are extremel rare. In e study of 39 cases, Pack o.nd Ariel found a recurrence rate of 20.5%', no metastnses, and 100% 5-yenr survivaL This t\U:lor has a greater predilection for the trunc~ than the extremities, and the location on this particular patient is fairly common, ~bough the p.nterior chest vall has a greater preponderance .
References : Kay, S., Sarcoma of the soft parts . Experience with eighty-five cases. Virginia ~led. Monthly N,: 619-626, 1960.
Stout, A .P.. The fibromatoses and fibrosarcoma. J:1ulle.tin of the Hosp. for Joint Diseases 12: 126-130, 1951.
Pack, G.T., and Ariel, J.M. Tumors of the soft somatic tissues. lioeber and Harper, li. i'. C., 1958.
. . Case 17 3949- 65
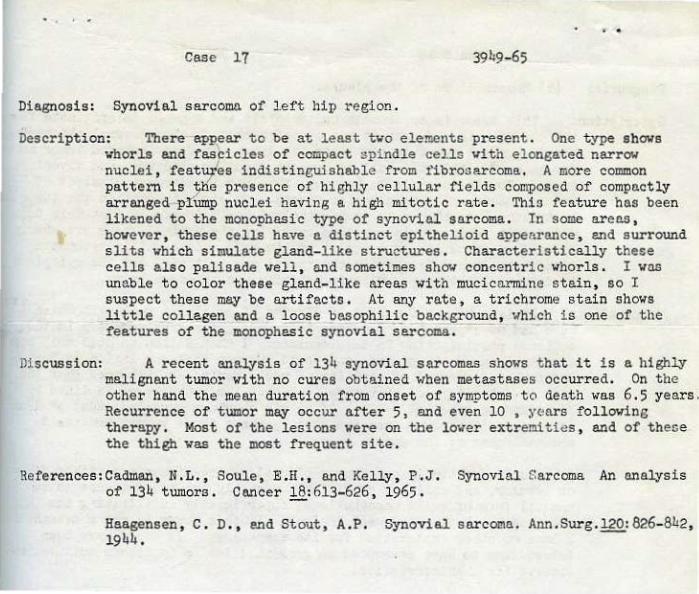
Diagnosis: Synovial sarcomo. of l ef t hip region.
Description: There appear to be at l east tvo elements present . One type shows vhorls and fascicles of compact spi ndle cel.ls vi th el ongated narrow nuclei, featutes indistinguishable from fibrosarcoma. A more common pattern is 'tjn'e presence of highly cellular fie lds composed of compactly arranged -ph unp nuclei having a. high mitotic rate. Thio feature has been l ikened to the monophasi c type of synovial sarcoma. In some areas , bovever , these cells have n distinct epithelioid appearance , end surround slits vhich simulate gland-like structures. Characteristically t hese cells also palisade well , and sometimes shov concentric whorls. I vas unable to color these gland-like areas with mucicarmine stein, so I suspect these mey be artifacts. At any rate, a trichrome stain shows little collagen and a loose basophilic background, ••hich i s one of the features of the monophasic synoVial sarcoma.
Discussion: A recent analysis of 134 synoVial sarcomas shows t hat it is a highly malignant tumor with no cures obt ained when metastases occurred. On the other hand the mean duration from onset of symptoms -to death was 6 .5 years . Recurrence of tumor m~ occur after 5, and even 10 , years following therapy. Most of the lesions were on the lover extremiti es , and of these tbe thigh was the most frequent site .
References:Cadman, N.L., Soule, E.H. , and Kelly, P.J. Synovial Sarcoma An analysis of 134 tumors. Cancer 18: 613-626 , 1965.
Haagensen, C. D., end Stout, A.P. Synovial sarcoma. Ann.Surg. l20:826- 842, 1944.
. . Case # 18
Diagnosis: (?)
,, w.V'M~,(\M,"-. ,,
Mesothelioma of c).-4.1 ""'--c'-' ~ ~
t he pleura.
5661-65
.. . . .
Description: Thi s tumor is apparently multicentri c and appears to originate from the pleura. I n one area it has causea me.rked fit•rous pleural thickening, but in general seems to push into the lung . In fact isolated tumor nests m~ be seen within the wall of bronchi, smaller arteries, ~~d alveolar septa. For the moot part, however, the lung involvement consists of nodular masses filling alveolar spaces. On close inspection the tumor h81 a striking resemblance to meningothelial meningioma. In fact this tumor would suit admirably in eey area overlying the brain. There are whorls of uniform round end oval nuclei vithin pale , eosinophilic cytoplasm vi thout borders. ~'requently the 'n\lclei are palisaded and t he cytoplasm is faintly fibrillary. Mitotic activity \fas not seen by me.
Discussion: I t is always rerieshins to discuss at least one case. lri. t h vhich I have bed no experience, end hope to be enlightened by somebody in the audience participating in this seminar . I should like to call tbis case a meningioma o~-t~e pleura , end would suspect that the lesion is benign. Before being accu~ed of senil~ty , I vould remind my listener~ that the dura is a tvo-leypred structure , and that the inner layer is l ined by flattened mesothelial cells. If ve can convince ourselves that at least some meningiomas come frofll the dura, perhaps these tumors ere really mesothel iomas of the dura.
While admittedly our common pleural mesotheliomas are either fibrow or tubul ar, end soli t~ or diffuse, possibly the present case is an unusual form of solid mesotheli oma, superficially i nfiltrating the lung, end resembling the meningeal lesions. If this tumor is not a mesothelia I have no other explanation for its morphology. It would have been interesting to have attempted to grow this lesion in tissue culture, and observe its characteristics .