Embed Size (px)
Citation preview
Journal of Antimicrobial Chemotherapy (2005) 56, 407–409
doi:10.1093/jac/dki206
Advance Access publication 21 June 2005
Antimicrobial susceptibility testing of Actinomyces specieswith 12 antimicrobial agents
A. J. Smith1*, V. Hall2, B. Thakker3 and C. G. Gemmell4
1Infection Research Group, Glasgow Dental Hospital, Glasgow, Scotland, UK; 2Anaerobe Reference Laboratory,
NPHS Microbiology Cardiff, University Hospital of Wales, Cardiff, Wales, UK; 3Bacteriology Department,
Glasgow Royal Infirmary, Scotland, UK; 4Division of Immunology, Infection and Inflammation,
Medical School, University of Glasgow, Scotland, UK
Received 6 April 2005; returned 25 April 2005; revised 24 May 2005; accepted 24 May 2005
Objective: This study was conducted to assess the susceptibility of human clinical isolates of Actino-myces species to 12 antimicrobial agents.
Methods: Human clinical isolates of Actinomyces spp. were collected from stored collections held at theMicrobiologyDepartment, EdinburghUniversity, AnaerobeReferenceLaboratory, Cardiff, GlasgowDentalHospital and Glasgow Royal Infirmary. Each isolate was identified by restriction analysis of amplified 16Sribosomal DNA. MICs of 12 antibiotics comprising benzyl penicillin, amoxicillin, ceftriaxone, linezolid,tetracycline, deoxycycline, clindamycin, erythromycin, clarithromycin, ciprofloxacin, meropenem andpiperacillin/tazobactam for 87 strains of Actinomyces species were obtained by Etest methodology.
Results: TheActinomyces species identified for this study comprised:Actinomyces israelii, Actinomycesgerencseriae, Actinomyces turicensis, Actinomyces funkei, Actinomyces graevenitzii and Actinomyceseuropaeus. All isolateswere susceptible to penicillin and amoxicillin. All but one strain ofA. turicensiswassusceptible to linezolid. Anumber ofA. europaeus andA.graevenitzii isolateswere resistant to ceftriaxoneand piperacillin/tazobactam. A number of isolates of A. turicensis and A. europaeus also demonstratedresistance to erythromycin. All Actinomyces species tested appeared resistant to ciprofloxacin.
Conclusions:Actinomyces species appear to be susceptible to awide range of b-lactam agents and these,when combined with b-lactamase inhibitors, should be regarded as agents of first choice. Ciprofloxacinperformed poorly. Tetracyclines also demonstrated poor performance. This is the first study of antimicro-bial susceptibilities for a number of accurately identified clinical isolates of Actinomyces spp. There area number of species differences in susceptibility profiles to the antimicrobials tested, suggesting thataccurate identification and speciation may have an impact on clinical outcome.
Keywords: Actinomyces israelii, Actinomyces gerencseriae, Actinomyces turicensis, Actinomyces funkei,Actinomyces graevenitzii, Actinomyces europaeus, antimicrobial susceptibility
Introduction
Actinomycosis is a chronic disease characterized by abscessformation, tissue fibrosis and draining sinuses. It is causedby non-spore-forming species of the genus Actinomyces. TheActinomyces species are Gram positive and commonly filamentousorganisms that are facultative anaerobes. The Actinomyces speciesare commensals and normal inhabitants of the oropharynx,gastrointestinal tract and female genital tract. Four clinical formsof actinomycosis, i.e. cervicofacial, thoracic, abdominopelvic andcerebral account for the majority of infections in humans. The face
and neck are the most common sites of actinomycosis.1–5 Othersites of infection are less common but share similar features, in thatan accurate diagnosis is essential for adequate therapy, which maynecessitate at least 6 weeks of antimicrobial chemotherapy.A combined medical–surgical approach is frequently requiredfor extensive disease.1,2
The clinical significance of the many recently describedActinomyces spp. has yet to be proven but some, includingActinomyces turicensis and Actinomyces europaeus are clearlyassociated with mixed infections in superficial soft-tissueabscesses.6
.............................................................................................................................................................................................................................................................................................................................................................................................................................
*Corresponding author. Tel: +44-141-211-9747; Fax: +44-141-211-9600; E-mail: [email protected].............................................................................................................................................................................................................................................................................................................................................................................................................................
407� The Author 2005. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved.
For Permissions, please e-mail: [email protected]
at Milton S. E
isenhower L
ibrary/ Johns Hopkins U
niversity on April 13, 2014
http://jac.oxfordjournals.org/D
ownloaded from
Those Actinomyces spp. that have been tested are susceptibleto a wide range of antimicrobial agents.7 However, interpretationof different studies is hampered by difficulties in the accurateidentification of members of the Actinomyces genus and taxonomicchanges. Susceptibility data on accurately identified Actinomyceswill become increasingly important as our knowledge of theinfections caused by the Actinomyces genus improves.
The aim of this study was to analyse the antimicrobial suscept-ibility of a wide range of Actinomyces spp. isolated from clinicalinfections and identified by restriction analysis of amplified 16Sribosomal DNA.
Materials and methods
Clinical strains
Clinical isolates were collected from stored collections held at theMicrobiologyDepartment, EdinburghUniversity, AnaerobeReferenceLaboratory, Cardiff, Glasgow Dental Hospital and Glasgow RoyalInfirmary.
Identification of isolates
There were 87 isolates available for analysis and each isolate wasidentified by restriction analysis of amplified 16S ribosomal DNA(ARDRA) as described previously.8
Susceptibility testing
The MICs for 12 antibiotics consisting of benzyl penicillin G, amox-icillin, ceftriaxone, linezolid, tetracycline, deoxycycline, clindamycin,erythromycin, clarithromycin, ciprofloxacin, meropenem and pipera-cillin/tazobactam were obtained by Etest methodology. All tests wereperformed on freshly poured Wilkens–Chalgren agar plates and wereincubated anaerobically for 48–72 h. The plates were inoculated with abacterial suspension in saline of turbidity equivalent to that ofMcFarland standard 4.9 Quality assurance was performed using Bac-teroides fragilis (ATCC25285) andEubacterium lentumATCC43055.
Results
Actinomyces species identified
Use of the ARDRA technique resulted in the identificationof 25 Actinomyces israelii, 23 Actinomyces gerencseriae,11 A. turicensis, 10 Actinomyces funkei, eight Actinomycesgraevenitzii and 10 A. europaeus.
Antimicrobial susceptibility
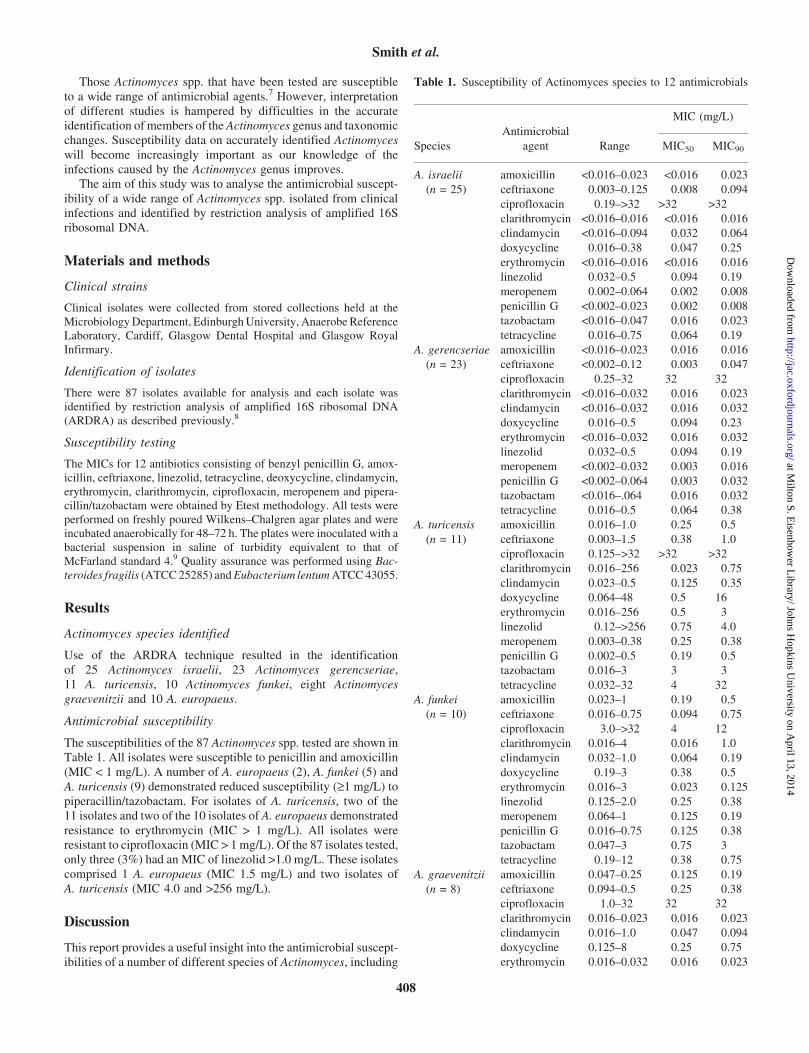
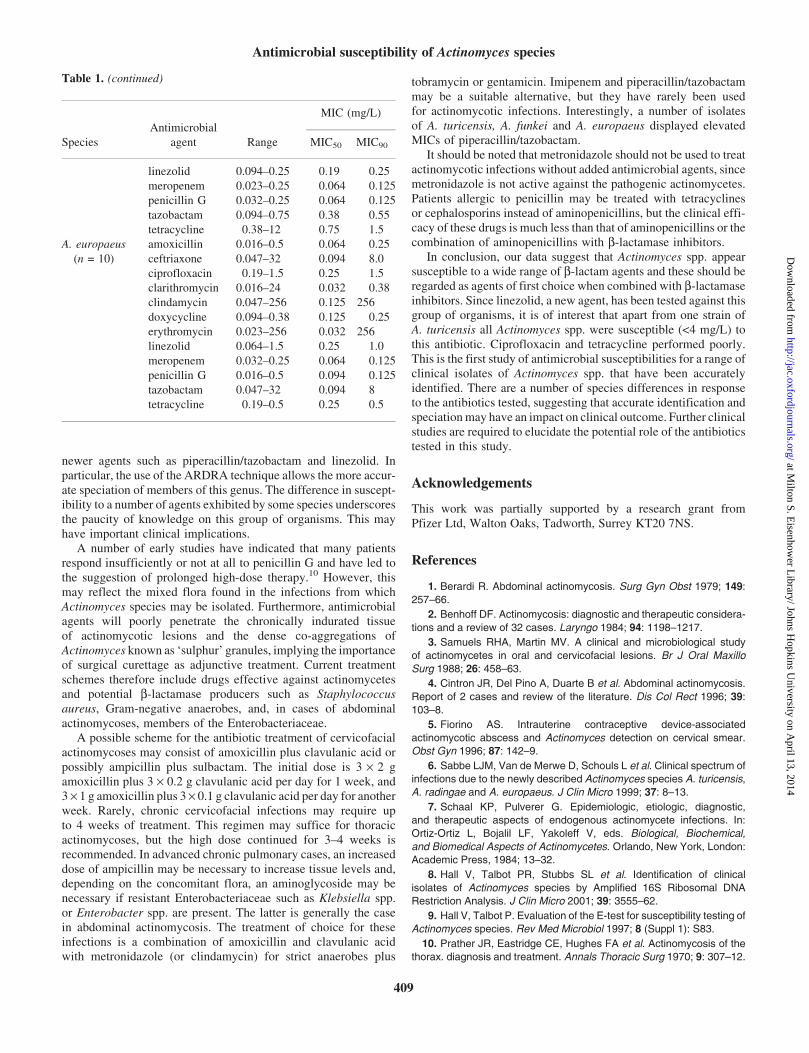
The susceptibilities of the 87 Actinomyces spp. tested are shown inTable 1. All isolates were susceptible to penicillin and amoxicillin(MIC < 1 mg/L). A number of A. europaeus (2), A. funkei (5) andA. turicensis (9) demonstrated reduced susceptibility (‡1 mg/L) topiperacillin/tazobactam. For isolates of A. turicensis, two of the11 isolates and two of the 10 isolates of A. europaeus demonstratedresistance to erythromycin (MIC > 1 mg/L). All isolates wereresistant to ciprofloxacin (MIC > 1mg/L). Of the 87 isolates tested,only three (3%) had an MIC of linezolid >1.0 mg/L. These isolatescomprised 1 A. europaeus (MIC 1.5 mg/L) and two isolates ofA. turicensis (MIC 4.0 and >256 mg/L).
Discussion
This report provides a useful insight into the antimicrobial suscept-ibilities of a number of different species of Actinomyces, including
Table 1. Susceptibility of Actinomyces species to 12 antimicrobials
Antimicrobial
MIC (mg/L)
Species agent Range MIC50 MIC90
A. israelii
(n = 25)
amoxicillin <0.016–0.023 <0.016 0.023
ceftriaxone 0.003–0.125 0.008 0.094
ciprofloxacin 0.19–>32 >32 >32
clarithromycin <0.016–0.016 <0.016 0.016
clindamycin <0.016–0.094 0.032 0.064
doxycycline 0.016–0.38 0.047 0.25
erythromycin <0.016–0.016 <0.016 0.016
linezolid 0.032–0.5 0.094 0.19
meropenem 0.002–0.064 0.002 0.008
penicillin G <0.002–0.023 0.002 0.008
tazobactam <0.016–0.047 0.016 0.023
tetracycline 0.016–0.75 0.064 0.19
A. gerencseriae
(n = 23)
amoxicillin <0.016–0.023 0.016 0.016
ceftriaxone <0.002–0.12 0.003 0.047
ciprofloxacin 0.25–32 32 32
clarithromycin <0.016–0.032 0.016 0.023
clindamycin <0.016–0.032 0.016 0.032
doxycycline 0.016–0.5 0.094 0.23
erythromycin <0.016–0.032 0.016 0.032
linezolid 0.032–0.5 0.094 0.19
meropenem <0.002–0.032 0.003 0.016
penicillin G <0.002–0.064 0.003 0.032
tazobactam <0.016–.064 0.016 0.032
tetracycline 0.016–0.5 0.064 0.38
A. turicensis
(n = 11)
amoxicillin 0.016–1.0 0.25 0.5
ceftriaxone 0.003–1.5 0.38 1.0
ciprofloxacin 0.125–>32 >32 >32
clarithromycin 0.016–256 0.023 0.75
clindamycin 0.023–0.5 0.125 0.35
doxycycline 0.064–48 0.5 16
erythromycin 0.016–256 0.5 3
linezolid 0.12–>256 0.75 4.0
meropenem 0.003–0.38 0.25 0.38
penicillin G 0.002–0.5 0.19 0.5
tazobactam 0.016–3 3 3
tetracycline 0.032–32 4 32
A. funkei
(n = 10)
amoxicillin 0.023–1 0.19 0.5
ceftriaxone 0.016–0.75 0.094 0.75
ciprofloxacin 3.0–>32 4 12
clarithromycin 0.016–4 0.016 1.0
clindamycin 0.032–1.0 0.064 0.19
doxycycline 0.19–3 0.38 0.5
erythromycin 0.016–3 0.023 0.125
linezolid 0.125–2.0 0.25 0.38
meropenem 0.064–1 0.125 0.19
penicillin G 0.016–0.75 0.125 0.38
tazobactam 0.047–3 0.75 3
tetracycline 0.19–12 0.38 0.75
A. graevenitzii
(n = 8)
amoxicillin 0.047–0.25 0.125 0.19
ceftriaxone 0.094–0.5 0.25 0.38
ciprofloxacin 1.0–32 32 32
clarithromycin 0.016–0.023 0.016 0.023
clindamycin 0.016–1.0 0.047 0.094
doxycycline 0.125–8 0.25 0.75
erythromycin 0.016–0.032 0.016 0.023
Smith et al.
408
at Milton S. E
isenhower L
ibrary/ Johns Hopkins U
niversity on April 13, 2014
http://jac.oxfordjournals.org/D
ownloaded from
newer agents such as piperacillin/tazobactam and linezolid. Inparticular, the use of the ARDRA technique allows the more accur-ate speciation of members of this genus. The difference in suscept-ibility to a number of agents exhibited by some species underscoresthe paucity of knowledge on this group of organisms. This mayhave important clinical implications.
A number of early studies have indicated that many patientsrespond insufficiently or not at all to penicillin G and have led tothe suggestion of prolonged high-dose therapy.10 However, thismay reflect the mixed flora found in the infections from whichActinomyces species may be isolated. Furthermore, antimicrobialagents will poorly penetrate the chronically indurated tissueof actinomycotic lesions and the dense co-aggregations ofActinomyces known as ‘sulphur’ granules, implying the importanceof surgical curettage as adjunctive treatment. Current treatmentschemes therefore include drugs effective against actinomycetesand potential b-lactamase producers such as Staphylococcusaureus, Gram-negative anaerobes, and, in cases of abdominalactinomycoses, members of the Enterobacteriaceae.
A possible scheme for the antibiotic treatment of cervicofacialactinomycoses may consist of amoxicillin plus clavulanic acid orpossibly ampicillin plus sulbactam. The initial dose is 3 · 2 gamoxicillin plus 3 · 0.2 g clavulanic acid per day for 1 week, and3 · 1 g amoxicillin plus 3 · 0.1 g clavulanic acid per day for anotherweek. Rarely, chronic cervicofacial infections may require upto 4 weeks of treatment. This regimen may suffice for thoracicactinomycoses, but the high dose continued for 3–4 weeks isrecommended. In advanced chronic pulmonary cases, an increaseddose of ampicillin may be necessary to increase tissue levels and,depending on the concomitant flora, an aminoglycoside may benecessary if resistant Enterobacteriaceae such as Klebsiella spp.or Enterobacter spp. are present. The latter is generally the casein abdominal actinomycosis. The treatment of choice for theseinfections is a combination of amoxicillin and clavulanic acidwith metronidazole (or clindamycin) for strict anaerobes plus
tobramycin or gentamicin. Imipenem and piperacillin/tazobactammay be a suitable alternative, but they have rarely been usedfor actinomycotic infections. Interestingly, a number of isolatesof A. turicensis, A. funkei and A. europaeus displayed elevatedMICs of piperacillin/tazobactam.
It should be noted that metronidazole should not be used to treatactinomycotic infections without added antimicrobial agents, sincemetronidazole is not active against the pathogenic actinomycetes.Patients allergic to penicillin may be treated with tetracyclinesor cephalosporins instead of aminopenicillins, but the clinical effi-cacy of these drugs is much less than that of aminopenicillins or thecombination of aminopenicillins with b-lactamase inhibitors.
In conclusion, our data suggest that Actinomyces spp. appearsusceptible to a wide range of b-lactam agents and these should beregarded as agents of first choice when combined with b-lactamaseinhibitors. Since linezolid, a new agent, has been tested against thisgroup of organisms, it is of interest that apart from one strain ofA. turicensis all Actinomyces spp. were susceptible (<4 mg/L) tothis antibiotic. Ciprofloxacin and tetracycline performed poorly.This is the first study of antimicrobial susceptibilities for a range ofclinical isolates of Actinomyces spp. that have been accuratelyidentified. There are a number of species differences in responseto the antibiotics tested, suggesting that accurate identification andspeciationmay have an impact on clinical outcome. Further clinicalstudies are required to elucidate the potential role of the antibioticstested in this study.
Acknowledgements
This work was partially supported by a research grant fromPfizer Ltd, Walton Oaks, Tadworth, Surrey KT20 7NS.
References
1. Berardi R. Abdominal actinomycosis. Surg Gyn Obst 1979; 149:257–66.
2. Benhoff DF. Actinomycosis: diagnostic and therapeutic considera-
tions and a review of 32 cases. Laryngo 1984; 94: 1198–1217.
3. Samuels RHA, Martin MV. A clinical and microbiological study
of actinomycetes in oral and cervicofacial lesions. Br J Oral Maxillo
Surg 1988; 26: 458–63.
4. Cintron JR, Del Pino A, Duarte B et al. Abdominal actinomycosis.
Report of 2 cases and review of the literature. Dis Col Rect 1996; 39:103–8.
5. Fiorino AS. Intrauterine contraceptive device-associated
actinomycotic abscess and Actinomyces detection on cervical smear.
Obst Gyn 1996; 87: 142–9.
6. Sabbe LJM, Van de Merwe D, Schouls L et al. Clinical spectrum of
infections due to the newly described Actinomyces species A. turicensis,
A. radingae and A. europaeus. J Clin Micro 1999; 37: 8–13.
7. Schaal KP, Pulverer G. Epidemiologic, etiologic, diagnostic,
and therapeutic aspects of endogenous actinomycete infections. In:
Ortiz-Ortiz L, Bojalil LF, Yakoleff V, eds. Biological, Biochemical,
and Biomedical Aspects of Actinomycetes. Orlando, New York, London:
Academic Press, 1984; 13–32.
8. Hall V, Talbot PR, Stubbs SL et al. Identification of clinical
isolates of Actinomyces species by Amplified 16S Ribosomal DNA
Restriction Analysis. J Clin Micro 2001; 39: 3555–62.
9. Hall V, Talbot P. Evaluation of the E-test for susceptibility testing of
Actinomyces species. Rev Med Microbiol 1997; 8 (Suppl 1): S83.
10. Prather JR, Eastridge CE, Hughes FA et al. Actinomycosis of the
thorax. diagnosis and treatment. Annals Thoracic Surg 1970; 9: 307–12.
Table 1. (continued)
Antimicrobial
MIC (mg/L)
Species agent Range MIC50 MIC90
linezolid 0.094–0.25 0.19 0.25
meropenem 0.023–0.25 0.064 0.125
penicillin G 0.032–0.25 0.064 0.125
tazobactam 0.094–0.75 0.38 0.55
tetracycline 0.38–12 0.75 1.5
A. europaeus
(n = 10)
amoxicillin 0.016–0.5 0.064 0.25
ceftriaxone 0.047–32 0.094 8.0
ciprofloxacin 0.19–1.5 0.25 1.5
clarithromycin 0.016–24 0.032 0.38
clindamycin 0.047–256 0.125 256
doxycycline 0.094–0.38 0.125 0.25
erythromycin 0.023–256 0.032 256
linezolid 0.064–1.5 0.25 1.0
meropenem 0.032–0.25 0.064 0.125
penicillin G 0.016–0.5 0.094 0.125
tazobactam 0.047–32 0.094 8
tetracycline 0.19–0.5 0.25 0.5
Antimicrobial susceptibility of Actinomyces species
409
at Milton S. E
isenhower L
ibrary/ Johns Hopkins U
niversity on April 13, 2014
http://jac.oxfordjournals.org/D
ownloaded from