Embed Size (px)
Citation preview

Antihypertensive Therapy in Hypertrophic Cardiomyopathy
Edgar Argulian, MD, MPH, Franz H. Messerli, MD, Emad F. Aziz, DO, MB, CHB, Glenda Winson, RN,Vikram Agarwal, MD, MPH, Firas Kaddaha, MD, MPH, Bette Kim, MD, and Mark V. Sherrid, MD*
Patients with coexisting hypertrophic cardiomyopathy (HC) and hypertension present diag-
HypertrophicLuke’s-RooseveltPhysicians and SSeptember 10, 2015, 2012.
See page 1044*CorrespondinE-mail addres
0002-9149/13/$ -http://dx.doi.org/1
nostic and therapeutic dilemmas. A retrospective cohort study of patients with HC with coex-isting hypertension referred to a specializedHCprogramwas conducted. HC and hypertensionwere confirmedby strict criteria. Echocardiographic datawere reviewed for peak instantaneousleft ventricular outflow tract gradients, at rest and with provocation. Symptom control, leftventricular outflow tract gradients, and hypertension control were compared between the firstand last visits. One hundred fifteen patients (94 obstructed and 21 nonobstructed) met theeligibility criteria for the study and were included in the analysis, with the mean follow-upduration of 36months. Because of the treatment strategy, there was a significant decrease in thenumber of patients treated with direct vasodilators and an increase in the use ofb blockers anddisopyramide. Twenty-one obstructed patients (22%) required septal reduction therapy.Overall, in obstructed patients, peak instantaneous left ventricular outflow tract gradient at restdecreased from 48 to 14mmHg (p<0.01), which was accompanied by significant improvementin functional class (2.4 vs 1.8, p <0.01). The prevalence of uncontrolled hypertension decreasedfrom 56% at the initial visit to 37% at the last visit (p [ 0.01). The cohort had a low rate ofadverse cardiovascular outcomes such as death, acute coronary syndromes, and stroke. Inconclusion, the present study demonstrates that stepwise, symptom-oriented therapy is feasibleand effective in patients with coexisting HC and hypertension. � 2013 Elsevier Inc. All rightsreserved. (Am J Cardiol 2013;111:1040e1045)
Hypertension is highly prevalent in the general population,and patients with hypertrophic cardiomyopathy (HC) are notexempt from hypertension. At the same time, treatment ofpatients with HC and hypertension can be challenging. Directvasodilators such as dihydropyridine calcium channelblockers and renin-angiotensin system blockers (angiotensin-converting enzyme [ACE] inhibitors and angiotensin receptorblockers [ARBs]) are among the most efficacious and well-tolerated medications for the treatment of hypertension ingeneral. However, these drugs can exacerbate outflow tractobstruction in patients with HC and may be potentiallyharmful.1,2 The 2011 American College of CardiologyFoundation and American Heart Association guidelines forthe diagnosis and treatment of HC provide little guidance forantihypertensive therapy in patients affected by both condi-tions.1 In the present retrospective study, we analyzed theefficacy and safety of antihypertensive therapy in patientswith HC as practiced at the St. Luke’s-Roosevelt HospitalCenter (SLRHC) HC program in New York.
Methods
We conducted a retrospective cohort study of patientswith HC with coexisting hypertension referred to the
Cardiomyopathy Program, Division of Cardiology, St.Hospital Center, Columbia University College of
urgeons, New York, New York. Manuscript received2; revised manuscript received and accepted December
for disclosure information.g author: Tel: 212-523-7372; fax: 212-523-7765.s: [email protected] (M.V. Sherrid).
see front matter � 2013 Elsevier Inc. All rights reserved.0.1016/j.amjcard.2012.12.026
SLRHC HC program from January 1995 to January 2011.Patients were referred for confirmation of diagnosis andtreatment recommendations. Criteria for diagnosis of HCin this study were echocardiographic demonstration ofa hypertrophied nondilated left ventricle �15 mm inappro-priate for the degree of hypertension severity and only if �1of the following 3 criteria were present: (1) dynamic leftventricular (LV) outflow tract (LVOT) obstruction due tosystolic anterior motion of the mitral valve and mitral-septalcontact at rest or with physiologic provocation, (2) echo-cardiographic abnormalities typical of HC and generally notseen in hypertensive heart disease (i.e., apical or apical-midhypertrophy sparing the base, marked asymmetric hyper-trophy with systolic anterior motion but with gradients<30 mm Hg, or severe asymmetric hypertrophy with mildhypertension),1,3e5 and (3) in patients with nonobstructiveHC, ancillary supportive criteria were a family history ofHC in a first-degree family member or genotype analysisshowing an HC-related sarcomeric protein mutation.
Hypertension was diagnosed conservatively only if 1 orboth of the following criteria were present at the initialevaluation: (1) the patient was being actively treated for anestablished diagnosis of hypertension with a vasodilator suchas a dihydropyridine calcium channel blocker, an ACEinhibitor, or an ARB; a thiazide-type diuretic; or clonidine,and (2) the patient had elevated blood pressure readings,defined as systolic pressure �140 mm Hg and/or diastolicpressure �90 mm Hg, on 2 consecutive SLRHC clinic visits.
Demographic, clinical, and laboratory data were obtainedby retrospective chart review. Blood pressure readings andmedications were compared between the initial and the lastvisits. The study was approved by the institutional reviewboard of St. Luke’s Roosevelt Hospital.
www.ajconline.org

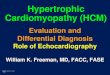
Figure 1. General approach to patients with symptomatic HC and hypertension. AV ¼ atrioventricular; CCB ¼ calcium channel blocker.
Cardiomyopathy/Hypertension in Hypertrophic Cardiomyopathy 1041
Maximal LV wall thickness was measured from para-sternal long-axis and short-axis views on 2-dimensionalechocardiography, as previously described.6 The initial andfollow-up echocardiograms were specifically assessed forsystolic anterior motion of the mitral valve and peakinstantaneous LVOT gradients. The simplified Bernoulliequation was used to calculate LVOT gradient, and thehighest instantaneous gradient was reported.7 Care wastaken to separate LVOT signal from that of mitral regurgi-tation. In all patients, the LVOT gradient was measured inthe supine left lateral decubitus position and during 3separate Valsalva maneuvers and after standing, as previ-ously reported.8 All patients capable of exercising under-went treadmill testing with the Bruce protocol and hadgradients acquired after exercise. Patients were excludedfrom exercise if they had orthopedic disabilities or suchsevere heart failure symptoms that they were deemed inca-pable of performing even a modified, reduced treadmillprotocol, or for rest gradients >80 mm Hg. Beta blockerswere held the morning of the stress test, while other medi-cations were continued. Postestress exercise continuous-wave Doppler gradients from the apical views were acquiredin the supine left lateral decubitus position within 30e60seconds after the completion of exercise and then again3 minutes later.9e11 Patients were deemed to be obstructed if
the maximal peak instantaneous LVOT gradient (at rest orprovoked, including postexercise) was �30 mm Hg.Patients with follow-up durations <30 days as well as thosewithout follow-up echocardiographic data were excluded.Patients were also excluded if they had severe mitralregurgitation thought to be unrelated to systolic anteriormotion, or severe aortic stenosis.
Patients underwent formal stratification for sudden deathrisk and implantation of implantable cardioverter-defibrillatorsif, after consideration, the benefits of implantation appeared tooutweigh the risks.1 In patients with symptomatic obstructiveHC, the initial treatment consisted of discontinuation ofvasodilators (if the patient was taking a vasodilator) andadministration of maximal tolerated doses of b blockers,nondihydropyridine calcium channel blockers, or both(Figure 1). Beta blockade was the first-line therapy. In patientsin whom hypertension was the main current problem, verap-amil or diltiazem was started as needed and as heart ratepermitted.1,12 If symptoms and elevated gradients persistedafter b blockade or nondihydropyridine calcium channelblockade, controlled-release disopyramide was generallyadded as previously reported.13e16 A combination of all3 agents was generally avoided unless the patient had apermanent pacemaker. Patients with symptoms refractoryto pharmacologic management and rest or provoked gradients

Table 1Baseline characteristics
Variable Overall (n ¼ 115) LVOT Obstruction p Value*
Yes (n ¼ 94) No (n ¼ 21)
Age (yrs) 60.0 � 11.7 60.2 � 11.6 59.2 � 12.5 0.73Men 67 (58%) 54 (58%) 13 (62%) 0.71Caucasian 93 (81%) 77 (82%) 16 (76%) 0.55Syncope 16 (14%) 14 (15%) 2 (10%) 0.52Dyspnea 86 (75%) 77 (82%) 9 (43%) <0.01Angina 42 (37%) 36 (38%) 6 (29%) 0.40Diabetes mellitus 15 (13%) 11 (12%) 4 (19%) 0.37Coronary artery disease 22 (19%) 21 (22%) 1 (5%) 0.07Percutaneous coronary intervention 11 (10%) 10 (11%) 1 (5%) 0.69Coronary bypass grafting 3 (3%) 3 (3%) 0 —
Congestive heart failure 12 (10%) 12 (13%) 0 —
Valve surgery 3 (3%) 3 (3%) 0 —
Atrial fibrillation 26 (23%) 20 (21%) 6 (29%) 0.47More than mild mitral regurgitation 21 (18%) 20 (21%) 1 (5%) 0.12More than mild aortic regurgitation 5 (4%) 4 (4%) 1 (5%) 1.0More than mild aortic stenosis 2 (2%) 2 (2%) 0 —
Implanted device 5 (4%) 3 (3%) 2 (10%) 0.23Septal myectomy 2 (2%) 1 (1%) 1 (5%) 0.33Alcohol septal ablation 2 (2%) 1 (1%) 1 (5%) 0.33Septal thickness (mm) 19.5 � 4.4 19.7 � 4.4 19.0 � 4.4 0.51
Data are expressed as mean � SD or as number (percentage).* Comparing obstructed to nonobstructed patients.
1042 The American Journal of Cardiology (www.ajconline.org)
>50 mm Hg were referred for surgical myectomy. Alcoholseptal ablation was reserved for patients with medicalcontraindications for surgery.1,17 DDD pacing with shortatrioventricular delay and complete ventricular capture wasapplied selectively in specific conditions: (1) in elderlypatients who failed pharmacologic therapy and who weredeemed to not be good candidates for any other intervention,(2) when an implantable cardioverter-defibrillator wasimplanted for sudden death prevention in an obstructed patientwith mild to moderate heart failure symptoms or syncope, and(3) for symptomatic bradycardia.1 In patients with persistenthypertension after the initial therapy as outlined, clonidine0.1 mg once or twice daily was given. In patients withrefractory hypertension, 12.5 mg (preferred) to 25 mghydrochlorothiazide was continued or added, generally inassociation with triamterene.
We first assessed the reduction of LVOT gradient at restand HC-related symptoms. Because many patients did notundergo repeat exercise testing for gradient provocationbecause symptoms diminished, we did not compare provokedLVOT gradients before and after treatment. Second, weexamined the prevalence of hypertension control, defined assystolic pressure <140 mm Hg and diastolic pressure<90 mm Hg at the last visit, and compared blood pressure onthe first visit and last visit. Symptoms were assessed by NewYork Heart Association functional class. Clinical outcomesincluded all-cause mortality, stroke, new-onset atrial fibrilla-tion, acute coronary syndromes, and congestive heart failurehospitalizations.
Means and proportions are reported for the initial andfollow-up visits. Continuous variables are reported as mean� SD. Means were compared using Student’s t tests, andproportions were compared using chi-square tests and
Fisher’s exact tests. Primary and secondary outcomes wereanalyzed separately for obstructed and nonobstructedpatients. For that purpose, 2-sided paired Student’s t testsand Wilcoxon’s tests were used to compare 2 means, andMcNemar’s tests were used to compare proportions. Allanalyses were performed using commercially availablestatistical software (SPSS for Windows version 16.0; SPSS,Inc., Chicago, Illinois).
Results
In this time period, 755 patients with HC had initialevaluation at SLRHC. One hundred fifteen patients (meanage 60 years, 58% men) met the eligibility criteria for thestudy and were included in the analysis, with a meanfollow-up period of 36 � 32 months (range 1 to 192).Patients with hypertension were older than the rest of theSLRHC cohort without hypertension (mean age 60 vs53 years, p <0.01). The baseline characteristics for theentire cohort (115 patients) and separately for theobstructed (94 patients, mean rest gradient 48 mm Hg,provoked gradient 112 mm Hg) and nonobstructed(21 patients) groups are listed in Table 1. Overall, patientscarried a high burden of symptoms, the most commonbeing dyspnea (75%). Sixty-two patients (54%) hadhypertension (blood pressure �140/90 mm Hg) at theinitial evaluation. Results are divided into obstructed andnonobstructed patient groups.
Because of our treatment strategy, there was a significantdecrease in the number of patients treated with peripheralvasodilators such as ACE inhibitors or ARBs (42% vs 14%,p <0.01) and dihydropyridine calcium channel blockers(13% vs 4%, p ¼ 0.03). More patients were treated with

Table 3Changes between the first and the last visits in nonobstructed patients(n ¼ 21)
Variable Initial Visit Last Visit p Value
Hypertensive 9 (43%) 6 (29%) 0.26Systolic blood pressure (mm Hg) 130 � 17* 124 � 17 0.13Diastolic blood pressure (mm Hg) 78 � 11* 75 � 9 0.12Heart rate (beats/min) 65 � 9 67 � 10 0.41New York Heart Association class 1.8 � 0.6 1.5 � 0.7 0.03Beta blockers 12 (57%) 13 (62%) 0.66Increase in dose 7 (58%)
Verapamil 4 (19%) 6 (29%) 0.41Diltiazem 2 (10%) 2 (10%) 1.00ACE inhibitors/ARBs 11 (52%) 7 (33%) 0.10Dihydropyridine calcium channel
blockers2 (10%) 4 (19%) 0.16
Thiazide diuretics 4 (19%) 3 (14%) 0.66Loop diuretics 5 (24%) 3 (14%) 0.16Clonidine 0 0 —
Data are expressed as mean � SD or as number (percentage).* Fifty-two percent of patients with nonobstructive HC with hypertension
were taking ACE inhibitors or ARBs and 10% were taking dihydropyridinecalcium channel blockers at initial evaluation.
Table 2Changes between the first and the last visits in obstructed patients (n ¼ 94)
Variable Initial Visit Last Visit p Value
Hypertensive 53 (56%) 35 (37%) 0.01Systolic blood pressure (mm Hg) 137 � 21* 131 � 16 0.01Diastolic blood pressure (mm Hg) 80 � 11* 77 � 8 0.05Heart rate (beats/min) 65 � 12 62 � 11 0.03Rest LVOT gradient (mm Hg) 48 � 49 14 � 26 <0.01Provoked LVOT gradient (mm Hg) 112 � 53†
New York Heart Association class 2.4 � 0.8 1.8 � 0.7 <0.01b blockers 58 (62%) 81 (86%) <0.01Increase in dose 44 (76%)
Verapamil 22 (23%) 15 (16%) 0.13Diltiazem 6 (6%) 10 (11%) 0.21ACE inhibitors/ARBs 39 (42%) 13 (14%) <0.01Dihydropyridine calcium channel
blockers12 (13%) 4 (4%) 0.03
Thiazide diuretics 18 (19%) 16 (17%) 0.66Disopyramide 8 (9%) 33 (35%) <0.01Loop diuretics 7 (8%) 8 (9%) 0.74Clonidine 3 (3%) 10 (11%) 0.02
Data are expressed as mean � SD or as number (percentage).* Forty-two percent of patients with obstructive HC with hypertension
were taking ACE inhibitors or ARBs and 13% were taking dihydropyridinecalcium channel blockers at initial evaluation.
† Many patients did not exercise again at follow-up if symptomatic reliefwas obtained.
Cardiomyopathy/Hypertension in Hypertrophic Cardiomyopathy 1043
b blockers (62% vs 86%, p <0.01) at the last visit comparedto the initial visit, and the doses were increased in 76% ofpatients who were taking b blockers at the initial evaluation(Table 2). Disopyramide therapy was increased from 9% to35% of patients. Despite optimal pharmacologic manage-ment, 21 obstructed patients (22%) required septal reductiontherapy for symptoms and resistant gradients (surgicalmyectomy in 19 and alcohol septal ablation in 2). In15 patients (16%), DDD pacing was used for gradientreduction.
With treatment that included septal reduction therapy inselected patients as outlined previously, peak instantaneousLVOT gradient at rest decreased from 48 to 14 mm Hg(p <0.01). Among obstructed patients who did not undergoseptal reduction therapy (n ¼ 73), peak instantaneous LVOTgradient at rest decreased from 41 to 18 mm Hg (p <0.01).Overall, the patients experienced a significant reduction insymptom burden during the follow-up period, as assessedby New York Heart Association class (2.4 vs 1.8, p <0.01).
The use of clonidine increased from 3% to 11%(p ¼ 0.02). The proportion of patients taking low-dosethiazide diuretics remained similar at 19% and 17%respectively. Despite our stopping peripheral vasodilatorssuch as ACE inhibitors or ARBs and dihydropyridinecalcium channel blockers, the average systolic pressuredecreased from 137 to 131 mm Hg (p ¼ 0.01). The preva-lence of uncontrolled hypertension decreased from 53 (56%)at the initial visit to 35 (37%) at the last visit (p ¼ 0.01;Table 2).
Twenty-one patients with HC had maximal provokedinstantaneous LVOT gradients <30 mm Hg on therapy atinitial evaluation (the nonobstructed group). In this group,
19 patients (90%) had patterns of LV hypertrophy typical ofHC and not generally seen in hypertensive heart diseasewith mild elevation of blood pressure. These were apical orapical-mid HC sparing the base in 5 (24%), asymmetricseptal hypertrophy with systolic anterior motion butprovoked LVOT gradients <30 mm Hg in 3 (14%), andmarked asymmetric thickening of the left ventricle dispro-portionate to the degree of hypertension in 11 (52%).5 Twopatients (10%) had septal reduction therapy before initialevaluation: 1 patient had septal myectomy and 1 patient hadalcohol septal ablation. In 8 patients (38%), the diagnosiswas supported by positive family history and/or genemutation characteristic of HC.
Symptoms were less troubling in the nonobstructedgroup compared to the obstructed patients: New York HeartAssociation class 1.8 versus 2.4 (p <0.01) and prevalence ofdyspnea 43% versus 82% (p <0.01). Eleven patients (52%)were taking direct vasodilators, and 4 (19%) were takingthiazide diuretics at initial evaluation. With this pharmaco-therapy, in the nonobstructed patients, 9 (43%) had hyper-tension at initial evaluation (Table 3). Beta blocker andcalcium channel blocker therapy was optimized in thesepatients for blood pressure and symptom control. Thesymptoms mildly diminished (New York Heart Associationclass 1.8 vs 1.5, p ¼ 0.03), and the prevalence of hyper-tension trended lower (43% vs 29%, p ¼ 0.26) at the lastvisit compared to the initial evaluation.
During the mean follow-up period of 36 months, only 1patient died from a noncardiovascular cause (small bowelobstruction). Six patients were newly diagnosed with atrialfibrillation. One patient sustained a stroke, 1 patient had anacute coronary syndrome, and 2 patients were hospitalizedfor acute decompensated heart failure. There was no dete-rioration in renal function in any patient due to withdrawalof an ACE inhibitor or ARB over the average 3-year follow-up period. Nineteen patients (17%) had implantablecardioverter-defibrillators inserted for sudden cardiac death

1044 The American Journal of Cardiology (www.ajconline.org)
prevention. There were 2 appropriate and no inappropriatedischarges during the follow-up period.
Discussion
Patients with HC and systemic hypertension presentclinicians with challenging therapeutic and diagnosticdilemmas. Consultants will frequently be referred symp-tomatic patients with HC who are already taking potentvasodilators, as were half the patients in this series.Although vasodilators are the most effective and well-tolerated agents for the treatment of hypertension, in patientswith HC, obstructed and nonobstructed, these drugs can beharmful.1,18 In obstructed patients, vasodilators mayprovoke heart failure symptoms, angina, or syncope bydecreasing preload and afterload and increasing LVOTobstruction.1,2,8 In certain nonobstructed patients, particu-larly those with small LV diastolic chambers, decreasingpreload can decrease stroke volume and cause symp-toms.3,18 However, in patients with nonobstructive HCwithout extreme encroachment of the LV cavity, vasodila-tors have traditionally been used without adverse effects.Hypertension control in this study was modest but wasbetter than the national average of approximately 50%.19 Ofnote, the evidence for treating complex patients with HCwith coexisting hypertension, focusing on symptom controland hypertension control, and long-term outcomes, isextremely scarce.
A hypertension treatment strategy as described in thisreport can provide a framework for management of patientswith HC and coexisting hypertension (Figure 1). Symptomcontrol, which is often the reason for specialist referral, isprioritized in obstructed patients. It may be achieved byvasodilator discontinuation and up-titration of a b blocker orverapamil as tolerated. Disopyramide is added in selectedsymptomatic patients for gradient reduction when symptomspersist despite b blockers or verapamil. If optimal pharma-cologic therapy fails and rest or provoked gradients are�50 mm Hg, septal reduction therapy leads to the abolitionof gradients and symptomatic improvement.
In patients with persistent hypertension despite optimalsymptom-control therapy, oral clonidine or a low-dosethiazide diuretic (12.5 to 25 mg of hydrochlorothiazide withtriamterene) can assist in blood pressure control. Clonidinesuppresses central sympathetic activity and as such may notincrease LVOT gradients. Low-dose thiazide can usuallyonly be used with potent concomitant negative inotropictherapy (i.e., disopyramide). We underscore that the strategywe used led not only to significant symptom reduction butalso better hypertension control despite discontinuation ofvasodilators in most patients. The long-term outcomes werefavorable, with low mortality and a low incidence of adversecardiovascular events.
We advance two hypotheses relevant to the concurrenceof HC and hypertension. First, hypertension is exceedinglycommon in the United States population, with an estimatedprevalence close to 30% in the adult population, while HChas a prevalence of 0.2% (1 in 500) in the general pop-ulation.19,20 By coincidence alone, one might expect thatclose to 1/3 of patients with HC may have hypertension.Several arguments support this. First, our hypertensive
patients with HC were older than normotensive patients withHC and presented for evaluation at a mean age of 60 years,congruent with the increased prevalence of hypertension inolder patients. Also, recent data from the Framingham studyhave shown that in the general population, asymptomaticpatients with mild hypertension and LV hypertrophy mayhave HC-associated sarcomeric protein mutations.21 Asecond hypothesis is that the systolic hypertension observedin our patients could have originated from the rapid ejectionof blood very early in systole, before LV obstruction occurs.Maron et al22 found that 75% of the LV forward flowvelocity was ejected in the first third of systole, compared to37% of forward flow velocity in normal patientss.21 Othershave observed rapid early volumetric flow on pulseDoppler23 and with cine angiography. This front-loading ofLV ejection may temporally overwhelm the compliance ofthe large arteries of older patients. Thus, there may be a LVhemodynamic component of hypertension in these patients.This hypothesis has potential therapeutic implications,because potent negative inotropic therapy decreases rapidLV ejection in early systole.24 We believe that the 2 mech-anisms for hypertension occur in patients with HC toa varying degree; the latter may be detected by pulsedDoppler echocardiographic interrogation of LV ejectionvelocities at the entrance of the LVOT upstream of themitral valve24 and in the aorta.22
Limitations of the present study include its observationalnature and single-center experience. Besides, hypertensioncontrol was assessed during office visits representing single-point measurements as opposed to a 24-hour observation, ascan be obtained by ambulatory blood pressure monitoring.Indeed, we used 24-hour blood pressure monitoring forselected patients with labile or white-coat hypertension inwhom the adequacy of blood pressure control was anongoing clinical question. Should all cardiac medicationshave been stopped several days before the initial evaluationto confirm the diagnosis of hypertension or obstruction? Weconsidered this approach but did not pursue it for threereasons. First, we hoped to correlate the patient’s currentsymptoms with the current LVOT gradient. We hoped tounderstand the cause of current symptoms because gradientreduction is the best strategy for symptom reduction.Second, stopping medications may lead to unacceptableblood pressure elevation that precludes exercise testing. Thisis especially true when b blockers are held for several days.Third, although holding vasodilators might have improvedgradients, we view vasodilator-induced obstruction to beanother form of provocation.
In conclusion, the present study demonstrates that step-wise, symptom-oriented therapy is feasible and effective inpatients with coexisting HC and hypertension.
Disclosures
The authors have no conflicts of interest to disclose.
1. Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS,Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE,Towbin JA, Udelson JE, Yancy CW. 2011 ACCF/AHA guideline forthe diagnosis and treatment of hypertrophic cardiomyopathy: a reportof the American College of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines. Developed in

Cardiomyopathy/Hypertension in Hypertrophic Cardiomyopathy 1045
collaboration with the American Association for Thoracic Surgery,American Society of Echocardiography, American Society of NuclearCardiology, Heart Failure Society of America, Heart Rhythm Society,Society for Cardiovascular Angiography and Interventions, and Societyof Thoracic Surgeons. J Am Coll Cardiol 2011;58:e212ee260.
2. Kyriakidis M, Triposkiadis F, Dernellis J, Androulakis AE, Mellas P,Kelepeshis GA, Gialafos JE. Effects of cardiac versus circulatoryangiotensin-converting enzyme inhibition on left ventricular diastolicfunction and coronary blood flow in hypertrophic obstructive cardio-myopathy. Circulation 1998;97:1342e1347.
3. Shah A, Duncan K, Winson G, Chaudhry FA, Sherrid MV. Severesymptoms in mid and apical hypertrophic cardiomyopathy. Echocar-diography 2009;26:922e933.
4. Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA2002;287:1308e1320.
5. Lewis JF, Maron BJ. Diversity of patterns of hypertrophy in patientswith systemic hypertension and marked left ventricular wall thickening.Am J Cardiol 1990;65:874e881.
6. Spirito P, Bellone P, Harris KM, Bernabo P, Bruzzi P, Maron BJ.Magnitude of left ventricular hypertrophy and risk of sudden deathin hypertrophic cardiomyopathy. N Engl J Med 2000;342:1778e1785.
7. Sasson Z, Yock PG, Hatle LK, Alderman EL, Popp RL. Dopplerechocardiographic determination of the pressure gradient in hypertro-phic cardiomyopathy. J Am Coll Cardiol 1988;11:752e756.
8. Joshi S, Patel UK, Yao SS, Castenada V, Isambert A, Winson G,Chaudhry FA, Sherrid MV. Standing and exercise Doppler echocar-diography in obstructive hypertrophic cardiomyopathy: the range ofgradients with upright activity. J Am Soc Echocardiogr 2011;24:75e82.
9. Klues HG, Leuner C, Kuhn H. Left ventricular outflow tract obstructionin patients with hypertrophic cardiomyopathy: increase in gradient afterexercise. J Am Coll Cardiol 1992;19:527e533.
10. Maron MS, Olivotto I, Zenovich AG, Link MS, Pandian NG, KuvinJT, Nistri S, Cecchi F, Udelson JE, Maron BJ. Hypertrophic cardio-myopathy is predominantly a disease of left ventricular outflow tractobstruction. Circulation 2006;114:2232e2239.
11. Drinko JK, Nash PJ, Lever HM, Asher CR. Safety of stress testing inpatients with hypertrophic cardiomyopathy. Am J Cardiol 2004;93:1443e1444.
12. Epstein SE, Rosing DR. Verapamil: its potential for causing seriouscomplications in patients with hypertrophic cardiomyopathy. Circula-tion 1981;64:437e441.
13. Sherrid MV, Barac I, McKenna WJ, Elliott PM, Dickie S, ChojnowskaL, Casey S, Maron BJ. Multicenter study of the efficacy and safety ofdisopyramide in obstructive hypertrophic cardiomyopathy. J Am CollCardiol 2005;45:1251e1258.
14. Wigle ED, Rakowski H, Kimball BP, Williams WG. Hypertrophiccardiomyopathy. Clinical spectrum and treatment. Circulation1995;92:1680e1692.
15. Fifer MA, Vlahakes GJ. Management of symptoms in hypertrophiccardiomyopathy. Circulation 2008;117:429e439.
16. Sherrid MV, Arabadjian M. A primer of disopyramide treatment ofobstructive hypertrophic cardiomyopathy. Prog Cardiovasc Dis2012;54:483e492.
17. Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ,Seidman CE, Shah PM, Spencer WH III, Spirito P, Ten Cate FJ, WigleED. American College of Cardiology/European Society of Cardiologyclinical expert consensus document on hypertrophic cardiomyopathy.A report of the American College of Cardiology Foundation TaskForce on Clinical Expert Consensus Documents and the EuropeanSociety of Cardiology Committee for Practice Guidelines. J Am CollCardiol 2003;42:1687e1713.
18. Topol EJ, Traill TA, Fortuin NJ. Hypertensive hypertrophic cardio-myopathy of the elderly. N Engl J Med 1985;312:277e283.
19. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness,treatment, and control of hypertension 1988e2008. JAMA 2010;303:2043e2050.
20. Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE.Prevalence of hypertrophic cardiomyopathy in a general population ofyoung adults. Echocardiographic analysis of 4111 subjects in theCARDIA Study. Circulation 1995;92:785e789.
21. Morita H, Larson MG, Barr SC, Vasan RS, O’Donnell CJ, HirschhornJN, Levy D, Corey D, Seidman CE, Seidman JG, Benjamin EJ. Single-gene mutations and increased left ventricular wall thickness in thecommunity: the Framingham Heart Study. Circulation 2006;113:2697e2705.
22. Maron BJ, Gottdiener JS, Arce J, Rosing DR, Wesley YE, Epstein SE.Dynamic subaortic obstruction in hypertrophic cardiomyopathy: analysisby pulsed Doppler echocardiography. J Am Coll Cardiol 1985;6:1e18.
23. Conklin HM, Huang X, Davies CH, Sahn DJ, Shively BK. Biphasicleft ventricular outflow and its mechanism in hypertrophic obstructivecardiomyopathy. J Am Soc Echocardiogr 2004;17:375e383.
24. Sherrid MV, Pearle G, Gunsburg DZ. Mechanism of benefit of negativeinotropes in obstructive hypertrophic cardiomyopathy. Circulation1998;97:41e47.