Embed Size (px)
Citation preview

Original article
Anti-nuclear antibody positivity and the use of certolizumabin inflammatory bowel disease patients who have had
arthralgias or lupus-like reactions from infliximabor adalimumab
Himanshu Dev VERMA,* Ellen Janice SCHERL,† Vinita Elizabeth JACOB† & Brian Paul BOSWORTH†
*Department of Medicine, Weil Cornell Medical College, New York Presbyterian Hospital, and †Division ofGastroenterology and Hepatology, Jill Roberts Inflammatory Bowel Disease Center, Weil Cornell Medical
College, New York, USA
OBJECTIVE: Tumor necrosis factor (TNF) inhibitorscan be used to treat inflammatory bowel disease (IBD)but may lead to anti-nuclear antibody (ANA) positiv-ity and lupus-like reactions. Because of its uniquestructure, certolizumab has lower rates of these com-plications. We sought to investigate whether patientswho have had lupus-like reactions to infliximab oradalimumab would be able to tolerate certolizumab.
METHODS: We performed a retrospective analysison the 23 patients at the Roberts Inflammatory BowelDisease Center who received certolizumab for thetreatment of Crohn’s disease from March 2008 toJune 2009. We identified 6 patients who wereswitched to this drug because of lupus-like reactionsfrom prior anti-TNF therapy and had documentedANA after the reaction and prior to certolizumab ini-tiation. We then rechecked the ANA status after cer-tolizumab initiation.
RESULTS: Five out of 6 patients had a resolutionof their arthralgias or lupus-like symptoms afterbeing switched to certolizumab (P < 0.001). Of the 4patients who were ANA positive after receiving inflix-imab or adalimumab, 2 became ANA negative afterinduction with certolizumab (P = 0.17). There wasno difference in Harvey Bradshaw index scores(10.3 vs. 9.8) pre-certolizumab and post-certolizumab(P = 0.73).
CONCLUSION: Nearly all patients experiencedrelief from their lupus-like symptoms with certoli-zumab and 2 out of 4 patients reversed their ANApositivity. While future investigation is warranted,patients who have lupus-like reactions from inflix-imab or adalimumab may benefit from switching tocertolizumab.
KEY WORDS: anti-nuclear antibody, inflammatory bowel disease, systemic lupus erythematosus, tumor necro-sis factor inhibitor.
Presented as a poster presentation at the American College of Gastroenterology in October 2009.Correspondence to: Himanshu Dev VERMA, Department of Medicine, Weil Cornell Medical College, New York Presbyterian Hospital, New York,NY 10021, USA. Email: [email protected]© 2011 The AuthorsJournal of Digestive Diseases © 2011 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji HospitalAffiliated to Shanghai Jiaotong University School of Medicine and Blackwell Publishing Asia Pty Ltd.
Journal of Digestive Diseases 2011; 12; 379–383 doi: 10.1111/j.1751-2980.2011.00522.x
379

INTRODUCTION
Tumor necrosis factor (TNF)-a is a pro-inflammatorycytokine that has been shown to be a key componentin the pathogenesis of several auto-immune diseases,including Crohn’s disease. This discovery ultimatelyled to the development of TNF-a-inhibiting drugs,with profound results on disease activity. In recentyears, as the medical literature and clinical experiencewith these drugs has grown, TNF-a inhibitors havebecome increasingly used for the treatment of Crohn’sdisease and ulcerative colitis.1–9 Infliximab, adali-mumab and certolizumab have shown a clinicalbenefit for moderate to severe disease and disease thatis refractory to conventional treatment and they havenow even become a first-line treatment in certaincases.10,11
However, TNF-a also plays a physiological role incell growth and death, development, oncogenesisand immune, inflammatory and stress responses. TheTNF-a blockade decreases disease activity in inflam-matory bowel disease (IBD) patients, but it is alsolinked to many complications including a possibleincreased risk of cancer, infection, neurologicaldisorders, auto-immunity, lupus-like reaction andanti-nuclear antibody (ANA) positivity. Lupus-likereactions and ANA positivity are among the adverseeffects with unclear mechanisms. However, the ratesof these reactions seem to be higher with infliximaband adalimumab than those with certolizumab.
While each of these drugs inhibits TNF-a, their funda-mental structures vary considerably. Infliximab andadalimumab are monoclonal antibodies consistingof both a fragment crystallizable (Fc) and fragmentantigen binding (Fab) region. They differ in that inflix-imab has a 30% murine Fab portion and adalimumabis nearly 100% human. Certolizumab is composedof a human Fab portion attached to a polyethyleneglycol molecule. Infliximab and adalimumab bind tosoluble and membrane-bound TNF-a, causing anti-body mediated, complement mediated and apoptoticcell death. Certolizumab, which lacks an Fc portionbinds to soluble and membrane-bound TNF-a it doesnot fix complement and lead to apoptosis with thesubsequent exposure of nuclear antigens.12
We hypothesized that patients who have had a lupus-like reaction or ANA positivity from infliximab oradalimumab would be able to tolerate certolizumaband its use may reverse their ANA positivity.
MATERIALS AND METHODS
We performed a retrospective analysis of the 23patients at the Jill Roberts Inflammatory BowelDisease Center who received certolizumab for thetreatment of inflammatory bowel disease from March2008 to June 2009 and identified 8 patients whowere switched to this drug because of arthralgias orlupus-like reactions from prior anti-TNF therapy. Alupus-like reaction was defined as any significant com-bination of rash, myalgias, arthralgias, or fever thatoccurred following the administration of a TNFinhibitor. One patient was excluded because she didnot have an ANA drawn after being switched to cer-tolizumab and another was excluded because she hadreceived prednisone for her lupus-like reactions andcertolizumab was ultimately stopped by the time herrepeat ANA was drawn. Five out of the 6 patientshad indeterminate colitis that had features of bothulcerative colitis and Crohn’s disease and could notbe definitely categorized by one diagnosis. Thus, 6patients were included in the study, each of whom hada documented ANA test after developing arthralgias ora lupus-like reaction to infliximab or adalimumab andprior to the initiation of treatment with certolizumab(Table 1). We then redrew ANA titers on the patientsafter they had received at least three doses of certoli-zumab. This data was tabulated and a standard t-testanalysis was performed to see whether there was asignificant change of ANA status after receivingcertolizumab. We also documented whether eachpatient had a resolution of the arthralgia or lupus-likesymptoms as and the Harvey Bradshaw index
Table 1. Participants’ baseline characteristics (n = 6)
Male : female ratio (%) 3:3 (50)Median age (years, range) 41 (27–58)Ratio of patients receiving adalimumab to
infliximab1:5
Currently on azathioprine or6-mercaptopurine
0
Median days of anti-TNF therapy prior tosymptoms (range)
15 (1–173)
Median days from symptoms to ANAdrawn pre-certolizumab (range)
34 (7–60)
Median days from symptoms tocertolizumab initiation
82 (14–132)
Median days from certolizumab initiationto repeat ANA (range)
92 (43–245)
Ratio of patients with IBD type Crohn’s:indeterminate colitis
1:5
ANA, anti-nuclear antibody; IBD, inflammatory bowel disease;TNF, tumor necrosis factor.
Journal of Digestive Diseases 2011; 12; 379–383380 HD Verma et al.
© 2011 The AuthorsJournal of Digestive Diseases © 2011 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to
Shanghai Jiaotong University School of Medicine and Blackwell Publishing Asia Pty Ltd.
(HBI) scores before and after certolizumab treatmentwith subsequent t-test analyses performed for thesevariables.
RESULTS
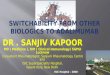
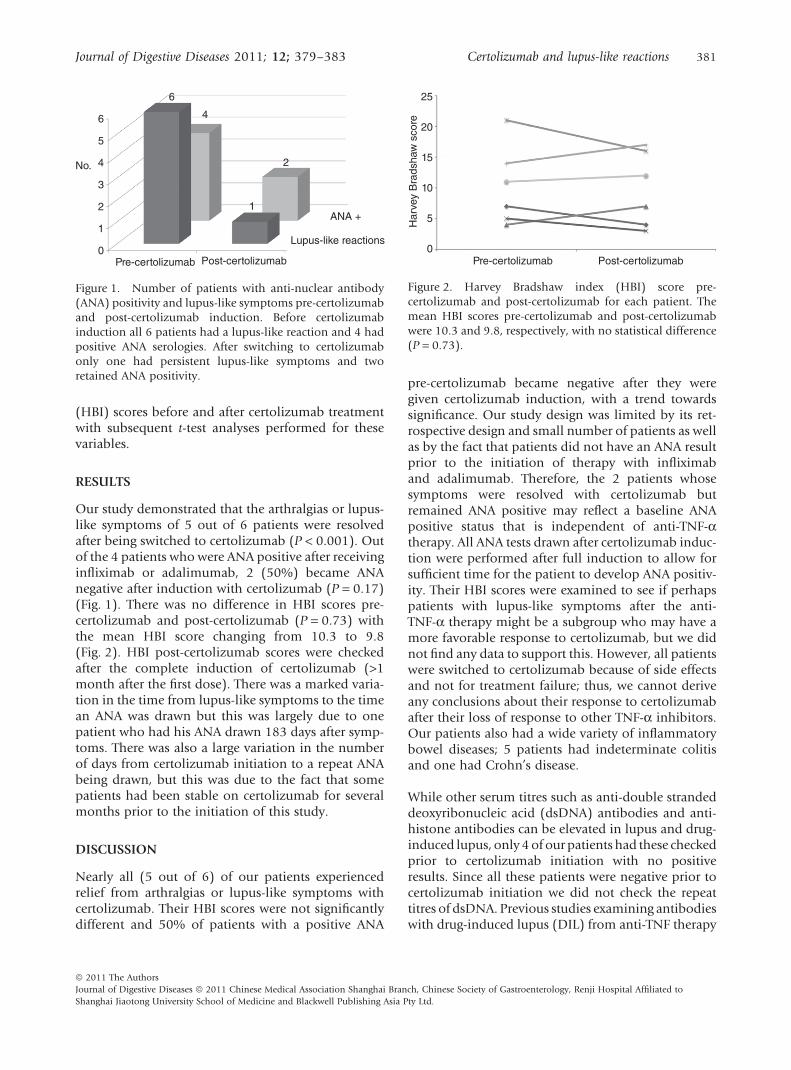
Our study demonstrated that the arthralgias or lupus-like symptoms of 5 out of 6 patients were resolvedafter being switched to certolizumab (P < 0.001). Outof the 4 patients who were ANA positive after receivinginfliximab or adalimumab, 2 (50%) became ANAnegative after induction with certolizumab (P = 0.17)(Fig. 1). There was no difference in HBI scores pre-certolizumab and post-certolizumab (P = 0.73) withthe mean HBI score changing from 10.3 to 9.8(Fig. 2). HBI post-certolizumab scores were checkedafter the complete induction of certolizumab (>1month after the first dose). There was a marked varia-tion in the time from lupus-like symptoms to the timean ANA was drawn but this was largely due to onepatient who had his ANA drawn 183 days after symp-toms. There was also a large variation in the numberof days from certolizumab initiation to a repeat ANAbeing drawn, but this was due to the fact that somepatients had been stable on certolizumab for severalmonths prior to the initiation of this study.
DISCUSSION
Nearly all (5 out of 6) of our patients experiencedrelief from arthralgias or lupus-like symptoms withcertolizumab. Their HBI scores were not significantlydifferent and 50% of patients with a positive ANA
pre-certolizumab became negative after they weregiven certolizumab induction, with a trend towardssignificance. Our study design was limited by its ret-rospective design and small number of patients as wellas by the fact that patients did not have an ANA resultprior to the initiation of therapy with infliximaband adalimumab. Therefore, the 2 patients whosesymptoms were resolved with certolizumab butremained ANA positive may reflect a baseline ANApositive status that is independent of anti-TNF-atherapy. All ANA tests drawn after certolizumab induc-tion were performed after full induction to allow forsufficient time for the patient to develop ANA positiv-ity. Their HBI scores were examined to see if perhapspatients with lupus-like symptoms after the anti-TNF-a therapy might be a subgroup who may have amore favorable response to certolizumab, but we didnot find any data to support this. However, all patientswere switched to certolizumab because of side effectsand not for treatment failure; thus, we cannot deriveany conclusions about their response to certolizumabafter their loss of response to other TNF-a inhibitors.Our patients also had a wide variety of inflammatorybowel diseases; 5 patients had indeterminate colitisand one had Crohn’s disease.
While other serum titres such as anti-double strandeddeoxyribonucleic acid (dsDNA) antibodies and anti-histone antibodies can be elevated in lupus and drug-induced lupus, only 4 of our patients had these checkedprior to certolizumab initiation with no positiveresults. Since all these patients were negative prior tocertolizumab initiation we did not check the repeattitres of dsDNA. Previous studies examining antibodieswith drug-induced lupus (DIL) from anti-TNF therapy
6
5
4
3
2
1
0
No.
Pre-certolizumab Post-certolizumab
Lupus-like reactions
ANA +
6
4
2
1
Figure 1. Number of patients with anti-nuclear antibody(ANA) positivity and lupus-like symptoms pre-certolizumaband post-certolizumab induction. Before certolizumabinduction all 6 patients had a lupus-like reaction and 4 hadpositive ANA serologies. After switching to certolizumabonly one had persistent lupus-like symptoms and tworetained ANA positivity.
25
20
15
10
5
0Pre-certolizumab
Har
vey
Bra
dsha
w s
core
Post-certolizumab
Figure 2. Harvey Bradshaw index (HBI) score pre-certolizumab and post-certolizumab for each patient. Themean HBI scores pre-certolizumab and post-certolizumabwere 10.3 and 9.8, respectively, with no statistical difference(P = 0.73).
Journal of Digestive Diseases 2011; 12; 379–383 Certolizumab and lupus-like reactions 381
© 2011 The AuthorsJournal of Digestive Diseases © 2011 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated toShanghai Jiaotong University School of Medicine and Blackwell Publishing Asia Pty Ltd.

show concomitant elevations of ANA and anti-dsDNA antibody in 98–100% and 68–92% of cases,respectively.13–15 However, these results are skewedbecause the antibody profiles were related to the diag-nosis of drug-induced lupus. The incidence of DIL fromanti-TNF therapy is unknown but seems to beextremely rare, with rates of 0.18% in a large Frenchnational survey.15 Furthermore, anti-histone antibod-ies elevation is seen much less frequently in lupusfrom anti-TNF-a therapy with a reported rate of about57%.13
The primary focus of our study was ANA positivityand lupus-like symptoms after certolizumab induc-tion. While the mechanism of lupus-like symptomsand ANA development and resolution is unclear,anti-TNF-a therapy has clearly been shown to causethis reaction.16,17 Three main theories have been pro-posed for the causes of these reactions; (i) T-helper1 lymphocyte suppression from anti-TNF-a therapyleads to an increase in T-helper 2 lymphocytes withthe subsequent upregulation of B cells, includingthose producing autoreactive Abs; (ii) there is anincrease in bacterial infection with anti-TNF-atherapy leading to immune and lymphocyte activa-tion with auto-antibody formation; and (iii) anti-TNF-a treatment leads to the exposure of nuclearmaterial from apoptotic cells to the serum with sub-sequent auto-antibody formation, as these antigensare presented to lymphocytes.18–23 These are all plau-sible explanations and perhaps all these mechanismsplay some role in the auto-immunity of TNF inhibi-tors. However, the rates of ANA positivity with inflix-imab and adalimumab seem to be higher than withcertolizumab, although this reaction has been moreextensively studied in the former drugs.1,2,6,7,16,17
Furthermore, in vitro studies have demonstrated thatinfliximab and adalimumab induce apoptosis andcomplement or antibody-mediated killing of cellswith membrane-bound TNF-a, whereas certoli-zumab, because of its pegylated structure and lack ofa Fc region, does not have these effects.12,18,19,24,25 Thishas led to the proposal that the downregulation ofmonocyte cytokines including lipopolysaccharide-induced interleukin (IL)-1b, independent of thedestruction of TNF-expressing cells, is the mechanismby which biological therapy works in Crohn’s dis-ease.12 The combined data that certolizumab does notcause apoptosis, antibody or complement-mediatedkilling of cells and that the rates of ANA positivity arereportedly lower with this drug, suggest that the thirdproposed theory may be a large contributor to thisexplanation.
Our initial hypothesis was that because certolizumabcauses less destruction of cells via Fc-mediated killingand apoptosis there would be less nuclear materialreleased into the serum and thus, patients with lupus-like reactions or ANA positivity associated with inflix-imab and adalimumab may have relief from theirsymptoms and experience a reversal of ANA positivitywith certolizumab. Despite its limitations, our datalends support to this theory. A larger multi-center trialperformed prospectively with a larger panel of auto-antibodies drawn at fixed intervals could help toclarify and strengthen our findings. While futureinvestigation is warranted, patients who have arthral-gias or lupus-like reactions from infliximab of adali-mumab may benefit from switching to certolizumab.
REFERENCES
1 Targan SR, Hanauer SB, van Deventer SJ et al. A short-termstudy of chimeric monoclonal antibody cA2 to tumornecrosis factor alpha for Crohn’s disease. Crohn’s DiseasecA2 Study Group. N Engl J Med 1997; 337: 1029–35.
2 Hanauer SB, Feagan BG, Lichtenstein GR et al. Maintenanceinfliximab for Crohn’s disease: the ACCENT I randomisedtrial. Lancet 2002; 359: 1541–9.
3 Hanauer SB, Sandborn WJ, Rutgeerts P et al. Humananti-tumor necrosis factor monoclonal antibody(adalimumab) in Crohn’s disease: the CLASSIC-I trial.Gastroenterology 2006; 130: 323–33.
4 Sandborn WJ, Rutgeerts P, Enns R et al. Adalimumabinduction therapy for Crohn’s disease previously treatedwith infliximab: a randomized trial. Ann Intern Med 2007;146: 829–38.
5 Colombel JF, Sandborn WJ, Rutgeerts P et al. Adalimumabfor maintenance of clinical response and remission inpatients with Crohn’s disease: the CHARM trial.Gastroenterology 2007; 132: 52–65.
6 Sandborn WJ, Feagan BG, Stoinov S et al. Certolizumabpegol administered subcutaneously is effective and welltolerated in patients with active Crohn’s disease: resultsfrom a 26-week placebo-controlled phase III study.(PRECiSE1). Gastroenterology 2006; 130: A–107.
7 Sandborn WJ, Colombel JF, Panes J, Scholmerich J,McColm JA, Schreiber S. Higher remission and maintenanceof response rates with subcutaneous monthly certolizumabpegol in patients with recent-onset Crohn’s disease: datafrom PRECiSE 2. Am J Gastroenterol 2006; 101: S454–455.
8 Colombel J, Schreiber S, Hanauer SB et al. Long-termtolerability of subcutaneous certolizumab pegol inactive Crohn’s disease: results from PRECISE 3 and 4.Gastroenterology 2007; 132: A503.
9 Rutgeerts P, Sandborn W, Feagan B et al. Infliximab forinduction and maintenenace therapy for ulcerative colitis.N Engl J Med 2005; 353 (23): 2462.
10 D’Haens G, Baert F, van Assche G et al. Early combinedImmunosuppression or conventional management inpatients with newly diagnosed Crohn’s disease: an openrandomised trial. Lancet 2008; 371: 660–7.
11 Hommes D, Baert F, van Assche G et al. The idealmanagement of Crohn’s disease: top down versus step upstrategies, a randomized controlled trial. Gastroenterology2006; 130: A–108.
Journal of Digestive Diseases 2011; 12; 379–383382 HD Verma et al.
© 2011 The AuthorsJournal of Digestive Diseases © 2011 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to
Shanghai Jiaotong University School of Medicine and Blackwell Publishing Asia Pty Ltd.

12 Nesbitt A, Fossati G, Bergin M et al. Mechanism of action ofcertolizumab pegol (CDP870): in vitro comparison withother anti-tumor necrosis factor alpha agents. Inflamm BowelDis 2007;13: 1323–32.
13 Costa M, Said N, Zimmermann B. Drug-induced lupus dueto anti-tumor necrosis factor agents. Semin Arthritis Rheum2008; 37: 381–7.
14 Ramos-Casals M, Brito-Zeron P, Munoz S et al.Autoimmune diseases induced by TNF-targeted therapies:analysis of 233 cases. Medicine 2007; 86: 242–51.
15 De Bandt M, Sibilia J, Le Loet X et al. Systemic lupuserythematosus induced by anti-tumour necrosis factor alphatherapy: a French national survey. Club Rhumatismes etInflammation. Arthritis Res Ther 2005; 7: R545–51.
16 Bacquet-Deschryver H, Jouen F, Quillard M et al. Impact ofthree anti-TNF-alpha biologics on existing and emergentautoimmunity in rheumatoid arthritis andspondylarthropathy patients. J Clin Immunol 2008; 28:445–55.
17 Charles PJ, Smeenk RJ, De Jong J, Feldmann M, Maini RN.Assessment of antibodies to double-stranded DNA inducedin rheumatoid arthritis patients following treatment withinfliximab, a monoclonal antibody to tumor necrosisfactor alpha: findings in open-label and randomizedplacebo controlled trials. Arthritis Rheum 2000; 43:2383–90.
18 Lugering A, Schmidt M, Lugering N, Pauels HG,Domschke W, Kucharzik T. Infliximab induces apoptosisin monocytes from patients with chronic active Crohn’sdisease by using a caspase-dependent pathway.Gastroenterology 2001; 121: 1145–57.
19 Van den Brande JMH, Braat H, van den Brink GR et al.Infliximab but not etanercept induced apoptosis in laminapropria T-lymphocytes from patients with Crohn’s disease.Gastroenterology 2003; 124: 1774–85.
20 D’Auria F, Rovere-Qeurini P, Giazzon M et al. Accumulationof plasma nucleosomes upon treatment with anti-tumournecrosis factor-alpha antibodies. J Intern Med 2004; 255:409–18.
21 Via CS, Shustov A, Rus V, Lang T, Nguyen P, Finkelman FD.In vivo neutralization of TNF-alpha promotes humoralautoimmunity by preventing the induction of CTL. JImmunol 2001; 167: 6821–6.
22 Ferraccioli G, Mecchia F, Di Poi E, Fabris M. Anticardiolipinantibodies in rheumatoid patients treated with etanerceptor conventional combination therapy: direct and indirectevidence for a possible association with infections. AnnRheum Dis 2002; 61: 358–61.
23 Zheng L, Fisher G, Miller RE, Peschon J, Lynch DH,Leonard MJ. Induction of apoptosis in mature Tcells by tumour necrosis factor. Nature 1995; 377:348–51.
24 Fossati G, Nesbitt A. In vitro complement-dependentcytotoxicity and antibody-dependent cellular cytotoxicity bythe anti-TNF agents adalimumab, etanercept, infliximab,and certolizumab pegol (CDP870). Am J Gastroenterol 2005;100: S299.
25 Fossati G, Nesbitt AM. Effect of the anti-TNF agents,adalimumab, etanercept, infliximab, and certolizumabPEGOL (CDP870) on the induction of apoptosis inactivated peripheral blood lymphocytes and monocytes.[Abstract] Am J Gastroenterol 2005; 100: S298–S299.
Journal of Digestive Diseases 2011; 12; 379–383 Certolizumab and lupus-like reactions 383
© 2011 The AuthorsJournal of Digestive Diseases © 2011 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated toShanghai Jiaotong University School of Medicine and Blackwell Publishing Asia Pty Ltd.