Embed Size (px)
Citation preview

SURGICAL ONCOLOGY AND RECONSTRUCTION
Sur
Ch
Sur
Ch
Sur
Ch
Sur
Ch
dat
Anterior Tibial Artery Perforator Flap forReconstruction of Intraoral Defects
*Attend
yAttendgery, X
ina.
zAssocigery, X
ina.
xAssocigery, X
ina.
kAssocgery, X
ina.
This wo
ion of C
Rong-Lin Wang, MD,* Ning Li, DDS, MD,y Can-Hua Jiang, DDS, MD,zFeng Guo, DDS, MD,x and Tong Su, DDS, MDk
Purpose: The present clinical study assessed the feasibility of using an anterior tibial artery perforator
(ATAP) flap for the reconstruction of an intraoral defect after ablative surgery for oral cancer.
Patients and Methods: A cohort of consecutive patients with oral cancer requiring reconstruction of
an intraoral defect using an ATAP flap were enrolled after ablative surgery for oral cancer and ipsilateral
neck dissection.
Results: Twelve patients had primary oral squamous cell carcinoma (8 with tongue cancer and 4 with
buccal cancer). All patients received intraoral defect repair using an ATAP flap from the lower left leg.
The flapmeasured 7� 4 to 8� 6 cm2. Flap thickness was approximately 4.8 mm (3 to 6mm). Anastomosis
of all ATAP flaps was straightforward because of the long and high-caliber vessel pedicle. All flaps survivedand yielded excellent esthetic results for intraoral reconstruction. Nomajor complications occurred in any
patient.
Conclusion: The main advantages of the ATAP flap included the thin and pliable tissue characteristics
and a long and high-caliber pedicle. For small and medium-size intraoral defects, the ATAP flap is a reliable
alternative to the radial forearm free flap.
� 2014 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 72:804-810, 2014
To optimally reconstruct an intraoral soft tissue defect
by a free flap, the flap should be relatively thin and
pliable to provide the best replacement for the soft
and mobile oral mucosa.1,2 Moreover, its vessel
pedicle should be long enough with adequate
caliber for vascular anastomosis, because commonlythe recipient vessels (the facial artery or superior
thyroid artery as the recipient artery and the
external jugular vein or branches of the internal
jugular vein as the recipient vein) in the head and
ing Physician, Jinan Stomatology Hospital, Jinan, China.
ing Physician, Department of Oral and Maxillofacial
iangya Hospital, Central South University, Changsha,
ate Professor, Department of Oral and Maxillofacial
iangya Hospital, Central South University, Changsha,
ate Professor, Department of Oral and Maxillofacial
iangya Hospital, Central South University, Changsha,
iate Professor, Department of Oral and Maxillofacial
iangya Hospital, Central South University, Changsha,
rk was supported by the National Natural Sciences Foun-
hina (grant 81000445), the Foundation of theDepartment
804
neck have a large diameter and are distant from
intraoral defects.
Although the radial forearm (RF) free flap has the
thin and pliable characteristics and a long and high-
caliber pedicle, its harvesting leaves an unsightly and
conspicuous scar at the donor site and results insome potential complications in the upper limb
because of scarification of an important vessel of the
forearm.3-5 The anterolateral thigh (ALT) free flap, as
a 4-season flap, is unsuitable for obese patients owing
of Science & Technology of Hunan Province in China (grant
2010TD2023), and the State Key Specialist Construction Projects
of China.
Conflict of Interest Disclosures: None of the authors reported any
disclosures.
Address correspondence and reprint requests to Dr Li: Depart-
ment of Oral and Maxillofacial Surgery, Xiangya Hospital, Central
South University, No 87, Xiangya Road, Changsha, 410008, People’s
Republic of China; e-mail: [email protected]
Received June 27 2013
Accepted October 29 2013
� 2014 American Association of Oral and Maxillofacial Surgeons
0278-2391/13/01412-2$36.00/0
http://dx.doi.org/10.1016/j.joms.2013.10.025

WANG ET AL 805
to excessive subcutaneous fat in the thighs, which re-
quires a flap-thinning procedure to achieve good re-
sults.6-8 However, the thinning procedure requires a
high degree of technical skill and exact knowledge
of the vascular anatomy to avoid accidental
perforator injuries.9,10 Acceptance of a jejunal graft is
restricted by its vulnerable mucosa and possible
postoperative complications, including adhesion-induced ileus, abdominal wall dehiscence, peritonitis,
or hernias.11 Except for total tongue reconstruction,
the rectus abdominis musculocutaneous flap is not
preferred for intraoral reconstruction owing to its
bulky volume.12 The lateral upper arm free flap is al-
ways thin and pliable; however, the small vessel diam-
eter, short pedicle length, deep location of the pedicle,
and close relation to the radial nerve are major disad-vantages.13,14 Other free flaps proposed for intraoral
lining have their limitations. Therefore, there is no
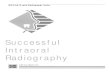
FIGURE 1. Anatomy of the ATAP flap and its surroundin
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillofac Sur
gold standard for the reconstruction of an intraoral
soft tissue defect by a free flap.
The choice of a free flap typemust bemade after tak-
ing into account the anatomic and functional charac-
teristics of the tissue removed, the recipient and
donor sites, the patient’s general condition, and the
experience of the surgeon. This report describes the
authors’ successful clinical application of a reliablefree flap, the anterior tibial artery perforator (ATAP)
free flap, with a long and high-caliber pedicle, for in-
traoral reconstruction. The ATAP flap results in an
inconspicuous scar and minimal functional conse-
quences to the donor site.
Patients and Methods
From July 2012 to March 2013, the free ATAP flapwas used to reconstruct intraoral soft tissue defects
g structures. ATAP, anterior tibial artery perforator.
g 2014.

806 ANTERIOR TIBIAL ARTERY PERFORATOR FLAP
in patients with oral cancer. Patients with varicosities
or restricted walking ability were excluded preopera-
tively. Then, anatomic variations of the 3 main arteries
in the lower legs of the remaining patients were
assessed further by computed tomographic angio-
graphic (CTA) examination. Patients with anterior
tibial artery (ATA) arteriosclerotic damage, a partly ste-
nosed ATA, or an entirely absent ATA were excluded.Color Doppler ultrasonography was used to predict
the location and pulse of a suitable perforator from
the ATA in the anterolateral lower leg in the remaining
patients. All patients had flaps raised in conjunction
with radical resection of the tumor, with safe margins
of at least 1.5 cm. This studywas approved by the Xian-
gya Hospital (Changsha, China) institutional review
board and all participants signed an informed consentagreement.
SURGICAL TECHNIQUE
Ablative resection of oral cancer and ipsilateral neck
dissection were completed under general anesthesia.
The size of the intraoral defect was assessed. The legfrom which the ATAP flap would be harvested was
bent at the knee joint. Themain septocutaneous perfo-
rators of the ATAP flap were identified near the
midpoint between the fibular head and the lateral mal-
leolus by preoperative Doppler. Then, a flap with the
required size was designed around the perforator
point and raised without a tourniquet to assess
the perforator. A dissection was initiated at the subfas-cial level from the posterior side of the designed
flap outline along the anterolateral direction and
continued to the perforator point. Then, the dissec-
tion was performed in the same way on the anterior
Table 1. DETAILS OF 12 PATIENTS TREATED WITH AN ANTER
Patient Age/Gender Lesion Flap Size (cm2)
1 34/male BC 8 � 5
2 47/male TC 8 � 5
3 45/male TC 7 � 5
4 39/female TC 7 � 5
5 58/male BC 8 � 6
6 49/male BC 7 � 4
7 50/male TC 8 � 4
8 33/male TC 8 � 4
9 36/male TC 9 � 5
10 54/female TC 8 � 5
11 32/male TC 8 � 4
12 61/male BC 7.5 � 4
Abbreviations: BC, buccal cancer; TC, tongue cancer.* Distance between fibular head and perforator.
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillofac Sur
side. When reaching the septocutaneous perforator,
the dissection proceeded deeply along the anterior in-
termuscular septum between the extensor digitorum
longus and tibialis anterior or peroneus longus
(Fig 1). After confirming the perforator as a branch
of the ATA, the perforator vessel was dissected
back to the ATA, leaving a small piece of fascia encir-
cling the perforator. Before harvesting the ATAP flap,ligation and dissection of the distal ATA were per-
formed in front of the origin point of the identified
perforator. Next, the ATA vessel was traced proximally
until a sufficient length was obtained. The vessel
pedicle was divided and the ATAP flap was harvested.
Manipulation was performed carefully to avoid injury
to the deep peroneal nerve. All flaps were anasto-
mosed to ipsilateral cervical vessels. In all cases, asplit-thickness skin graft was required for the
donor site.
Results
Initially, 3 patients with varicosities of the lower leg
were excluded from the 19 oral cancer cases. CTAassessment in the remaining 16 patients led to the sec-
ondary exclusion of 4 cases (1 for bilateral ATA steno-
sis and 3 for arteriosclerotic damage). The remaining
12 patients received preoperative Doppler examina-
tion, and the main perforators of the ATA in the antero-
lateral lower leg were identified. Clinical details of the
12 enrolled patients (10 men and 2 women; mean age,
44.8 yr) are presented in Table 1. The mean flap sizewas 36.4 cm2 (7� 4 to 8� 6 cm2). Themean thickness
of the flapwas 4.8mm (3 to 6mm). Anastomosis of the
ATAP flap was straightforward because of the high
caliber (artery, 2 to 3 mm; veins, 2 to 4.5 mm; data
IOR TIBIAL ARTERY PERFORATOR FLAP
Position of
Perforator (cm)*
Length of Vessel
Pedicle (cm)
Flap Thickness
(mm)
10.5 5.7 4
13. 6 5
12.7 6 6
16 4 5
15.1 7.5 4.5
14 9 5.5
13.5 8 6
16.5 10 5
14.4 7.5 4.5
14.3 6 4
15 6 5
12.4 8.5 3
g 2014.

FIGURE 4. An anterior tibial artery perforator flap with a 2-cmsegment of anterior tibial artery.
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillo-
fac Surg 2014.
FIGURE 2. A 45-year-old man with primary squamous cell carci-noma of the left tongue.
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillo-
fac Surg 2014.
WANG ET AL 807
not shown) and suitable length (maximum, 10 cm;
mean, 7.5 cm) of the vessel pedicle. All flaps sur-
vived. Patients could swallow a soft diet and speak
intelligibly at 10 days after surgery. All flaps yielded
excellent esthetic and functional results. All grafted
full-thickness skin in the lower leg healed well
without any functional complications at the donor
site.
REPORT OF CASES
Case 1 (Patient 3)
A 45-year-old man presented with T2N0M0 squa-
mous cell carcinoma (SCC) of the left tongue (Fig 2).
The patient underwent a radical excision, includingthe left side of the tongue, and ipsilateral modified
neck dissection. A 7-� 5-cm2 ATAP flap was harvested
(Fig 3) with a 6-cm vessel pedicle (including 2 cm of
the ATA; Fig 4) for the soft tissue defect of the tongue.
FIGURE 3. A 7- � 5-cm2 anterior tibial artery perforator flap washarvested.
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillo-
fac Surg 2014.
The artery of the ATAP flap was anastomosed to the su-
perior thyroid artery and the vein was anastomosed to
the external jugular vein. Full-thickness skin grafting
was performed at the donor site and healed well.
The reconstructed contour of the right tongue was
satisfactory at 10-month follow-up (Fig 5).
Case 2 (Patient 1)
The patient was a 34-year-old man with left buccal
mucosa SCC (Fig 6). After a radical excision, a 7- � 5-
cm2 soft tissue defect was left on the left buccal site.
An ATAP flap was harvested with a segment of the
ATA as its vessel pedicle (Fig 7). The artery of the
vessel pedicle was anastomosed to the superior thy-
roid artery and the vein was anastomosed to the inter-
nal jugular vein. Full-thickness skin grafting wasperformed at the donor site. After surgery, the flap
(Fig 8) and the donor site (Fig 9) healed well without
any major events.
FIGURE 5. The result of tongue reconstruction after 10 months.
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillo-
fac Surg 2014.

FIGURE 8. Intraoral view after repair.
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillo-
fac Surg 2014.
FIGURE 6. A 34-year-old man with left buccal mucosa squamouscell carcinoma.
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillo-
fac Surg 2014.
808 ANTERIOR TIBIAL ARTERY PERFORATOR FLAP
Discussion
Septocutaneous perforator flaps using the lower leg
as a donor site have been developed and applied for
FIGURE 7. An anterior tibial artery perforator flap with a segmentof anterior tibial artery was harvested.
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillo-
fac Surg 2014.
reconstructive surgery since the early 1980s.15 Perfo-
rators of lower leg flaps derive from 3 main vessels:
the ATA, the posterior tibial artery, and the peroneal ar-
tery.16 Carriquiry et al17 divided these septocutaneous
perforators of the lower leg into 3 groups: medial(from the posterior tibial vessels), anterolateral (from
the anterior tibial vessels), and posterolateral (from
FIGURE 9. The donor site healed well without any major events.
Wang et al. Anterior Tibial Artery Perforator Flap. J Oral Maxillo-
fac Surg 2014.

WANG ET AL 809
the peroneal vessels). Cormack and Lamberty18 found
that most ATA perforators course along the anterior
peroneal septum, between the extensor digitorum
longus and tibialis anterior or peroneus longus, in
the anterolateral area of lower leg. Based on anatomic
and color Doppler imaging data, Panagiotopoulos
et al19 considered that a series of ATA septocutaneous
perforators with large diameter were clustered in theproximal and intermediate segments of the lower leg
and penetrated the deep fascia to form an intercon-
necting network supplying the skin. However, there
was a relative lack of large perforators in the distal
segment of the lower leg. In the present study, the sep-
tocutaneous perforators in the intermediate segment
of the lower leg were chosen as the main perforators
of the ATAP flap, because the intermediate area ofthe anterolateral lower leg can provide a longer vessel
pedicle than the proximal area and ensure more perfo-
rators than the distal area.
Kim et al20 developed a free flap based on perfora-
tors originating from ATA branches to repair lower
leg defects. However, the short and low-caliber
(approximately 0.6 to 1.2 mm) vessel pedicle could
be unsuitable for vessel anastomosis in the head andneck. Although the ‘‘supermicrosurgery’’ technique
enables surgeons to successfully anastomose blood
vessels 0.5 to 0.8 mm in diameter, a sufficient learning
time and substantial skills are required for surgeons to
successfully anastomose such vessels.21 In the present
study, themethod ofKimet alwasmodified and a series
of ATAPflapswith a segment of ATAas its vessel pedicle
were harvested to reconstruct intraoral defects func-tionally and esthetically. Compared with other types
of free flap, the ATAP flap has distinct advantages,
including a thin and pliable skin paddle, a long and
high-caliber vessel pedicle, an inconspicuous and hid-
den scar at the donor site, a straightforward way for
flap raising, and the feasibility for 2-teamwork. Howev-
er, the donor site should be covered by a full-thickness
skin graft, which is more time consuming and causesscarring of the lower leg. Compared with the RF flap,
the donor-site scar of the ATAP flap is less conspicuous
because the lower leg scar can be covered by trousers.
However, the surgical procedure of harvesting anATAP
flap is not as straightforward as the harvesting of an RF
flap for a novice. Moreover, the sacrifice of ATA conti-
nuity remains a concern for surgeons and could result
in potential complications for the lower leg, such asvenous congestion, arterial insufficiency, and foot
drop.22 However, in the present cases, the authors
found the obvious repulse of the distal ATA residual
within 15 minutes after the segmental ATA had been
dissected. They considered that retrograde blood
flow from the posterior tibial artery might cause the
repulse of the distal ATA, which might decrease post-
operative complications of the lower limb. Moreover,
just like the ATAP flap, the peroneal artery perforator
flap has some similar advantages for intraoral repair;
however, exposure of the peroneal vessel is more diffi-
cult and demanding even when using the lateral
approach.23
In the present study, preoperative CTA was per-
formed to exclude patients with anatomic variations
of the 3 main vessels, especially the ATA. Althoughthe ATA is an important artery of the lower leg, it
can be too narrow, deficient to a greater or lesser
extent, or entirely wanting. Its function can be sup-
plied by perforating branches from the posterior tibial
or peroneal artery. In addition, Chiu et al24 considered
that preoperative CTA could be used to map the perfo-
rator accurately and evaluate the dominant vascularity
before transferring ALT flaps. However, the authors ofthe present study did not identify the exact course of
the perforator of the ATAP flap in the lower leg using
CTA. High-resolution CTA or magnetic resonance angi-
ography might help visualize the ATA perforators,
which needs further confirmation. Although preoper-
ative Doppler examination can help predict the loca-
tion and pulse of a septocutaneous perforator,
especially those with large diameter, operator depen-dence and false positive detection are its main disad-
vantages.25 Therefore, their intraoperative presence
is most important for proper selection.
In conclusion, the authors believe the ATAP flap can
be used to reconstruct intraoral soft tissue defects
functionally and esthetically and is a reliable alterna-
tive to the RF flap for small and medium-size defects
in the head and neck.
References
1. Eckardt A, Fokas K: Microsurgical reconstruction in the headand neck region: An 18-year experience with 500 consecutivecases. J Craniomaxillofac Surg 31:197, 2003
2. Amarante J, Reis J, Costa-Ferreira A, et al: Head and neckreconstruction: A review of 117 cases. Eur J Plast Surg 23:404, 2000
3. Heller F, Wei W, Wei FC: Chronic artery insufficiency of the handwith fingertip necrosis one year after harvesting a radial forearmfree flap. Plast Reconstr Surg 114:728, 2004
4. Yang GF, Chen PJ, Gao YZ, et al: Forearm free skin flap transplan-tation: A report of 56 cases. Br J Plast Surg 50:162, 1981
5. Huang CH, Chen HC, Huang YL, et al: Comparison of the radialforearm flap and the thinned anterolateral thigh cutaneous flapfor reconstruction of tongue defects: An evaluation of donor-sitemorbidity. Plast Reconstr Surg 114:1704, 2004
6. Park CW, Miles BA: The expanding role of the anterolateral thighfree flap in head and neck reconstruction. Curr Opin Otolar-yngol Head Neck Surg 19:263, 2011
7. Huang JJ, Wallace C, Lin JY, et al: Two small flaps from one ante-rolateral thigh donor site for bilateral buccal mucosa reconstruc-tion after release of submucous fibrosis and/or contracture.J Plast Reconstr Aesthet Surg 63:440, 2010
8. Kimura N, Satoh K, Hasumi T, et al: Clinical application of thefree thin anterolateral thigh flap in 31 consecutive patients. PlastReconstr Surg 108:1197, 2001
9. Wei FC, Jain V, Celik N, et al: Have we found an ideal soft-tissueflap? An experience with 672 anterolateral thigh flaps. Plast Re-constr Surg 109:2219, 2002

810 ANTERIOR TIBIAL ARTERY PERFORATOR FLAP
10. Kimura N, Satoh K: Consideration of a thin flap as an entity andclinical applications of the thin anterolateral thigh flap. Plast Re-constr Surg 97:985, 1996
11. Gluckmann JL, McDonough J, McCafferty GJ, et al: Complica-tions associated with free jejunal graft reconstruction of thepharyngoesophagus—A multiinstitutional experience with 52cases. Head Neck Surg 7:200, 1985
12. Koshima I, Soeda S: Inferior epigastric artery skin flap withoutrectus abdominis muscle. Br J Plast Surg 42:645, 1989
13. Gehrking E, Remmert S, Majocco A: Topographic and anatomicstudy of lateral upper arm transplants. Anat Anz 180:275, 1998
14. Matloub HS, Larson DL, Kuhn JC, et al: Lateral arm free flap inoral cavity reconstruction: A functional evaluation. Head Neck11:205, 1989
15. Ponten B: The fasciocutaneous flap: Its use in soft tissue defectsof the lower leg. Br J Plast Surg 34:215, 1981
16. Haertsch PA: The blood supply of the skin of the leg: A post mor-tem investigation. Br J Plast Surg 34:470, 1981
17. Carriquiry C, Costa A, Vasconez LO: An anatomic study of the sep-tocutaneous vessels of the leg. Plast Reconstr Surg 76:354, 1985
18. Cormack GC, Lamberty BG: The Arterial Anatomy of Skin Flaps(ed 2). New York, NY, Churchill Livingstone, 1994, p 252
19. Panagiotopoulos K, Soucacos PN, Korres DS, et al: Anatomicalstudy and colour Doppler assessment of the skin perforatorsof the anterior tibial artery and possible clinical applications. JPlast Reconstr Aesthet Surg 62:1524, 2009
20. Kim NG, Lee KS, Choi TH, et al: Aesthetic reconstruction oflower leg defects using a new anterolateral lower leg perforatorflap. J Plast Reconstr Aesthet Surg 61:934, 2008
21. Koshima I, Nanba Y, Tsutsui T, et al: Medial plantar perforatorflaps with supermicrosurgery. Clin Plast Surg 30:447, 2003
22. Dong JS, Peng YP, Zhang YX, et al: Reverse anterior tibial arteryflap for reconstruction of foot donor site. Plast Reconstr Surg112:1604, 2003
23. Klaus DW, Florian B, Jennifer W, et al: Peroneal perforator flapfor intraoral reconstruction. Br J Oral Maxillofac Surg 50:25,2012
24. Chiu WK, Lin WC, Chen SY, et al: Computed tomography angi-ography imaging for the chimeric anterolateral thigh flap inreconstruction of full thickness buccal defect. ANZ J Surg 81:142, 2011
25. Rozen WM, Ashton MW, Pan WR, et al: Anatomical variations inthe harvest of anterolateral thigh flap perforators: A cadavericand clinical study. Microsurgery 29:16, 2009