Embed Size (px)
Citation preview

Anterior Non-granulomatous Uveitis:Differential Diagnosis
Marina Papadia, Naoual Jennane, and Carl P. Herbort
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Characteristics of Non-granulomatous Versus
Granulomatous Uveitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Differential Diagnosis of Non-granulomatous Anterior
Uveitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Case 1: HLA-B27 Uveitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Case 2: Uveitis Associated with Juvenile IdiopathicArthritis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Case 3: Uveitis Mistakenly Described as Non-granulomatous with Very DeleteriousConsequences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Case 4: Uveitis Related to a Streptococcal Infection/Para-infectious Uveitis . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Further Comments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Suggested Reading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
M. Papadia (*)Department of Ophthalmology, Ospedale Antero Micone,Genoa, Italy
Retinal and Inflammatory Eye Diseases, Centre forOphthalmic Specialized Care (COS), Teaching CentreClinic Montchoisi, Lausanne, Switzerlande-mail: [email protected]
N. JennaneRetinal and Inflammatory Eye Diseases, Centre forOphthalmic Specialized Care (COS), Teaching CentreClinic Montchoisi, Lausanne, Switzerland
Private Practice, Rabat, Moroccoe-mail: [email protected]
C.P. HerbortRetinal and Inflammatory Eye Diseases, Centre forOphthalmic Specialized Care (COS), Teaching CentreClinic Montchoisi, Lausanne, Switzerland
University of Lausanne, Lausanne, Switzerlande-mail: [email protected]; [email protected]
# Springer India 2016V. Gupta et al. (eds.), The Uveitis Atlas,DOI 10.1007/978-81-322-2506-5_12-1
1

Introduction
The anatomical classification of uveitis into ante-rior, intermediate, and posterior forms is veryuseful to conduct the work-up and eventually toreach a diagnosis, even though inflammation doesnot always respect these anatomical boundaries.Anterior uveitis is the term used for the group ofinflammatory disorders for which the preponder-ant part of the inflammation is situated at the levelof the pars plicata of the ciliary body, the retro-iridal space, the iris, and the anterior chamber.
The anatomical diagnosis of anterior uveitisshould first be verified by excluding spilloverinflammation associated with uveitis of the poste-rior segment (intermediate or posterior uveitis).To exclude posterior involvement, pupil dilatationis mandatory in all cases. Secondly, the type ofclinical presentation has to be characterized asnon-granulomatous or granulomatous in order tocorrectly orient work-up and differentialdiagnosis.
Characteristics of Non-granulomatousVersus Granulomatous Uveitis
Non-granulomatous uveitis is characterizedmainly by the type of keratic precipitates (KPs)that present as fine KPs producing endothelialdusting. In severe cases fibrinous clotting orhypopyon can occur depending on whether pro-tein influx or cellular infiltration is predominant(Figs. 1, 2, and 3). In case of severe inflammation,it is also common to find posterior synechiae, andpressure tends to be more often decreased thanincreased (Fig. 2).
In contrast, granulomatous uveitis is character-ized by KPs that are larger than the dusty KPs ofnon-granulomatous uveitis. These KPs are betterindividualized but their size varies depending onthe inflammatory process. The medium- andlarge-size granulomatous KPs are called mutton-fat KPs. Other characteristic features of granulo-matous uveitis are Koeppe and Busacca nodulesmade of inflammatory cells at the pupillary mar-gin (Koeppe) or within the iris stroma (Busacca).
Synechiae are common in more pronouncedinflammation. Pressure changes when present areusually characterized by increased intraocularpressure. In this context it is important to insiston the fact that Fuchs’ uveitis is a granulomatousuveitis unlike what is written in several textbooks.Fuchs KPs are structured, usually in a stellatefashion; they can be easily individualized andare larger than just dust (Fig. 4). The presence ofKoeppe nodules in a substantial number of casesis further confirming the granulomatous characterof Fuchs’ uveitis. The term of granulomatous
Fig. 1 Fibrinous clot in the anterior chamber in typicalcase of HLA-B27-related uveitis
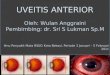
Fig. 2 Posterior irido-lenticular synechiae. The ring ofpigment deposits on the crystalline lens shows where theiris was attached (synechiae). There is one remainingsynechia at 6 o’clock on the verge of detaching itselffollowing the administration of massive dilating drops.The presence of pigment deposits on crystalline lens isuseful to confirm previous episodes of anterior uveitis
2 M. Papadia et al.

uveitis is in fact a misnomer because a histopath-ologic term is used to describe clinical conditionsbased on certain clinical features including spe-cific KPs and iris nodules, among other clinicalsigns. Originally the clinical term of granulomatousuveitis was still based on the histopathologic pres-ence of granulomatous lesions which today is nomore always the case. It has become a clinicalcategory, a clinical terminology for which in somecases an underlying granulomatous histopathologycan be found such as in sarcoidosis and tuberculo-sis, but this clinical terminology has extended toother conditions where the underlying histopathol-ogy is not granulomatous such as in Fuchs’ uveitisor birdshot retinochoroiditis or not always granulo-matous such as in Vogt-Koyanagi-Harada disease.
Although this clinical distinction betweengranulomatous and non-granulomatous is a veryuseful classification, the subdivision is not anabsolute one. A granulomatous uveitis may ini-tially present as non-granulomatous before takingits granulomatous aspect. On the other hand, when
dusty KPs are very numerous and thick, they maybe mistaken as granulomatous (Table 1).
Symptoms and Signs of Non-granulomatous Anterior UveitisThe severity of symptoms in anterior uveitisranges from no symptoms in chronic diseasesuch as anterior uveitis related to juvenile idio-pathic arthritis (JIA) to very severe symptoms inacute uveitis such as HLA-B27-related uveitis.Symptoms of acute anterior uveitis include pho-tophobia, redness, pain, decreased vision, andtearing in the absence of discharge.
Fig. 3 Hypopyon. Sedimented white cells form a level atthe bottom of the anterior chamber, associated with a ringof fibrin on the surface of the crystalline lens (top) indicat-ing broken synechiae. One remaining synechia on themeridian of 7 o’clock
Table 1 Common causes of non-granulomatousuveitis
HLA-B27-related uveitis and HLA-B27-associateddiseases
Behçet’s uveitis
Uveitis associated with juvenile idiopathic arthritis
Uveitis associated with scleritis
Uveitis associated with streptococcal infection
Uveitis associated with tubulointerstitial nephritis anduveitis (TINU)
Rare entity psoriatic uveitis (Tanaka et al. 2015),relapsing polychondritis uveitis
Fig. 4 Stellate KPs, typical of Fuchs’ uveitis
Anterior Non-granulomatous Uveitis: Differential Diagnosis 3

The Signs of Anterior Non-granulomatousUveitis (Listed in Table 2)
1. Conjunctival injection in anterior uveitis canbe diffuse or localized circumferentially at thelimbus (perikeratic injection) or mixed (diffuseand perikeratic injection).
2. Keratic precipitates (KPs) are small and dif-fuse causing dusting of the endothelium. IfKPs are larger than dust and can easily beindividualized, even if they are small, theyshould be considered as granulomatous suchas in Fuchs’ uveitis presenting micro-granulomatous stellate KPs.
3. Anterior chamber flare is caused by exudationof proteins into the normally clear aqueoushumor from iris vessels or across the ciliarybody epithelium following the breakdown ofthe blood-aqueous barrier. The intensity offlare is measured in a standard fashion follow-ing the grading system proposed by the ProctorGroup in San Francisco in 1959 (Table 3). Thisgrading system is however only qualitative.When the concentration of proteins in theaqueous is very high, they agglomerate andform fibrinous clots, a finding more commonin acute non-granulomatous uveitis (Fig. 1).
4. Posterior synechiae: Depending on the amountand composition of aqueous inflammatory pro-teins, adherences between the iris and anteriorcapsule of the crystalline lens can form (poste-rior synechiae) (Figs. 1–3).
Since a few years, it is now possible tomeasure flare in a quantitative and objectivefashion, using laser flare photometry (LFP)(Fig. 5). This new technology makes flare theonly quantitative parameter to measure intra-ocular inflammation. So far cells were esti-mated to be more accurate to measureinflammatory activity in uveitis. At best thismeasurement is however only semiquantita-tive. LFP was shown to be more sensitivethan slit-lamp assessment of cells to measurethe evolution of inflammatory activity, makingflare the new gold standard to assess intraocu-lar inflammation. LFP allows to detect subclin-ical flare intensities and changes that can bepredictive of clinical recurrence. A closerfollow-up of therapy is so possible, leading toincrease of treatment in case of resistance totherapy but often also leading to corticosteroidsparing in case of lowered and stabilized LFPvalues. When available, laser flare photometrycertainly allows improved management of uve-itis and should be acknowledged as such.
5. Aqueous cells used to be the reference parameterfor inflammatory activity because their evalua-tion was somewhat quantifiable by slit-lampexamination. Nowadays this is no longer true,when LFP is available. LFP is now the quantifi-able gold standard to measure inflammatoryactivity even in chronic inflammation withchronic breakdown of the hemato-ocular bar-riers; LFP can detect active inflammation thatresponds to therapy. The notion that cells are nolonger the hallmark of activity will take time tobe acknowledged as, unfortunately, LFP is stillnot used universally in uveitis centers. Until thentextbooks will continue to present cells as thesign of activity. Grading of cells in the anteriorchamber has been standardized by Hoganet al. at the Proctor Foundation in 1959 (Table 4).
It is important to make the differencebetween pigment clumps and inflammatorycells and to examine the anterior chamber
Table 2 Signs of anterior uveitis
1.1. Conjunctival and perikeratic injection
1.2. Keratic precipitates (dust)
1.3. Aqueous flare/fibrinous clots (Fig. 1)
1.4. Posterior synechiae between the iris and the capsuleof the lens (Fig. 2)
1.5. Aqueous cells/hypopyon (Fig. 3)
1.6. Iris rubeosis
1.7. Intraocular pressure changes (hypotony in severeacute anterior non-granulomatous uveitis)
Table 3 Slit-lamp grading of aqueous flare (1 mm �3 mm beam)
No flare 0
Faint, just detectable +
Moderate, iris details clear ++
Marked, iris details hazy +++
Intense, fibrin ++++
4 M. Papadia et al.

prior to mydriasis as cells and especially pig-ment dispersion can sometimes be seen afterpupillary dilatation.
When the quantity of cells is very dense,they sediment and cause a hypopyon, a signmore often seen in HLA-B27-related uveitis,Behçet’s uveitis, and uveitis related to juvenileidiopathic arthritis (JIA) (Fig. 3).
6. In severe and long-standing uveitis, irisrubeosis can develop. It is in fact most often apseudo-rubeosis that is reversible after intro-duction of anti-inflammatory treatment. Evenwhen a real rubeosis has developed, it is usu-ally situated at the pupillary border of the irisand is much less aggressive and proliferativethan ischemic rubeosis iridis.
7. Intraocular pressure changes due to uveitiscan present either as hypotension or hyperten-sion. Hypotony is usually measured in severeuveitis involving the ciliary body such as acute
anterior non-granulomatous HLA-B27-relateduveitis, hypertony being usually associatedwith granulomatous uveitis, especially herpessimplex or herpes zoster uveitis, where atrabeculitis is associated.
Differential Diagnosis of Non-granulomatous Anterior Uveitis
1. In case of simple, fibrinous, or hypopyonnon-granulomatous unilateral uveitis, the onlyfirst-line work-up test we presently perform isthe detection of the HLA-B27 antigen.HLA-B27 testing is performed even if theinflammation is only moderate. If the test ispositive, it will avoid further unnecessary testingduring a subsequent episode, and it is reassuringfor the patient and the doctor to know the specificdiagnosis, especially when it is a benign disease.In case of a positive result, no further investiga-tion is performed at the ophthalmological level. Itis however recommended to take an orientedhistory that will allow, with the help of the inter-nist or rheumatologist when necessary, to sub-classify the affection into ankylosingspondyloarthritis, Reiter’s syndrome, Crohn’sdisease, ulcerative colitis, or simply HLA-B27uveitis without systemic associated disease.
PMTAmplifier
Counter
Interface
Controller
He-Ne laserOptical scanner
Computer
Fig. 5 Laser flare photometry
Table 4 Slit-lamp grading of aqueous cells (1 mm �3–4 mm beam)
No cells 0
1–5 cells �6–10 cells +
11–20 cells ++
21–50 cells +++
>50 cells ++++
Anterior Non-granulomatous Uveitis: Differential Diagnosis 5

About 50–55 % of acute anterior non-granulo-matous uveitides are HLA-B27 positive inEurope. In different parts of the world, B27positivity varies from one geographical area toanother, being, for instance, quite low in Japan.In the remaining 45–50 % of cases, a specificdiagnosis is more difficult to establish.
If the episode of B27-negative non-granu-lomatous uveitis is of limited severity and/orresponds readily to classical topical corticoste-roid therapy, no other investigation than to searchfor the HLA-B27 antigen is performed.
2. In case of an anterior uveitis with hypopyon(Fig. 6), signs and symptoms found in Behçet’ssyndrome should be searched for, in particularoral and/or genital ulcerations (Fig. 7), cutaneoussigns such as erythema nodosum and pustules,arthralgias, thrombophlebitis, and cardiovascu-lar, pulmonary, gastrointestinal, or central
nervous system involvement. If Behçet’s uveitisis suspected, we find it useful to look for theHLA-B51 antigen that, when present, representsan additional argument for the diagnosis ofBehçet’s uveitis (but is not diagnostic), especiallyin themilder forms of Behçet’s uveitis seen in theEuropean Caucasian population. Isolated ante-rior Behçet’s uveitis can occur, but posteriorinvolvement should be searched for byfundoscopy and is best investigated byperforming a fluorescein angiography lookingfor retinal vasculitis (Fig. 8) (Table 5).
3. In case of non-granulomatous uveitis in chil-dren (with or without band keratopathy), his-tory should be directed toward juvenileidiopathic arthritis (JIA). Inflammatory symp-toms can be completely absent, contrastingwith the severe signs of uveitis such ashypopyon and synechiae that can occur in awhite externally non-inflamed eye, features ofJIA-related uveitis (Fig. 9). Uveitis is usuallyassociated with the oligoarticular form of JIA,and testing should include antinuclear anti-bodies (ANA) that are present in up to 70 %of JIA patients with uveitis (Jones NP, anillustrative manual). In elderly children it isalso useful to test for the presence of HLA-B27antigen.
Fig. 6 Hypopyon uveitis in a patient who complained oralaphthae whose final diagnosis was Behçet’s uveitis
Fig. 7 Aphthae on the tongue of patient with hypopyonanterior uveitis
Fig. 8 Same patient as in Figs. 6 and 7; one zone ofperipheral retinal vasculitis in this patient with hypopyonuveitis and oral aphthae makes the diagnosis of Behçet’suveitis most probable
6 M. Papadia et al.

A bilateral non-granulomatous uveitis in children,but also in adults, should prompt to search orexclude tubulointerstitial nephritis and uveitis(TINU) syndrome, an often neglected diagnosis.Renal function should be tested, starting with thedosage of creatininemia requiring sometimes renalbiopsy, and urinalysis should be performed lookingfor glucosuria and dosage of beta-2-microglobulinwhich is found to be elevated in the urine in TINU.
In children pars planitis can initially presentwith an anterior participation and can be mistakenfor an anterior uveitis if the posterior segment isnot carefully examined.
In case of non-responding HLA-B27-negativeanterior uveitis or in case of recurrence, we pursuethe work-up in the same fashion as for a granulo-matous uveitis.
Case 1: HLA-B27 Uveitis
Case 1a. A 33-year-old man consulted for a redpainful right eye since 2 days. He said that he hadhad previous episodes sometimes in the right andsometimes in the left eye but never in both eyes atthe same time. Visual acuity was conserved anduncorrected VA in both eyes was 1.0. At the slitlamp, there were fine KPs not exceeding dust onthe endothelial surface predominant inferiorly. Inthe anterior chamber, there was a 3 to 4+ flare andfibrin with posterior irido-lenticular synechiae onnearly 360º. Laser flare photometry was increasedto 433 ph/ms in the right eye and was normal(3.8 ph/ms) in the left eye. Aqueous cellsamounted to 2+. Pressure was reduced to5 mmHg on the right, while the left contralateraleye had a normal pressure of 12 mmHg. Treat-ment was started immediately applying predniso-lone acetate 1 % drops every 10 min, alternatingwith a dilating cocktail containing 2.5 % phenyl-ephrine, 0.5 % tropicamide, and 0.25 % scopol-amine. The synechiae were broken after 2 h(Fig. 10), and the patient was dismissed with thetreatment including hourly 1 % prednisolone ace-tate drops and prednisolone 0.5 % ointment atnight, as well as tropicamide 0.5 % ten times per
Table 5 Flowchart: diagnostic steps in anteriornon-granulomatous uveitis
Fig. 9 Hypopyon in a non-inflamed eye in a patient withJIA-associated uveitis
Fig. 10 Fibrinous clot and ring on crystalline lens,sequelae of posterior synechiae
Anterior Non-granulomatous Uveitis: Differential Diagnosis 7

day. When the patient came back on the followingmorning, slit-lamp flare and cells were estimatedat 2+. LFP values decreased to 98.7 ph/ms, show-ing that the treatment was efficient. After 1 dayLFP values went down to 25.8 ph/ms and to 14.3after 2 days (Fig. 11). Dilatation was stopped onthe second follow-up day, as synechiae usually donot develop with LFP values under the value of30 ph/ms. Prednisolone drops were tapered andfinally stopped after 16 days with nearly normalLFP values of 6.1 ph/ms indicating good recoveryof blood-ocular barrier (BOB) HLA-B27 antigen,never tested before, was searched and came backpositive.
Case 1b. A second patient consulted our emer-gency ward with the same type of presentation. Hewas seen for a left red eye and presented anterior
chamber cells (2+), slit-lamp flare (3+), and fibrin,synechiae, and hypotony (Fig. 12). Laser flare pho-tometry values were very elevated up to 298.7 ph/ms The same therapy as in the first patient wasapplied, and the inflammation seemed to improveat the slit lamp showing release of synechiae but theeye was still painful after 2 days. After 12, 24, and48 h, the LFP values remained high around 295 ph/ms and even increased to 309 ph/ms at 48 h indi-cating resistance to the classic topical treatmentapplied for acute anterior HLA-B27 uveitis(Fig. 11). It was then decided to perform an orbitalfloor injection of aqueous betamethasone 4 mg(Celestone®). Twelve hours after the periocularinjection, LFP value decreased to 14.8 ph/ms(Fig. 11), and all topical treatment could be stoppedafter 19 days with an LFP value of 8.1 ph/msshowing a slight residual BOB, in accordancewith standard evolution of HLA-B27-relatedacute anterior uveitis (Fig. 13).
These two typical HLA-B27 uveitis cases opti-mally benefit from LFP. Without LFP it is notpossible to follow flare changes in such highflare situations; it would have been impossible todetect that case 2 was resistant to standard topicaltherapy. In such cases it is necessary to give addi-tional orbital corticosteroid injections. It wasshown that in nine resistant cases, periocularaqueous corticosteroid injection led to a 50 %flare reduction after only 12 h (Herbortet al. 1997) (Fig. 14). On the other hand, in low
Fig. 11 Laser flarephotometry
Fig. 12 HLA-B27 uveitis corresponding to the second
8 M. Papadia et al.

flare situations, at the end of an episode, it wouldnot be possible to determine the end of dilatationwhen LFP reaches values below 40 ph/ms, a valueunder which synechiae formation is improbable.
Case 2: Uveitis Associatedwith Juvenile Idiopathic Arthritis
An 8-year-old patient came to see us for secondopinion. She had presented uveitis and an initialattack of juvenile idiopathic arthritis of theoligoarticular at 2 years of age. At age 7 a bilateral
cataract operation with intraocular lens implanta-tion was performed. We saw the patient 1 year aftercataract surgery with a vision reduced tofingercounting on the right and 3/60 on the left, andthe patient was already registered in a special schoolfor visually impaired persons. Slit-lamp examinationshowed complete pre- and retro-IOL opacificationand band keratopathy on both sides (Figs. 15 and16). The patient was merely under topical treatment,receiving one single daily drop of prednisolone ace-tate 1 %.Thisminimalistic treatmentwas justified bythe fact that there were no aqueous cells; hence therewas no active inflammation. Slit-lamp examination
Fig. 13 Graph indicatingmean evolution curve ofHLA-B27 uveitis treated ina standard fashion
Fig. 14 Graph showingmean evolution after oneorbital floor injection ofwater-solublebetamethasone of a group ofHLA-B27 uveitis resistantto classic topical therapy.There is a 50 % flarereduction 12 h only after theperiocular injection
Anterior Non-granulomatous Uveitis: Differential Diagnosis 9

of the anterior segment showed no cells but a 3+ flareODS. The posterior segment was barely visible butno major lesions could be seen, and OCT showedthat there was no major loss of architecture of themacular retina. Visual fields showed a nearly totalloss of mean sensitivity ODS (Fig. 17). Laser flarephotometry (LFP) values were very elevated up to435 ph/ms on the right and 292 ph/ms on the left.Intraocular pressure (IOP) was 6 mmHg on the rightand 11 mmHg on the left, and phthisis bulbi wasfeared OD.
Massive inflammation-suppressive treatment(IST) was started including dexamethasone0.1 % drops and nonsteroidal drops six times
daily, prednisone 1.7 mg/kg with subsequentslow tapering, and azathioprine 2.5 mg/kg. After1 month, visual acuity (VA) improved fromfingercounting to 0.1 OD and from 3/60 to 0.15OS. LFP values decreased to 261 ph/ms OD and124 ph/ms OS. Band keratopathy was removedusing EDTA 2 % drops together with milling andscratching of calcium deposits. YAG lasercapsulotomies were performed ODS. After6 months BCVA improved to 0.2 OD and 0.6OS (Figs. 18 and 19). LFP values decreased to226 OD and 99.6 OS. Intraocular pressure stabi-lized around 9–10 mmHg OU. After 24 monthsBCVA increased to 0.7 OD and 0.8 OS. Visualfield improved substantially on both sides(Fig. 17). After 11 years under several ISTs,including immunosuppressants such asmycophenolic acid and cyclosporine as well asbiologics such as infliximab and adalimumab,the situation stabilized in this patient that finallycould follow a normal school and was employedas a medical assistant. BCVAwas 0.2 OD and 0.8OS. LFP values stabilized at 95.3 ph/ms OD and39.7 ph/ms OS with IOP values of 7 mmHg ODand 12 mmHg OS.
This case shows that the axiom “no aqueouscells means no active inflammation” has to berevised especially in non-granulomatous uveitis. Itis shown here that very high LFP values do notnecessarily mean irreversible BOB breakdown. Asubstantial proportion of BOB in chronic
Fig. 15 (a) Bandkeratopathy. (b) Bandkeratopathy
Fig. 16 Opacification in the pupillary through pre- andretro-IOL opacification
10 M. Papadia et al.

inflammation corresponds to active inflammationeven though there are no inflammatory cells presentand maximal IST has to be applied to determine
which part of BOB can be reversed and whichproportion is truly irreversible BOB. Improvementof LFP values clearly here had a tremendousimpact on visual function. Obviously close moni-toring of the level of BOB and evolution of aque-ous flare can only be performedwith LFP, today theonly quantitative and precise modality to exactlymeasure the level of intraocular inflammation.
Case 3: Uveitis Mistakenly Describedas Non-granulomatous with VeryDeleterious Consequences
A 19-year-old lady complained of headaches withslightly fuzzy vision. She consulted her eye doc-tor, who described bilateral non-granulomatous
Fig. 17 Visual fields
Fig. 18 Cleared media after band keratopathy removaland YAG laser capsulotomy
Anterior Non-granulomatous Uveitis: Differential Diagnosis 11

uveitis with fine KPs, vitritis, and hothyperfluorescent disks. The best corrected visualacuity was 0.9 ODS. The ophthalmologist sent thepatient for internal medicine work-up where sherevealed to the internist that she presents oralaphthae four to five times a year. The search forHLA-B51 was positive and the diagnosis ofBehçet’s uveitis is made. The patient was treatedwith systemic corticosteroids with an initial dosageof 60 mg of prednisone tapered down to 10 mg after8months. In addition the patient was given 15mg ofmethotrexate orally once a week that subsequentlyhad to be stopped because of suspected liver toxic-ity.We saw the patient 3 years later when the patienthad put 8 kg of weight.
BCVAwas still 0.9 ODS. On the endotheliumon both sides, very fine however well-identifiablestellate KPs could be seen (Fig. 20). Laser flarephotometry values were 9.7 ph/ms OD and10.3 ph/ms OS. The brown iris showed a slightdegree of atrophy (Fig. 20). There were 1–2+ cellsin the anterior vitreous. On the right there wassmall posterior subcapsular cataract (Fig. 20).The patient brought with her the fluorescein angi-ographies performed elsewhere that showed bilat-eral disk hyperfluorescence without significantvasculitis (Fig. 21) that is classically seen inFuchs’ uveitis, which obviously was the diagnosisin this patient. Treatment was discontinued afterwhich the situation remained stable. Such a
misdiagnosis would never have happened if theKPs would have been interpreted as granuloma-tous, a definition which applies to all KPs that aremore than dust, that can be individualized. Suchgranulomatous KPs are an absolute exclusion cri-terion of Behçet’s uveitis.
Case 4: Uveitis Relatedto a Streptococcal Infection/Para-infectious Uveitis
A 9-year-old girl complained of pain in her righteye especially at night with a slightly decreasedvision. She had been treated with penicillin sinceseveral days for an angina. Visual acuity was 0.9OD and 1.0 OS. Slit-lamp examination showed a2–3+ flare and a 1+ cell in the right anteriorchamber, while the left eye looked uninflamed.Intraocular pressure was 6 mmHg OD and10 mmHg OS. There were very few vitreouscells to be seen in the anterior vitreous. Laserflare photometry values were elevated to 176 ph/msOD and slightly elevated to 15.7 ph/ms. Fundusexamination showed a prominent papillitis OD,while the disk was slightly hyperemic at most OS(Fig. 22). Visual fields were normal. Blood labo-ratory tests showed an elevated sedimentation rate(35/h) and an elevated c-reactive protein(CRP = 24, normal value < 5), and
Fig. 19 Evolution of LFPversus visual acuity in thiscase of severe JIA-relateduveitis
12 M. Papadia et al.

antistreptolysins were elevated and over 500 (nor-mal value < 200). Treatment consisted of sys-temic prednisone (20 mg per day, tapered over3 months) and topical prednisolone acetate 1 %five times daily ODS, tapered down to zero over aperiod of 5 months. After 5 months LFP valueswere down to 7.0 ph/ms OD (slight persistentBOB) and to 3.6 ph/ms (normal value). Thepapillitis decreased progressively with an almostnormal aspect after 5 months (Fig. 22).
Further Comments
Classification of anterior uveitis into granuloma-tous and non-granulomatous is extremely usefulas it allows to orient the clinician in establishinghis diagnosis, as long as the criteria distinguishingthe two groups are well understood. Indeed somespecific entities can be excluded categoricallythanks to this differentiation. For instance, thepresence of micro-granulomatous KPs as seen in
Fig. 20 Case of bilateral Fuchs’ uveitis that was classifiedas non-granulomatous leading to misdiagnosis as Behçet’suveitis. Micro-granulomatous KPs can be seen in both
eyes, as well as a posterior subcapsular cataract (middlepicture). It has to be noted that Fuchs’ uveitis can bebilateral in about 10 % of cases
Fig. 21 Case of bilateral Fuchs’ uveitis that was classifiedas non-granulomatous leading to misdiagnosis as Behçet’suveitis. Hyperfluorescent is part of the semiology of Fuchs’
uveitis, together with micro-granulomatous KPs and vitre-ous cellular infiltration
Anterior Non-granulomatous Uveitis: Differential Diagnosis 13

Fuchs’ uveitis absolutely allows to excludeBehçet’s uveitis. The problem is that in sometextbooks the small KPs seen as Fuchs’ uveitisare described as non-granulomatous and Fuchs’uveitis is classified into the group ofnon-granulomatous uveitis entities, leading tothe misdiagnosis that happened in caseno. 4. Finally there is some confusion in the clin-ical use of the term granulomatous. This termshould not be taken in its histopathologic sense:It is in fact a misnomer as it uses a histopathologicterm to categorize a clinical spectrum includingdiseases that, if histopathology were done, do nothave histopathologic granulomatous features.
Conclusion
Non-granulomatous anterior uveitis entities canpresent with very high flare values that however,in general, respond well to corticosteroid therapy,usually topical but that sometimes need to be givenby periocular injections and even systemically,sometimes needing to be very aggressive. Evolu-tion of these entities is nowadays best performedusing laser flare photometry (LFP) that allowsobjective and precise measurement of flare. Bothin high and low flare situations, LFP can detectslight flare changes imperceptible to the humaneye at the slit lamp, allowing to step up with treat-ment in case of LFP-detected resistance to therapy.On the other hand, in low flare situations, LFPavoids overtreatment if it detects decrease of flareagain not perceptible at the slit lamp.
Key Points• Non-granulomatous anterior uveitides are uve-
itis entities characterized by fine retro-descemetic keratic precipitates (KPs) no largerthan dust, associated with hypopyon or fibrinclots in severe forms.
• This distinction allows to orient diagnostic work-up and identify a number of specific entities.
• The more frequent entities include HLA-B27-related uveitis, JIA-associated uveitis predom-inant in children, and Behçet’s uveitis.
• In the initial stages, granulomatous anterioruveitis can sometimes present itself asnon-granulomatous.
• Non-granulomatous entities can often presentwith high flare and cell values that are stillgraded using the Proctor grading systemtaken over by the SUN system. In order toprecisely monitor these patients nowadays,however, laser flare photometry is the methodof choice, able to detect small flare variationsboth in high and low flare states.
• In severe cases, hypotony is often found espe-cially in inflammation involving the ciliarybody such as acute anteriornon-granulomatous HLA-B27-related uveitis.
Suggested Reading
Agrawal R, Keane PA, Singh J, Saihan Z, Kontos A,Pavesio C. Comparative analysis of anterior chamberflare grading between clinicians with different levels ofexperience and semi-automated laser flare photometry.Ocul Immunol Inflamm. 2016;24(2):184-93.
Fig. 22 Papillitis in streptococcal-related para-infectious uveitis
14 M. Papadia et al.

Ben Salah R, Frikha F, Hentali Y, Kallel S, Ghorbel A,Mnif Z, Bahloul Z. Recurrent anterior uveitis withhypopyon revealing relapsing polychondritis. InternMed. 2012;51:3173–6.
Bernasconi O, Papadia M, Herbort CP. Sensitivity of laserflare photometry compared to slit-lamp cell evaluationin monitoring anterior chamber inflammation. IntOphthalmol. 2010;30:495–500.
Conway R, Low C, Coughlan RJ, O’Donnell MJ, CareyJJ. Risk of liver injury among methotrexate users: ameta-analysis of randomised controlled trials. SeminArthritis Rheum. 2015;45(2):156–62.
FuchsHerbort CP, Guex-Crosier Y, de Ancos E, Pittet N. Use of
laser flare photometry to assess and monitor inflamma-tion in uveitis. Ophthalmology. 1997;104:64–72.
Hogan MJ, Kimura SJ, Thygeson P. Signs and symptomsof uveitis. 1. Anterior uveitis. Am J Ophthalmol.1959;47:155–70.
Jones NP. Juvenile chronic arthritis and uveitis. In: JonesNP, editor. Uveitis, an illustrated Manuel. Oxford:Butterworth Heinemann; 1998. p. 129–35.
Mackensen F, Smith JR, Rosenbaum JT. Enhanced recog-nition, treatment and prognosis of tubulointerstitialnephritis and uveitis syndrome. Ophthalmology.2007;114:995–9.
Rehman US, Anand S, Reddy A, Backhouse OC,Mohamed M, Mahomed I, Atkins AD, JamesT. Poststreptococcal syndrome uveitis: a descriptivecase series and literature review. Ophthalmology.2006;113(4):701–6.
Rosenbaum JT. HLA B27-associated diseases. In: PeposeJS, Holland GN, Wilhelmus KR, editors. Ocular infec-tion and immunity. St Louis: Mosby-Yearbook; 1996.p. 475–84.
Tanaka R, Takamoto M, Komae K, Ohtomo K, Fujino Y,Kaburaki T. Clinical features of psoriatic uveitis inJapanese patients. Graefes Arch Clin Exp Ophthalmol.2015;253:1175–80.
Tran VT, Auer C, Guex-Crosier Y, Pittet N, HerbortCP. Epidemiological characteristics of uveitis in Swit-zerland. Int Ophthalmol. 1995;18:293–8.
Tugal-Tutkun I, Herbort CP. Laser flare photometry, anon-invasive, objective and quantitative method tomeasure intraocular inflammation. Int Ophthalmol.2010;30:453–64.
Tugal-Tutkun I, Onal S, Altan-Yaycinglu R, HuseyinAltunbas H, Urgancioglu M. Uveitis in Behçet’s dis-ease, an analysis of 880 patients. Am J Ophthalmol.2004;138:373–80.
Anterior Non-granulomatous Uveitis: Differential Diagnosis 15