Embed Size (px)
Citation preview

Anterior cruciate ligament reconstruction
The two-incision technique
Thomas J. Gill, MDa,*, J. Richard Steadman, MDb,c
aDepartment of Orthopedic Surgery, Harvard Medical School, Massachusetts General Hospital Ambulatory Care Center,
15 Parkman Street Boston, MA 02114, USAbThe Steadman Hawkins Clinic, 181 West Meadow Drive, Vail, CO, USA
cSouthwestern Medical School, Dallas, TX, USA
The anterior cruciate ligament (ACL) can be
successfully reconstructed using a variety of surgical
techniques. Historically, the two-incision technique
was the standard of practice. It allows predictable,
near-anatomic placement of the femoral tunnel and
provides highly reproducible results with few com-
plications. As arthroscopic techniques continue to
advance, the all-endoscopic reconstruction technique
has gained tremendous popularity. Advocates of the
endoscopic method cite the avoidance of a second
lateral incision and decreased operative time as its
major advantages, with the implication that better
functional outcomes result.
There are several major advantages of the two-
incision technique over endoscopic methods. These
include consistent femoral tunnel placement, elimina-
tion of concern for ‘‘blowing out the back wall,’’
elimination of the problem of graft– tunnel mismatch,
elimination of the problem of screw divergence, and
ease of use for revision ACL reconstruction proce-
dures. The angle of the ACL graft is also more
anatomic, matching the angle of the native ACL.
In this chapter we present our technique for
reconstruction of the ACL using the two-incision
approach. Indications for its use are discussed.
Advantages and disadvantages of the two-incision
method compared with the all-endoscopic approach
are reviewed.
Technical considerations of the endoscopic and
two-incision techniques
Femoral tunnel placement
Incorrect placement of the femoral tunnel results
in one of the more common surgical errors made
when reconstructing the ACL. ‘‘Over-the-top’’ place-
ment is nonisometric, producing an increase in graft
length and tension with progressive knee extension.
Anterior displacement of the femoral tunnel causes
an increase in graft strain with increasing knee
flexion, resulting in decreased joint motion and
arthrofibrosis postoperatively and possible graft im-
pingement in extension.
The native ACL changes less than 3 mm in length
with passive knee motion [1,2]. This change in length
occurs because of the cam effect of the femoral
condyles, which causes a change in the position of
the instant center of rotation of the knee in the sagittal
plane. Because the center of rotation is closer to the
femoral attachment than the tibial attachment site,
there is little room for error when placing the femoral
tunnel if knee kinematics are to be optimized [3]. As a
result, it is imperative to place an ACL graft so that
there is less than 3 mm of graft motion from 0� to 90�of knee flexion. In fact, we believe that 2 mm of graft
motion is the maximum amount of motion that should
be permitted when performing an ACL reconstruction.
An isometer may be used before fixation of the graft to
accurately assess the potential degree of graft motion
[4]. In this manner, graft tension can be minimized in
the postoperative rehabilitation period [2,5].
0030-5898/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0030 -5898 (02 )00030 -5
* Corresponding author.
E-mail address: [email protected] (T.J. Gill).
Orthop Clin N Am 33 (2002) 727–735

Radiographic studies have confirmed the impor-
tance of femoral tunnel placement. Clinical results
correlate positively with femoral tunnels placed at
least 60% posterior to the anterior origin Blumen-
saat’s line [6]. A loss of knee flexion and increased
graft strain results from a femoral tunnel placed
more anteriorly.
The two-incision technique can eliminate the
problem of anterior femoral tunnel placement. The
‘‘rear-entry guide’’ that is available in most surgical
sets does not, in general, permit significantly anterior
graft placement. These guides are designed to be
placed on the back wall of the intercondylar notch,
maximizing posterior placement of the graft. Because
the lateral femoral condyle serves as the conduit for
the femoral bone block, there is no concern about
‘‘blowing out the back wall’’ of the intercondylar
notch. In contrast, the endoscopic technique relies on
this back wall for bone block stability and fixation.
Once disrupted, the endoscopic technique cannot be
used without sacrificing optimal femoral graft place-
ment. It is likely this concern results in some sur-
geons erring on the anterior side when placing an
endoscopic femoral tunnel.
Graft– tunnel mismatch
A major factor in the success of an endoscopic
ACL reconstruction relates to the length of the tibial
tunnel, especially when using fixed-length bone–
patellar tendon–bone autografts. Fixation of the graft
in the femoral tunnel is usually a fixed variable.
Regardless of the length of the femoral bone block,
the end of the bone block is placed at the opening of
the intercondylar notch to allow biomechanically
superior ‘‘articular’’ fixation with interference screws.
This construct minimizes the incidence of the ‘‘wind-
shield wiper effect,’’ tunnel widening, and graft
elongation. Seeding the bone block more proximally
in the femur also exposes the graft to the risk of
abrasion on the tunnel opening or severance while
inserting an endoscopically placed interference screw.
As a result of the fixed variable of femoral graft
placement, the length of the patellar tendon and tibial
bone block become a central concern for endoscopic
reconstructions. Graft – tunnel mismatch can occur
when the length of the graft is too long or too short
with regard to the tibial tunnel. If the tibial tunnel is
placed at too acute an angle, its length is shortened,
and graft extrusion can occur. The ability to achieve
interference screw fixation is compromised if at least
15 to 20 mm of graft is not inside the tunnel. An
excessively long tunnel may result in blind placement
of the interference screw deep inside the tibial tunnel,
with potential problems of screw divergence or articu-
lar penetration.
To avoid problems with graft– tunnel mismatch,
surgeons using the endoscopic technique often use
one of a variety of mathematical formulas to deter-
mine the correct angle to drill or to create the desired
tibial tunnel length [7,8]. An indirect technique,
called the N + 7 rule, adds 7� to the length of the
patellar tendon (N) to calculate the proper angle to
drill the tibial tunnel [9]. Some surgeons add 5 mm
to the length of the tendon in their calculations to
compensate for the obliquity of the tibial tunnel [7].
All such calculations are unimportant when per-
forming the two-incision technique. Because the
femoral bone blocks and tibial bone blocks are placed
and secured under direct vision, the graft can be
advanced or retracted in the femoral and tibial tunnels
as needed to optimize placement near the articular
surface while eliminating the possibility of graft
extrusion at either end. The tibial tunnel can therefore
be drilled at virtually any angle, within reason. This is
an especially important point when combined ACL/
posterior cruciate ligament (PCL) reconstructions are
performed, and a proper bone bridge (about 2 cm) is
desired between the two tibial tunnels to avoid tunnel
overlap and to optimize fixation.
Screw divergence
Screw divergence occurs when graft fixation
screws are not placed parallel to the long axis of
the bone block. It is generally accepted that the
fixation sites of ACL grafts are the weakest points
of an ACL reconstruction in the immediate post-
operative period. Interference screws provide the
most secure fixation when using a bone–patellar
tendon graft [10,11]. If the screws diverge or con-
verge from the graft, fixation strength may be com-
promised or the bone block can be fractured.
Divergence angles exceeding 15� to 30� have been
associated with an increased incidence of graft pull-
out in several in vitro load-to-failure studies [12–14].
Interference screw fixation in the femoral tunnel is
accomplished under direct visualization when using
the two-incision technique, using a cannulated screw
placed over a guide wire. Several studies have dem-
onstrated that endoscopic placement of the screw is not
as accurate as using the two-incision technique [15].
Endoscopic guides such as the ‘‘two-pin passer’’
(Linvatec, Largo, FL) have been developed to aid in
parallel screw placement. A slotted guide pin used for
graft passage is placed through the femoral tunnel,
with the guide wire for the femoral screw placed in
parallel through the slot and out the femur. The
T.J. Gill, J.R. Steadman / Orthop Clin N Am 33 (2002) 727–735728

problem of screw divergence is virtually eliminated
when using such a guide, but it is still essential to use
a graft protector when advancing the interference
screw to prevent injury to the graft from the screw
threads. It is also important to hyperflex the knee
until the guide wire is completely straight to facilitate
screw advancement, protect the graft, and prevent
guide pin breakage.
The two-incision surgical technique
Graft harvest
A longitudinal incision is made along the medial
border of the patellar tendon between the inferior pole
of the patella and the tibial tubercle. The subcuta-
neous tissue is dissected down to the level of the
paratenon. The paratenon is incised and elevated as a
distinct layer to allow closure after harvesting of the
tendon is completed. The medial and lateral borders
of the tendon are defined, and the width of the tendon
measured. One third of the tendon is harvested, with a
10-mm graft generally chosen. If the width is less
than 27 mm, a 9-mm graft is used.
A 2-mm drill bit is used to weaken the distal
attachments of the bone blocks rather than using an
oscillating saw, which could ‘‘past point’’ and leave a
stress riser. On the patellar side, the drill enters at a
30� angle to make a more bullet-shaped graft that is
easier to pass into the femoral tunnel. Lateral saw cuts
are made at a 20� angle to make a more trapezoidal
graft. A pick is used to weaken the patella at the
inferior pole so that the patellar bone block does not
break into the joint upon harvest.
Graft sizers are used to trim the bone plugs.
Maximizing the size of the bone plugs within the
respective tunnels is important to obtain rigid fixation
of the graft. Leaving a large gap for the passage of
instruments between the tibial bone plug and the wall
of the tunnel decreases the interference fit and results
in less optimal fixation [11]. Two number 5 Ethibond
sutures are placed at either end of the bone blocks.
We do not typically ‘‘tube’’ the graft. The tibial block
is generally 35 mm by 10 mm, and the patellar block
is usually 25 mm by 10 mm. If 25 mm represents
more than one third the longitudinal length of the
patella, a 20-mm graft is generally harvested instead.
Tibial tunnel placement
Although early studies stressed a more anterior
placement of the tibial tunnel within the ACL tibial
footprint, we use a more posterior placement. The
anterior aspect of the native ACL is concave and
accommodates the anterior aspect of the intercondylar
roof to avoid ligamentous impingement [16]. Placing
the tibial tunnel too far anteriorly increases graft
tension in flexion and results in impingement of the
graft on the intercondylar roof as the knee moves into
extension. Although it is not common to place the
graft too posteriorly, excessively posterior placement
of the graft theoretically increases graft tension in
extension and may damage the tibial attachment of
the PCL during tunnel drilling [3,17]. A more pos-
terior placement orients the graft more vertically with
respect to the tibial joint surface. This orientation can
decrease the ability of the ACL to resist anterior
displacement of the tibia.
We typically use a landmark for the ACL guide
pin that is 7 to 9 mm anterior to the PCL and 7 mm
lateral to the medial femoral condyle on the down-
slope of the medial tibial spine (Fig. 1). Such
placement minimizes the risk of impingement on
the intercondylar roof and the lateral wall. This
placement is supported by the work of Morgan et
al [18]. They reported that at 90� of knee flexion, thedistance from the central insertion site of the ACL to
the anterior margin of the PCL is a constant 7 mm,
independent of variations in knee dimensions. The
guide pin should enter the joint on a line drawn
parallel to the anterior edge of the femoral condyles
from the edge of the femoral condyles. Because
individual anatomy may vary, this secondary guide
confirms correct placement of the guide pin.
Medial– lateral placement is equally important to
prevent graft impingement on the lateral femoral
condyle and in general should be 6 to 7 mm from
the medial femoral condyle.
A tibial tunnel guide with a variable arm is used.
In general, an angle of 55� is chosen. Creating a tibial
Fig. 1. Tibial tunnel placement 7 mm anterior to the PCL on
the downslope of medial tibial spine.
T.J. Gill, J.R. Steadman / Orthop Clin N Am 33 (2002) 727–735 729

tunnel at a constant angle without regard to the
patellar tendon length can lead to a higher incidence
of graft– tunnel mismatch when using the endoscopic
method [19]. This is a nonissue when using the two-
incision technique. A point is chosen for the entrance
to the tibial tunnel at a position at least 1 cm medial to
the tibial tubercle.
After the guide pin is passed, placement is con-
firmed by lifting the heel to passively extend the knee
while arthroscopically observing for pin impinge-
ment on the intercondylar roof. Yaru et al reported
that the anterior tibial displacement caused by the
active pull of the quadriceps tendon results in graft
impingement an average of 9� earlier than that
obtained from passive extension of the knee. They
recommended a more extensive notchplasty to ac-
count for this difference [20]. We recommend a notch
width of at least 18 mm to help avoid lateral wall
impingement. Most arthroscopic pituitary rongeurs
are 17 mm in width when fully opened and can be
used as a guide for notch size. A stenotic notch is
widened using a curved osteotome and motorized
burr. Because the posterior notch can also contribute
to impingement, this area should be made into an
oval to ovoid lateral impingement.
Femoral tunnel placement
The femoral tunnel is established from the outside
in using the two-incision technique. A longitudinal
incision is made along the lateral aspect of the distal
femur. The incision is begun at a level 2 cm proximal
to the superior pole of the patella and extended
proximally for a distance of 3 to 4 cm (Fig. 2). The
iliotibial band is split longitudinally, exposing the
vastus lateralis. The vastus lateralis is dissected off of
the intermuscular septum and retracted anteriorly to
expose the lateral aspect of the distal femoral meta-
physis (Fig. 3). Cauterize the perforating veins
through the intermuscular septum to avoid a post-
operative hematoma. The septum is divided distally.
After the femur has been exposed, a 70� arthroscopeis inserted through the anterior inferior lateral portal.
The torn ACL remnant is debrided, exposing the
lateral wall of the intercondylar notch. The notch-
plasty is examined, and an oval posterior wall is
confirmed. A long, curved vascular clamp is inserted
through the inferomedial portal. It is passed around
the posterior aspect of the lateral femoral tunnel,
through the over-the-top position. The clamp is used
to perforate a hole in the posterior capsule to allow
passage of the rear-entry femoral guide. As long as
the clamp is passed laterally, adhering closely to the
posterior aspect of the femur, there is no danger to the
neurovascular structures. Once the septum has been
perforated by the clamp, a curved hook passer is
inserted through the inferomedial portal, along the
over-the-top position (Fig. 4), and through the inter-
muscular septum into the lateral operative field. At
this point, the rear-entry guide is hooked onto the
eyelet at the distal tip of the curved passer. The passer
is then withdrawn, pulling the rear-entry guide into
the joint without danger to the neurovascular struc-
tures (Fig. 5A, B).
The femoral tunnel can then be established. The
tip of the rear-entry drill guide is positioned at the
back wall of the notch, 2 mm anterior to the back wall
Fig. 2. Location of skin incision.
Fig. 3. Elevation of vastus lateralis.
Fig. 4. Passing of rear-entry guide retriever through over the
top position.
T.J. Gill, J.R. Steadman / Orthop Clin N Am 33 (2002) 727–735730
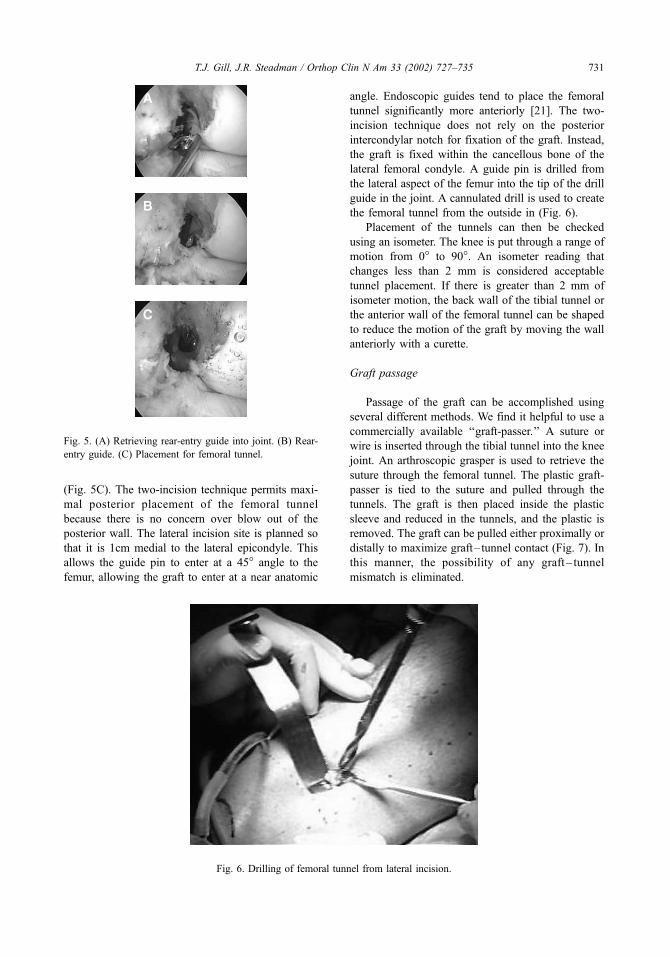
(Fig. 5C). The two-incision technique permits maxi-
mal posterior placement of the femoral tunnel
because there is no concern over blow out of the
posterior wall. The lateral incision site is planned so
that it is 1cm medial to the lateral epicondyle. This
allows the guide pin to enter at a 45� angle to the
femur, allowing the graft to enter at a near anatomic
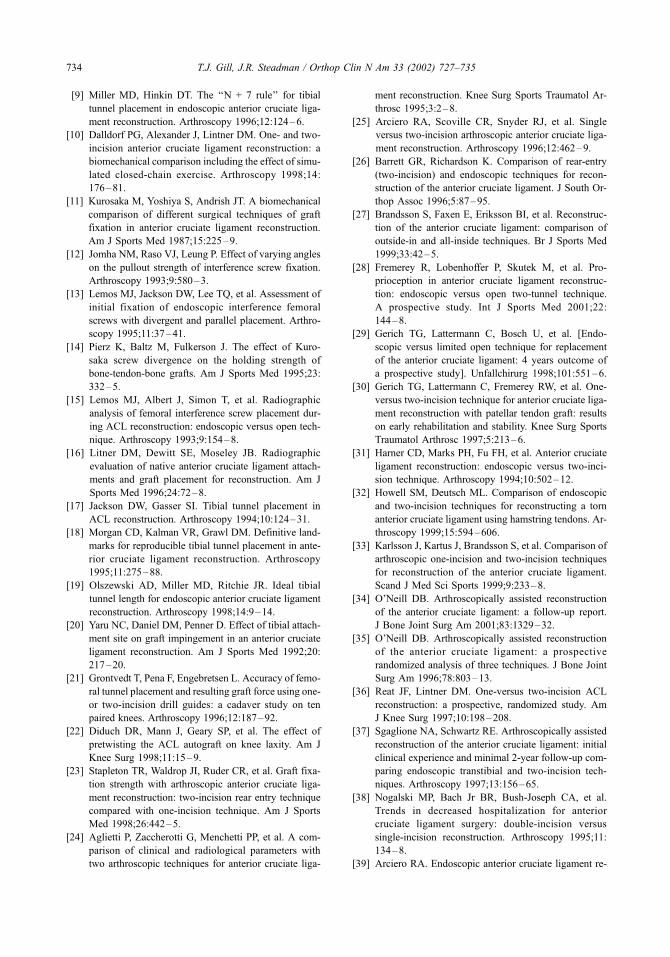
angle. Endoscopic guides tend to place the femoral
tunnel significantly more anteriorly [21]. The two-
incision technique does not rely on the posterior
intercondylar notch for fixation of the graft. Instead,
the graft is fixed within the cancellous bone of the
lateral femoral condyle. A guide pin is drilled from
the lateral aspect of the femur into the tip of the drill
guide in the joint. A cannulated drill is used to create
the femoral tunnel from the outside in (Fig. 6).
Placement of the tunnels can then be checked
using an isometer. The knee is put through a range of
motion from 0� to 90�. An isometer reading that
changes less than 2 mm is considered acceptable
tunnel placement. If there is greater than 2 mm of
isometer motion, the back wall of the tibial tunnel or
the anterior wall of the femoral tunnel can be shaped
to reduce the motion of the graft by moving the wall
anteriorly with a curette.
Graft passage
Passage of the graft can be accomplished using
several different methods. We find it helpful to use a
commercially available ‘‘graft-passer.’’ A suture or
wire is inserted through the tibial tunnel into the knee
joint. An arthroscopic grasper is used to retrieve the
suture through the femoral tunnel. The plastic graft-
passer is tied to the suture and pulled through the
tunnels. The graft is then placed inside the plastic
sleeve and reduced in the tunnels, and the plastic is
removed. The graft can be pulled either proximally or
distally to maximize graft– tunnel contact (Fig. 7). In
this manner, the possibility of any graft – tunnel
mismatch is eliminated.
Fig. 6. Drilling of femoral tunnel from lateral incision.
Fig. 5. (A) Retrieving rear-entry guide into joint. (B) Rear-
entry guide. (C) Placement for femoral tunnel.
T.J. Gill, J.R. Steadman / Orthop Clin N Am 33 (2002) 727–735 731

We do not twist the graft before fixation. This is
supported by Diduch et al [22], whose study indi-
cated that pre-twisting the patellar tendon autograft
in ACL reconstruction had no significant short-term
effect on knee laxity as determined by instrumented
testing or clinical examination.
Graft fixation
Interference screw fixation is ideal with the two-
incision technique. Interference screws are placed
along guide wires inserted parallel to the bone
blocks. Guide wires decrease the possibility of
screw divergence, which has been shown to weaken
the initial fixation strength of ACL grafts. The
femoral screw is generally placed first (Fig. 8),
leaving the proximal head of the screw at the level
of the lateral femoral cortex. Although there is a
report suggesting stronger fixation with the endo-
scopic versus two-incision technique [23], this dif-
ference does not seem to be clinically relevant. In
the senior author’s series, there have been no fail-
Fig. 8. Placement of femoral interference screw.
Fig. 7. Passage of patellar tendon graft in antegrade fashion.
T.J. Gill, J.R. Steadman / Orthop Clin N Am 33 (2002) 727–735732

ures of fixation using the two-incision technique in
over 2000 cases.
After femoral screw placement is performed, the
knee is cycled with tension applied to the graft. The
tibial inference screw is then placed with the knee in
full extension, and tension is applied to the sutures on
the tibial bone block.
The sutures used to pass the graft are left prom-
inent after screw fixation to allow the screws to be
located in the event of a revision reconstruction, even
if there is bony overgrowth.
Outcomes: endoscopic versus two-incision
Advocates of endoscopic reconstruction tech-
niques frequently cite the avoidance of a lateral
incision and decreased operative time as the major
advantages of the technique when compared with
the two-incision procedure. The suggestion is that
avoiding the lateral incision decreases morbidity,
allows earlier and more aggressive rehabilitation,
and thus improves outcomes. In over 2000 cases
done by the senior author, there have been no
complaints localized to the lateral incision site.
However, to the best of our knowledge, there have
been no studies to date that have demonstrated
improved outcomes using the endoscopic technique.
In contrast, multiple studies have reported no sig-
nificant difference in outcomes between endoscopic
and two-incision techniques [24–37]. Besides the
functional outcomes, there does not seem to be a
difference in proprioception [28] or the ability to
begin early rehabilitation between the two groups
[10,30]. The endoscopic technique does offer advan-
tages with regard to cosmesis [32] and decreased
operative time [27,32]. Hospital stay and cost
may be slightly higher with the two-incision tech-
nique [38].
Complications
The two-incision ACL reconstruction technique
has been used by one of us (JRS) for over 3000 pa-
tients. We have never had an incident in which there
was damage to the popliteal artery, popliteal vein,
or tibial nerve. In contrast to unsubstantiated con-
cerns over the safety of the two-incision technique,
several studies have reported a higher rate of com-
plications when using the endoscopic method [15,25,
33,39–41]. Screw divergence and violation of the
back wall of the femoral tunnel were most commonly
cited. Heterotopic ossification has been reported for
two-incision reconstructions [42].
Conclusion
It is not possible to create a normal cruciate
ligament with ACL reconstruction surgery. Instead,
the surgeon should strive to recreate a functionally
stable knee. Although there are many important
considerations, accurate graft placement and secure
fixation is paramount in achieving a successful recon-
struction, regardless of the technique used. The two-
incision technique eliminates many of the pitfalls of
endoscopic reconstructions, including graft– tunnel
mismatch, violation of the posterior femoral tunnel,
screw-divergence, and anterior placement of the fem-
oral tunnel. Perhaps one of the greatest utilities of the
two-incision technique is its use for revision of a
failed endoscopic reconstruction because the femoral
tunnel placement can be optimized without concern
about overlapping with the previous femoral tunnel or
blowing out the back wall. The two-incision tech-
nique, when performed properly, allows highly pre-
dictable, consistent results with few complications.
References
[1] Barrett GR, Treacy SH. The effect of intraoperative
isometric measurement on the outcome of anterior cru-
ciate ligament reconstruction: a clinical analysis. Ar-
throscopy 1996;12:645–51.
[2] Penner DA, Daniel DM, Wood P, et al. An in vitro
study of anterior cruciate ligament graft placement
and isometry. Am J Sports Med 1988;16:238–43.
[3] Johnson DL, Fu FH. Anterior cruciate ligament recon-
struction: why do failures occur? In: Instructional
course lectures. Rosemont, IL: American Academy of
Orthopaedic Surgeons; 1995. p. 391–404.
[4] Jackson DW, Jennings LD. Arthroscopically assisted
reconstruction of the anterior cruciate ligament using
a patella tendon bone autograft. Clin Sports Med 1988;
7:785–800.
[5] Drez Jr D, DeLee JC. Orthopaedic sports medicine,
principles and practice. Philadelphia: WB Saunders;
1994. p. 2.
[6] Khalfayan EE, Sharkey PF, Alexander AH, et al. The
relationship between tunnel placement and clinical re-
sults after anterior cruciate ligament reconstruction.
Am J Sports Med 1996;24:335–41.
[7] Kenna B, Simon TM, Jackson DW, et al. Endo-
scopic ACL reconstruction: a technical note on tun-
nel length for interference fixation. Arthroscopy
1993;9: 228–30.
[8] Shaffer B, Gow W, Tibone JE. Graft-tunnel mismatch
in endoscopic anterior cruciate ligament reconstruc-
tion: a new technique of intraarticular measurement
and modified graft harvesting. Arthroscopy 1993;9:
633–46.
T.J. Gill, J.R. Steadman / Orthop Clin N Am 33 (2002) 727–735 733
[9] Miller MD, Hinkin DT. The ‘‘N + 7 rule’’ for tibial
tunnel placement in endoscopic anterior cruciate liga-
ment reconstruction. Arthroscopy 1996;12:124–6.
[10] Dalldorf PG, Alexander J, Lintner DM. One- and two-
incision anterior cruciate ligament reconstruction: a
biomechanical comparison including the effect of simu-
lated closed-chain exercise. Arthroscopy 1998;14:
176–81.
[11] Kurosaka M, Yoshiya S, Andrish JT. A biomechanical
comparison of different surgical techniques of graft
fixation in anterior cruciate ligament reconstruction.
Am J Sports Med 1987;15:225–9.
[12] Jomha NM, Raso VJ, Leung P. Effect of varying angles
on the pullout strength of interference screw fixation.
Arthroscopy 1993;9:580–3.
[13] Lemos MJ, Jackson DW, Lee TQ, et al. Assessment of
initial fixation of endoscopic interference femoral
screws with divergent and parallel placement. Arthro-
scopy 1995;11:37–41.
[14] Pierz K, Baltz M, Fulkerson J. The effect of Kuro-
saka screw divergence on the holding strength of
bone-tendon-bone grafts. Am J Sports Med 1995;23:
332–5.
[15] Lemos MJ, Albert J, Simon T, et al. Radiographic
analysis of femoral interference screw placement dur-
ing ACL reconstruction: endoscopic versus open tech-
nique. Arthroscopy 1993;9:154–8.
[16] Litner DM, Dewitt SE, Moseley JB. Radiographic
evaluation of native anterior cruciate ligament attach-
ments and graft placement for reconstruction. Am J
Sports Med 1996;24:72–8.
[17] Jackson DW, Gasser SI. Tibial tunnel placement in
ACL reconstruction. Arthroscopy 1994;10:124–31.
[18] Morgan CD, Kalman VR, Grawl DM. Definitive land-
marks for reproducible tibial tunnel placement in ante-
rior cruciate ligament reconstruction. Arthroscopy
1995;11:275–88.
[19] Olszewski AD, Miller MD, Ritchie JR. Ideal tibial
tunnel length for endoscopic anterior cruciate ligament
reconstruction. Arthroscopy 1998;14:9–14.
[20] Yaru NC, Daniel DM, Penner D. Effect of tibial attach-
ment site on graft impingement in an anterior cruciate
ligament reconstruction. Am J Sports Med 1992;20:
217–20.
[21] Grontvedt T, Pena F, Engebretsen L. Accuracy of femo-
ral tunnel placement and resulting graft force using one-
or two-incision drill guides: a cadaver study on ten
paired knees. Arthroscopy 1996;12:187–92.
[22] Diduch DR, Mann J, Geary SP, et al. The effect of
pretwisting the ACL autograft on knee laxity. Am J
Knee Surg 1998;11:15–9.
[23] Stapleton TR, Waldrop JI, Ruder CR, et al. Graft fixa-
tion strength with arthroscopic anterior cruciate liga-
ment reconstruction: two-incision rear entry technique
compared with one-incision technique. Am J Sports
Med 1998;26:442–5.
[24] Aglietti P, Zaccherotti G, Menchetti PP, et al. A com-
parison of clinical and radiological parameters with
two arthroscopic techniques for anterior cruciate liga-
ment reconstruction. Knee Surg Sports Traumatol Ar-
throsc 1995;3:2–8.
[25] Arciero RA, Scoville CR, Snyder RJ, et al. Single
versus two-incision arthroscopic anterior cruciate liga-
ment reconstruction. Arthroscopy 1996;12:462–9.
[26] Barrett GR, Richardson K. Comparison of rear-entry
(two-incision) and endoscopic techniques for recon-
struction of the anterior cruciate ligament. J South Or-
thop Assoc 1996;5:87–95.
[27] Brandsson S, Faxen E, Eriksson BI, et al. Reconstruc-
tion of the anterior cruciate ligament: comparison of
outside-in and all-inside techniques. Br J Sports Med
1999;33:42–5.
[28] Fremerey R, Lobenhoffer P, Skutek M, et al. Pro-
prioception in anterior cruciate ligament reconstruc-
tion: endoscopic versus open two-tunnel technique.
A prospective study. Int J Sports Med 2001;22:
144–8.
[29] Gerich TG, Lattermann C, Bosch U, et al. [Endo-
scopic versus limited open technique for replacement
of the anterior cruciate ligament: 4 years outcome of
a prospective study]. Unfallchirurg 1998;101:551–6.
[30] Gerich TG, Lattermann C, Fremerey RW, et al. One-
versus two-incision technique for anterior cruciate liga-
ment reconstruction with patellar tendon graft: results
on early rehabilitation and stability. Knee Surg Sports
Traumatol Arthrosc 1997;5:213–6.
[31] Harner CD, Marks PH, Fu FH, et al. Anterior cruciate
ligament reconstruction: endoscopic versus two-inci-
sion technique. Arthroscopy 1994;10:502–12.
[32] Howell SM, Deutsch ML. Comparison of endoscopic
and two-incision techniques for reconstructing a torn
anterior cruciate ligament using hamstring tendons. Ar-
throscopy 1999;15:594–606.
[33] Karlsson J, Kartus J, Brandsson S, et al. Comparison of
arthroscopic one-incision and two-incision techniques
for reconstruction of the anterior cruciate ligament.
Scand J Med Sci Sports 1999;9:233–8.
[34] O’Neill DB. Arthroscopically assisted reconstruction
of the anterior cruciate ligament: a follow-up report.
J Bone Joint Surg Am 2001;83:1329–32.
[35] O’Neill DB. Arthroscopically assisted reconstruction
of the anterior cruciate ligament: a prospective
randomized analysis of three techniques. J Bone Joint
Surg Am 1996;78:803–13.
[36] Reat JF, Lintner DM. One-versus two-incision ACL
reconstruction: a prospective, randomized study. Am
J Knee Surg 1997;10:198–208.
[37] Sgaglione NA, Schwartz RE. Arthroscopically assisted
reconstruction of the anterior cruciate ligament: initial
clinical experience and minimal 2-year follow-up com-
paring endoscopic transtibial and two-incision tech-
niques. Arthroscopy 1997;13:156–65.
[38] Nogalski MP, Bach Jr BR, Bush-Joseph CA, et al.
Trends in decreased hospitalization for anterior
cruciate ligament surgery: double-incision versus
single-incision reconstruction. Arthroscopy 1995;11:
134–8.
[39] Arciero RA. Endoscopic anterior cruciate ligament re-
T.J. Gill, J.R. Steadman / Orthop Clin N Am 33 (2002) 727–735734

construction: complication of graft rupture and a meth-
od of salvage. Am J Knee Surg 1996;9:27–31.
[40] Bush-Joseph CA, Bach Jr BR, Bryan J. Posterior cort-
ical violation of the femoral tunnel during endoscopic
anterior cruciate ligament reconstruction. Am J Knee
Surg 1995;8:130–3.
[41] Jackson DW, Kenna R, Simon TM, et al. Endoscopic
ACL reconstruction. Orthopedics 1993;16:951–8.
[42] Ogilvie-Harris DJ, Sekyi-Otu A. Periarticular het-
erotopic ossification: a complication of arthroscopic
anterior cruciate ligament reconstruction using a two-
incision technique. Arthroscopy 1995;11:676–9.
T.J. Gill, J.R. Steadman / Orthop Clin N Am 33 (2002) 727–735 735








![The Evolution of Anatomic Anterior Cruciate Ligament ... · The Evolution of Anatomic Anterior Cruciate Ligament Reconstruction ... tunnel placement in the axial plane [23]. These](https://img.dokumen.tips/doc/110x75/5f03ed437e708231d40b74ae/the-evolution-of-anatomic-anterior-cruciate-ligament-the-evolution-of-anatomic.jpg)




















