-
Journal of Pediatric Urology (2017) 13, 305.e1e305.e6
Department of PaediatricUrology, Royal ManchesterChildren’s
Hospital, OxfordRoad, Manchester, UK
Correspondence to: R.M.Cervellione, Department ofPaediatric
Urology, RoyalManchester Children’s Hospital,Oxford Road,
Manchester, M139WL, UK, Tel.: þ44 161 7018161
[email protected](R.M. Cervellione)
Keywords
Antegrade sclerotherapy; Vari-cocele; Adolescent
Received 22 August 2016Accepted 29 December 2016Available online
29 January2017
http://dx.doi.org/10.1016/j.j1477-5131/Published by Elsevi
Antegrade sclerotherapy in adolescentvaricocele patients
D.J.B. Keene, R.M. Cervellione
Summary
IntroductionIn the 1970s, Tauber described the
antegradesclerotherapy technique to treat varicoceles, andreported
a 10% recurrence rate. The present studyaimed to evaluate
paediatric success rates and theeffect of modifications to the
surgical technique.
MethodsA prospective study was performed of all
adolescentpatients undergoing antegrade sclerotherapy sur-gery.
Each patient had an idiopathic varicocele withspontaneous venous
reflux on Doppler examination,and underwent cannulation of a
pampiniform plexusvein via a scrotal incision under general
anaesthetic.Aethoxysklerol� 3% (2 ml/kg) maximum 3 ml wasinjected
into the pampiniform plexus vein underfluoroscopic monitoring.
Success was assessed byclinical examination and Doppler ultrasound
3, 6 and9 months after surgery. Data were presented asmedian
(interquartile range). Patients were splitinto three groups: Group
A e liquid sclerotherapywith Y connector; Group B e liquid
sclerotherapy
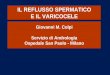
Table Group-wise comparison of success rates
Group A
Modifications totechnique
Liquid sclerotherapy þintravenous connector
Number of patients 14Age of patients (yrs) 14.6 (13.5 �
15.0)Success (%) 58%
*P Z 0.03 (Gp A vs B), **P Z 0.01 (Gp A vs C).
purol.2016.12.018er Ltd on behalf of Journal of Pediatric
Urology Compa
direct to cannula; and Group C e foam sclerotherapydirect to
cannula. Fisher’s exact test was used tocompare the success rates
in each group.
ResultsA total of 91 patients underwent antegrade
sclero-therapy. The median age was 14.8 years (range13.7e15.5).
Eleven persistent varicoceles occurredand were diagnosed by Doppler
ultrasound. Thesuccess rate of surgery was 58% in Group A, 90%
inGroup B and 96% in Group C. Success was signifi-cantly higher in
Group B and Group C compared withGroup A. No testicular atrophy
occurred; two woundinfections, two haematomas and one hydrocelewere
recorded (Table).
ConclusionIntroduction of antegrade sclerotherapy in
theadolescent population resulted in a safe and cost-effective
method for the management of adolescentvaricocele. Several
modifications to the techniquehave been introduced to achieve a
high success rate(96%) with minimal complications.
using Fisher’s exact test.
B C
Liquid sclerotherapydirect to cannula
Foam sclerotherapydirect to cannula
50 2714.7 (13.6 � 15.4) 15.2 (14.1 � 16.6)90% 96%
ny.
mailto:[email protected]:[email protected]://crossmark.crossref.org/dialog/?doi=10.1016/j.jpurol.2016.12.018&domain=pdfhttp://dx.doi.org/10.1016/j.jpurol.2016.12.018http://dx.doi.org/10.1016/j.jpurol.2016.12.018http://dx.doi.org/10.1016/j.jpurol.2016.12.018
-
305.e2 D.J.B. Keene, R.M. Cervellione
Introduction
Varicocele is a common urological condition and presents in8e16%
of adolescent males [1]. The majority of adolescentpatients with a
varicocele remain asymptomatic. Varico-celes are associated with an
increased risk of subfertility inadult males [2]. The challenge for
managing children andadolescents with varicoceles is to avoid under
or overtreatment [1].
Testicular asymmetry (>20%) is seen in approximately10% of
teenagers with a varicocele [2]. Patients with largervolume
differentials have more impaired semen parameters[3]. “Catch-up
growth” following varicocele surgery is seenin this group [4,5].
Other indications for varicocele surgeryinclude symptoms of pain or
heaviness, which is usuallydescribed as a dull ache around the
scrotum that is wors-ened after long periods of standing [6,7].
Routine spermanalysis is being increasingly offered to physically
matureadolescents and young adults [3,8], with varicocele
surgerybeing offered when subfertility is detected [1].
Many techniques have been described for the manage-ment of
varicocele, including: open inguinal [9], highretroperitoneal [10],
laparoscopic (with or without arteryand lymphatic sparing) [11] and
sclerotherapy [12]. There isgreat variability in practice regarding
choice of surgicaltechnique, and with each technique comes
differingcomplication rates [13,14]. Tauber described the
antegradesclerotherapy (AS) technique in the 1970s to treat
varico-celes, and reported a 10% recurrence rate [12]. Within
thepaediatric population, a 10% recurrence rate and 14% risk
ofhydrocele was reported [15].
The present study aimed to: further evaluate paediatricoutcomes
following AS in the management of varicocele;assess complications;
and demonstrate the effect ofmodifying the surgical technique on
success.
Methods
A prospective study was performed of all adolescent pa-tients
presenting to the Varicocele Clinic with idiopathicleft sided
varicocele. All varicoceles that were includedwere clinically
evident: Grade II or Grade III according tothe Dubin and Amelar
clinical classification [16]. Every pa-tient underwent testicular
venous Doppler and only thosewith spontaneous venous reflux on
Doppler ultrasound wereincluded [17]. Paediatric testicular volume
was predictedusing the formula: volume in ml Z 0.52 � L �W � H,
withthe definition of asymmetry being a difference in volume
of>20% [18,19]. Patients included underwent surgery be-tween
2012 and 2016. The indications for surgery included:pain;
testicular asymmetry >20%; subfertility on spermanalysis at 17
years of age (sperm concentration
-
Antegrade sclerotherapy 305.e3
occurred during the study. Two wound infections and
twohaematomas were recorded. Testicular asymmetryimproved in all 28
patients who had an initial median vol-ume difference of 33.9%
(range 26e40.8) and a final volumedifference of 10% (range
0e17).
All 38 patients treated for pain had resolution of painsymptoms
following surgery. One of the three patientstreated for
sub-fertility had, to date, performed a repeatsperm test
postoperatively. His sperm parameters were allimproved: sperm
concentration from
-
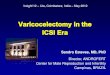
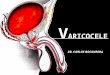
Figure 2 a. Antegrade venography demonstrates a singleinternal
testicular vein. b. Foam sclerotherapy is seen to fillthe internal
testicular vein and displace the contrast up to therenal vein.
305.e4 D.J.B. Keene, R.M. Cervellione
Antegrade sclerotherapy was initially described in the1970s. It
has shown to have the highest economic effec-tiveness of all forms
of surgical management for varicocele,costing £36.64 per case when
performed under localanaesthetic [27], and has a low complication
rate in adults[13,23]. Paediatric studies have reported persistent
vari-cocele rates of 2% [28], 4.5% [29], 7% [30] and 10% [15].
Thevariations in recurrence rates may be due to the differ-ences in
the clinical grades of varicoceles treated in eachstudy. Those
studies using screening to identify patientshave a higher
proportion of small varicoceles (Grades 1 and2), which may be less
prone to persistence [12]. Zaupa
reported that less than half of their patients had
Grade-3varicoceles [30] compared to 86% in the present series.
Adult studies have reported complications of AS,including:
scrotal haematoma in 2.2% of patients, testicularatrophy at a rate
of 0.6%, haematoma and wound infectionsin 3% [30]. In the present
series, two patients (2.2%)experienced a scrotal haematoma and
there were no casesof testicular atrophy.
Postoperative hydrocele formation has its highestcomplication
rate following mass ligation procedures (openor laparoscopic
Palomo) with rates quoted between 3 and23% [31]. Laparoscopic
surgery remains the most widelyused surgical method for the
management of adolescentvaricocele [32]. Techniques utilising
methylene blue eitherto stain the lymphatic channels or to inject
into the veinseffectively reduce the rate of hydrocele formation by
0e5%[33]. These techniques are more time consuming and
costlycompared with AS. Antegrade sclerotherapy is
naturallylymphatic sparing, and so results in low rates of
post-operative hydroceles, which was confirmed in the presentstudy
that reported a 1% hydrocele rate.
The present study reported 11 recurrences followingantegrade
sclerotherapy, which were confirmed by Dopplerultrasound. All
recurrences were treated successfully withrepeat AS. Group A had
the highest recurrence rate (58%);this was thought to be due to the
use of a Y-shaped intra-venous connector between the cannula and
syringe. Wheninjecting such a small volume of sclerosant (maximum 3
ml)a significant portion remained within the connector,
thusreducing its efficacy. After the first 14 procedures (GroupA),
the syringe was connected directly to the cannula(Groups B and C).
This ensured that all the sclerosant wasdelivered into the vein,
ensuring maximum efficacy. Thecombined success rate after this
adjustment to the tech-nique was 93% in Groups B and C, which was
similar to the90% success rate reported by Tauber [12].
A second modification was introduced (Group C) with
theAethoxysklerol� being prepared as a microfoam instead of
aliquid. The preparation technique described by the manu-facturer
involves mixing the Aethoxysklerol� with 7 ml ofair and making it
into a foam using a micro-foam adaptor toproduce 10 ml of a stable,
homogenous and viscousmicrofoam with fine bubbles [34]. The
micro-foam fills theinternal testicular vein(s), displaces the
omnipaque, andallows precise radiological control over the foam
volumerequired (Figs. 1b and 2b). The viscosity of the
microfoamreduces fast “run-off” into the renal vein and
systemiccirculation; the white foam can be seen remaining in
thepampiniform plexus veins during wound closure. Themicrofoam
increases the surface area and contact timebetween the sclerosant
and vessel wall. This technique hasbeen described for varicose vein
treatment, with improvedefficacy and no safety concerns [35]. The
median volume ofthe microfoam injected in the present study was 6
ml(range 5.5e8). Group C had a higher success rate (96%) thanGroup
B (90%); however, with the smaller numbers in GroupC, to date, this
did not achieve significance. The authorssuggest that a relative
contraindication to the microfoampreparation of Aethoxysklerol� may
be pre-pubertal pa-tients with very small pampiniform plexus veins.
The highviscosity of the microfoam can occlude very small
pampi-niform plexus veins before sufficient sclerosant has
flowed
-
Antegrade sclerotherapy 305.e5
into the main internal testicular veins. In these patients,the
sclerosant may be better injected “neat” with the 1 mlair-block
technique, as described by Tauber [12] and as perGroup B
patients.
Overall, the complication rates for this procedurecompared
favourably to those reported in the literature. Thisexperience of
AS in the adolescent population has demon-strated an initial steep
learning curve to optimise the tech-nique by direct injection of
the sclerosant into the cannulawithout the need for an intravenous
connector. Preparationof the sclerosant as a micro-foam has made
the techniquemuch more controlled, with reductions in the amount
ofsclerosant injected and potential gains in success rates.
Conclusion
Introduction of antegrade sclerotherapy in the
adolescentpopulation has resulted in a safe and cost-effective
methodfor the management of adolescent varicocele. Several
mod-ifications to the technique have been introduced to achieve
ahigh success rate (96%) with minimal complications.
Conflict of interest statement
None.
Funding source
No external funding was received. The authors are bothNational
Health Service Employees.
Ethical approval
NHS trust audit approval was obtained. Ethical approvalwas not
required, except for the 21 patients co-enrolled inthe randomised
controlled study of early varicocele surgeryversus conservative
management [20] REC 09/H1013/15.
References
[1] Kolon TF. Evaluation and management of the
adolescentvaricocele. J Urol 2015;194:1194e201.
[2] The influence of varicocele on parameters of fertility in
alarge group of men presenting to infertility clinics. WorldHealth
Organization. Fertil Steril 1992;57:1289e93.
[3] Diamond DA, Zurakowski D, Bauer SB, Borer JG, Peters
CA,Cilento Jr BG, et al. Relationship of varicocele grade
andtesticular hypotrophy to semen parameters in adolescents. JUrol
2007;178:1584e8.
[4] Kass EJ, Belman AB. Reversal Testic growth Fail by
varicoceleligation 1987;137:475e6.
[5] Lund L, Tang YC, Roebuck D, Lee KH, Liu K, Yeung
CK.Testicular catch-up growth after varicocele correction in
ad-olescents. Pediatr Surg Int 1999;15:234e7.
[6] Keene DJB, Sajad Y, Rakoczy G, Cervellione RM.
Testicularvolume and semen parameters in patients aged 12 to 17
yearswith idiopathic varicocele. J Pediatr Surg 2012;47:383e5.
[7] Abrol N, Panda A, Kekre NS. Painful varicoceles: role of
vari-cocelectomy. Indian J Urol 2014;30:369e73.
[8] Keene DJB, Fitzgerald CT, Cervellione RM. Sperm
concentra-tion and forward motility are not correlated with age
in
adolescents with an idiopathic varicocele and
symmetricaltesticular volumes. J Pediatr Surg 2016;51:293e5.
[9] Ivanissevich O. Left varicocele caused by reflux. (Study
basedon 42 years of clinicosurgical experience with 4470
operatedcases. J Int Coll Surg 1960;13:521.
[10] Palomo A. Radical cure of varicocele by a new
technique;preliminary report. J Urol 1949;61:604e7.
[11] Esposito C, Iaquinto M, Escolino M, Cortese G, De Pascale
T,Chiarenza F, et al. Results and complications of
laparoscopicsurgery for pediatric varicocele. J Pediatr Surg
2001;36:767e9.
[12] Tauber R, Johnsen N. Antegrade scrotal sclerotherapy for
thetreatment of varicocele: technique and late results. J
Urol1994;151:386e90.
[13] Coutinho K, McLeod D, Stensland K, Stock JA. Variations in
themanagement of asymptomatic adolescent grade 2 or 3
leftvaricoceles: a survey of practitioners. J Pediatr Urol
2014;10:430e4.
[14] Pastuszak AW, Kumar V, Shah A, Roth DR. Diagnostic
andmanagement approaches to pediatric and adolescent vari-cocele: a
survey of pediatric urologists. Urology 2014;84:450e5.
[15] Fette A, Mayr J. Treatment of varicoceles in childhood
andadolescence with Tauber’s antegrade scrotal sclerotherapy.
JPediatr Surg 2000;35:1222e5.
[16] Dubin L, Amelar RD. Varicocele size and results of
varicoce-lectomy in selected subfertile men with varicocele.
FertilSteril 1970;21:606e9.
[17] Hirsh AV, Cameron KM, Tyler JP, Simpson J, Pryor JP.
TheDoppler assessment of varicoceles and internal spermatic
veinreflux in infertile men. Br J Urol 1980;52:50e6.
[18] Diamond DA, Paltiel HJ, DiCanzio J, Zurakowski D, Bauer
SB,Atala A, et al. Comparative assessment of pediatric
testicularvolume: orchidometer versus ultrasound. J Urol
2000;164:1111e4.
[19] Zampieri N, Cervellione RM. Varicocele in adolescents: a
6-year longitudinal and followup observational study. J
Urol2008;180:1653e6. discussion 1656.
[20] ISRCTN57825419-Manchester Adolescent Varicocele
Study[Internet]. [cited 2013 Jun 3]. Available from:
http://www.controlled-trials.com/ISRCTN57825419/.
[21] Pinto KJ, Kroovand RL, Jarow JP. Varicocele related
testicularatrophy and its predictive effect upon fertility. J Urol
1994;152:788e90.
[22] Johnsen SG, Agger P. Quantitative evaluation of
testicularbiopsies before and after operation for varicocele.
Fertil Steril1978;29:58e63.
[23] Kroese AC, de Lange NM, Collins J, Evers JL. Surgery
orembolization for varicoceles in subfertile men. CochraneDatabase
Syst Rev 2012;10:CD000479.
[24] Li F, Chiba K, Yamaguchi K, Okada K, Matsushita K, Ando
M,et al. Effect of varicocelectomy on testicular volume in
chil-dren and adolescents: a meta-analysis. Urol
2012;79:1340e5.
[25] Gendel V, Haddadin I, Nosher JL. Antegrade
pampiniformplexus venography in recurrent varicocele: case report
andanatomy review. World J Radiol 2011;3:194e8.
[26] Hsi RS, Dearn J, Dean M, et al. Effective and organ
specificradiation doses from videourodynamics in children. J
Urol2013;190:1364e70.
[27] Johnsen N, Tauber R. Financial analysis of antegrade
scrotalsclerotherapy for men with varicoceles. Br J Urol
1996;77:129e32.
[28] Ficarra V, Sarti A, Novara G, Dalpiaz O, Galfano A,
Cavalleri S,et al. Modified antegrade scrotal sclerotherapy in
adolescentpatients with varicocele. J Pediatr Surg
2004;39:1034e6.
[29] Mazzoni G, Spagnoli A, Lucchetti MC, Villa M, Capitanucci
ML,Ferro F. Adolescent varicocele: Tauber antegrade sclerother-apy
versus Palomo repair. J Urol 2001;166:1462e4.
http://refhub.elsevier.com/S1477-5131(17)30038-4/sref1http://refhub.elsevier.com/S1477-5131(17)30038-4/sref1http://refhub.elsevier.com/S1477-5131(17)30038-4/sref1http://refhub.elsevier.com/S1477-5131(17)30038-4/sref2http://refhub.elsevier.com/S1477-5131(17)30038-4/sref2http://refhub.elsevier.com/S1477-5131(17)30038-4/sref2http://refhub.elsevier.com/S1477-5131(17)30038-4/sref2http://refhub.elsevier.com/S1477-5131(17)30038-4/sref3http://refhub.elsevier.com/S1477-5131(17)30038-4/sref3http://refhub.elsevier.com/S1477-5131(17)30038-4/sref3http://refhub.elsevier.com/S1477-5131(17)30038-4/sref3http://refhub.elsevier.com/S1477-5131(17)30038-4/sref3http://refhub.elsevier.com/S1477-5131(17)30038-4/sref4http://refhub.elsevier.com/S1477-5131(17)30038-4/sref4http://refhub.elsevier.com/S1477-5131(17)30038-4/sref4http://refhub.elsevier.com/S1477-5131(17)30038-4/sref5http://refhub.elsevier.com/S1477-5131(17)30038-4/sref5http://refhub.elsevier.com/S1477-5131(17)30038-4/sref5http://refhub.elsevier.com/S1477-5131(17)30038-4/sref5http://refhub.elsevier.com/S1477-5131(17)30038-4/sref6http://refhub.elsevier.com/S1477-5131(17)30038-4/sref6http://refhub.elsevier.com/S1477-5131(17)30038-4/sref6http://refhub.elsevier.com/S1477-5131(17)30038-4/sref6http://refhub.elsevier.com/S1477-5131(17)30038-4/sref7http://refhub.elsevier.com/S1477-5131(17)30038-4/sref7http://refhub.elsevier.com/S1477-5131(17)30038-4/sref7http://refhub.elsevier.com/S1477-5131(17)30038-4/sref8http://refhub.elsevier.com/S1477-5131(17)30038-4/sref8http://refhub.elsevier.com/S1477-5131(17)30038-4/sref8http://refhub.elsevier.com/S1477-5131(17)30038-4/sref8http://refhub.elsevier.com/S1477-5131(17)30038-4/sref8http://refhub.elsevier.com/S1477-5131(17)30038-4/sref9http://refhub.elsevier.com/S1477-5131(17)30038-4/sref9http://refhub.elsevier.com/S1477-5131(17)30038-4/sref9http://refhub.elsevier.com/S1477-5131(17)30038-4/sref10http://refhub.elsevier.com/S1477-5131(17)30038-4/sref10http://refhub.elsevier.com/S1477-5131(17)30038-4/sref10http://refhub.elsevier.com/S1477-5131(17)30038-4/sref11http://refhub.elsevier.com/S1477-5131(17)30038-4/sref11http://refhub.elsevier.com/S1477-5131(17)30038-4/sref11http://refhub.elsevier.com/S1477-5131(17)30038-4/sref11http://refhub.elsevier.com/S1477-5131(17)30038-4/sref11http://refhub.elsevier.com/S1477-5131(17)30038-4/sref12http://refhub.elsevier.com/S1477-5131(17)30038-4/sref12http://refhub.elsevier.com/S1477-5131(17)30038-4/sref12http://refhub.elsevier.com/S1477-5131(17)30038-4/sref12http://refhub.elsevier.com/S1477-5131(17)30038-4/sref13http://refhub.elsevier.com/S1477-5131(17)30038-4/sref13http://refhub.elsevier.com/S1477-5131(17)30038-4/sref13http://refhub.elsevier.com/S1477-5131(17)30038-4/sref13http://refhub.elsevier.com/S1477-5131(17)30038-4/sref13http://refhub.elsevier.com/S1477-5131(17)30038-4/sref14http://refhub.elsevier.com/S1477-5131(17)30038-4/sref14http://refhub.elsevier.com/S1477-5131(17)30038-4/sref14http://refhub.elsevier.com/S1477-5131(17)30038-4/sref14http://refhub.elsevier.com/S1477-5131(17)30038-4/sref14http://refhub.elsevier.com/S1477-5131(17)30038-4/sref15http://refhub.elsevier.com/S1477-5131(17)30038-4/sref15http://refhub.elsevier.com/S1477-5131(17)30038-4/sref15http://refhub.elsevier.com/S1477-5131(17)30038-4/sref15http://refhub.elsevier.com/S1477-5131(17)30038-4/sref16http://refhub.elsevier.com/S1477-5131(17)30038-4/sref16http://refhub.elsevier.com/S1477-5131(17)30038-4/sref16http://refhub.elsevier.com/S1477-5131(17)30038-4/sref16http://refhub.elsevier.com/S1477-5131(17)30038-4/sref17http://refhub.elsevier.com/S1477-5131(17)30038-4/sref17http://refhub.elsevier.com/S1477-5131(17)30038-4/sref17http://refhub.elsevier.com/S1477-5131(17)30038-4/sref17http://refhub.elsevier.com/S1477-5131(17)30038-4/sref18http://refhub.elsevier.com/S1477-5131(17)30038-4/sref18http://refhub.elsevier.com/S1477-5131(17)30038-4/sref18http://refhub.elsevier.com/S1477-5131(17)30038-4/sref18http://refhub.elsevier.com/S1477-5131(17)30038-4/sref18http://refhub.elsevier.com/S1477-5131(17)30038-4/sref19http://refhub.elsevier.com/S1477-5131(17)30038-4/sref19http://refhub.elsevier.com/S1477-5131(17)30038-4/sref19http://refhub.elsevier.com/S1477-5131(17)30038-4/sref19http://www.controlled-trials.com/ISRCTN57825419/http://www.controlled-trials.com/ISRCTN57825419/http://refhub.elsevier.com/S1477-5131(17)30038-4/sref21http://refhub.elsevier.com/S1477-5131(17)30038-4/sref21http://refhub.elsevier.com/S1477-5131(17)30038-4/sref21http://refhub.elsevier.com/S1477-5131(17)30038-4/sref21http://refhub.elsevier.com/S1477-5131(17)30038-4/sref22http://refhub.elsevier.com/S1477-5131(17)30038-4/sref22http://refhub.elsevier.com/S1477-5131(17)30038-4/sref22http://refhub.elsevier.com/S1477-5131(17)30038-4/sref22http://refhub.elsevier.com/S1477-5131(17)30038-4/sref23http://refhub.elsevier.com/S1477-5131(17)30038-4/sref23http://refhub.elsevier.com/S1477-5131(17)30038-4/sref23http://refhub.elsevier.com/S1477-5131(17)30038-4/sref24http://refhub.elsevier.com/S1477-5131(17)30038-4/sref24http://refhub.elsevier.com/S1477-5131(17)30038-4/sref24http://refhub.elsevier.com/S1477-5131(17)30038-4/sref24http://refhub.elsevier.com/S1477-5131(17)30038-4/sref25http://refhub.elsevier.com/S1477-5131(17)30038-4/sref25http://refhub.elsevier.com/S1477-5131(17)30038-4/sref25http://refhub.elsevier.com/S1477-5131(17)30038-4/sref25http://refhub.elsevier.com/S1477-5131(17)30038-4/sref26http://refhub.elsevier.com/S1477-5131(17)30038-4/sref26http://refhub.elsevier.com/S1477-5131(17)30038-4/sref26http://refhub.elsevier.com/S1477-5131(17)30038-4/sref26http://refhub.elsevier.com/S1477-5131(17)30038-4/sref27http://refhub.elsevier.com/S1477-5131(17)30038-4/sref27http://refhub.elsevier.com/S1477-5131(17)30038-4/sref27http://refhub.elsevier.com/S1477-5131(17)30038-4/sref27http://refhub.elsevier.com/S1477-5131(17)30038-4/sref28http://refhub.elsevier.com/S1477-5131(17)30038-4/sref28http://refhub.elsevier.com/S1477-5131(17)30038-4/sref28http://refhub.elsevier.com/S1477-5131(17)30038-4/sref28http://refhub.elsevier.com/S1477-5131(17)30038-4/sref29http://refhub.elsevier.com/S1477-5131(17)30038-4/sref29http://refhub.elsevier.com/S1477-5131(17)30038-4/sref29http://refhub.elsevier.com/S1477-5131(17)30038-4/sref29
-
305.e6 D.J.B. Keene, R.M. Cervellione
[30] Zaupa P, Mayr J, Höllwarth ME. Antegrade scrotal
sclero-therapy for treating primary varicocele in children. BJU
Int2006;97:809e12.
[31] Hassan JM, Adams MC, Pope JC, Demarco RT, Brock JW.
Hydro-cele formation following laparoscopic varicocelectomy. J
Urol2006;175:1076e9.
[32] Harel M, Herbst KW, Nelson E. Practice patterns in the
surgicalapproach for adolescent varicocelectomy. SpringerPlus
2015;4:772.
[33] Keene DJ, Cervellione RM. Intravenous methylene
bluevenography during laparoscopic paediatric varicocelectomy.
JPediatr Surg 2014;49:308e11. discussion 311.
[34] http://www.Aethoxysklerol-international.com/foam/.[35] Rabe
E, Otto J, Schliephake D, Pannier F. Efficacy and
safety of great saphenous vein sclerotherapy using stand-ardised
polidocanol foam (ESAF): a randomised controlledmulticentre
clinical trial. Eur J Vas Endovasc Surg 2008;35:238e45.
http://refhub.elsevier.com/S1477-5131(17)30038-4/sref30http://refhub.elsevier.com/S1477-5131(17)30038-4/sref30http://refhub.elsevier.com/S1477-5131(17)30038-4/sref30http://refhub.elsevier.com/S1477-5131(17)30038-4/sref30http://refhub.elsevier.com/S1477-5131(17)30038-4/sref31http://refhub.elsevier.com/S1477-5131(17)30038-4/sref31http://refhub.elsevier.com/S1477-5131(17)30038-4/sref31http://refhub.elsevier.com/S1477-5131(17)30038-4/sref31http://refhub.elsevier.com/S1477-5131(17)30038-4/sref32http://refhub.elsevier.com/S1477-5131(17)30038-4/sref32http://refhub.elsevier.com/S1477-5131(17)30038-4/sref32http://refhub.elsevier.com/S1477-5131(17)30038-4/sref33http://refhub.elsevier.com/S1477-5131(17)30038-4/sref33http://refhub.elsevier.com/S1477-5131(17)30038-4/sref33http://refhub.elsevier.com/S1477-5131(17)30038-4/sref33http://www.Aethoxysklerol-international.com/foam/http://refhub.elsevier.com/S1477-5131(17)30038-4/sref35http://refhub.elsevier.com/S1477-5131(17)30038-4/sref35http://refhub.elsevier.com/S1477-5131(17)30038-4/sref35http://refhub.elsevier.com/S1477-5131(17)30038-4/sref35http://refhub.elsevier.com/S1477-5131(17)30038-4/sref35http://refhub.elsevier.com/S1477-5131(17)30038-4/sref35
Antegrade sclerotherapy in adolescent varicocele
patientsIntroductionMethodsResultsDiscussionConclusionConflict of
interest statementFunding sourceEthical approvalReferences