Embed Size (px)
Citation preview
www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2010) 45, 213–219
Antegrade colonic enemas and intestinal diversion arehighly effective in the management of children withintractable constipationEmily R. Christison-Lagaya, Leonel Rodriguezb, Michael Kurtza, Kristin St. Pierrec,Daniel P. Doodyc, Allan M. Goldsteinc,⁎
aDepartment of Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114, USAbDepartment of Pediatric Gastroenterology, Children's Hospital, Boston, MA 02115, USAcDepartment of Pediatric Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114, USA
Received 5 October 2009; accepted 6 October 2009
0d
Key words:Constipation;Colonic dysmotility;Ileostomy;Colostomy;Antegrade colonic enemas;Colectomy
AbstractPurpose: Intractable constipation in children is an uncommon but debilitating condition. When medicaltherapy fails, surgery is warranted; but the optimal surgical approach has not been clearly defined. Wereviewed our experience with operative management of intractable constipation to identify predictors ofsuccess and to compare outcomes after 3 surgical approaches: antegrade continence enema (ACE),enteral diversion, and primary resection.Methods: A retrospective review of pediatric patients undergoing ACE, diversion, or resection forintractable, idiopathic constipation from 1994 to 2007 was performed. Satisfactory outcome was definedas minimal fecal soiling and passage of stool at least every other day (ACE, resection) or functionalenterostomy without abdominal distension (diversion).Results: Forty-four patients (range = 1-26 years, mean = 9 years) were included. Sixteen patientsunderwent ACE, 19 underwent primary diversion (5 ileostomy, 14 colostomy), and 9 had primarycolonic resections. Satisfactory outcomes were achieved in 63%, 95%, and 22%, respectively. Of the19 patients diverted, 14 had intestinal continuity reestablished at a mean of 27 months postdiversion,with all of these having a satisfactory outcome at an average follow-up of 56 months. Five patientsunderwent closure of the enterostomy without resection, whereas the remainder underwent resectionof dysmotile colon based on preoperative colonic manometry studies. Of those undergoing ACEprocedures, age younger than 12 years was a predictor of success, whereas preoperative colonicmanometry was not predictive of outcome. Second manometry 1 year post-ACE showedimprovement in all patients tested. On retrospective review, patient noncompliance contributed toACE failure.
Presented at the 40th Annual Meeting of the American Pediatric Surgical Association, Fajardo, Puerto Rico, May 28-June 1, 2009.⁎ Corresponding author. Tel.: +1 617 726 0270; fax: +1 617 726 2167.E-mail address: [email protected] (A.M. Goldstein).
022-3468/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2009.10.034

214 E.R. Christison-Lagay et al.
Conclusions: Antegrade continence enema and enteral diversion are very effective initial procedures in themanagement of intractable constipation. Greater than 90% of diverted patients have an excellent outcomeafter the eventual restoration of intestinal continuity. Colon resection should not be offered as initialtherapy, as it is associated with nearly 80% failure rate and the frequent need for additional surgery.© 2010 Elsevier Inc. All rights reserved.
Severe constipation can present a formidable management Subjects met the criteria for functional constipation as
Table 1 Diagnostic criteria for functional constipation
Must include 2 or more of the following in a child with adevelopmental age of at least 4 y with insufficient criteria for a
problem. Most cases of constipation, a condition thataccounts for 25% of pediatric gastroenterology evaluations,respond to diet modification or medications. In theremainder, where the child has medically refractoryconstipation, treatment options are limited. Fortunately,these cases are infrequent. Affected children often experi-ence chronic abdominal pain and bloating, fecal inconti-nence, frequent hospitalizations, and social withdrawal. Forthese cases, surgical management options need to beconsidered. Unfortunately, the relative effectiveness of thevarious surgical options is currently unknown. Althoughmany studies have examined the outcomes after variousoperations in the treatment of chronic idiopathic constipationin adults [1,2], few have systematically explored this issue inchildren. The purpose of this study is to identify the mosteffective surgical approaches for the management of severeconstipation in young patients.
Intractable constipation in children can result from avariety of causes, including colonic dysmotility, functionaldisorders of the anorectum, abnormalities of the pelvic floor,and behavioral disorders. A thorough evaluation is critical totarget therapy appropriately. The workup often includesimaging to rule out mechanical obstruction and to assess fordilatation of the bowel, and a variety of functional assays,including anorectal manometry, sitz marker studies, colonicmotility, and defecography, tailored to the child's symptoms.However, despite complete assessment, many cases remainidiopathic. Even in cases where colonic dysmotility isidentified, no specific treatment is available. In all of thesecases, achieving colonic evacuation is essential to minimizethe symptoms of constipation and allow the child to regain anormal life.
Several surgical options have been described for themanagement of intractable constipation in children. Theseinclude colonic resection [3], intestinal diversion [4], andantegrade colonic enema (ACE) [5,6]. We reviewed ourexperience using these different approaches and find thatdiversion and ACE are both very effective in achieving goodfunctional outcomes, whereas the results after resection arehighly variable and often poor.
diagnosis of irritable bowel syndrome:1. Two or fewer defecations in the toilet per week2. At least 1 episode of fecal incontinence per week3. History of retentive posturing or excessive volitional stoolretention4. History of painful or hard bowel movements5. Presence of a large fecal mass in the rectum6. History of large diameter stools that may obstruct the toilet
1. Methods
We performed a retrospective review of all patients treatedsurgically for intractable constipation by the Department ofPediatric Surgery at MassGeneral Hospital for Children.
defined by Rome III (Table 1) and for intractableconstipation, defined as failure to respond to conventionaltherapy as described by the North American Society ofPediatric Gastroenterology and Nutrition [7,8]. Childrenyounger than 4 years (n = 5), who cannot strictly meet RomeIII criteria, had encopresis and 2 or fewer defecations perweek. After obtaining Institutional Review Board approval,44 subjects were identified as having had an operation to treatconstipation in the period from 1994 to 2007. The age ofsubjects ranged from 1 to 26 years at the time of the initialoperation. All ileostomies, colostomies, bowel resections,appendicostomies, and cecostomies performed for intractableconstipation were included. Length of follow-up was aminimum of 3 months. Patients were excluded if they hadHirschsprung disease, anorectal malformation, mechanicalobstruction, or inadequate follow-up.
Preoperative evaluation included anorectal manometry(ARM) to exclude anal achalasia or a hypertonic analsphincter as the cause of constipation. Those with abnormalARM underwent botulinum toxin injection of the internalanal sphincter, as previously described [9]. Those who didnot respond to botox and underwent additional surgery fortheir constipation were included in this study (n = 9).Children with normal ARM or those failing to respond tobotulinum toxin injection typically underwent colonicmotility studies (30 of 44, 68%) or sitz marker studies.Other imaging studies, such as barium enema, were oftenperformed as well, depending on the preference of thereferring gastroenterologist and the surgeon. Rectal biopsywas always done as part of the initial workup to excludeHirschsprung disease.
Age at procedure, sex, type of operation, results ofpreoperative studies, clinical and psychiatric diagnoses,pathologic diagnoses, postoperative continence status andstool frequency, and need for subsequent procedures were
Table 2 Patient demographics
No. of patients 44SexMale 19Female 25
Mean age (range) 9 (1-26)Initial procedureACE 16Diversion 19Resection 9
Crossover patients a 26Requiring N2 procedures 6Neurologically impaired 8
a Refers to subjects requiring a second operation, excluding stomareversal.
215Management of children with intractable constipation
recorded. All patients were followed primarily by a pediatricgastroenterologist with a special focus in intestinal motility.Selection of operative procedure was guided by the surgeonand the gastroenterologist based on the preoperative workupand personal experience. No standardized algorithm wasused during the course of this retrospective study. The ACEprocedures included appendicostomy or cecostomy, thelatter being performed either openly or laparoscopically,with or without endoscopic assistance. Intestinal diversionincluded ileostomy or colostomy. Colonic resection variedfrom segmental resection to total abdominal proctocolect-omy with ileoanal anastomosis.
Outcomes were deemed “favorable” if patients stooled atleast every 2 days with minimal or no soiling after resectionor ACE, or had regular stomal output without abdominaldistension after diversion. Quality of life was assessed usingthe Pediatric Quality of Life Inventory (PedsQL), a validatedquestionnaire assessing gastrointestinal symptoms as well associal, physical, and emotional performance according to the
Table 3 Clinical outcome after surgical treatment of intractable cons
Primary procedure Satisfactoryoutcome
Age (y)(range)
Follow-up (or ti2nd operation) (
ACE (n = 16) 10 (63%) 10 (3-17) 19 (6-45)Satisfactory (n = 10) 8 (3-14) 23 (12-45)Unsatisfactory (n = 6) 12 (5-17) 12 (6-15)
Diversion (n = 19) 18 (95%) 8 (1-21) 24 (6-60)Satisfactory (n = 18) 8 (1-21)
Unsatisfactory (n = 1) 16
Resection (n = 9) 2 (22%) 9 (1-17) 39 (5-168)Satisfactory (n = 2) 11 (7,15)Unsatisfactory (n = 7) 9 (1-17)
NA indicates not applicable.
child and caregiver [10]. Scores were derived from thereports by linear transformation to a 0 to 100 scale, with 100indicating the best possible quality of life. Caregiver andpatient scores were recorded separately. Statistical compar-ison of these results was made using 2-tailed Student's t test.
2. Results
A total of 44 subjects were identified as having undergonea surgical procedure for treatment of intractable constipation.Subject demographics are described in Table 2, and clinicaloutcomes are summarized in Table 3. Follow-up wasavailable on all children with a range of 3 to 108 months.Three categories of surgical intervention were performed:ACE procedure, diversion, and primary resection withanastomosis. A satisfactory outcome was defined as minimalor no fecal soiling and passage of stool at least every otherday (ACE, resection) or functional enterostomy withoutabdominal distension (diversion).
2.1. ACE procedure
Sixteen children underwent an ACE procedure, including3 appendicostomies, 2 open cecostomies, and 11 laparo-scopic cecostomies with endoscopic assistance. A satisfac-tory clinical outcome was observed in 10 (63%) of all ACEpatients, with an average length of follow-up of 23 months.Although preoperative colonic manometry was not predic-tive of outcome, our practice has been to recommenddiversion over ACE in children with colonic inertia,potentially biasing these results. Antegrade colonic enemaswere initiated 1 week after the procedure and consisted ofdaily polyethylene glycol-electrolyte solution. All patientswere still using antegrade enemas at the time of follow-up,
tipation
me tomo) (range)
Secondaryprocedure(s)
Secondary outcome
None NA4 2 well post resection
1 well diverted1 resected, then diverted,now well
Reversal: 4Resection: 9
4 of 4 well7 of 9 well
1 Reversal, then resection twice,now improved
None NADiversion: 2Re-resection: 2
2 of 2 well0 of 2 well

216 E.R. Christison-Lagay et al.
although some had successfully weaned the frequency to lessthan daily. Of the 6 subjects with an unsatisfactory outcomeowing to persistent constipation, 4 underwent a subsequentsurgical procedure after an average of 13 months: 2 hadcolonic resections with primary reanastomosis, and 2underwent diversion. The average age of children achievingsatisfactory results after ACE was 8 years (range, 3-14),whereas the average age of children with unsatisfactoryresults was 12 years (range, 5-17) (P = .08), suggesting atrend but not achieving statistical significance. Lack ofcooperation among teenage patients in administering theenemas was identified by caregivers as sometimes contrib-uting to ACE failure. Six patients with a satisfactory outcomeunderwent postprocedural colorectal manometry at anaverage follow-up period of 1 year. All 6 demonstratedimproved colonic motility with the presence of a gastrocolicresponse and at least partial propagation of high-amplitudepropagating contractions (HAPCs). In all but 1 patient, thatfinding correlated with successful decrease of enema use.Complications occurred after the ACE procedure in 1 patient,who required revision of the cecostomy.
2.2. Intestinal diversion
Nineteen children underwent primary diversion, including5 ileostomies, 8 transverse colostomies, and 6 sigmoidcolostomies. A satisfactory outcome after diversion wasachieved in 18 (95%) patients. Fourteen patients subsequent-ly had continuity reestablished after a mean duration of 27months (range, 6-60 months). Five of these patients had asimple colostomy or ileostomy reversal without additionalcolonic resection. All of these patients had demonstratedrestoration of normal colonic motility on postdiversionmanometry or colonic transit studies before the stomareversal. Four of these have done well, whereas 1 developedrecurrent constipation, required 2 resections, and now has asatisfactory outcome. The remaining 9 children who have hadclosure of their stoma had a concomitant left colectomy at thetime of their stoma reversal. These children demonstratedrestoration of right-sided colonic motility with persistent left-sided dysmotility on preoperative manometry. Of these 9, 2required rediversion for recurrent constipation, although 1was able to have continuity reestablished at a fourthoperation. Average length of follow-up on all patientsundergoing reestablishment of continuity was 56 months(range, 8-108months) after stoma reversal. Overall, diversionwas associated with a larger number of long-term complica-tions than ACE, most notably stomal prolapse. Of the 19children undergoing primary diversion, 5 (26%) requiredstoma revision for prolapse, all of these occurring withcolostomies and none with ileostomies.
The single patient with an unsatisfactory outcome in thediverted group had pervasive developmental delay andpersistent constipation despite a sigmoid colostomy. Transitstudies in this patient demonstrated poor motility through thetransverse and descending colon. She subsequently under-
went a subtotal colectomy with a cecorectal anastomosis.However, she continued to have constipation and ultimatelyunderwent proctectomy with ileoanal anastomosis, with asatisfactory outcome at 54 months of follow-up.
2.3. Colonic resection
Primary resection was performed in 9 patients with asatisfactory outcome in only 2 (22%). Colonic manometryresults were available and abnormal in 2 subjects, whereassitz marker passage was delayed in another 6 subjects. Of the7 subjects with a clinically unsatisfactory outcome, persistentconstipation was present in 4 and fecal incontinence occurredin 3, each with a coloanal anastomosis performed 1 to 2 cmabove the dentate line. Three of the patients with continuedconstipation and 1 with fecal incontinence underwentreoperation. Two of these patients subsequently experienceddebilitating incontinence, with 1 ultimately requiring intes-tinal diversion. A third child has intermittent incontinence,and the fourth is diverted. Seven of 9 patients initiallyunderwent coloanal anastomosis. The 2 children with acolorectal anastomosis were among those with persistentconstipation after resection. Average age of patientsundergoing primary resection was 9 years. The 2 satisfactoryoutcomes occurred in a 7-year-old and a 15-year-old, both ofwhom underwent rectosigmoid resection with pull-throughprocedures. The average duration of follow-up for allresection patients was 52 months (range, 11-96 months).
2.4. Histology
Histologic evaluation of rectal or colonic biopsies wasperformed in all patients, except for 3 of those undergoingACE. Intestinal neuronal dysplasia (IND), defined byhyperganglionosis and giant ganglia, was diagnosed in 1 of13 ACE patients, 8 of 19 children undergoing diversion, and4 of 9 children undergoing resection. Hypoganglionosis wasdiagnosed in 0 of 13 ACEs, 1 of 19 diversions, and 3 of 9resections. We examined the data and found that histologydid not correlate with manometry results nor was it predictiveof clinical outcome. For example, of the 18 diverted subjectswho did well, 8 had IND, 1 had hypoganglionosis, and 9 hadnormal histology. Of the 7 patients who did poorly aftercolonic resection, 4 had IND, 2 had hypoganglionosis, and 1had normal histology. The small numbers of subjects andretrospective nature of the study limit statistical analysis ofthese histology results.
2.5. Colonic manometry
Preoperative colon manometry was performed in 15 of 16children undergoing ACE, 13 of 19 subjects that werediverted, and 2 of 9 subjects undergoing resection. In theACE group, 3 patients had normal preoperative manometry;and 2 of these had poor outcomes. Nine children had
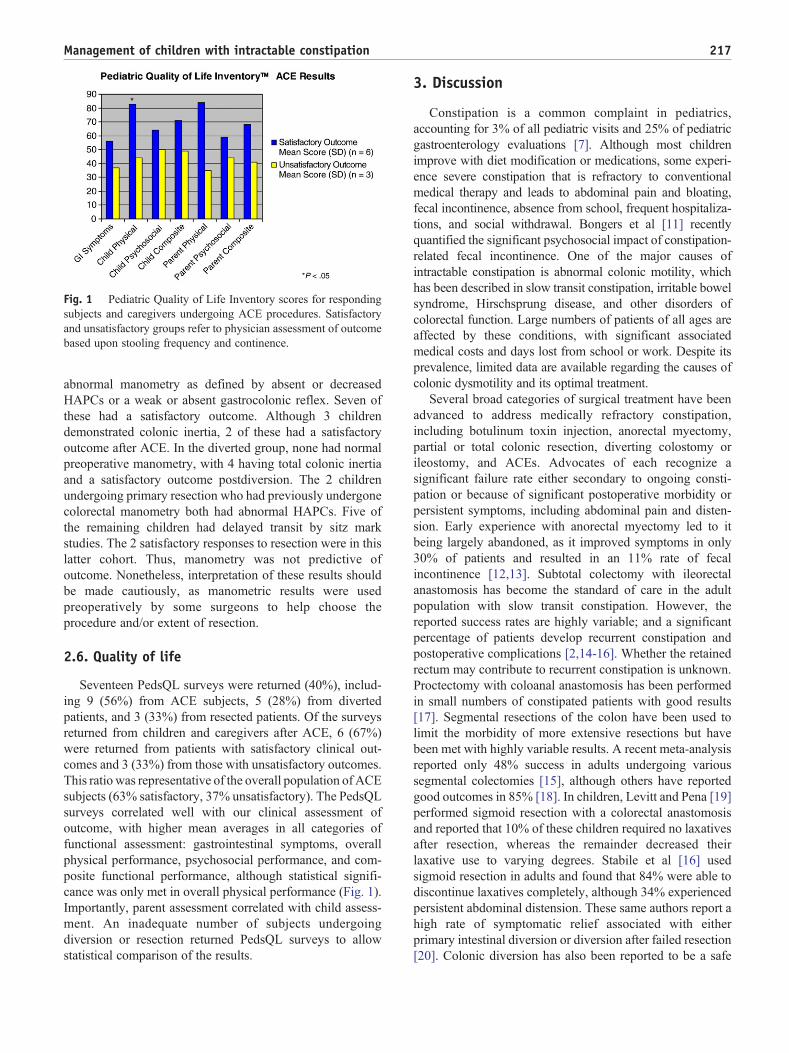
Fig. 1 Pediatric Quality of Life Inventory scores for respondingsubjects and caregivers undergoing ACE procedures. Satisfactoryand unsatisfactory groups refer to physician assessment of outcomebased upon stooling frequency and continence.
217Management of children with intractable constipation
abnormal manometry as defined by absent or decreasedHAPCs or a weak or absent gastrocolonic reflex. Seven ofthese had a satisfactory outcome. Although 3 childrendemonstrated colonic inertia, 2 of these had a satisfactoryoutcome after ACE. In the diverted group, none had normalpreoperative manometry, with 4 having total colonic inertiaand a satisfactory outcome postdiversion. The 2 childrenundergoing primary resection who had previously undergonecolorectal manometry both had abnormal HAPCs. Five ofthe remaining children had delayed transit by sitz markstudies. The 2 satisfactory responses to resection were in thislatter cohort. Thus, manometry was not predictive ofoutcome. Nonetheless, interpretation of these results shouldbe made cautiously, as manometric results were usedpreoperatively by some surgeons to help choose theprocedure and/or extent of resection.
2.6. Quality of life
Seventeen PedsQL surveys were returned (40%), includ-ing 9 (56%) from ACE subjects, 5 (28%) from divertedpatients, and 3 (33%) from resected patients. Of the surveysreturned from children and caregivers after ACE, 6 (67%)were returned from patients with satisfactory clinical out-comes and 3 (33%) from those with unsatisfactory outcomes.This ratio was representative of the overall population of ACEsubjects (63% satisfactory, 37% unsatisfactory). The PedsQLsurveys correlated well with our clinical assessment ofoutcome, with higher mean averages in all categories offunctional assessment: gastrointestinal symptoms, overallphysical performance, psychosocial performance, and com-posite functional performance, although statistical signifi-cance was only met in overall physical performance (Fig. 1).Importantly, parent assessment correlated with child assess-ment. An inadequate number of subjects undergoingdiversion or resection returned PedsQL surveys to allowstatistical comparison of the results.
3. Discussion
Constipation is a common complaint in pediatrics,accounting for 3% of all pediatric visits and 25% of pediatricgastroenterology evaluations [7]. Although most childrenimprove with diet modification or medications, some experi-ence severe constipation that is refractory to conventionalmedical therapy and leads to abdominal pain and bloating,fecal incontinence, absence from school, frequent hospitaliza-tions, and social withdrawal. Bongers et al [11] recentlyquantified the significant psychosocial impact of constipation-related fecal incontinence. One of the major causes ofintractable constipation is abnormal colonic motility, whichhas been described in slow transit constipation, irritable bowelsyndrome, Hirschsprung disease, and other disorders ofcolorectal function. Large numbers of patients of all ages areaffected by these conditions, with significant associatedmedical costs and days lost from school or work. Despite itsprevalence, limited data are available regarding the causes ofcolonic dysmotility and its optimal treatment.
Several broad categories of surgical treatment have beenadvanced to address medically refractory constipation,including botulinum toxin injection, anorectal myectomy,partial or total colonic resection, diverting colostomy orileostomy, and ACEs. Advocates of each recognize asignificant failure rate either secondary to ongoing consti-pation or because of significant postoperative morbidity orpersistent symptoms, including abdominal pain and disten-sion. Early experience with anorectal myectomy led to itbeing largely abandoned, as it improved symptoms in only30% of patients and resulted in an 11% rate of fecalincontinence [12,13]. Subtotal colectomy with ileorectalanastomosis has become the standard of care in the adultpopulation with slow transit constipation. However, thereported success rates are highly variable; and a significantpercentage of patients develop recurrent constipation andpostoperative complications [2,14-16]. Whether the retainedrectum may contribute to recurrent constipation is unknown.Proctectomy with coloanal anastomosis has been performedin small numbers of constipated patients with good results[17]. Segmental resections of the colon have been used tolimit the morbidity of more extensive resections but havebeen met with highly variable results. A recent meta-analysisreported only 48% success in adults undergoing varioussegmental colectomies [15], although others have reportedgood outcomes in 85% [18]. In children, Levitt and Pena [19]performed sigmoid resection with a colorectal anastomosisand reported that 10% of these children required no laxativesafter resection, whereas the remainder decreased theirlaxative use to varying degrees. Stabile et al [16] usedsigmoid resection in adults and found that 84% were able todiscontinue laxatives completely, although 34% experiencedpersistent abdominal distension. These same authors report ahigh rate of symptomatic relief associated with eitherprimary intestinal diversion or diversion after failed resection[20]. Colonic diversion has also been reported to be a safe

218 E.R. Christison-Lagay et al.
and effective alternative in children by Villarreal et al [4],who reported resolution of constipation in a group of 12children with idiopathic constipation and megacolon under-going colostomy or ileostomy. Greater than 90% of thesepatients had resolution of bowel dilatation after diversion,and 75% had improvement in colonic contractility by colonicmanometry. All children had eventual restoration ofcontinuity, with only 1 patient experiencing ongoingconstipation [4]. Woodward et al [13] similarly reportedsuccessful treatment of constipation by colostomy in 10children, but had less success in reestablishing continuity inthis population. In adults, diversion of the fecal stream hasbeen reported to be effective in 65% of patients [15].
The Malone ACE was initially described in 1990 as amethod of colonic irrigation that avoids the emotionaldistress associated with repeated retrograde enemas [21].Many modifications of the procedure have been described,with antegrade conduits now often created as laparoscopicbutton cecostomies. Success in functional constipation withantegrade enemas has been reported in 40% to 81% of bothpediatric and adult patients [5,22-25], similar to our results.The presence of HAPCs in the colon and a normal HAPCresponse after stimulation with bisacodyl have beensuggested to be predictive of ACE success [26].
Our study compares the outcomes of children withidiopathic intractable constipation treated by ACE, diversion,or resection to identify an optimal treatment paradigm oralgorithm for this notoriously difficult population. Interest-ingly, the choice of surgical procedure changed over the studyperiod, with resection predominating as the treatment ofchoice over the early years of enrollment, diversion favored inthe middle years, and ACE favored as an initial approachmore recently. Part of the reason for this shift was that primaryresection was associated with a low rate of success. Childrenreconstructed with a colorectal anastomosis were notablyconstipated postoperatively, whereas those undergoing acoloanal anastomosis often had either ongoing constipationor fecal incontinence. Only 22% of resected patientsexhibited normal defecation patterns, and 44% requiredmore than one procedure. In patients with capacious, dilatedcolons, a secondary enteropathy may occur because ofincreased colonic wall tension. Moreover, in patients withchronic rectal dilatation, there is often loss of the normalrectoanal inhibitory reflex that facilitates defecation. Primaryresection with colorectal anastomosis, although it mayremove dysmotile colon, does not address either extendedsecondary colonic dysmotility or impaired rectal sensation,both of which may contribute to ongoing constipation. Incontrast, proximal diversion allows for colonic rest. Afterdiversion, the defunctionalized distal bowel has the oppor-tunity to return to normal caliber over time, potentiallyallowing for return of colonic motility. Moreover, the absenceof a high-pressure sphincter also theoretically allows bowelproximal to the ostomy to rest. We found that thedecompressed colon often demonstrates improved contrac-tility in postoperative motility studies. Moreover, sustained
evacuation of the rectal vault seems to permit it to reset itsresting volume, although studies by van den Berg et al [6]suggest that it never reaches the size of normal volunteers.
Intestinal diversion was associated with a high degree ofsuccess. It not only reduced abdominal symptoms andeliminated encopresis, but more than three quarters of thosediverted had continuity successfully reestablished withnegligible constipation or incontinence. Of the 5 patients inour cohort who remain diverted, one was lost to follow-upafter 3 months, 2 have pervasive neurologic disorders andsmall bowel dysmotility, and 1 has been diverted for only 15months. This child has normalization of colonic motility bymanometry and has a scheduled operative date for ostomyreversal. As a treatment of constipation, diversion isoverwhelmingly successful. However, its success in treatingconstipation needs to be balanced against the risk of stomalprolapse and the potential psychosocial impact of a stoma inschool-aged children.
Based on our results, ACE appears to be an appropriatefirst-line treatment for many children with medically intrac-table constipation. In our population, ACE was associatedwith a success rate of nearly 70%, with only 1 complicationrequiring surgical revision. Importantly, quality of life scoresdemonstrate that physician assessment of a satisfactoryclinical outcome correlates with patient and family satisfactionin terms of both psychosocial and gastrointestinal function.The antegrade enema regimen can be tailored to each child'sspecific needs and weaned as tolerated. Although preoperativecolonic manometry was not found to correlate with ACEsuccess, this retrospective study may have inherent patientselection bias. In patients who either fail ACE or are felt not tobe good candidates, diversion should be offered as the nextsurgical alternative. The outcomes of diversion after ACEshould be as good as those after diversion as the initialoperation. In our experience, in addition to improvement ingastrointestinal symptoms after ACE or diversion, manychildren also exhibit improved social performance and weightgain. Further studies on the surgical treatment of thesechallenging patients, and on the psychosocial and physicalimpacts of these interventions, are warranted.
Acknowledgments
We thank Julie Piotrowski, PNP, and CarenHarris, PNP, fortheir expert care of these patients. We are grateful to the MAPIResearch Trust for providing the PedsQL surveys. AMG issupported by National Institutes of Health R01DK080914.
References
[1] Pfeifer J, Agachan F, Wexner SD. Surgery for constipation: a review.Dis Colon Rectum 1996;39(4):444-60.
[2] Knowles CH, Scott M, Lunniss PJ. Outcome of colectomy for slowtransit constipation. Ann Surg 1999;230(5):627-38.
219Management of children with intractable constipation
[3] Platell C, Scache D, Mumme G, et al. A long-term follow-up ofpatients undergoing colectomy for chronic idiopathic constipation.Aust N Z J Surg 1996;66(8):525-9.
[4] Villarreal J, Sood M, Zangen T, et al. Colonic diversion for intractableconstipation in children: colonic manometry helps guide clinicaldecisions. J Pediatr Gastroenterol Nutr 2001;33(5):588-91.
[5] Wong AL, Kravarusic D, Wong SL. Impact of cecostomy andantegrade colonic enemas on management of fecal incontinence andconstipation: ten years of experience in pediatric population. J PediatrSurg 2008;43(8):1445-51.
[6] van den Berg MM, Voskuijl WP, Boeckxstaens GE, et al. Rectalcompliance and rectal sensation in constipated adolescents, recoveredadolescents and healthy volunteers. Gut 2008;57(5):599-603.
[7] Baker SS, Liptak GS, Colletti RB, et al. Constipation in infants andchildren: evaluation and treatment. A medical position statement of theNorth American Society for Pediatric Gastroenterology and Nutrition.J Pediatr Gastroenterol Nutr 1999;29(5):612-26.
[8] Rasquin A, Di Lorenzo C, Forbes D, et al. Childhood functionalgastrointestinal disorders: child/adolescent. Gastroenterology2006;130(5):1527-37.
[9] Irani K, Rodriguez L, Doody DP, et al. Botulinum toxin for thetreatment of chronic constipation in children with internal analsphincter dysfunction. Pediatr Surg Int 2008;24(7):779-83.
[10] Varni JW, Seid M, Rode CA. The PedsQL: measurement model for thepediatric quality of life inventory. Med Care 1999;37(2):126-39.
[11] Bongers ME, van Dijk M, Benninga MA, et al. Health related qualityof life in children with constipation-associated fecal incontinence.J Pediatr 2009.
[12] Pinho M, Yoshioka K, Keighley MR. Long-term results of anorectalmyectomy for chronic constipation. Dis Colon Rectum 1990;33(9):795-7.
[13] Woodward MN, Foley P, Cusick EL. Colostomy for treatment offunctional constipation in children: a preliminary report. J PediatrGastroenterol Nutr 2004;38(1):75-8.
[14] Mollen RM, Kuijpers HC, Claassen AT. Colectomy for slow-transitconstipation: preoperative functional evaluation is important but not aguarantee for a successful outcome. Dis Colon Rectum 2001;44(4):577-80.
[15] Gladman MA, Scott SM, Lunniss PJ, et al. Systematic review ofsurgical options for idiopathic megarectum and megacolon. Ann Surg2005;241(4):562-74.
[16] Stabile G, Kamm MA, Hawley PR, et al. Colectomy for idiopathicmegarectum and megacolon. Gut 1991;32(12):1538-40.
[17] Stabile G, Kamm MA, Phillips RK, et al. Partial colectomy andcoloanal anastomosis for idiopathic megarectum and megacolon. DisColon Rectum 1992;35(2):158-62.
[18] Lundin E, Karlbom U, Pahlman L, et al. Outcome of segmental colonicresection for slow-transit constipation. Br J Surg 2002;89(10):1270-4.
[19] Levitt MA, Pena A. Surgery and constipation: when, how, yes, or no?J Pediatr Gastroenterol Nutr 2005;41(Suppl 1):S58-60.
[20] Stabile G, Kamm MA, Hawley PR, et al. Results of stoma formationfor idiopathic megarectum and megacolon. Int J Colorectal Dis1992;7(2):82-4.
[21] Malone PS, Curry JI, Osborne A. The antegrade continenceenema procedure why, when and how? World J Urol 1998;16(4):274-8.
[22] Curry JI, Osborne A, Malone PS. How to achieve a successful Maloneantegrade continence enema. J Pediatr Surg 1998;33(1):138-41.
[23] Curry JI, Osborne A, Malone PS. The MACE procedure: experience inthe United Kingdom. J Pediatr Surg 1999;34(2):338-40.
[24] Poirier M, Abcarian H, Nelson R. Malone antegrade continent enema:an alternative to resection in severe defecation disorders. Dis ColonRectum 2007;50(1):22-8.
[25] King SK, Sutcliffe JR, Southwell BR, et al. The antegrade continenceenema successfully treats idiopathic slow-transit constipation. J PediatrSurg 2005;40(12):1935-40.
[26] van den Berg MM, Hogan M, Caniano DA, et al. Colonic manometryas predictor of cecostomy success in children with defecationdisorders. J Pediatr Surg 2006;41(4):730-6.
Discussion
Marc Levitt, MD (Cincinnati, OH): Your first imageshowed a typical megarectosigmoid, and I am curious toknow how many of your patients had that image, becauseyour treatments of ACE, diversion, or colonic resectiontransabdominally—none of them treat the problem,which is the rectum. Perhaps if the rectum was removed,perhaps transanally, that would solve the problem.
Can you also comment on your lack of success withACE? ACE is enemas. It is really reserved for patientswho are fecally incontinent. These patients have an intactcontinence mechanism. Why wouldn't they be treated bymore aggressive laxative therapy?
Emily R. Christison-Lagay, MD (Boston, MA): We did notspecifically image all of the patients in this study, whichwas a total of 44; however, I would say in reconsideringthe data, the vast majority had megarectum or would havea CT or KUB findings that were consistent with those Ishowed, though we did not specifically look at those ascriteria for including these patients in the study.
In terms of the role of ACE, we have used ACE to treatconstipation for patients who have failed primary laxativemanagement or primary management with enemas givenrectally. We have not found that the success rate of ACEis actually predicted as other groups have found bypreoperative colonic motility studies, preoperative colo-nic manometry, with some patients with total colonicinertia doing well with ACE and some patients withapparently normal motility doing poorly with ACE.
Brian Gilchrist, MD (Boston, MA): I curious as to whyyou have not mentioned the pathology. Did any ofthese children have mitochondrial disease or neuroin-testinal dysplasia?
Dr Christison-Lagay: It was just a limitation of time thatprevented us from including that data. We found nostatistical difference between the pathology in any of thegroups, with approximately 30% of patients beingcategorized as having neurointestinal dysplasia andapproximately 20% having hypoganglionosis. However,those findings did not segregate between groups.