Embed Size (px)
Citation preview

Animal models of gastrointestinal and liver diseases. Animal models ofnecrotizing enterocolitis: pathophysiology, translational relevance,and challenges
Peng Lu,1 Chhinder P. Sodhi,1 Hongpeng Jia,1 Shahab Shaffiey,1 Misty Good,3 Maria F. Branca,1
and David J. Hackam1,2
1Department of Surgery, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania; 2Division of PediatricSurgery, Children’s Hospital of Pittsburgh of UPMC, Pittsburgh, Pennsylvania; 3Division of Newborn Medicine, Departmentof Pediatrics, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania
Submitted 9 December 2013; accepted in final form 18 April 2014
Lu P, Sodhi CP, Jia H, Shaffiey S, Good M, Branca MF,Hackam DJ. Animal models of gastrointestinal and liver diseases.Animal models of necrotizing enterocolitis: pathophysiology, transla-tional relevance, and challenges. Am J Physiol Gastrointest LiverPhysiol 306: G917–G928, 2014. First published April 24, 2014;doi:10.1152/ajpgi.00422.2013.—Necrotizing enterocolitis is the lead-ing cause of morbidity and mortality from gastrointestinal disease inpremature infants and is characterized by initial feeding intoleranceand abdominal distention followed by the rapid progression to coag-ulation necrosis of the intestine and death in many cases. Although therisk factors for NEC development remain well accepted, namelypremature birth and formula feeding, the underlying mechanismsremain incompletely understood. Current thinking indicates that NECdevelops in response to an abnormal interaction between the mucosalimmune system of the premature host and an abnormal indigenousmicroflora, leading to an exaggerated mucosal inflammatory responseand impaired mesenteric perfusion. In seeking to understand themolecular and cellular events leading to NEC, various animal modelshave been developed. However, the large number and variabilitybetween the available animal models and the unique characteristics ofeach has raised important questions regarding the validity of particularmodels for NEC research. In an attempt to provide some guidance tothe growing community of NEC researchers, we now seek to reviewthe key features of the major NEC models that have been developedin mammalian and nonmammalian species and to assess the advan-tages, disadvantage, challenges and major scientific discoveriesyielded by each. A strategy for model validation is proposed, theprincipal models are compared, and future directions and challengeswithin the field of NEC research are explored.
necrotizing enterocolitis; animal model; TLR4; innate immunity;microflora
NECROTIZING ENTEROCOLITIS (NEC) is the leading cause of deathfrom gastrointestinal disease in premature infants and is nowrecognized as a major cause of morbidity in patients who arefortunate to survive the initial disease. NEC develops in �1 in1,000 live births (51), and since there were 3.95 million livebirths in 2012 according to the Centers for Disease Control andPrevention, �4,000 infants were expected to develop thisdevastating disease in the past year alone. The typical infantwith NEC is a premature child born at around 30 wk gestation,who was offered infant formula for nutrition, and who at �2–3
wk of age develops feeding intolerance, abdominal distention,and bloody stools. In approximately half of cases, the childbecomes progressively ill, with systemic sepsis and cardiovas-cular collapse requiring aggressive resuscitation. Clinical de-terioration leads to abdominal exploration in nearly 30% ofcases, where the hallmarks of NEC, i.e., death of parts or all ofthe small and/or large intestine, are encountered. Risk factorsfor NEC development include prematurity and the administra-tion of formula feeds, and treatment is relatively nonspecific,which includes a combination of broad-spectrum antibioticsand removal of the diseased intestine (78). Although a fulldescription of the clinical course and management of NEC arebeyond the scope of the present review, the current consensusindicates that the incidence of NEC is either stable or increas-ing in frequency, that the overall survival for patients with thisdisease has not changed since the initial description 30 yearsago (12, 72), and that the societal costs for patients whodevelop the disease, especially due to the long-term neurode-velopmental and intestinal effects, are enormous (33).
Insights into the pathophysiology of NEC have been gainedthrough the study of clinical specimens and the careful selec-tion and usage of animal models. Although the pathophysiol-ogy of NEC is generally agreed to be multifactorial (40, 78),our understanding of the cellular and physiological mecha-nisms that lead to NEC has changed significantly in the pastdecade or so. Initially, NEC was thought to develop as a resultof an ischemic event leading to a disruption of an immatureintestinal epithelium and mucosal barrier, which leads to bac-terial translocation and the development of systemic sepsis(77). Although this explanation could account for the presenceof intestinal epithelial disruption that is characteristic of NEC,it could not account for the presence of intestinal necrosis thatis seen in patients with this disease, nor could this explanationreadily reconcile the observation that most patients who de-velop NEC do not actually have an antecedent ischemic event(104). Previous authors have reviewed the major mechanisticfactors thought to lead to the development of NEC (46, 78),and although a thorough evaluation is beyond the scope of thepresent review, current thinking suggests that formula feedingof the premature host that is colonized with a select microbialflora leads to an enhanced cellular and innate immune responsein the context of host genetic factors and an impaired intestinalmicrovascular network, resulting in aggressive mucosal in-flammation and reduced mesenteric perfusion. The ensuingtissue death leads to a cascade of bacterial translocation,systemic sepsis, and multisystem organ failure. There are many
Address for reprint requests and other correspondence: D. J. Hackam,Division of Pediatric Surgery, Children’s Hospital of Pittsburgh of UPMC,One Children’s Hospital Dr., 4401 Penn Ave., Pittsburgh, PA 15224 (e-mail:[email protected]).
Am J Physiol Gastrointest Liver Physiol 306: G917–G928, 2014.First published April 24, 2014; doi:10.1152/ajpgi.00422.2013. Themes
0193-1857/14 Copyright © 2014 the American Physiological Societyhttp://www.ajpgi.org G917

important pathogenetic questions that remain to be answeredincluding how the process leading to mucosal inflammation isinitiated, whether the abnormal bacterial colonization that isobserved in the premature infant with NEC is a cause or aconsequence of the disease, how the inflammatory responsewithin the intestinal epithelium is coordinated, and the deter-minants of when a “tipping point” is reached, beyond whichreversibility and restoration of the intestinal mucosal barrierare unachievable. To address these (among others) importantgaps in our knowledge, careful study of clinical specimensfrom infants with and without NEC alongside carefully vali-dated animal models of this disease is required. This reviewwill now summarize the considerations in the selection ofanimal models for NEC research to address these importantquestions, will assess the key challenges associated with ani-mal models in this field, and will then discuss the key animalmodels available to researchers with an assessment of the keycontributions already gained from each, their strengths andtheir weaknesses. A summary of the major results from animalmodels that have provided a unifying approach to our under-standing of the causes of NEC and the strategies that preventthis disease is shown in Fig. 1.
General Considerations and Challenges in the Selection ofAnimal Models for NEC Research
There are some unique challenges associated with the selec-tion of appropriate animal models for use in NEC research.Many of these challenges pertain to the unique features of NECthat distinguish this disease from other inflammatory or septicprocesses, and which together reduce the number of reliable
options that are available for animal-based NEC research. Forinstance, NEC is known to primarily affect premature infantswho receive formula as opposed to breast milk. Thus, if onewishes to reliably reproduce the clinical disease in animals, amodel in an animal at an age that shows features of immaturityneeds to be selected. Furthermore, although models in smallanimals such as mice and rats offer the advantages of being ofrelatively low cost and readily available in large numbers, theylack the clinical robustness that is seen in larger animal modelssuch as piglets, in which the comparison to a premature humanis more readily obvious (a premature human infant that devel-ops NEC can be of a similar size and weight as a prematurepiglet). More important considerations for the selection of aparticular animal model relate to the specific question that isbeing asked, and a subsequent determination of how “reduc-tionist” the particular animal model needs to be. For instance,if the intent is to test a particular molecular pathway that ishypothesized to play a role in the pathogenesis of NEC, orperhaps a new therapeutic agent for the prevention or treatmentof NEC, then an animal model should be selected in which thispathway is affected under conditions that mimic the keyfeatures of NEC as seen in humans. By contrast, if the inves-tigator wishes to test a reagent that may be capable of inhib-iting or enhancing the signaling through a specific pathway thatis already known to be important in NEC pathogenesis, then areductionist approach can be selected in which this particularpathway is manipulated and subsequent effects on remotetissues including the gut can be assessed. Furthermore, asknowledge of the underpinnings of NEC have evolved, theanimal models that researchers employ to study the diseasemust necessarily evolve. For instance, with a greater under-standing that an abnormal community of enteric bacteria playsan important role in the pathogenesis of NEC in humans,comes the need to actively incorporate enteric bacteria associ-ated with NEC development in animal models of this disease.Additional considerations for the selection of a particularmodel include the cost, ease of implementation of the strategyfor induction of NEC, need for gene deletion, and availabilityof the required reagents. However, the overriding determina-tion of a particular model should be its relevance to the diseasein question, and for this reason it is important to understandhow a particular model of NEC should be validated, as will bediscussed below. An overview of each of the commonly usedanimal models used in NEC research is provided in Tables 1–3,and a comparative analysis is summarized in Table 4.
How Should Animal Models of NEC Be Validated?
The relatively large number of animal models that investi-gators have used to study NEC suggests that an approach isrequired to clearly define what constitutes a model of NEC inthe first place and to then apply a validation scheme so that theresults of studies can be compared within an appropriatecontext. At a minimum, animal models should replicate mostof the cardinal histopathological features that are seen inhuman NEC, which include the presence of mucosal edema,pneumatosis intestinalis (i.e., the presence of gas within thewall of the intestine due to microbial activity), epithelialsloughing/villous atrophy, evidence of enterocyte apoptosis,vascular thrombosis, and discontinuous necrotic segments ofintestine (so called “skip lesions”; Ref. 78). In addition, as a
Prematurity
Increased TLR4
Stressed microbiome
Breast milk Amniotic fluid TLR4 blockade
• Increased mucosal injury
• Reduced intestinal perfusion
• Reduced mucosal repair
• Intestinal stem cell loss
• Increased mucosal injury
• Reduced intestinal perfusion
• Reduced mucosal repair
• Intestinal stem cell loss
Premature infant with NEC
TLR9 agonists Cytosolic Hsp70
Immature immunity
Probiotics
Clinical Features of NEC: • abdominal distention • ventilatory support • ill appearing • feeding intolerance
Fig. 1. Pathogenesis of necrotizing enterocolitis (NEC). Graphical representa-tion of the mechanisms that lead to the development of NEC, as well asprotection from NEC, based on findings from experiments performed in animalmodels as discussed in this review.
Themes
G918 ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

validation strategy, it should be possible to attenuate theseverity of NEC in a particular animal model through the useof experimental strategies that have been shown to attenuateNEC in humans, such as the administration of broad-spectrumantibiotics (57) or the substitution of formula with breast milk(44). Furthermore, the mechanisms by which the models areinduced should parallel the clinical condition in human NEC tothe extent that is possible. In this regard, models that includethe simple occlusion of the blood supply to the bowel (90) ormechanical obstruction of the distal bowel (27) are likely tohave a reduced overlap with models that meet all of the abovecriteria. By contrast, models that include factors associatedwith NEC development, including prematurity, formula ga-vage, manipulation of the microbiome, and external stressorssuch as hypothermia or hypoxia, are more likely to result in aphenotype that resembles the clinical condition.
Experimental Necrotizing Enterocolitis in Rats
The earliest rat NEC model, which was developed by for-mula feeding and hypoxia in newborn rats, was described byBarlow and colleagues in 1974 (7), the results of which led tothe conclusion that the gut flora and absence of breast milkwere suggested to play important roles in NEC pathogenesis.One year later, this model was modified to include the combi-nation of formula feeding, hypoxia, and hypothermia (6) toincrease the severity of the histological changes that were seen.In this model, formula feeding and hypoxia-hypothermia(100% nitrogen for 50 s followed by exposure to 4°C for 10min) are the two critical instigating factors, since all maternallyfed animals or animals without exposure to hypoxia-hypother-mia showed normal intestinal histology. To prevent any ma-ternal milk exposure, researchers have studied premature neo-natal rats delivered by the cesarean section 1 day before thescheduled birth (14) or rat pups collected immediately afterbirth (29). This rat NEC model includes the widely acceptedmajor risk factors of NEC, i.e., intestinal immaturity, enteralfeeding, and inappropriate bacterial colonization (78), and istherefore widely considered to be very applicable for the studyof pathogenetic mechanisms associated with this disease.
Many laboratories have used this model to study variousaspects of the pathogenesis of NEC. These include the expres-sion of the cytokines interleukin 18 and interleukin 12 in NECdevelopment (47); the roles of intestinal epithelial apoptosis(58), bacteria, and the lipopolysaccharide (LPS) receptor TLR4(59); and the role of maternal milk (28). Additional studiesusing the rat model have evaluated the pathogenetic roles ofplatelet-activating factor (PAF, 15), epidermal growth factor(29), bile acids (48), and intestinal microcirculatory dysfunc-tion (53) in NEC pathogenesis. Several laboratories havemodified this formula-feeding/hypoxia/hypothermia rat NECmodel by adding extra factors to increase the incidence ofNEC, including the addition of commensal bacteria typicallyfound in stool (13, 25), or by reducing various factors tosimplify the protocol. This modified model has been used todetermine the roles of platelet-activating factor receptor (14),nuclear factor-�B (25), heat shock protein 70 (HSP70, 66),probiotics (88), and nitric oxide dysregulation (37) in thepathogenesis of NEC. Feng et al. (32) utilized a modification inwhich formula-fed newborn or preterm born rats were exposedto intragastric LPS followed by hypoxia/hypothermia stress,
and this formula-feeding/hypoxia/hypothermia/LPS rat NECmodel was subsequently applied to demonstrate the pathogenicrole of nitric oxide synthase dysregulation (38) and the protec-tive role of heparin-binding epidermal growth factor-likegrowth factor (HB-EGF) in decreasing the NEC incidence(32), increasing intestinal microvascular blood flow (105), andprotecting intestinal stem cells (21). Others used reoxygenation(100% O2 for 5 min) to enhance the intestinal injury (62),whereas various laboratories have modified the hypoxia pro-cess using 5% oxygen for relatively long periods, i.e., 3 to 10min, and omitted the addition of hypothermia, to simplify theinduction of NEC (19). Because of its relative simplicity andreproducibility, the formula-feeding/hypoxia rat NEC modelwas widely accepted and used to determine the roles ofendotoxin (19, 43), the glutathione antioxidant system (60),surface integrins (82), nitric oxide (20, 106), carbon monoxide(107), P-glycoprotein (44), human milk oligosaccharide (54),and the expression of TLRs and cytokines (67) in NEC. Someresearchers have introduced Cronobacter sakazakii (CS), for-merly known as Enterobacter sakazakii, which is a bacteriathat was reported to be associated with NEC (99), to theformula-feeding/hypoxia rat NEC model (52). Okada and col-leagues (79) have modified the particular feeding regimen, byutilizing formula containing casein as the protein source toexert a greater burden on the intestines than whey, and,strikingly, overfeeding caused NEC-like intestinal injury inhalf of the animals after 24 h.
Other Rat Models Used for the Study of NEC
Additional models in the rat have been developed to inves-tigate the pathogenesis of NEC. For instance, the ischemia-reperfusion rat NEC model was developed based on the sen-sitivity of the intestine to oxidative stress. In this model,ischemia of the intestine is induced by interruption of bloodflow in superior mesenteric artery or isolated ileal loop, andreperfusion generates reactive oxygen stress, which leads tointestinal injury (50). Although this model is clearly an oxida-tive stress model, the links to clinical NEC remain uncertain,since this model does not involve formula feeding, is oftenperformed in older animals, and involves occlusion of thesuperior mesenteric artery, which is not seen in clinical NEC.The intestinal ischemia in this model can also be induced byhypoxia, and rats that underwent hypoxia and reoxygenationshowed similar lesions as seen in neonatal NEC (80). Althoughseveral authors have used this model, the links to NEC remainspeculative, since there is rarely a global ischemic injuryassociated with this disease clinically.
Taken together, these studies performed in rats have beenused to generate important observations regarding the patho-genesis of NEC. The low cost, high litter size, and readyavailability of rats makes them an attractive species for per-forming these studies. The major drawbacks of the use of ratsinclude the lack of readily available transgenic strains and theincreased tolerance for bacteria/endotoxin between rats andother animals including humans (9). These drawbacks have ledinvestigators to pursue models of NEC in other species, asreviewed below. A summary of the experimental details,strengths, and limitations of NEC models in rats is shown inTable 1.
Themes
G919ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

Experimental Necrotizing Enterocolitis in Mice
Compared with rat models, the induction of experimentalNEC in mice offers many advantages including high geneticsimilarity of inbred strains and the opportunity to utilizesophisticated transgenic approaches. However, the biggestchallenge to establish the mouse NEC models is the need tofeed the relatively small and fragile mouse pups. Similar to therat NEC models, the most popular mouse NEC models arebased on intestinal immaturity and enteral feeding. In 2006,Jilling and colleagues (59) developed a NEC model using micedelivered by cesarean section between embryonic day (E)20and E21, and NEC was induced by combined formula feeding,hypoxia, and hypothermia, resulting in 66% NEC incidencewith gross and microscopic evidence of intestinal necrosis.This formula-feeding/hypoxia/hypothermia mouse NEC modelwas subsequently validated in preterm and term mice deliveredby cesarean section (30, 44) and was utilized to assess the roleof various genes in NEC pathogenesis, including TLR4 (59),interleukin 18 (49), MDR1a (44), and MUC2 (71). Variousinvestigators have modified this mouse model of NEC bycolonizing neonatal mice with adult commensal bacteria inaddition to formula feeding, hypoxia, and hypothermia, result-ing in increased NEC incidence (10), and the roles of bacteria(16), endogenous PAF-acetylhydrolase (68), and probiotics(10) were investigated with this modified model.
In 2007, Hackam and colleagues (64) developed a NECmodel in 10-day-old mice using a combination of gavageformula feeding and intermittent hypoxia, resulting in the grossappearance of edema and necrosis in the small intestine thatresembles human NEC. Representative histomicrographs re-vealing the typical histology of the terminal ileum from mice
that were either untreated or were induced to develop NEC byusing this model are shown in Fig. 2, in which the comparisonwith human NEC can be observed. This formula-feeding/hypoxia mouse NEC model was validated in several studiesand was utilized to induce NEC in mice with modifications invarious genes including IFN-� (64), global TLR4 (63), intes-tinal TLR4 (95), endothelial TLR4 (103), TLR9 (42), induciblenitric oxide synthase (iNOS; Ref. 20), HSP70 (2), and au-tophagy-related protein 7 epithelium conditional knockoutmice (75). The protective functions of TLR9 (42), NOD2 (83),amniotic fluid (39), and small molecule inhibitors of TLR4(74) were also investigated by this model. This model wasslightly modified by other laboratories and was used to deter-mine the roles of phosphatidylinositol 3-kinase (3), TNF-� (4),oxidative stress (5), and heme oxygenase-1 (86) in NECpathogenesis.
Studies performed in mice have shed light on the reasons forwhich prematurity contributes to the pathogenesis of NECthrough effects, in part, on the regulation of the innate immunesystem of the developing gut (69). Specifically, we have shownthat the TLR4 expression is significantly increased in thepremature intestine compared with the full-term intestine,which reflects the recently recognized role of TLR4 in regu-lating normal intestinal differentiation and development (95).We and others have shown that, in the postnatal period, TLR4activation drives intestinal injury and reduces intestinal perfu-sion, as reviewed above, implying that the signaling propertiesof TLR4 in utero are distinct from its signature role in hostdefense. Given that the expression of TLR4 in the developingmouse intestinal lining rises during embryonic developmentand then falls precipitously at birth (42, 102), it can be
Table 1. Experimental details, strengths, and limitations of models of NEC in rats
Experimental Details Strengths Limitations References
Formula feeding and hypoxia (newborn rats). Utilizes known clinical risk factors. Rats may be exposed to maternal breastmilk before induction of the model.
7
Formula feeding, hypoxia and hypothermia(newborn rats).
Utilizes known clinical risk factors. Rats may be exposed to maternal breastmilk before induction of the model.
6High disease severity.
Formula feeding, hypoxia and hypothermia(premature rats).
No maternal milk exposure. Cesarean section is required. 14, 15, 28, 29, 47, 48,53, 58, 59Intestinal barrier is immature. In patients, NEC does not develop
immediately after birth questioningthe clinical relevance.
Formula-feeding, hypoxia and hypothermiawith the addition of commensal bacteriafrom adult rats (premature rats).
Includes risk factors associatedwith bacterial colonization.
The bacterial components that areadded may not be representative ofthe clinical situation.
13, 14, 25, 37, 66, 88
High disease severity.Formula-feeding, hypoxia and hypothermia
with the addition of intragastric LPS.The introduction of bacterial
component (i.e., LPS).LPS is not representative of all
bacterial components relevant toNEC.
21, 32, 38
Formula-feeding, hypoxia, hypothermiareoxygenation (100% O2 for 5 min).
Increased intestinal injury. The delivery of 100% oxygen topremature infants is avoided givenknown toxicity.
62
Formula-feeding and hypoxia, reoxygenation(5% oxygen for 3 to 10 min), nohypothermia.
Avoidance of hypothermiasimplifies the model.
Clinical relevance is uncertain given theprolonged reoxygenation.
19
Formula-feeding and hypoxia, addition ofCronobacter sakazakii.
Allows for the direct investigationof the role of Cronobactersakazakii, which is associatedwith NEC.
Cronobacter sakazakii causes aminority of NEC cases in patients,and is more likely to be associatedwith other infections (i.e.,meningitis).
52
Ischemia and reperfusion of the intestine inolder rats.
More accurately is an oxidativestress model.
Performed in older animals when theintestine is more mature; relevance toclinical NEC is uncertain.
50, 80
NEC, necrotizing enterocolitis.
Themes
G920 ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

speculated that the premature infant, in which the expression ofintestinal TLR4 remains persistently elevated, the developmen-tal role for TLR4 switches to a proinflammatory role upon itsinteraction with colonizing microbes, leading to mucosal in-flammation and NEC development. Additional studies areneeded to further identify the molecules that are involved in theswitch of TLR4 from a predominantly developmental to adefensive role. Moreover, strategies that can attenuate theextent of TLR4 signaling in the infant born prematurely mayoffer effective therapeutic approaches to the development ofNEC.
Other Mouse Models Used in NEC Research
Researchers have developed additional mouse models forNEC research, each having varying degrees of relevance to theclinical disease. The ischemia-reperfusion model involves sur-gical occlusion of both superior mesenteric vessels, resulting in
intestinal lesions (61), although the direct relevance to clinicalNEC is uncertain. A very novel approach to model humanNEC includes the “humanized mouse model,” or the “xeno-graft transplant model.” This model, as first described byWalker and colleagues (34, 73), involves the implantation of2-cm sections of human fetal ileum from 12 to 20 wk gestationsubcutaneously into mice with severe combined immunodefi-ciency. Xenografts are then harvested 20 and 30 wk posttrans-plantation to allow for examination of the intestine, as well asexpression of cytokines and innate immune inflammatorygenes. This model allows for the use of a highly reductionistapproach to study NEC in mice, while allowing for the inter-rogation of human tissue.
Clear advantages of mouse work include the low cost andready availability of these animals, as well as the ability toharness the power of transgenics, which is of particular impor-tance given the homology of the mouse and human genome,
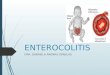
Human
Piglet
Mouse
Control NEC
Control NEC
Control NEC
A
B
C
Fig. 2. Histological appearance of necrotiz-ing enterocolitis in the human, piglet, andmouse. Representative micrographs showinghematoxylin and eosin-stained sections of theterminal ileum from a premature human in-fant (A), piglet (B), and mouse (C) without(left) or with (right) NEC as described in thisreview. Size bar � 50 �m.
Themes
G921ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

especially for inflammatory and metabolic genes (101). How-ever, important drawbacks of mice include their small size andassociated difficulty with feeding and handling small pups. Asummary of the experimental details, strengths, and limitationsof NEC models in mice is shown in Table 2. These disadvan-tages may be addressed through the use of the piglet model, asdescribed below.
Experimental Necrotizing Enterocolitis in Piglets
Compared with rodents, piglets share a high degree ofanatomical, developmental, nutritional, and physiological sim-ilarity of the gastrointestinal tract with human infants (81).However, unlike primates, which are viable from 70% gesta-tion, piglets are not viable until after 90% gestation (84), andmodels of NEC are typically induced in piglets under condi-tions that do not require significant resuscitative cardiac orventilator support. Therefore, the first piglet models of NECwere developed in neonatal term piglets based on the fact thatpreterm infants often undergo ischemic injury that can be
induced by hypoxia (89). Subsequently, hypothermia was in-troduced in piglet models of NEC, which yielded high NECseverity (18, 23). Given the acceptance that enteral feeding isone of the most important risk factors associated with NECdevelopment in humans, infant formula or casein was intro-duced to neonatal piglets to develop NEC. In 1994, Crissingerand colleagues (24) produced a piglet NEC model by luminalperfusion of 1-day-old piglet jejunoileum with predigested andbile acid-solubilized preterm cow milk-based infant formulacoupled with ischemia and reperfusion, and the importance ofthe lipid fraction of the formula in NEC pathogenesis wassuggested. Di Lorenzo and colleagues (26) injected acidifiedcasein solution into the intestinal loop of neonatal piglets andsuccessfully induced intestinal damage. In 2006, Sangild andcolleagues (85) induced NEC in preterm piglets, which weredelivered by cesarean section at 92% gestation, by administer-ing total parenteral nutrition, then administering infant formulawithout exposure to hypoxia or hypothermia. This preterm-birth/formula-feeding piglet NEC model was further validated
Table 3. Experimental details, strengths, and limitations of models of necrotizing enterocolitis in piglets
Experimental Details Strengths Limitations References
Ischemia induced by hypoxia in neonatal termpiglets.
Mimics the ischemic injurythat may be seen inNEC.
Term piglets are used raising questions regardingthe clinical significance.
89
Lack of enteral feeding.Hypoxia and hypothermia in neonatal term
piglets.Mimic the ischemic injury. Term piglets are used. 18, 23High NEC severity. No enteral feeding.
Uncertain clinical significanceLuminal perfusion of 1-day-old piglet
jejunoileum with predigested and bile acid-solubilized preterm cow milk-based infantformula coupled with ischemia andreperfusion.
Short duration of themodel.
Term piglets were used. 24Uncertain clinical significance.
Injection of acidified casein solution into theintestinal loop of neonatal piglets.
Introduction of intestinaldysmotility, which is arisk factor for NEC.
Term piglets are used and the experimentalmodel is very short, raising questions.regarding the clinical significance.
26
Administration of total parenteral nutritionfollowed by the administration of infantformula in preterm piglets which aredelivered by cesarean section at 92%gestation.
Combined preterm-birth,parenteral nutrition andformula-feeding increasethe clinical relevance.
Need for a well-equipped veterinary surgicalfacility.
8, 55, 56, 85, 91,92, 93, 98,100
Table 2. Experimental details, strengths, and limitations of models of necrotizing enterocolitis in mice
Experimental Details Strengths Limitations References
Formula feeding, hypoxia and hypothermia inpreterm or term mice delivered by cesareansection.
Preterm pups. Technical challenges of handling prematurepups.
30, 44, 49, 59, 71
Clinical NEC does not occur immediatelyafter birth so the clinical relevance issomewhat in question.
Formula feeding, hypoxia and hypothermia inmice delivered by cesarean section, withthe addition of commensal bacteriaobtained from adult mice.
Preterm pups. Difficulty in handling preterm pups. 10, 16, 68High NEC incidence. Clinical NEC does not occur immediately
after birth.Addition of commensal bacteriaincreases clinical relevance.
Formula feeding and hypoxia in 10-day-oldmice.
Technically easier to handle the10-day-old mice.
The model does not use preterm pups. 2, 3, 4, 5, 20, 39, 42,64, 63, 74, 75, 83,86, 95, 103NEC is induced at a time in
which it is observedclinically within the postnatalperiod.
Ischemia and reperfusion by surgicalocclusion of both superior mesentericvessels.
More accurately is an oxidativestress model.
Clinical NEC does not involve occlusion ofthe mesenteric vessels, so the relevanceof this model is uncertain.
61
Implantation of human fetal ileumsubcutaneously into SCID mice.
Allows for interrogation ofhuman tissue.
Requirement for human fetal tissue. 73, 34Technically challenging.
Themes
G922 ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

via demonstration of an increase in the proinflammatory cyto-kine IL-6, one of the signature cytokines found in NEC infants(93). This model was used to determine the effects of colos-trum (85), human milk (55), amniotic fluid (91), carbohydratemaldigestion (98), and glucagon-like peptide-2 (8) and wasalso used to study the changes in the microvasculature (100).Furthermore, a recent report on the role of antibiotics in thismodel, and an initial report demonstrating the role of gutcolonization, provide additional important evidence for thevalidity of the model (56, 92). We have recently modified thismodel by delivering piglets at 92% estimated gestation andadministered infant formula without exposure to hypoxia orhypothermia or the provision of total parenteral nutrition andobserve mucosal inflammation similar to mouse and humanNEC (Fig. 2).
The utilization of piglet models for the study of NEC offerthe advantages of using a large animal model for this diseasethat has anatomic and functional properties of the intestine thatare comparable to the human infant. These factors provide asuitable clinical platform for the investigation of drugs forpotential use in humans, as well as for an assessment of
whether biochemical pathways that were identified in rodentmodels may have relevance across species. However, the largecost of performing piglet NEC work, as well as the relativedifficulty of maintaining and feeding a group of prematurepiglets, offer unique disadvantages of this approach (Table 3).
Experimental Necrotizing Enterocolitis in Hamstersand Rabbits
Besides the most commonly used mouse, rat, and pigletNEC models, other animals, such as hamster and rabbit, havebeen used in the past to induce experimental NEC. In 1989,hypothermia was applied to weanling hamsters, and 50% ofcold-stressed animals showed colonic damage that resembledNEC (18). This hypothermia hamster NEC model was used todetermine the role of reactive oxygen species in NEC, andcold-stressed hamsters showed a significant decrease in xan-thine dehydrogenase/xanthine oxidase activity ratio (18). In2004, Erdener and colleagues (31) developed a hypoxia/reoxy-genation rabbit NEC model, in which newborn rabbits received5-min hypoxia followed by 5-min reoxygenation, which
Table 4. A comparative overview of the advantages, disadvantages, and applications of experimental models for the study ofNEC
Model Organism Advantages Disadvantages Applications
Rats Low cost. Lack of readily available transgenicstrains.
Biomarker identification.
High litter size. Marked difference in bacterial/endotoxintolerance between rats and human(increased tolerance in rats).
Investigation of pathogenesis anddisease mechanisms.
Ready availability. Uncertain relevance to human disease. Drug discovery.Ease of disease induction.Uniform genetic backgrounds.Short gestational period.
Mice Low cost. Difficulty in feeding and handling smalland fragile pups.
Biomarker identification.High litter size. Investigation of pathogenesis and
disease mechanisms.Ready availability.Ease of disease induction. Drug discovery.Uniform genetic backgrounds.Short gestational period.High genetic similarity.Availability of knockout strains.Sophisticated transgenic
approaches.Piglets High degree of anatomic,
developmental, nutritional,functional and physiologicalsimilarity of the gastrointestinaltract with human infants.
High cost. Drug discovery.
Similar size to human preterminfants.
Difficulty in maintaining and feeding agroup of premature piglets.
Validation of biochemicalpathways.
Variability of genetic background. Study of pathogenesis.Need for a well-equipped surgical
facility to perform cesarean sectionand safely manage a litter of piglets.
Evaluation of specific feedingregimens.
Preclinical drug studies.Development of early
noninvasive spectroscopicdiagnostic methods.
Hamsters and rabbits Relatively large size. High cost relative to rats and mice. Underlying mechanisms ofdisease.Ease of handling. Variability of genetic background.
Nematode (Caenorhabditis elegans) Relatively low cost. Lacks many physiological and dietaryfeatures of mammals, making theclinical and scientific relevance toNEC uncertain.
The study of single cells andcell-microbial interactions.Easy genetic manipulation.
Well-characterized genome.Epithelialized gastrointestinal tract.
Invertebrate (Drosophila) Low cost. Relevance to disease in mammaliansystems is uncertain.
Study of underlying mechanisms.Easy genetic manipulation.
Themes
G923ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

yielded intestinal lesions similar to human NEC, and whichwas applied to determine the effect of pentoxifylline on NEC.In a modification of this rabbit NEC model, Choi et al. (22)used a combination of LPS, hypoxia, and hypothermia in termNew Zealand White rabbits before weaning (i.e., 0–4 wk) toassess intestinal perfusion by noninvasive, Doppler ultrasound-based methodology. Although hamster and rabbit models ofNEC may offer advantages with respect to their relatively largesize and ease of handling, their costs are much higher thanmice or rats, and they lack the physiological and anatomicadvantages of piglets, making their overall role in NEC re-search somewhat unclear. A comparison of the advantages,disadvantages, and applicability of models of NEC in each ofthese species is shown in Table 4.
Highly Reductionist Experimental Approaches to NECResearch: Nematode and Invertebrate Systems
Although the models of NEC described above have cleartranslational significance to clinical NEC, they are by defini-tion limited by the complex nature of mammalian in vivosystems. Important questions in the field, such as the role thatindividual cell types may play in governing the extent ofintestinal injury in NEC, may not be readily addressed bymammalian models, given the complex and interrelated sys-tems that are activated during the experimental conditions. Toaddress this potential pitfall, various authors have utilizedhighly reductionist approaches that allow for the study ofsingle cells and cell-microbial interactions, to gain insights intothe pathogenesis of NEC. For instance, the nematode Caeno-rhabditis elegans is characterized by a remarkably well-char-acterized genome and has an epithelialized gastrointestinaltract with a predictable number and arrangement of cells, thatcan be fed a diet of bacteria of various species. By using thismodel, mechanisms leading to gut epithelial necrosis in re-sponse to bacterial products can be readily assessed withoutneeding to control for other cell types found in mammaliansystems. The genome of C. elegans is completely sequencedand is known to share homology with that of mammals (94).Work in C. elegans has been used to identify the role ofproteases in mediating necrotic gut epithelial death, whichapproximates that seen in clinical NEC (11, 70). Similarly,
investigators have performed important studies using flies,which have shed light on the processes that regulate epithelialhomeostasis within the intestine (96), and have identifiedcritical molecular determinants required for intestinal epithelialapoptosis (87) and proliferation (45). Although it would beinaccurate to indicate that these models in flies and worms area surrogate for complex studies that can be performed inmammalian systems, it is fair to indicate that studies in thesesystems offer advantages of easy genetic manipulation whileassessing conditions known to be important in NEC research(Table 4).
An Approach to Model Selection for NEC Research
Having reviewed the various animal models available forNEC research, we now propose an approach to model selec-tion. For the majority of NEC studies, the development ofmodels in rodents will be most appropriate, given their advan-tages of low cost, ready availability, and relative ease ofdisease induction. Full-term rats and mice are relatively imma-ture compared with full-term infants, so that delivery of pre-mature pups by cesarean section may not be necessary. Exper-imental rats and mice have relatively uniform genetic back-grounds and a short gestational period and can mimic themacroscopic, microscopic, and biochemical features of NEC;they are therefore appropriate models for identification ofbiomarkers, pathogenetic mechanisms, and drug discovery.Compared with rodents, neonatal piglets share greater anatom-ical, physiological, and metabolic similarities with the humanneonate, and the preterm-delivered piglet approximates thepreterm human infant in terms of size. The piglet is thereforeuseful in studies of pathogenesis, and also in the evaluation ofspecific feeding regimens and in preclinical drug studies forprevention and potential therapy, as well as for the develop-ment of early radiological diagnostic methods (35). However,the relatively high cost, the variability of genetic background,and the need for a well-equipped surgical facility to perform acesarean section limits the application and widespread use ofpiglet NEC models. Although no particular animal model canfully incorporate all the characteristics in human NEC, signif-icant progress has already been achieved in advancing ourunderstanding of this disease by use of these animal models,
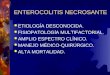
Mouse Human E-cadherin Muc-II DAPI
E-cadherin Lysozyme DAPI
A B
Fig. 3. Cultured enteroids from human andmouse crypts. Representative confocal mi-crographs of enteroids that were derivedfrom the intestinal stem cell compartment ofa newborn mouse (A) or premature infant (B)and maintained for 5 days in culture. Sizebar � 10 �m.
Themes
G924 ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

and the major advantages, disadvantages, and applicability ofthese models are shown in Table 4. Through an understandingof more than one particular model, and collaboration betweeninvestigators who work across models, greater insights into thisdevastating disease can be gained.
Future Directions in NEC Model Development
As we learn more about the pathogenesis of NEC, in partthrough the studies described above, as well as in part from thecareful study of clinical tissues obtained from patients with andwithout NEC at similar gestational ages, it is imperative thatour modeling evolves to more readily count for nuances in theunderstanding of the disease. For instance, as a greater under-standing of the role of the microbiome in NEC becomesapparent, it will be important to factor in various strains ofbacteria to induce NEC and to take into account the relativeroles of varying microbial communities in animal experimentsin which NEC is observed to varying degrees. Similarly, as therole of the host genome on NEC development becomes moreapparent, specific experiments in mice, or in lower organismsas described above, could be performed to better understandthe role of host genetics in disease pathogeneses, which untilrecently was considered a passive bystander in the process(41). In addition, owing in part to the recently emerging geneediting technologies using zinc-finger nucleases (36), tran-scription activator-like effector nucleases (97, 17) andCRISPR-Cas systems (65), genetically manipulated rats, pig-lets, and other mammals may be available for NEC study in thenear future. Finally, the recent identification of techniques forthe culture and growth of intestinal stem cells from mice andhumans with and without NEC has opened doors for thepossibility of generating cultures of the intact intestinal epithe-lium for mechanistic studies, as well as to provide a platformfor drug discovery (Fig. 3) (1, 76). The immediate future holdsgreat promise for the field of NEC research, in part due to thepowerful and rapid advances that have been made recently infundamental mechanisms that lead to NEC development, butalso in the identification of specific preventative or treatmentapproaches.
ACKNOWLEDGMENTS
The authors acknowledge the large number of talented researchers in thefield and apologize to those dedicated scientists whose important work wasinadvertently not referenced.
GRANTS
D. J. Hackam is supported by The Hartwell Foundation, Memphis, TN andby R01GM078238, R01DK083752, and P50GM053789 from the NationalInstitutes of Health.
DISCLOSURES
No conflicts of interest, financial or otherwise, are declared by the author(s).
AUTHOR CONTRIBUTIONS
P.L., C.P.S., H.J., S.S., M.G., and D.J.H. conception and design of research;P.L., C.P.S., H.J., S.S., M.G., M.F.B., and D.J.H. performed experiments; P.L.,C.P.S., H.J., S.S., M.G., M.F.B., and D.J.H. analyzed data; P.L., C.P.S., H.J.,S.S., M.G., and D.J.H. interpreted results of experiments; P.L., C.P.S., H.J.,S.S., M.G., and D.J.H. prepared figures; P.L., C.P.S., H.J., S.S., M.G., andD.J.H. drafted manuscript; P.L., C.P.S., H.J., S.S., M.G., and D.J.H. edited andrevised manuscript; P.L., C.P.S., H.J., S.S., M.G., M.F.B., and D.J.H. approvedfinal version of manuscript.
REFERENCES
1. Afrazi A, Branca MF, Sodhi CP, Good M, Yamaguchi Y, Egan CE,Lu P, Jia H, Shaffiey S, Lin J, Ma C, Vincent G, Prindle T Jr,Weyandt S, Neal MD, Ozolek JA, Wiersch J, Tschurtschenthaler M,Shiota C, Gittes GK, Billiar TR, Mollen KP, Kaser A, Blumberg R,Hackam DJ. Toll like receptor 4-mediated endoplasmic reticulum stressin intestinal crypts induces necrotizing enterocolitis. J Biol Chem 289:9584–9599, 2014.
2. Afrazi A, Sodhi CP, Good M, Jia H, Siggers R, Yazji I, Ma C, NealMD, Prindle T, Grant ZS, Branca MF, Ozolek J, Chang EB, HackamDJ. Intracellular heat shock protein-70 negatively regulates TLR4 sig-naling in the newborn intestinal epithelium. J Immunol 188: 4543–4557,2012.
3. Baregamian N, Rychahou PG, Hawkins HK, Evers BM, Chung DH.Phosphatidylinositol 3-kinase pathway regulates hypoxia-inducible fac-tor-1 to protect from intestinal injury during necrotizing enterocolitis.Surgery 142: 295–302, 2007.
4. Baregamian N, Song J, Bailey CE, Papaconstantinou J, Evers BM,Chung DH. Tumor necrosis factor-alpha and apoptosis signal-regulatingkinase 1 control reactive oxygen species release, mitochondrial autophagy,and c-Jun N-terminal kinase/p38 phosphorylation during necrotizing entero-colitis. Oxid Med Cell Longev 2: 297–306, 2009.
5. Baregamian N, Song J, Papaconstantinou J, Hawkins HK, EversBM, Chung DH. Intestinal mitochondrial apoptotic signaling is acti-vated during oxidative stress. Pediatr Surg Int 27: 871–877, 2011.
6. Barlow B, Santulli TV. Importance of multiple episodes of hypoxia orcold stress on the development of enterocolitis in an animal model.Surgery 77: 687–690, 1975.
7. Barlow B, Santulli TV, Heird WC, Pitt J, Blanc WA, Schullinger JN.An experimental study of acute neonatal enterocolitis—the importance ofbreast milk. J Pediatr Surg 9: 587–595, 1974.
8. Benight NM, Stoll B, Olutoye OO, Holst JJ, Burrin DG. GLP-2 delaysbut does not prevent the onset of necrotizing enterocolitis in preterm pigs.J Pediatr Gastroenterol Nutr 56: 623–630, 2013.
9. Berczi I, Bertok L, Bereznai T. Comparative studies on the toxicity ofEscherichia coli lipopolysaccharide endotoxin in various animal species.Can J Microbiol 12: 1070–1071, 1966.
10. Bergmann KR, Liu SX, Tian R, Kushnir A, Turner JR, Li HL, ChouPM, Weber CR, De Plaen IG. Bifidobacteria stabilize claudins at tightjunctions and prevent intestinal barrier dysfunction in mouse necrotizingenterocolitis. Am J Pathol 182: 1595–1606, 2013.
11. Bhatia SR, Miedel MT, Chotoo CK, Graf NJ, Hood BL, Conrads TP,Silverman GA, Luke CJ. Using C. elegans to identify the proteasetargets of serpins in vivo. Meth Enzymol 499: 283–299, 2011.
12. Blakely ML, Lally KP, McDonald S, Brown RL, Barnhart DC,Ricketts RR, Thompson WR, Scherer LR, Klein MD, Letton RW,Chwals WJ, Touloukian RJ, Kurkchubasche AG, Skinner MA, MossRL, Hilfiker ML. Postoperative outcomes of extremely low birth-weightinfants with necrotizing enterocolitis or isolated intestinal perforation: aprospective cohort study by the NICHD Neonatal Research Network.Ann Surg 241: 984–989; discussion 989–994, 2005.
13. Caplan MS, Hedlund E, Adler L, Hsueh W. Role of asphyxia andfeeding in a neonatal rat model of necrotizing enterocolitis. PediatrPathol 14: 1017–1028, 1994.
14. Caplan MS, Hedlund E, Adler L, Lickerman M, Hsueh W. Theplatelet-activating factor receptor antagonist WEB 2170 prevents neona-tal necrotizing enterocolitis in rats. J Pediatr Gastroenterol Nutr 24:296–301, 1997.
15. Caplan MS, Lickerman M, Adler L, Dietsch GN, Yu A. The role ofrecombinant platelet-activating factor acetylhydrolase in a neonatal ratmodel of necrotizing enterocolitis. Pediatr Res 42: 779–783, 1997.
16. Carlisle EM, Poroyko V, Caplan MS, Alverdy JA, Liu D. Gramnegative bacteria are associated with the early stages of necrotizingenterocolitis. PloS One 6: e18084, 2011.
17. Carlson DF, Tan W, Lillico SG, Stverakova D, Proudfoot C, Chris-tian M, Voytas DF, Long CR, Whitelaw CB, Fahrenkrug SC. Effi-cient TALEN-mediated gene knockout in livestock. Proc Natl Acad SciUSA 109: 17382–17387, 2012.
18. Cassutto BH, Misra HP, Pfeiffer CJ. Intestinal post-ischemic reperfu-sion injury: studies with neonatal necrotizing enterocolitis. Acta PhysiolHung 73: 363–369, 1989.
19. Cetin S, Ford HR, Sysko LR, Agarwal C, Wang J, Neal MD, Baty C,Apodaca G, Hackam DJ. Endotoxin inhibits intestinal epithelial resti-
Themes
G925ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

tution through activation of Rho-GTPase and increased focal adhesions.J Biol Chem 279: 24592–24600, 2004.
20. Cetin S, Leaphart CL, Li J, Ischenko I, Hayman M, Upperman J,Zamora R, Watkins S, Ford HR, Wang J, Hackam DJ. Nitric oxideinhibits enterocyte migration through activation of RhoA-GTPase in aSHP-2-dependent manner. Am J Physiol Gastrointest Liver Physiol 292:G1347–G1358, 2007.
21. Chen CL, Yu X, James IO, Zhang HY, Yang J, Radulescu A, ZhouY, Besner GE. Heparin-binding EGF-like growth factor protects intes-tinal stem cells from injury in a rat model of necrotizing enterocolitis.Lab Invest 92: 331–344, 2012.
22. Choi YH, Kim IO, Cheon JE, Kim JE, Kim EK, Kim WS, Yeon KM.Doppler sonographic findings in an experimental rabbit model of necro-tizing enterocolitis. J Ultrasound Med 29: 379–386, 2010.
23. Cohen IT, Nelson SD, Moxley RA, Hirsh MP, Counihan TC, MartinRF. Necrotizing enterocolitis in a neonatal piglet model. J Pediatr Surg26: 598–601, 1991.
24. Crissinger KD, Burney DL, Velasquez OR, Gonzalez E. An animalmodel of necrotizing enterocolitis induced by infant formula and isch-emia in developing piglets. Gastroenterology 106: 1215–1222, 1994.
25. De Plaen IG, Liu SX, Tian R, Neequaye I, May MJ, Han XB, HsuehW, Jilling T, Lu J, Caplan MS. Inhibition of nuclear factor-kappaBameliorates bowel injury and prolongs survival in a neonatal rat model ofnecrotizing enterocolitis. Pediatr Res 61: 716–721, 2007.
26. Di Lorenzo M, Bass J, Krantis A. An intraluminal model of necrotizingenterocolitis in the developing neonatal piglet. J Pediatr Surg 30:1138–1142, 1995.
27. Di Lorenzo M, Bass J, Krantis A. Use of L-arginine in the treatment ofexperimental necrotizing enterocolitis. J Pediatr Surg 30: 235–240;discussion 240–231, 1995.
28. Dvorak B, Halpern MD, Holubec H, Dvorakova K, Dominguez JA,Williams CS, Meza YG, Kozakova H, McCuskey RS. Maternal milkreduces severity of necrotizing enterocolitis and increases intestinalIL-10 in a neonatal rat model. Pediatr Res 53: 426–433, 2003.
29. Dvorak B, Halpern MD, Holubec H, Williams CS, McWilliam DL,Dominguez JA, Stepankova R, Payne CM, McCuskey RS. Epidermalgrowth factor reduces the development of necrotizing enterocolitis in aneonatal rat model. Am J Physiol Gastrointest Liver Physiol 282: G156–G164, 2002.
30. Emami CN, Chokshi N, Wang J, Hunter C, Guner Y, Goth K, WangL, Grishin A, Ford HR. Role of interleukin-10 in the pathogenesis ofnecrotizing enterocolitis. Am J Surg 203: 428–435, 2012.
31. Erdener D, Bakirtas F, Alkanat M, Mutaf I, Habif S, Bayindir O.Pentoxifylline does not prevent hypoxia/reoxygenation-induced necrotiz-ing enterocolitis. An experimental study. Biol Neonate 86: 29–33, 2004.
32. Feng J, El-Assal ON, Besner GE. Heparin-binding epidermal growthfactor-like growth factor decreases the incidence of necrotizing entero-colitis in neonatal rats. J Pediatr Surg 41: 144–149; discussion 144–149,2006.
33. Ganapathy V, Hay JW, Kim JH, Lee ML, Rechtman DJ. Long termhealthcare costs of infants who survived neonatal necrotizing enteroco-litis: a retrospective longitudinal study among infants enrolled in TexasMedicaid. BMC Pediatr 13: 127, 2013.
34. Ganguli K, Meng D, Rautava S, Lu L, Walker WA, Nanthakumar N.Probiotics prevent necrotizing enterocolitis by modulating enterocytegenes that regulate innate immune-mediated inflammation. Am J PhysiolGastrointest Liver Physiol 304: G132–G141, 2013.
35. Gay AN, Lazar DA, Stoll B, Naik-Mathuria B, Mushin OP, Rodri-guez MA, Burrin DG, Olutoye OO. Near-infrared spectroscopy mea-surement of abdominal tissue oxygenation is a useful indicator ofintestinal blood flow and necrotizing enterocolitis in premature piglets. JPediatr Surg 46: 1034–1040, 2011.
36. Geurts AM, Cost GJ, Freyvert Y, Zeitler B, Miller JC, Choi VM,Jenkins SS, Wood A, Cui X, Meng X, Vincent A, Lam S, Michalk-iewicz M, Schilling R, Foeckler J, Kalloway S, Weiler H, Menoret S,Anegon I, Davis GD, Zhang L, Rebar EJ, Gregory PD, Urnov FD,Jacob HJ, Buelow R. Knockout rats via embryo microinjection ofzinc-finger nucleases. Science (New York, NY) 325: 433, 2009.
37. Giannone PJ, Alcamo AA, Schanbacher BL, Nankervis CA, BesnerGE, Bauer JA. Poly(ADP-ribose) polymerase-1: a novel therapeutictarget in necrotizing enterocolitis. Pediatr Res 70: 67–71, 2012.
38. Giannone PJ, Nankervis CA, Richter JM, Schanbacher BL, ReberKM. Prenatal lipopolysaccharide increases postnatal intestinal injury in a
rat model of necrotizing enterocolitis. J Pediatr Gastroenterol Nutr 48:276–282, 2009.
39. Good M, Siggers RH, Sodhi CP, Afrazi A, Alkhudari F, Egan CE,Neal MD, Yazji I, Jia H, Lin J, Branca MF, Ma C, Prindle T, GrantZ, Shah S, Slagle D 2nd, Paredes J, Ozolek J, Gittes GK, Hackam DJ.Amniotic fluid inhibits Toll-like receptor 4 signaling in the fetal andneonatal intestinal epithelium. Proc Natl Acad Sci USA 109: 11330–11335, 2012.
40. Gribar SC, Anand RJ, Sodhi CP, Hackam DJ. The role of epithelialToll-like receptor signaling in the pathogenesis of intestinal inflamma-tion. J Leukoc Biol 83: 493–498, 2008.
41. Gribar SC, Richardson WM, Sodhi CP, Hackam DJ. No longer aninnocent bystander: epithelial toll-like receptor signaling in the develop-ment of mucosal inflammation. Mol Med 14: 645–659, 2008.
42. Gribar SC, Sodhi CP, Richardson WM, Anand RJ, Gittes GK,Branca MF, Jakub A, Shi XH, Shah S, Ozolek JA, Hackam DJ.Reciprocal expression and signaling of TLR4 and TLR9 in the patho-genesis and treatment of necrotizing enterocolitis. J Immunol 182:636–646, 2009.
43. Grishin AV, Wang J, Potoka DA, Hackam DJ, Upperman JS, BoyleP, Zamora R, Ford HR. Lipopolysaccharide induces cyclooxygenase-2in intestinal epithelium via a noncanonical p38 MAPK pathway. JImmunol 176: 580–588, 2006.
44. Guner YS, Franklin AL, Chokshi NK, Castle SL, Pontarelli E, WangJ, Wang L, Prasadarao NV, Upperman JS, Grishin AV, Ford HR.P-glycoprotein induction by breast milk attenuates intestinal inflamma-tion in experimental necrotizing enterocolitis. Lab Invest 91: 1668–1679,2011.
45. Guo Z, Driver I, Ohlstein B. Injury-induced BMP signaling negativelyregulates Drosophila midgut homeostasis. J Cell Biol 201: 945–961,2013.
46. Hackam DJ, Afrazi A, Good M, Sodhi CP. Innate immune signaling inthe pathogenesis of necrotizing enterocolitis. Clin Dev Immunol 2013:475415, 2013.
47. Halpern MD, Holubec H, Dominguez JA, Williams CS, Meza YG,McWilliam DL, Payne CM, McCuskey RS, Besselsen DG, Dvorak B.Up-regulation of IL-18 and IL-12 in the ileum of neonatal rats withnecrotizing enterocolitis. Pediatr Res 51: 733–739, 2002.
48. Halpern MD, Holubec H, Saunders TA, Dvorak K, Clark JA, DoelleSM, Ballatori N, Dvorak B. Bile acids induce ileal damage duringexperimental necrotizing enterocolitis. Gastroenterology 130: 359–372,2006.
49. Halpern MD, Khailova L, Molla-Hosseini D, Arganbright K, Reyn-olds C, Yajima M, Hoshiba J, Dvorak B. Decreased development ofnecrotizing enterocolitis in IL-18-deficient mice. Am J Physiol Gastro-intest Liver Physiol 294: G20–G26, 2008.
50. Hammerman C, Goldschmidt D, Caplan MS, Kaplan M, BromikerR, Eidelman AI, Gartner LM, Hochman A. Protective effect ofbilirubin in ischemia-reperfusion injury in the rat intestine. J PediatrGastroenterol Nutr 35: 344–349, 2002.
51. Holman RC, Stoll BJ, Curns AT, Yorita KL, Steiner CA, Schon-berger LB. Necrotising enterocolitis hospitalisations among neonates inthe United States. Paediatr Perinatal Epidemiol 20: 498–506, 2006.
52. Hunter CJ, Singamsetty VK, Chokshi NK, Boyle P, Camerini V,Grishin AV, Upperman JS, Ford HR, Prasadarao NV. Enterobactersakazakii enhances epithelial cell injury by inducing apoptosis in a ratmodel of necrotizing enterocolitis. J Infect Dis 198: 586–593, 2008.
53. Ito Y, Doelle SM, Clark JA, Halpern MD, McCuskey RS, Dvorak B.Intestinal microcirculatory dysfunction during the development of exper-imental necrotizing enterocolitis. Pediatr Res 61: 180–184, 2007.
54. Jantscher-Krenn E, Zherebtsov M, Nissan C, Goth K, Guner YS,Naidu N, Choudhury B, Grishin AV, Ford HR, Bode L. The humanmilk oligosaccharide disialyllacto-N-tetraose prevents necrotising en-terocolitis in neonatal rats. Gut 61: 1417–1425, 2012.
55. Jensen ML, Sangild PT, Lykke M, Schmidt M, Boye M, Jensen BB,Thymann T. Similar efficacy of human banked milk and bovine colos-trum to decrease incidence of necrotizing enterocolitis in preterm piglets.Am J Physiol Regul Integr Comp Physiol 305: R4–R12, 2013.
56. Jensen ML, Thymann T, Cilieborg MS, Lykke M, Molbak L, JensenBB, Schmidt M, Kelly D, Mulder I, Burrin DG, Sangild PT. Antibi-otics modulate intestinal immunity and prevent necrotizing enterocolitisin preterm neonatal piglets. Am J Physiol Gastrointest Liver Physiol 306:G59–G71, 2014.
Themes
G926 ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

57. Jiang P, Jensen ML, Cilieborg MS, Thymann T, Wan JM, Sit WH,Tipoe GL, Sangild PT. Antibiotics increase gut metabolism and anti-oxidant proteins and decrease acute phase response and necrotizingenterocolitis in preterm neonates. PloS One 7: e44929, 2012.
58. Jilling T, Lu J, Jackson M, Caplan MS. Intestinal epithelial apoptosisinitiates gross bowel necrosis in an experimental rat model of neonatalnecrotizing enterocolitis. Pediatr Res 55: 622–629, 2004.
59. Jilling T, Simon D, Lu J, Meng FJ, Li D, Schy R, Thomson RB,Soliman A, Arditi M, Caplan MS. The roles of bacteria and TLR4 in ratand murine models of necrotizing enterocolitis. J Immunol 177: 3273–3282, 2006.
60. Kelly N, Friend K, Boyle P, Zhang XR, Wong C, Hackam DJ,Zamora R, Ford HR, Upperman JS. The role of the glutathioneantioxidant system in gut barrier failure in a rodent model of experimen-tal necrotizing enterocolitis. Surgery 136: 557–566, 2004.
61. Krasna IH, Howell C, Vega A, Ziegler M, Koop CE. A mouse modelfor the study of necrotizing enterocolitis. J Pediatr Surg 21: 26–29, 1986.
62. Le Mandat Schultz A, Bonnard A, Barreau F, Aigrain Y, Pierre-Louis C, Berrebi D, and Peuchmaur M. Expression of TLR-2, TLR-4,NOD2 and pNF-kappaB in a neonatal rat model of necrotizing entero-colitis. PloS One 2: e1102, 2007.
63. Leaphart CL, Cavallo J, Gribar SC, Cetin S, Li J, Branca MF,Dubowski TD, Sodhi CP, Hackam DJ. A critical role for TLR4 in thepathogenesis of necrotizing enterocolitis by modulating intestinal injuryand repair. J Immunol 179: 4808–4820, 2007.
64. Leaphart CL, Qureshi F, Cetin S, Li J, Dubowski T, Baty C,Beer-Stolz D, Guo F, Murray SA, Hackam DJ. Interferon-gammainhibits intestinal restitution by preventing gap junction communicationbetween enterocytes. Gastroenterology 132: 2395–2411, 2007.
65. Li W, Teng F, Li T, Zhou Q. Simultaneous generation and germlinetransmission of multiple gene mutations in rat using CRISPR-Cas sys-tems. Nat Biotechnol 31: 684–686, 2013.
66. Liedel JL, Guo Y, Yu Y, Shiou SR, Chen S, Petrof EO, Hu S, MuschMW, Claud EC. Mother’s milk-induced Hsp70 expression preservesintestinal epithelial barrier function in an immature rat pup model.Pediatr Res 69: 395–400, 2011.
67. Liu Y, Zhu L, Fatheree NY, Liu X, Pacheco SE, Tatevian N, RhoadsJM. Changes in intestinal Toll-like receptors and cytokines precedehistological injury in a rat model of necrotizing enterocolitis. Am JPhysiol Gastrointest Liver Physiol 297: G442–G450, 2009.
68. Lu J, Pierce M, Franklin A, Jilling T, Stafforini DM, Caplan M. Dualroles of endogenous platelet-activating factor acetylhydrolase in a murinemodel of necrotizing enterocolitis. Pediatr Res 68: 225–230, 2010.
69. Lu P, Sodhi CP, Hackam DJ. Toll-like receptor regulation of intestinaldevelopment and inflammation in the pathogenesis of necrotizing entero-colitis. Pathophysiology 21: 81–93, 2014.
70. Luke CJ, Pak SC, Askew YS, Naviglia TL, Askew DJ, Nobar SM,Vetica AC, Long OS, Watkins SC, Stolz DB, Barstead RJ, MoulderGL, Bromme D, Silverman GA. An intracellular serpin regulatesnecrosis by inhibiting the induction and sequelae of lysosomal injury.Cell 130: 1108–1119, 2007.
71. Martin NA, Mount Patrick SK, Estrada TE, Frisk HA, Rogan DT,Dvorak B, Halpern MD. Active transport of bile acids decreases mucin2 in neonatal ileum: implications for development of necrotizing entero-colitis. PloS One 6: e27191, 2011.
72. Mizrahi A, Barlow O, Berdon W, Blanc WA, Silverman WA. Necro-tizing enterocolitis in premature infants. J Pediatr 66: 697–705, 1965.
73. Nanthakumar NN, Young C, Ko JS, Meng D, Chen J, Buie T,Walker WA. Glucocorticoid responsiveness in developing human intes-tine: possible role in prevention of necrotizing enterocolitis. Am J PhysiolGastrointest Liver Physiol 288: G85–G92, 2005.
74. Neal MD, Jia H, Eyer B, Good M, Guerriero CJ, Sodhi CP, Afrazi A,Prindle T Jr, Ma C, Branca M, Ozolek J, Brodsky JL, Wipf P,Hackam DJ. Discovery and validation of a new class of small moleculeToll-like receptor 4 (TLR4) inhibitors. PloS One 8: e65779, 2013.
75. Neal MD, Sodhi CP, Dyer M, Craig BT, Good M, Jia H, Yazji I,Afrazi A, Richardson WM, Beer-Stolz D, Ma C, Prindle T, Grant Z,Branca MF, Ozolek J, Hackam DJ. A critical role for TLR4 inductionof autophagy in the regulation of enterocyte migration and the pathogen-esis of necrotizing enterocolitis. J Immunol 190: 3541–3551, 2013.
76. Neal MD, Sodhi CP, Jia H, Dyer M, Egan CE, Yazji I, Good M,Afrazi A, Marino R, Slagle D, Ma C, Branca MF, Prindle T Jr, GrantZ, Ozolek J, Hackam DJ. Toll-like receptor 4 is expressed on intestinalstem cells and regulates their proliferation and apoptosis via the p53
up-regulated modulator of apoptosis. J Biol Chem 287: 37296–37308,2012.
77. Neu J. Necrotizing enterocolitis: the search for a unifying pathogenictheory leading to prevention. Pediatr Clin N Am 43: 409–432, 1996.
78. Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med 364:255–264, 2011.
79. Okada K, Fujii T, Ohtsuka Y, Yamakawa Y, Izumi H, Yamashiro Y,Shimizu T. Overfeeding can cause NEC-like enterocolitis in prematurerat pups. Neonatology 97: 218–224, 2010.
80. Okur H, Kucukaydin M, Kose K, Kontas O, Dogam P, Kazez A.Hypoxia-induced necrotizing enterocolitis in the immature rat: the role oflipid peroxidation and management by vitamin E. J Pediatr Surg 30:1416–1419, 1995.
81. Puiman P, Stoll B. Animal models to study neonatal nutrition inhumans. Curr Opin Clin Nutr Metab Care 11: 601–606, 2008.
82. Qureshi FG, Leaphart C, Cetin S, Li J, Grishin A, Watkins S, FordHR, Hackam DJ. Increased expression and function of integrins inenterocytes by endotoxin impairs epithelial restitution. Gastroenterology128: 1012–1022, 2005.
83. Richardson WM, Sodhi CP, Russo A, Siggers RH, Afrazi A, GribarSC, Neal MD, Dai S, Prindle T Jr, Branca M, Ma C, Ozolek J,Hackam DJ. Nucleotide-binding oligomerization domain-2 inhibits toll-like receptor-4 signaling in the intestinal epithelium. Gastroenterology139: 904–917, 917.e1–e6, 2010.
84. Sangild PT, Petersen YM, Schmidt M, Elnif J, Petersen TK, Bud-dington RK, Greisen G, Michaelsen KF, Burrin DG. Preterm birthaffects the intestinal response to parenteral and enteral nutrition innewborn pigs. J Nutr 132: 3786–3794, 2002.
85. Sangild PT, Siggers RH, Schmidt M, Elnif J, Bjornvad CR, Thy-mann T, Grondahl ML, Hansen AK, Jensen SK, Boye M, Moelbak L,Buddington RK, Westrom BR, Holst JJ, Burrin DG. Diet- andcolonization-dependent intestinal dysfunction predisposes to necrotizingenterocolitis in preterm pigs. Gastroenterology 130: 1776–1792, 2006.
86. Schulz S, Wong RJ, Jang KY, Kalish F, Chisholm KM, Zhao H,Vreman HJ, Sylvester KG, Stevenson DK. Heme oxygenase-1 defi-ciency promotes the development of necrotizing enterocolitis-like intes-tinal injury in a newborn mouse model. Am J Physiol Gastrointest LiverPhysiol 304: G991–G1001, 2013.
87. Seisenbacher G, Hafen E, Stocker H. MK2-dependent p38b signallingprotects Drosophila hindgut enterocytes against JNK-induced apoptosisunder chronic stress. PLoS Genet 7: e1002168, 2011.
88. Shiou SR, Yu Y, Guo Y, He SM, Mziray-Andrew CH, Hoenig J, SunJ, Petrof EO, Claud EC. Synergistic protection of combined probioticconditioned media against neonatal necrotizing enterocolitis-like intesti-nal injury. PloS One 8: e65108, 2013.
89. Sibbons P, Spitz L, van Velzen D, Bullock GR. Relationship of birthweight to the pathogenesis of necrotizing enterocolitis in the neonatalpiglet. Pediatr Pathol 8: 151–162, 1988.
90. Sibbons PD, Spitz L, van Velzen D. Necrotizing enterocolitis inducedby local circulatory interruption in the ileum of neonatal piglets. PediatrPathol 12: 1–14, 1992.
91. Siggers J, Ostergaard MV, Siggers RH, Skovgaard K, Molbak L,Thymann T, Schmidt M, Moller HK, Purup S, Fink LN, Frokiaer H,Boye M, Sangild PT, Bering SB. Postnatal amniotic fluid intake reducesgut inflammatory responses and necrotizing enterocolitis in pretermneonates. Am J Physiol Gastrointest Liver Physiol 304: G864–G875,2013.
92. Siggers RH, Siggers J, Boye M, Thymann T, Molbak L, Leser T,Jensen BB, Sangild PT. Early administration of probiotics alters bacte-rial colonization and limits diet-induced gut dysfunction and severity ofnecrotizing enterocolitis in preterm pigs. J Nutr 138: 1437–1444, 2008.
93. Siggers RH, Thymann T, Jensen BB, Molbak L, Heegaard PM,Schmidt M, Buddington RK, Sangild PT. Elective cesarean deliveryaffects gut maturation and delays microbial colonization but does notincrease necrotizing enterocolitis in preterm pigs. Am J Physiol RegulIntegr Comp Physiol 294: R929–R938, 2008.
94. Silverman GA, Luke CJ, Bhatia SR, Long OS, Vetica AC, Perlmut-ter DH, Pak SC. Modeling molecular and cellular aspects of humandisease using the nematode Caenorhabditis elegans. Pediatr Res 65:10–18, 2009.
95. Sodhi CP, Neal MD, Siggers R, Sho S, Ma C, Branca MF, Prindle TJr, Russo AM, Afrazi A, Good M, Brower-Sinning R, Firek B,Morowitz MJ, Ozolek JA, Gittes GK, Billiar TR, Hackam DJ.Intestinal epithelial Toll-like receptor 4 regulates goblet cell development
Themes
G927ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org

and is required for necrotizing enterocolitis in mice. Gastroenterology143: 708–718.e1–e5, 2012.
96. Takeishi A, Kuranaga E, Tonoki A, Misaki K, Yonemura S, KanukaH, Miura M. Homeostatic epithelial renewal in the gut is required fordampening a fatal systemic wound response in Drosophila. Cell Rep 3:919–930, 2013.
97. Tesson L, Usal C, Menoret S, Leung E, Niles BJ, Remy S, SantiagoY, Vincent AI, Meng X, Zhang L, Gregory PD, Anegon I, Cost GJ.Knockout rats generated by embryo microinjection of TALENs. NatBiotechnol 29: 695–696, 2011.
98. Thymann T, Moller HK, Stoll B, Stoy AC, Buddington RK, BeringSB, Jensen BB, Olutoye OO, Siggers RH, Molbak L, Sangild PT,Burrin DG. Carbohydrate maldigestion induces necrotizing enterocolitisin preterm pigs. Am J Physiol Gastrointest Liver Physiol 297: G1115–G1125, 2009.
99. van Acker J, de Smet F, Muyldermans G, Bougatef A, Naessens A,Lauwers S. Outbreak of necrotizing enterocolitis associated with En-terobacter sakazakii in powdered milk formula. J Clin Microbiol 39:293–297, 2001.
100. van Haver ER, Oste M, Thymann T, Sys SU, Lamers WH, WeynsAL, Sangild PT, van Ginneken CJ. Enteral feeding reduces endothelialnitric oxide synthase in the caudal intestinal microvasculature of pretermpiglets. Pediatr Res 63: 137–142, 2008.
101. Waterston RH, Lindblad-Toh K, Birney E, Rogers J, Abril JF,Agarwal P, Agarwala R, Ainscough R, Alexandersson M, An P,Antonarakis SE, Attwood J, Baertsch R, Bailey J, Barlow K, Beck S,Berry E, Birren B, Bloom T, Bork P, Botcherby M, Bray N, BrentMR, Brown DG, Brown SD, Bult C, Burton J, Butler J, CampbellRD, Carninci P, Cawley S, Chiaromonte F, Chinwalla AT, ChurchDM, Clamp M, Clee C, Collins FS, Cook LL, Copley RR, Coulson A,Couronne O, Cuff J, Curwen V, Cutts T, Daly M, David R, Davies J,Delehaunty KD, Deri J, Dermitzakis ET, Dewey C, Dickens NJ,Diekhans M, Dodge S, Dubchak I, Dunn DM, Eddy SR, Elnitski L,Emes RD, Eswara P, Eyras E, Felsenfeld A, Fewell GA, Flicek P,Foley K, Frankel WN, Fulton LA, Fulton RS, Furey TS, Gage D,Gibbs RA, Glusman G, Gnerre S, Goldman N, Goodstadt L, Graf-ham D, Graves TA, Green ED, Gregory S, Guigo R, Guyer M,Hardison RC, Haussler D, Hayashizaki Y, Hillier LW, Hinrichs A,Hlavina W, Holzer T, Hsu F, Hua A, Hubbard T, Hunt A, JacksonI, Jaffe DB, Johnson LS, Jones M, Jones TA, Joy A, Kamal M,Karlsson EK, Karolchik D, Kasprzyk A, Kawai J, Keibler E, Kells C,Kent WJ, Kirby A, Kolbe DL, Korf I, Kucherlapati RS, KulbokasEJ, Kulp D, Landers T, Leger JP, Leonard S, Letunic I, Levine R, LiJ, Li M, Lloyd C, Lucas S, Ma B, Maglott DR, Mardis ER, Matthews
L, Mauceli E, Mayer JH, McCarthy M, McCombie WR, McLaren S,McLay K, McPherson JD, Meldrim J, Meredith B, Mesirov JP,Miller W, Miner TL, Mongin E, Montgomery KT, Morgan M, MottR, Mullikin JC, Muzny DM, Nash WE, Nelson JO, Nhan MN, NicolR, Ning Z, Nusbaum C, O’Connor MJ, Okazaki Y, Oliver K,Overton-Larty E, Pachter L, Parra G, Pepin KH, Peterson J, Pe-vzner P, Plumb R, Pohl CS, Poliakov A, Ponce TC, Ponting CP,Potter S, Quail M, Reymond A, Roe BA, Roskin KM, Rubin EM,Rust AG, Santos R, Sapojnikov V, Schultz B, Schultz J, SchwartzMS, Schwartz S, Scott C, Seaman S, Searle S, Sharpe T, Sheridan A,Shownkeen R, Sims S, Singer JB, Slater G, Smit A, Smith DR,Spencer B, Stabenau A, Stange-Thomann N, Sugnet C, Suyama M,Tesler G, Thompson J, Torrents D, Trevaskis E, Tromp J, Ucla C,Ureta-Vidal A, Vinson JP, Von Niederhausern AC, Wade CM, WallM, Weber RJ, Weiss RB, Wendl MC, West AP, Wetterstrand K,Wheeler R, Whelan S, Wierzbowski J, Willey D, Williams S, WilsonRK, Winter E, Worley KC, Wyman D, Yang S, Yang SP, ZdobnovEM, Zody MC, Lander ES. Initial sequencing and comparative analysisof the mouse genome. Nature 420: 520–562, 2002.
102. Wolfs TG, Derikx JP, Hodin CM, Vanderlocht J, Driessen A, deBruïne AP, Bevins CL, Lasitschka F, Gassler N, van Gemert WG,Buurman WA. Localization of the lipopolysaccharide recognition com-plex in the human healthy and inflamed premature and adult gut. InflammBowel Dis 16: 68–75, 2010.
103. Yazji I, Sodhi CP, Lee EK, Good M, Egan CE, Afrazi A, Neal MD,Jia H, Lin J, Ma C, Branca MF, Prindle T, Richardson WM, OzolekJ, Billiar TR, Binion DG, Gladwin MT, Hackam DJ. EndothelialTLR4 activation impairs intestinal microcirculatory perfusion in necro-tizing enterocolitis via eNOS-NO-nitrite signaling. Proc Natl Acad SciUSA 110: 9451–9456, 2013.
104. Young CM, Kingma SD, Neu J. Ischemia-reperfusion and neonatalintestinal injury. J Pediatr 158: e25–e28, 2011.
105. Yu X, Radulescu A, Zorko N, Besner GE. Heparin-binding EGF-likegrowth factor increases intestinal microvascular blood flow in necrotizingenterocolitis. Gastroenterology 137: 221–230, 2009.
106. Zamora R, Vodovotz Y, Betten B, Wong C, Zuckerbraun B, GibsonKF, Ford HR. Intestinal and hepatic expression of BNIP3 in necrotizingenterocolitis: regulation by nitric oxide and peroxynitrite. Am J PhysiolGastrointest Liver Physiol 289: G822–G830, 2005.
107. Zuckerbraun BS, Otterbein LE, Boyle P, Jaffe R, Upperman J,Zamora R, Ford HR. Carbon monoxide protects against the develop-ment of experimental necrotizing enterocolitis. Am J Physiol GastrointestLiver Physiol 289: G607–G613, 2005.
Themes
G928 ANIMAL MODELS OF NECROTIZING ENTEROCOLITIS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00422.2013 • www.ajpgi.org