Embed Size (px)
Citation preview

Advanced Drug Delivery Reviews 50 (2001) 45–60www.elsevier.com/ locate /drugdeliv
Animal models for the study of intestinal lymphatic drugtransport
a b bGlenn A. Edwards , Christopher J.H. Porter , Suzanne M. Caliph ,b b ,*Shui-Mei Khoo , W.N. Charman
a
Department of Veterinary Science, University of Melbourne, 250 Princes Highway, Werribee, Victoria 3030, AustraliabDepartment of Pharmaceutics, Victorian College of Pharmacy, Monash University, 381 Royal Parade, Parkville, Victoria 3052,
Australia
Received 7 January 2001; accepted 3 April 2001
Abstract
Drug transport via the intestinal lymphatic system has been shown to contribute to the absorption of a number of orallyadministered highly lipophilic drugs. In order to investigate this phenomenon and assist in the development of improved oralformulations, the use of appropriate animal models is required. This paper reviews the use of various animal models for thispurpose, and describes in detail the conscious rat and dog models used in our laboratory. The advantages and disadvantagesof both small and large animal models are explored, as well as the factors which have been found to influence the outcomeof intestinal lymphatic drug transport studies with these models. 2001 Elsevier Science B.V. All rights reserved.
Keywords: Thoracic duct; Mesenteric duct; Dog; Rat; Cannulation
Contents
1. Introduction ............................................................................................................................................................................ 462. Anatomy and physiology of the lymphatic system ..................................................................................................................... 463. Animal models used for intestinal lymphatic transport studies .................................................................................................... 47
3.1. Small animal models ........................................................................................................................................................ 473.1.1. The unconscious rat model...................................................................................................................................... 473.1.2. Conscious restrained rat models .............................................................................................................................. 483.1.3. A conscious un-restrained rat model ........................................................................................................................ 48
3.1.3.1. Methodology............................................................................................................................................. 493.1.3.2. Assessment of the efficiency of lipid absorption in the conscious rat model ................................................... 51
3.1.4. Conclusions ........................................................................................................................................................... 513.2. Large animal models ........................................................................................................................................................ 52
3.2.1. Pig models............................................................................................................................................................. 52
*Corresponding author. Tel.: 1 61-3-9903-9519; fax: 1 61-3-9903-9583.E-mail address: [email protected] (W.N. Charman).
0169-409X/01/$ – see front matter 2001 Elsevier Science B.V. All rights reserved.PI I : S0169-409X( 01 )00148-X

46 G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60
3.2.2. Sheep models......................................................................................................................................................... 523.2.3. Dog models ........................................................................................................................................................... 53
3.2.3.1. Methodology............................................................................................................................................. 533.2.3.2. Assessment of the efficiency of lipid absorption in the conscious dog model .................................................. 54
4. Model related factors influencing the outcome of intestinal drug transport studies ........................................................................ 565. Conclusions ............................................................................................................................................................................ 57References .................................................................................................................................................................................. 58
1. Introduction anatomy and physiology, it is necessary to developboth reliable and appropriate animal models in order
Studies of the uptake and transport of drugs into to investigate the processes involved in the uptake ofthe body via the intestinal lymphatic system have drugs via the intestinal lymphatic system.received increasing attention in recent years [1–6]. This article will review the use of animal modelsDrug transport via the intestinal lymphatic system used in the investigation of the intestinal lymphatichas been shown to contribute to the absorption of a absorption of drugs, and will describe the advantagesnumber of highly lipophilic drugs when administered and disadvantages of both small and large animalorally [3,5–10], and can have a considerable impact models. A detailed description of the surgical pro-on the absorption and metabolic profile of the drug cedures used in our laboratory to establish theserelative to absorption via the portal system. As well models, along with the data used to validate theas increasing the bioavailability of these drugs, there models with respect to lipid absorption will also beare other potential advantages for this route of described.absorption such as avoidance of hepatic first-passmetabolism, direct targeting of the lymphoid tissue,and indirect targeting of specific sites associated with 2. Anatomy and physiology of the lymphaticlow-density lipoprotein receptors [11,12]. The trans- systemport of lipophilic compounds via the intestinallymphatics generally occurs in tandem with lipopro- The lymphatic system consists of a system oftein biosynthesis, and consequently a common ap- lymphatic ducts and lymph nodes which serve toproach for enhancing lymphatic drug transport via transport and drain the interstitial space and gastroin-oral administration is the co-administration of appro- testinal tract of excess fluid, proteins and lipids thatpriate lipids. are not reabsorbed by the blood capillaries to the
The time scale of lymphatic transport is slower systemic circulation. Unlike the vascular system, thethan that for portal blood absorption owing to the lymphatic system has a unidirectional flow of lymphcomplex sequence of events inherent in lymphatic from the peripheral tissues and viscera to the centraltransport. Therefore, the plasma profile of a drug blood circulation. The small terminal lymphatics inabsorbed via the portal blood as well as transported the peripheral tissues of the body collect lymph andvia the lymphatics would typically be broad, reflect- unite to form a series of collecting (afferent)ing the slow input of lipoproteins (and associated lymphatic ducts which transport lymph to the re-drug) to the systemic circulation. This may also gional lymph nodes [14]. Postnodal (efferent)result in the appearance of double peaks in plasma lymphatic ducts move the lymph between successiveprofiles, although this can also arise through gastric sets of lymph nodes and ducts into the cisterna chyliemptying and/or resolubilization effects leading to which acts as a collecting reservoir, receiving lymphportal blood absorption [13]. from lymphatic vessels draining the caudal peripher-
Significant differences exist, however, in the meth- al tissues, intestinal, hepatic and lumbar areas. Theods and animal models used to study intestinal major lymphatic vessel, the thoracic duct, runs fromlymph drug transport, making comparison across the cisterna chyli through the thorax alongside thedata sets difficult. Due to the complex nature of the aorta, collecting further lymph from the mediastinumintestinal lymphatic system in regard to both and cranial parts of the body, to empty directly into

G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60 47
the venous system at the junction of the left jugular the systemic circulation. Different animal and sur-vein and the left subclavian vein. gical models may impact on the apparent efficacy of
All lymph therefore passes through at least one set lymphatic transport. Awareness of how these meth-of lymph nodes on its passage from the periphery or odological differences can influence lymphatic trans-intestinal tract back to systemic circulation [15]. port is therefore critical when interpreting and asses-Lymph enters the lymph node via one, or many, sing lymphatic transport data.afferent lymph ducts and flows through medullarysinuses lined with large numbers of macrophages 3.1. Small animal modelswhich are responsible for the phagocytosis of cellularand particulate material. The lymph exits the node Although there have been a number of animalthrough the hilus into (usually) a single efferent models described in the literature for estimatinglymphatic. The exchange of various materials be- intestinal lymphatic drug transport, and for assess-tween the blood and lymph occurs within the lymph ment of the effect of different formulations andnode, however, the mechanisms of this exchange are experimental factors on this process, the majority ofpoorly understood. The lymph nodes are also a the studies have, until recently, predominantly beencentre for lymphocyte proliferation with B-lympho- performed in anaesthetised rats.cytes, T-lymphocytes, and B-lymphocyte-derivedantibodies entering the lymph via the lymph nodes 3.1.1. The unconscious rat model[16]. Numerous experimental protocols have been re-
The intestinal lymphatics perform a specialised ported for the assessment of intestinal lymphaticfunction, namely the transport of absorbed lipids drug transport in the rat [17–21]. The generalfrom the intestine to the systemic circulation. methodological differences associated with the dif-Lipoproteins, synthesised in the enterocyte pass into ferent preparations include site of cannulation andthe mesenteric lymphatic capillaries draining the lymph fistulation, and variations in animal treatmentsmall intestine and subsequently progress from the before and after the surgery (in terms of feeding andmesenteric lymph via the cisterna chyli into the rehydration, dosing and sampling procedures). Thethoracic lymph. In general, lipophilic drugs that are unconscious rat model used in our laboratory hastransported to the systemic circulation via the intesti- been previously described by Porter et al. [22], and isnal lymphatics do so in association with lymph based on protocols used elsewhere [8,19]. The modellipoproteins, and therefore follow the same path to includes the cannulation of the carotid artery for thethe systemic circulation. collection of systemic blood samples; the mesenteric
Significant variations can however exist in the lymph duct for collection of intestinal lymph; theexact anatomical arrangement of the lymphatic sys- duodenum for the administration of rehydrationtem, both between species, and between individuals solution and, if necessary, the jugular vein to facili-within a species, and this can lead to surgical tate intravenous administration.complications when trying to access the lymphatics As cannulation of the mesenteric lymph in thisand reproducibly assess the extent of lymphatic drug model essentially collects all the lymph draining thetransport. small intestine, the absolute quantity of drug trans-
ported is simply calculated by multiplication of theconcentration in lymph by the corresponding volume
3. Animal models used for intestinal lymphatic of lymph produced (assessed gravimetrically) duringtransport studies each collection period. It is also important, however,
to determine the extent of absorption occurring viaDrug transport via the intestinal lymphatics is the the portal blood to fully characterise the oral bio-
culmination of a number of steps which include availability of the drug. In this regard, it is reason-absorption via the enterocyte, association with the able to assume that systemic plasma concentrationsproducts of lipid digestion, secretion into the mesen- of drug in the lymph-fistulated rat reflect absorptionteric lymph, and transport via the thoracic duct into of drug via the portal blood. Therefore, the contribu-

48 G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60
tion of portal blood absorption to bioavailability can ing cage or strapped in a harness containing change-be determined by comparison of the relative areas able lymph collection bottles [1,21,24]. In the con-under the plasma concentration–time profiles ob- scious rat model described by Raub et al. [1], thetained in orally dosed lymph-fistulated rats and in a methodology is similar to that described for theparallel group of sham operated animals after in- anaesthetised model (Section 3.1.1) except that thetravenous administration. lymph and jugular vein cannulas are tunnelled under
The use of anaesthetised animals in the study of the skin to exit the animal at the back of the neck,intestinal lymphatic drug transport has a number of where they are connected to a saddle / swivel leashadvantages, most significantly the removal of prob- arrangement to allow continuous infusion and sam-lems associated with animal movement during lymph pling. In this case, the jugular line is used for bothcollection. In this regard, one of the most common saline rehydration (1–2 ml /h) and blood sampling.reasons for experimental failure in lymphatic trans- The protocol describes a 3-day recovery periodport studies is occlusion of the cannula draining the between jugular vein surgery and lymphatic cannula-lymph, and this is considerably more likely in freely tion, and a 2-day recovery period after abdominalmoving animals. Lymph flow rate, however is in- surgery. As the rats are orally dosed and rehydratedfluenced by the conscious state of the animal. In intravenously, there is no need in this model for theanaesthetised rats, it ranges between 0.1–0.6 ml /h intraduodenal cannula used in the unconsciousand in the un-anaesthetised rats it may increase up to model. Whilst these systems are an improvement1–3 ml /h [23]. This reduction in lymph flow in the over anaesthetised models, restraint and the positionanaesthetised animal may be explained by a decrease of the saddle strap may have negative impact onin motility and function of the gastrointestinal tract, lymph formation and lymph flow rate by compromis-altered capillary permeability and reduced interstitial ing venous return and normal gastrointestinal func-fluid formation and venous return in anaesthetised, as tioning [1]. Consequently, a fully conscious un-re-opposed to conscious animals. Furthermore, the rate strained rat model has been developed in our labora-of absorption of poorly water soluble, lipophilic tory, and others [25], for the investigation ofdrugs such as those which are likely to be candidates lymphatic drug transport after oral administration.for intestinal lymphatic transport is generally slow. This model allows for oral dosing, continuous lymphConsequently, an extended period of anaesthesia collection over 12 h and simultaneous systemic(16–24 h including surgery) is usually required to blood collection over 30 h.collect a complete pharmacokinetic profile. Theimplications of such an extended period of anaes-thesia include unacceptably high mortality rates and 3.1.3. A conscious un-restrained rat modelalso considerable logistical problems when running In general, the model is designed to facilitate thean experiment, since the anaesthetised animals re- conduct of a parallel study with both orally dosedquire continual observation over the experimental and intravenously dosed groups of rats. Surgicalperiod. In addition, oral formulations are commonly procedures for orally dosed rats include mesentericadministered to anaesthetised animals via the cannula lymph duct fistulation for continuous lymph collec-implanted within the duodenum (i.e. intra-duodenal tion, carotid artery cannulation for systemic blooddosing). Consequently, the potential beneficial effect collection and intra-duodenal cannulation for over-of effective shear and mixing on gastric emptying night rehydration. A second orally dosed group mayand lipid digestion within the stomach are largely be included to assess overall bioavailability in nonneglected [21]. lymph-cannulated animals, which do not have can-
nulae implanted in the mesenteric lymph duct, but3.1.2. Conscious restrained rat models maintain cannulae in the carotid artery and
Increasingly, conscious restrained rat models have duodenum. A control group of animals may also bebeen employed in lymphatic drug delivery studies. used to allow estimation of absolute bioavailability.Most commonly, animals are allowed to recover In this case, rats have cannulae implanted in the rightfrom anaesthesia and then either placed in a restrain- jugular vein for dose administration, the left carotid

G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60 49
artery for systemic blood sampling and the kidney. Immediately caudal and parallel to the lymphduodenum for rehydration. duct, the mesenteric artery appears as a pulsating
All surgical procedures are performed in non- dark red vessel. Occasionally, a small branch of thefasted animals. This offers a surgical advantage in lymph vessel (an accessory or inferior mesentericlymph-cannulated animals as non-fasted animals lymph duct) may be present caudal to the muchprovide for better visualisation of the mesenteric larger superior mesenteric lymph duct.lymph duct and therefore minimise experimental The three-part mesenteric lymph cannula is con-failures. Animals are fasted during the recovery structed from a 4-mm length of polyethylene (PE)period to allow lymph and plasma TG levels to tubing (0.5 mm I.D., 0.8 mm O.D.), connected to a
return to basal (fasting) levels prior to dosing. 5-cm length of flexible Silastic tube (0.51 mm I.D.,0.94 mm O.D.) connected to a further 20-cm length
3.1.3.1. Methodology of PE tubing (0.5 mm I.D., 0.8 mm O.D.). ThisSurgical anaesthesia is initiated in the rat by the cannula is passed underneath the peri-renal fat bed at
intra-peritoneal (i.p.) injection of 3 ml /kg of an the lower margin of the right kidney and through theinduction solution ‘FFM’, containing 1 part (by connective tissue layers immediately below the vena
volume) Hypnorm (fluanisone 10 mg/ml, fentanyl cava, in a direction parallel with the superior mesen-0.2 mg/ml), 1 part Hypnovel (midazolam 5 mg/ teric lymph duct, such that the short (4 mm) end of
ml) and 2 parts purified water [26]. This combination the cannula is immediately adjacent to the mesentericproduces neuroleptanalgesia with profound surgical lymph duct. Prior to cannulation, the mesentericanaesthesia and good muscle relaxation in rats within lymph duct is isolated from the layers of connective2–5 min of intra-peritoneal (i.p.) injection, without tissues and surrounding fatty tissues by blunt dissec-significant salivary production or bronchial secretion. tion. This is essential, as insufficient isolation orFor the duration of the surgery, additional i.p. doses cleaning of the lymph duct will frequently lead to theof 0.5–1 ml /kg of the solution can be administered insertion of the cannula between the lymph duct andevery 20–40 min. connective tissue layers resulting in poor or no
3.1.3.1.1. Mesenteric lymph duct cannulation The lymph flow. After isolating the lymph duct, a smallrat is placed in dorsal recumbency on a heated hole is made (closer to the vena cava than the lymph(378C) surgical pad, which is used to maintain the node) with the aid of iridectomy scissors, taking carebody temperature of the animal during all surgical not to completely sever the vessel, the short (4 mm)procedures. An area of abdominal skin from the right end of the lymph cannula (previously filled with 1%flank to the mid-line is shaved two inches down from disodium EDTA as an anticoagulant) is then insertedthe right costal margin and aseptically prepared with into the mesenteric lymphatic for approximately 2–4antiseptic solutions. A straight para-costal incision mm of its length. After the cannula is in place,extending from the xiphoid process to the right flank gradual flow of firstly anticoagulant solution fol-is made 1.5 cm below the costal margin. A 4.5-cm lowed by intestinal lymph should be seen from theincision is then made through the exposed abdominal free collecting end of the cannula. After effectivemuscle wall from 4 to 5 mm lateral to the mid line to cannulation of the lymph duct is ascertained, thethe right flank. The small intestine is retracted and cannula is secured by placing a small drop ofgently pushed under the left abdominal muscle wall cyanoacrylate glue over the entry point of theusing two or three pieces of sterile gauze saturated cannula. If an accessory lymph duct is present, this iswith normal saline. To enhance visualisation of the severed and occluded with superglue. The cannula ismesenteric lymph duct, the rat can be ‘bridged’ over then tunnelled to exit at the back of the neck, anda 10-ml plastic syringe placed horizontally under the attached to a swivel / tether to allow free movementrat at the level of right kidney and the right hind of the animal.limb. The superior mesenteric lymph duct can be 3.1.3.1.2. Duodenal cannulation Cannulation ofvisualised as a white opaque vessel, approximately the duodenum is performed using a 30-cm piece of0.8 mm in diameter in a 300-g rat, and running PE 50 tubing that is tunnelled subcutaneously fromtransversely at the level of the hilum of the right the back of the neck to emerge near the right flank.

50 G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60
Prior to insertion a small portion of the cannula artery is then dilated with the aid of angled jewellerstoward the insertion end is looped back on itself and forceps and the heparin saline filled cannula slowlylightly heated to form a U-shaped anchor point 2 cm inserted toward the clavicle. The forceps occludingfrom the bevelled tip. The duodenum can be iden- the blood flow are then removed and the cannulatified as the bright pink (more vascular and thinned rapidly advanced to the 2.5-cm mark. A smallwall) section of the small intestine, which upon volume of blood is aspirated to ascertain the patencygentle downward traction exposes the pyloric sphinc- of the cannula and the line flushed until filled withter and stomach. A small puncture hole is made clear anticoagulant solution. Finally, the cannula isapproximately 2 cm below the pylorus with a 23-G secured in the vessel by firmly knotting the twoneedle through which the cannula can be inserted ligatures. A third tie may also be introduced in-and glued into place. After completion of the intra- between the two ties. The heparinised saline filledduodenal cannulation, the abdominal incision in the syringe is subsequently removed from the end of theabdominal muscle wall is sutured using simple cannula and the open end of the cannula is heat-interrupted stitches of 3-O silk. The skin incision is sealed. The cannula is then tunnelled subcutaneouslyclosed by applying a few drops of tissue adhesive around the neck and beneath the left ear and(cyanacrylate) along the side of the incision and exteriorised at the back of the neck through the exitpinching the skin up well away from the underlying used for the lymph and duodenal cannulae. The skinmusculature, and opposing. incision on the throat is closed by a continuous
3.1.3.1.3. Carotid artery cannulation The carotid suture using 3-O polydioxanone sutures.artery is cannulated using a cannula prepared from a 3.1.3.1.4. Jugular vein cannulation To cannulate50-cm length of PE 50 tubing with one end bevelled the jugular vein, a 2.5-cm vertical skin incision isat an angle of 308. A mark 2.5 cm from the bevel is centred over the intersection of two imaginary lines;made using a permanent marker to identify the one line connecting the right ear and left elbow, theportion of the tubing that should be inserted into the other connecting the chin and the right elbow. Theartery. The other end of the cannula is connected to a connective and adipose tissues are subsequentlysyringe filled with heparin (20 Units /ml) in normal dissected to expose the external jugular vein, and thesaline. The cannula is soaked with the anticoagulant vein carefully isolated and mobilised to provide asolution overnight. To facilitate cannulation, the 1-cm section immediately caudal to the bifurcation.anaesthetised rat is placed in dorsal recumbency with Small artery clamps are used to occlude the vessel atthe neck stretched and head pointing towards the the point of bifurcation and the vein ligated at twooperator. The area over the throat and the clavicle points using 3-O silk sutures, one immediatelyregion is shaved and aseptically prepared. A 2.5-cm rostral to the clamp, and the second loosely aroundlongitudinal incision is made along the left of the the vessel closer to the clavicle end of the exposedtrachea in the sagittal plane. The tough subcutaneous section. A small hole is then cut between the twoconnective tissues are then dissected away to expose ligatures, and the jugular vein cannula, filled withthe underlying paired neck muscles. These muscles heparinised saline solution (20 IU/ml) insertedare retracted to reveal the left carotid artery, which is whilst gently lifting the chest by the skin to preventcleaned of overlying connective tissue, and a 1-cm the cannula entering the subclavicular vein. Thelong section carefully isolated, taking care not to cannula should be previously marked at 3.5 cm fromdamage the adjacent vagal nerve track. A 20-cm the bevelled tip in order to assess the extent ofpiece of 3-O silk thread is then passed beneath the insertion. When the cannula is inserted to the 3.5-cmartery and the vessel ligated. The ends of this tie are mark, the tip of the cannula should be at the level ofthen clamped using a pair of baby-mosquito forceps, the right atrium. Patent cannulation is ascertained byand a second piece of silk thread tied loosely at the blood aspiration after which the cannula is gentlyopposite end of the exposed section of the artery flushed with anticoagulant. The artery forceps arecloser to the clavicle. The artery is then carefully then removed and the two ligatures tied to anchor thelifted to occlude the blood flow by sliding forceps cannula into the vessel. The free end of the cannulaunderneath it. At this point, a small cut is made in is sealed by heating and is tunnelled subcutaneouslythe artery using iridectomy scissors. The hole in the around the neck to emerge at the back of the neck.

G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60 51
The skin incision in the neck is then closed by a chain triglyceride lipid (peanut oil) and found to becontinuous suture of 3-O polydioxanone suture. quite constant with respect to time (1.160.1 g/h,
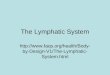
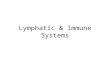
3.1.3.1.5. Post-surgical recovery Following the mean6S.E., n 5 4), although an increase was seensurgical procedures, the animal is left on a heated during the first 4 h post dose. These values areplate (378C) to fully recover from the anaesthesia similar to the value (1.660.4 ml /h) previouslybefore transferring to a wire bottom cage. A small obtained in conscious restrained rats after intra-du-harness which allows connection of the swivel tether odenal infusion with 0.9% normal saline at a rate ofis then placed around the front paws of the animal. 2.2 ml /h [1]. Peak lymph output was found to occurThe harness is attached to the swivel tether using 2–3 h after lipid dosing (Fig. 1) which was alsovelcro. Animals are not fasted prior to surgery, consistent with the previously reported time to reachhowever, food is withheld during the recovery period peak lymph flow and lymph chylomicron appearance(12–16 h) and up to 12 h post-dose. Lactated in long chain lipid infused rats [30,31]. To examineRinger’s solution is used to rehydrate the rat immedi- the efficiency of lymph lipid output in this model asately after the intra-duodenal cannula is implanted a function of time, the cumulative lymphatic trans-and is continued at 1.5 ml /h until 2 h prior to drug port of lipid (C based long chain triglyceride) was18
administration. Water is made available ad libitum assessed over 12 h (Fig. 2). The total amount of lipidfrom 3 h after dosing. As described previously, recovered in the intestinal lymph (0.14760.07 g,intra-duodenal infusion of lactated Ringer’s solution mean6S.E., n 5 4) was greater than the amount ofduring post surgical recovery is found to significantly exogenous lipid administered (0.1 g), suggesting thatimprove lymph flow [27,28]. However, in orally absorption of exogenous lipid was essentially com-dosed rats, this is discontinued 2 h prior to dosing in plete. The apparent stimulation of endogenous lipidorder to minimise any potential alteration in the synthesis by exogenous lipid administration is con-luminal dissolution profile [28,29]. Following dis- sistent with data from previous investigations [32].continuation of intra-duodenal rehydration, animalsresume normal drinking behaviour and consistently 3.1.4. Conclusionsconsume the water provided in the drinking bottles. The advantages of lymphatic transport studiesThis behaviour in addition to a return to normal performed in rats are that they are robust, inexpen-grooming behaviour is indicative of a return to sive and straightforward in regard to drug adminis-normal health and also helps to maintaining suffi- tration and sampling. The model described is rela-cient lymph flow throughout the lymph collection tively simple, inexpensive to set up, and delivers aperiod. success rate of approximately 70% when a trained
To facilitate oral dosing of conscious un-restrainedrats, a short-acting barbiturate anaesthetic, Brietal
Sodium (methohexatone sodium 5%, Lilly, Aus-tralia) at a dose of 1 ml /kg may be administeredslowly over 10 s via the jugular cannula to producerapid light anaesthesia of approximately 2-min dura-tion. This brief period of anaesthesia allows oraldosing by gavage to occur without the possibleproblem associated with animal struggling that bothmay increase the level of animal stress and thepossibility of kinking or displacement of the variouscannulae.
3.1.3.2. Assessment of the efficiency of lipid absorp-tion in the conscious rat model
To validate the model with respect to lipid absorp- Fig. 1. Mesenteric lymph flow rate (mean (g /h)6S.E., n 5 4) intion, intestinal lymph flow was assessed over 12 h conscious rats after oral administration of 0.1 g of long C chain18
following oral administration with 0.1 g of long triglyceride lipid (peanut oil).

52 G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60
accurate assessment of the modes of absorption oflipophilic drugs a number of models have beendescribed using larger animals including the dog[34–36] and pig [37].
3.2.1. Pig modelsAn anaesthetised pig model [37], which allows for
the simultaneous sampling of mesenteric lymph,hepatic portal blood and systemic blood was de-veloped by White et al. [38] on the basis of therecognised similarities between the gastro-intestinalprofile in the pig and human. This method involvedthe oral administration of a lipophilic dye (Sudan
Fig. 2. Cumulative intestinal lymphatic transport of triglyceride black) prior to the cannulation of the lymphatics to(mean % dose6S.E., n 5 4) in rats orally dosed with 0.1 g of long facilitate better visualisation of the mesenteric lymphchain (C ) triglyceride peanut oil vehicle.18 duct. However, the model allowed only for periodic
sampling (and not continuous collection) of lymphoperator is employed. Throughout the experiment, and therefore the effective quantitative assessment ofthe animals remain mobile and quickly resume the extent of intestinal lymph transport was notnormal grooming and drinking behaviour as well as possible. To this point the anaesthetised pig modelexcretory function. The model facilitates simple and has not found widespread application elsewhere.fast oral dosing of formulations, continuous collec- Conscious pig models which employ an externaltion of intestinal lymph over 12 h and simultaneous thoracic duct–venous shunt [39,40], have been de-sampling of systemic blood over 30 h. This model veloped recently, but these have only been used tohas been subsequently utilised to investigate the study lymphatic transport after the parenteral ad-lymphatic transport and absorption into the blood of ministration of proteins [40]. Since the thoracica model lipophilic directing drug from lipid-based lymph is returned to the systemic circulation inand lipid-free oral formulations [33]. models employing a thoracic duct-jugular vein shunt,
Unfortunately, limitations associated with the rat these preparations can be maintained for longlymph model make it difficult to confidently extrapo- periods, and therefore allow for the possibility oflate absolute lymphatic transport data from rats to crossed over study designs. The return of the lymphother pre-clinical and clinical situations. In the rat, to the circulation also allows simultaneous moni-bile flow is continuous and independent of food toring of lymph levels and the corresponding bloodintake, whereas in higher species, food or lipid is levels which include the systemic contribution ofrequired to stimulate the numerous digestion-related lymphatic transport. A drawback however, is thatprocesses [22]. Therefore, it is difficult to obtain pre- lymph is only sampled, and not collected, andand post-prandial intestinal environments in the rat therefore the absolute mass of drug transported viathat are reflective of the situation in humans. From a the lymph cannot be calculated.drug delivery perspective, the small size of the ratalso precludes the administration of full size, human 3.2.2. Sheep modelsdose forms and therefore limits the examination of A conscious sheep model has been developed inlymphatic transport after dosing of realistic volumes our laboratories to study the lymphatic transport ofof lipid. proteins after subcutaneous injection [41] and is
described in more detail in a later article in this3.2. Large animal models theme issue [42]. In this preparation, thoracic lymph
is collected via direct cannulation of the thoracicIn an attempt to overcome the limitations associ- duct at its entry point into the left internal jugular
ated with the rat model and to provide a more vein after ligation of any auxiliary lymph vessels.

G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60 53
Whilst this model has been utilised in the study of duct’s entry into the vein. These factors make itlymphatic transport after parenteral administration, difficult to isolate the vein segment containing thethe differences and complexity of the gastrointestinal ampulla of the thoracic duct without causing pneu-tract of ruminants compared to monogastric species mothorax or obstruction of the venous return at thewould likely limit its application to the examination caval bifurcation. In contrast, Witte et al. [47]of lymph transport after oral administration. reported a high success rate in cannulating the
thoracic duct directly in the neck of dogs at its3.2.3. Dog models junction with the left external jugulo-subclavian
Initial reports of lymph collection in the dog venous juncture. This technique has also been de-employed methods of cannulation of the thoracic scribed by Brisco [48] using a ventral surgicalduct within the thorax, rather than mesenteric lymph approach.[43]. In 1970, Gralla et al. [44] reported a technique We have recently reported a simpler and morefor the chronic cannulation of the canine thoracic reliable method for the direct cannulation of theduct in which a T-shaped, silicone rubber cannula thoracic lymph duct as part of a triple-cannulatedwas inserted into the thoracic duct within the thorax. dog model to study intestinal lymphatic drug trans-Unfortunately, they experienced a high failure rate port [6,36]. In this model, intestinal lymphatic drugdue to clotting of lymph within the cannula. Dedo transport is determined via collection of thoracic ductand Ogura [45] also described a directly cannulated lymph directly, and portal and systemic blood isthoracic lymph model in dogs which utilised a sampled for the assessment of non-lymphatic drugclosed-system in order to collect lymphocytes in absorption and possible enterocyte-based metabo-their studies which were aimed at manipulating the lism.immune system. They directly cannulated thethoracic duct with a double-lumen cannula which 3.2.3.1. Methodologyreturned the lymph into the right external jugular Adult male greyhound dogs (28–35 kg) are used.vein when not being collected. However a continu- Each dog is fed a small lipid meal prior to premedi-ous infusion of heparinised saline was necessary to cation with acetylpromazine maleate (0.5 mg/kg),prevent clotting. The principle drawback with these by subcutaneous injection. The dog is then anaesthet-early thoracic duct cannulation models, was the need ised with an intravenous injection of propofol (3–6to perform a thoracotomy to gain access to the duct. mg/kg) and intubated. Anaesthesia is maintained byThis significantly complicates and lengthens the the delivery of halothane and oxygen. The dog alsosurgery, including the need for mechanical ventila- receives an intravenous infusion of 0.9% normaltion under anaesthesia and more intensive post- saline and an intravenous injection of the antibioticoperative care of the animals. cephazolin (20 mg/kg) and the analgesic carprofen
In 1972, Rajpal and Kirkpatrick [46] reported a (4 mg/kg).model in which thoracic duct lymph was collected 3.2.3.1.1. Portal vein cannulation The dog isvia a reservoir pouch, created by ligation of the placed in dorsal recumbency and the ventral ab-external jugular vein in the neck of dogs, above and domen is clipped and prepared for aseptic surgery. Abelow the entry of the thoracic duct into the vein. 5-cm long ventral midline laparotomy is performedInsertion of a cannula into this isolated segment of to allow a loop of jejunum to be exteriorised. Athe jugular vein allowed for chronic collection of the 133-mm (5.25 in) long, 16 Gauge cannula is thenlymph [46,1]. This method was suggested to be more inserted into a jejunal vein to the level of the portalrobust and less invasive as it avoided the vein. The cannula is stabilised in the vein with athoracotomy required to facilitate direct cannulation ligature of 3-O silk and a minimal volume extensionof the thoracic duct. tube, filled with heparinised saline is attached to the
In our experience however, this technique is a cannula. The extension tube is then externaliseddifficult and challenging surgical model because of through a separate stab incision in the left flank 4 cmthe required depth of the surgical dissection into the lateral to the midline and stabilised with sutures. Thethoracic inlet and the variability of the thoracic laparotomy wound is then closed in anatomical

54 G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60
layers with 3-O polydioxinone sutures. The position surgical wound is closed in layers with 3-O poly-of the cannula in the portal vein can be confirmed by dioxinone sutures. The externalised cannula is placedX-ray following the injection of a contrast dye in a collection bottle held in place by a bag hung(Iohexol). The patency of the cannula is maintained around the neck of the dog.by frequent flushing with a small volume of heparin- 3.2.3.1.3. Post surgical recovery Followingised saline. surgery, the dogs are allowed to recover unrestrained
3.2.3.1.2. Thoracic duct cannulation The dog is in a run for a period of 12–16 h. In the initialthen placed in right lateral recumbency with the left recovery period, fluids are administered intravenous-leg pulled caudally to facilitate cannulation of the ly to ensure adequate hydration and to preventthoracic duct. The left ventral neck area and cranial hypoproteinaemia. The dogs are allowed to return tothorax are clipped and prepared for aseptic surgery. normal ambulatory movement before the commence-A curved incision is made over the left external ment of a study. Immediately prior to the start of ajugular vein and the vein is dissected from the study, a 20-Gauge intravenous cannula is insertedsurrounding connective tissues to the axillary vein. into the left cephalic vein and kept patent throughoutExposure may be aided by retraction of the ster- the day by flushing with heparinised saline. The dogsnocephalicus muscle, and the ligation and division of are encouraged to drink water throughout the studythe distal communicating branch of the cephalic vein as long-term loss of lymph may result in dehydra-and the descending branch of the omocervical artery. tion, electrolyte imbalances and hypoproteinemiaAt the junction of the internal jugular and left [49]. Interestingly, previous experiments have shownexternal jugular veins, the thoracic duct ampulla, that the loss of protein via the thoracic lymph is notwhich has a whitish appearance can be identified by directly reflected in a reduction in plasma protein,careful dissection (Fig. 3). This is then ligated at the suggesting that appreciable amounts of newly formedpoint of its entrance into the external jugular vein, protein are added to the circulation during lymphand all tributaries converging to the thoracic duct are fistulation [50,51].identified and ligated to ensure the return of lymph The optimised surgical protocol described abovethrough the main lymphatic canal. The thoracic duct afforded a robust model with a success rate ofis cannulated directly with PVC tubing (1.4 mm I.D., greater than 80%. Failure has predominantly been1.9 mm O.D.) which is brought through the skin via due to the lymph cannulas being pulled out by thea separate stab incision and stabilised in place with dogs during the recovery period. In comparison to3-O silk ligatures and cyanoacrylate adhesive. The the published methods, direct cannulation of the
thoracic duct in the neck reduced the operating timeto less than an hour, and the dogs were oftenstanding upright within an hour after surgery. Theincidence of clot formation and cannula blockagewas also reduced with this method. Whilst theanatomy of the lymphatic system of dogs has beenreported to be highly variable [52,53], our methodallowed ready accommodation of the inevitableanatomical variations, which was often not possiblewith the previously published method. The adminis-tration of a small lipid meal (corn oil) prior tosurgery was helpful in the identification and visuali-sation of the thoracic duct.
3.2.3.2. Assessment of the efficiency of lipid absorp-Fig. 3. Schematic diagram to show the left lateral area of the neck
tion in the conscious dog modelof the dog during surgery to insert a thoracic lymph duct cannula.The total mass of triglyceride transported inThe thoracic duct is identified as it enters the left external jugular
vein adjacent to its junction with the internal jugular vein. thoracic duct lymph, and systemic plasma concen-

G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60 55
trations of triglyceride are routinely determined to of lymph collected from fasted dogs was much lowerover the same period (2796230 g). The appearanceconfirm the integrity of the lymph duct cannulationof lymph collected from fasted and fed dogs was alsoand to ensure the collection of all thoracic lymph.vastly different. Lymph from fasted dogs appearedAcceptance criteria for the post-prandial modelclear and straw-coloured whereas lymph collectedincluded the recovery of at least 85% (by mass) offrom fed dogs was milky white, indicating thethe triglyceride lipid administered (present in food)presence of chylomicrons. Lymph TG output rates inin thoracic duct lymph and correspondingly lowfed and fasted greyhounds are shown in Fig. 5. Insystemic plasma triglyceride concentrations. Plasmathese studies, dogs were fed a meal containingtriglyceride levels are typically similar in either fedapproximately 34 g of lipid. Typically 90–105% ofor fasted lymph cannulated animals and range be-the ingested TG is recovered in the lymph over thetween 0.3 and 0.6 mg/ml. This compares with levelspost dose period.in control (non-cannulated) animals of approximately
In summary, a novel and robust triple-cannulated0.5–1.0 mg/ml under fasted conditions and 1–5conscious dog model has been developed for themg/ml post prandially. High plasma triglycerideassessment of absorption, enterocyte-based metabo-concentrations in lymph-cannulated animals ( . 0.7–lism and lymphatic transport of candidate lipophilic0.8 mg/ml) are usually indicative of a colateraldrugs under realistic pre- and post-prandial con-lymph duct which was not isolated and ligated,ditions. The model enables the rapid identification ofallowing passage of lymph into the systemic blood.lipophilic drug candidates, which may be substratesUnder these circumstances data were discarded. Asfor intestinal lymphatic transport and can assist in theexpected, lymph flow rates for the post-prandial dogdevelopment of lipid formulation to maximise oralare considerably higher than that in the fasted dogdrug bioavailability. This model also allowed the(Fig. 4). In the initial period following feeding,oral administration of clinically relevant full sizegreater than 100 g of lymph can be collected eachhuman dose forms in representative fed and fastedhour and the total mass of lymph collected over astates, and has been used to establish the relative10-h period in post-prandial dogs was 9466108 groles of lymphatic transport and enterocyte-based(mean6S.D.). In contrast, the mean6S.D. total mass
Fig. 4. Thoracic lymph flow rate (mean (g /h)6S.E., n 5 4) in Fig. 5. Triglyceride output (mean (mg/h)6S.E., n 5 4) in thefasted (s) greyhound dogs and dogs fed a standard meal thoracic duct lymph in fasted (s) greyhound dogs and dogs fed acontaining approximately 34 g lipid (d). standard meal containing approximately 34 g lipid (d).

56 G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60
metabolism in the oral bioavailability of the antima- lymph chylomicron appearance time using hydratedlarial drug halofantrine following fed and fasted (normal saline infusion via jugular vein) and non-administration [36]. hydrated rats. Animals were intraduodenally infused
with a lipid emulsion containing radio-labelled oleicacid, monoolein and sodium taurocholate in phos-
4. Model related factors influencing the outcome phate buffer for a period of 3 h. Steady state lymphof intestinal drug transport studies lipoprotein output was reached 2 h after lipid ad-
ministration in the hydrated animals, however, non-The rate and extent of intestinal lymphatic drug hydrated rats failed to reach steady state lymph
transport may be affected by fasting before and after output during the 3 h of lipid infusion. Although thesurgery, the rate and extent of rehydration and the eventual extent of lymph lipid transport was notpresence or absence of lipid feeding prior to surgery altered, the rate of formation and transport of lymph(to improve visualisation of the lymph duct). For lipoproteins into the intestinal lymph after lipidexample, Charman et al. [54] demonstrated that the administration was affected by both rehydration andextent of intestinal lymphatic transport of DDT lipid administration.increased by two-fold, when the period of fasting The influence of anaesthesia on lymphatic trans-after cannulation, and prior to drug administration port is more difficult to assess. In the rat, dosing ofwas altered from 2 to 48 h in mesenteric lymph duct anaesthetised animals is achieved via a duodenalcannulated anaesthetised rats. The authors suggested cannula, whilst oral dosing is generally employed inthat mobilisation of endogenous lipids during fasting conscious animals. Therefore it is difficult to assessand increased lipoprotein synthesis on subsequent the influence of the anaesthetic alone, when gastricadministration of a lipid vehicle, were responsible processing is only active in the orally dosed animals.for the increased rate and extent of lymph formation For example, the intestinal lymphatic transport ofand intestinal lymphatic drug transport [54]. halofantrine was found to be lower after intraduoden-
Infusion of rehydration solutions in lymph-cannu- al administration of a lipid solution formulation tolated rats may also affect the rate of appearance of anaesthetised rats when compared with oral adminis-intestinal lymph lipoproteins and the lymph flow. tration to conscious rats. However, when the formu-Tso [29] demonstrated significant increases in lymph lation was dispersed to form a micellar solution priorflow and chylomicron transport after enteral rehydra- to dosing, the extent of lymphatic transport wastion in rats, due to expansion of the interstitial matrix similar (and maximal) in both anaesthetised andand enhanced interstitial fluid formation. These conscious animals [20]. This data suggests that thefindings were consistent with the positive relation- primary disadvantage of anaesthetised animals, is notship previously observed between the rate of intra- the anaesthetic per se, but the inability of anaesthet-duodenal saline infusion (0.9% NaCl containing ised animals to effectively disperse and process lipid0.09% KCl) and the lymph flow in conscious based delivery systems prior to absorption.restrained rats [1]. Rats may tolerate infusion rates The site of lymphatic cannulation is also importantup to 7.3 ml /h intra-duodenally and 2.2 ml /h via the and one disadvantage of the dog model describedjugular vein [1], and these rehydration strategies are here is that lymph is collected from the thoracic ductuseful tools for the enhancement of lymph flow and rather than the mesenteric duct. Although an orallyas an aide to maintenance of lymphatic patency. administered drug directly gains access to mesenteric
Not surprisingly, lipid infusion also alters the rate lymph after absorption through the enterocyte, it canand extent of lymph lipoprotein transport and the also indirectly gain access to peripheral lymph bylymph flow in rats and dogs. An approximately 75% equilibration from systemic blood across peripheralincrease in lymph flow was reported after co-infusion capillary beds [55]. Collection of thoracic lymphof a combination of Ringer’s solution with a tri- may therefore overestimate the actual intestinalglyceride lipid solution compared with the infusion lymphatic transport because the thoracic duct collectsof Ringer’s solution alone in rats [28]. Tso [29] also lymph from hepatic and peripheral sources in addi-demonstrated the importance of rehydration on the tion to the small intestine [56,57]. For example,

G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60 57
Noguchi et al. [24] demonstrated a significant in- animals remain mobile, and quickly resume normalcrease in lymphatic recovery of orally administered activities whilst allowing for the continuous collec-DDT when assessed in thoracic lymph when com- tion of lymph.pared with mesenteric lymph cannulated animals. In Recent appreciation of the role of membranecontrast, however, we have assessed the extent of transporter systems and intracellular carriers in lipidtransfer of the lipophilic antimalarial halofantrine digestion and absorption has led to the utilisation ofinto the thoracic lymph of greyhound dogs after i.v. genetically modified animals to examine specificadministration, and shown that a low 1.560.2% parts of this pathway. These include animals de-(mean6S.D., n 5 3) of the dose is recovered in ficient in: fatty acid binding proteins such as I-FABPthoracic lymph over a 12-h post dose period [58]. [59], synthetic enzymes such as acyl CoA:cholesterolThese more recent data suggest that in the dog acyltransferase (ACAT) [60] and acylmodel, where the extent of lymphatic transport might CoA:diacylglycerol acyltransferase (DGAT) [61],be expected to be more accurately reflect the human apolipoproteins such as apo-B [62,63] and ABCsituation, the contribution of equilibration across anti-transporters such as MDR1 and MDR3 P-gpscapillary beds to overall drug transport into the [64]. These models will provide extremely usefulthoracic lymph is minimal. information in terms of the mechanistic aspects of
In summary, a large number of factors impact on lymphatic transport. The cost associated with thethe accurate estimation of intestinal lymphatic trans- development of genetically modified animals, how-port of lipophilic drugs including variations in the ever, has almost exclusively restricted these studiesperiod of animal fasting, the rate and extent of to mice and whilst improved thoracic lymph ductrehydration, the degree of lipid feeding and anaes- cannulation methods have been described in thethesia, and the site of lymphatic cannulation. These mouse [65], these very small animal models areexperimental variables need to be carefully con- difficult to dose with realistic drug formulations.trolled during the development of experimental Their small size also precludes the sampling of largemodels and protocols in order to facilitate effective enough volumes of lymph or blood to facilitate drugcomparison of data. assay by anything other than the most sensitive
techniques (such as the use of radiolabelled tracers).Conduct of lymphatic drug transport studies in
5. Conclusions larger omnivorous species such as the dog hassignificant advantages over studies in smaller (often
It is now well recognised that intestinal lymphatic herbivorous) animals such as the rat or mouse, as thetransport may contribute significantly to the oral gastrointestinal tract and gastric transit profile of thebioavailability of selected highly lipophilic drugs. A dog more accurately reflect the human situation.number of animal models are available to study these Furthermore, the physical size of the dog can facili-compounds and to establish the contribution of tate the dosing of full size human dose forms and thelymphatic transport to oral bioavailability. The re- administration of more realistic volume of lipid on asults of such studies and the use of these models may mass per kilogram basis [1,6,34]. Larger animalalso subsequently guide the rational development of models (especially the dog and the pig) also have thecandidate formulations for lipophilic drugs. Many of advantage of gastric transit and biliary secretionthe studies to date have utilised unconscious rat profiles that more clearly resemble the human situa-models. Whilst these models are simple, robust and tion and are more useful in the assessment of, fordo not have the problems associated with animal example, post prandial lymphatic transport profiles.movement during lymph collection, they have the However, these higher species models are expensiveattendant disadvantage of requiring long periods of to set up and monitor, and are therefore impracticalanaesthesia to obtain a complete pharmacokinetic for the initial screening or evaluation of intestinalprofile. We have described the use of a conscious rat lymphatic transport. These studies will usefullymodel that has the advantages of relative simplicity, continue to utilise smaller animal models such as thelow expense and success rates of around 70%. The rat.

58 G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60
response, in: R. Rhoades, R. Pflanzer (Eds.), Human Physi-Referencesology, Saunders College Press, Orlando, FL, 1996, pp. 824–852.
[1] T.J. Raub, S.L. Douglas, G.W. Melchior, W.N. Charman,[17] W.N. Charman, V.J. Stella, Estimating the maximal potential
Methodology for assessing intestinal lymphatic transport, in:for intestinal lymphatic transport of lipophilic drug mole-
W.N. Charman, J. Stella (Eds.), Lymphatic Transport ofcules, Int. J. Pharm. 33 (1986) 175–178.
Drugs, CRC Press, Boca Raton, FL, 1992, pp. 63–111.[18] J.J. van Dongen, R. Remie, J.W. Rensema, G.H.J. van
[2] C.J.H. Porter, Drug delivery to the lymphatic system, Crit.Wunnik, Techniques in the behavioural and neural sciences,
Rev. Ther. Drug Carrier Syst. 14 (1997) 333–393.in: J.P. Huston (Ed.), Manual of Microsurgery On the
[3] D.J. Hauss, S.E. Fogal, J.V. Ficorilli, C.A. Price, T. Roy,Laboratory Rat, Vol. 4, Elsevier, Amsterdam, 1990, pp.
A.A. Jayaraj, J.J. Keirns, Lipid-based delivery systems for11–15.
improving the bioavailability and lymphatic transport of a[19] W.N. Charman, Lipid vehicle and formulation effects on
poorly water-soluble LTB inhibitor, J. Pharm. Sci. 874 intestinal lymphatic transport, in: W.N. Charman, J. Stella(1998) 164–169.
(Eds.), Lymphatic Transport of Drugs, CRC Press, Boca[4] C.J.H. Porter, W.N. Charman, Uptake of drugs into the
Raton, Fl, 1992, pp. 113–179.intestinal lymphatics after oral administration, Adv. Drug.
[20] C.J.H. Porter, S.A. Charman, W.N. Charman, LymphaticDeliv. Rev. 25 (1997) 71–89.
transport of halofantrine in the triple-cannulated anesthetized[5] G.Y. Kwei, L.B. Novak, L.H. Hettrick, E.R. Reiss, E.K.
rat model: effect of lipid vehicle dispersion, J. Pharm. Sci. 85Fong, T.V. Olah, A.E. Loper, Lymphatic uptake of MK-386,
(1996) 351–356.a sterol 5-alpha reductase inhibitor, from aqueous and lipid
[21] C.J.H. Porter, S.A. Charman, A.J. Humberstone, W.N. Char-formulations, Int. J. Pharm. 164 (1998) 37–44.
man, Lymphatic transport of halofantrine in the conscious rat[6] S.-M. Khoo, C.J.H. Porter, G.A. Edwards, W.N. Charman,
when administered as either the free base or the hydrochlo-Intestinal lymphatic transport is the primary absorption route
ride salt: effect of lipid class and lipid vehicle dispersion, J.for halofantrine after oral post-prandial administration,
Pharm. Sci. 85 (1996) 357–361.Pharm. Sci. 1 (1999) S642.
[22] C.J.H. Porter, W.N. Charman, Model systems for intestinal[7] D.L. Yeung, M.J. von Saigent, Absorption of retinol andlymphatic transport studies, in: R.T. Borchardt et al. (Ed.),retinyl esters via the lymph and the portal vein in the rat,Models for Assessing Drug Absorption and Metabolism,Can. J. Physiol. Pharmacol. 50 (1972) 753–760.Plenum Press, New York, 1996, pp. 85–102.[8] T. Noguchi, W.N. Charman, V.J. Stella, Lymphatic appear-
[23] S.G. Turner, J.A. Barrowman, Intestinal lymph flow andance of DDT in thoracic mesenteric lymph duct cannulatedlymphatic transport of protein during fat absorption, Q. J.rats, Int. J. Pharm. 24 (1985) 185–192.Exp. Physiol. Cogn. Med. Sci. 62 (1977) 175–180.[9] E. Fukui, H. Kurohara, A. Kageyu, Y. Kurosaki, T.
[24] T. Noguchi, W.N. Charman, V.J. Stella, Lymphatic appear-Nakayama, T. Mimura, Enhancing effect of medium chainance of DDT in thoracic or mesenteric lymph duct cannu-triglyceride on intestinal absorption of d-a-tocopherol ace-lated rats, Int. J. Pharm. 24 (1985) 185–192.tate from lecithin-dispersed preparations in the rat, J. Phar-
[25] D.J. Hauss, S.E. Fogal, J.V. Ficorilli, Chronic collection ofmacobio-Dyn. 12 (1989) 80–86.mesenteric lymph from conscious, tethered rats, Contemp.[10] T. Ichihashi, H. Kinoshita, H. Yamada, Absorption andTopics Lab. Anim. Sci. 37 (1998) 56–58.disposition of epithiosteroids in rats (2): Avoidance of first
[26] P.A. Flecknell (Ed.), Laboratory Animal Anaesthesia, Aca-pass metabolism of mepitiostane by lymphatic absorption,demic Press, London, 1987.Xenobiotica 1 (1991) 873–880.
[27] J.S. Lee, Lymph flow, lymph protein concentration, and[11] M.K. Bijsterbosch, T.J.C. van Berkel, Native and modifiedprotein output from rat small intestine, Am. J. Physiol. 248lipoproteins as drug delivery systems, Adv. Drug Deliv. Rev.(1985) G670–G675.5 (1990) 231–251.
[28] P. Tso, V. Pitts, D.N. Granger, Role of lymph flow in[12] W.N. Charman, V.J. Stella, Transport of lipophilic moleculeschylomicron transport, Am. J. Physiol. 249 (1985) G21–28.by the intestinal lymphatic system, Adv. Drug Deliv. Rev. 7
[29] P. Tso, J.A. Balint, Formation and transport of chylomicrons(1991) 1–14.by enterocytes to the lymphatics, Am. J. Physiol. 250 (1986)[13] W.N. Charman, M.C. Rogge, A.W. Boddy, W.H. Barr, B.M.G715–G726.Berger, Absorption of danazol after administration to differ-
[30] W.J. Simmonds, The role of micellar solubilization in lipident sites of the gastrointestinal tract and the relationship toabsorption, Aust. J. Exp. Biol. Med. Sci. 33 (1955) 305–313.single- and double-peak phenomena in the plasma profiles, J.
[31] P. Shepherd, W.J. Simmonds, Some conditions affecting theClin. Pharmacol. 33 (1993) 1207–1213.maintenance of a steady lymphatic absorption of fat Aust, J.[14] J.M. Yoffey, F.C. Courtice, Lymphatics, Lymph and theExp. Biol. Med. Sci. 37 (1959) 1–10.Lymphomyeloid Complex, Academic Press, London, 1970.
[32] Y.F. Shiau, D.A. Popper, M. Reed, Intestinal triglycerides are[15] C.M. O’Driscoll, Anatomy and physiology of the lymphatics,derived from both endogenous and exogenous sources, Am.in: W.N. Charman, V.J. Stella (Eds.), Lymphatic Transport ofJ. Physiol. 248 (1985) G164–G169.Drugs, CRC Press, London, 1992, pp. 1–35.
[33] S.M. Caliph, W.N. Charman, C.J.H. Porter, Effect of short-,[16] R. Rhoades, R. Pflanzer, Body defense and the immune

G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60 59
medium-, and long-chain fatty acid-based vehicles on the [48] D.E. Brisco, Canine thoracic duct cannulation revisited,absolute oral bioavailability and intestinal lymphatic trans- Lymphology 14 (1981) 32–34.port of halofantrine and assessment of mass balance in [49] N. Tilney, J. Murray, Chronic thoracic duct fistula: operativelymph-cannulated and non-cannulated rats, J. Pharm. Sci. 89 technique and physiologic effects in man, Ann. Surg. 167(2000) 1073–1084. (1968) 1–8.
[34] M.D. Rajpal, R. Kirkpatrick, Creation of a thoracic duct [50] W.W.L. Glenn, S.L. Cresson, F.X. Bauer, F. Glodstein, O.fistula: an improved technique, J. Surg. Res. 13 (1972) Hoffman nan, J.E. Healey, Experimental thoracic duct260–261. fistula: observations on the technique, the absorption of fat
[35] S.-M. Khoo, C.J.H. Porter, G.A. Edwards, W.N. Charman, A and fluid from the intestine, and protein depletion, Surg.novel triple-cannulated conscious dog model for assessment Gynecol. Obstet. 89 (1949) 200–208.of the absorption, enterocyte-based metabolism and lympho- [51] P.I. Korner, B. Morris, F.C. Courtice, An analysis of thecyte transport of candidate lipophilic drugs, Pharm. Sci. 1 factors affecting lymph flow and protein composition during(1999) S647. gastric absorption of food and fluids and during intravenous
[36] S.-M. Khoo, G.A. Edwards, C.J.H. Porter, W.N. Charman, A infusion, Aust. J. Exp. Biol. Med. Sci. 32 (1954) 301–320.conscious dog model for assessing the absorption, en-
[52] J. Markowitz, J. Archibald, H.G. Downie, in: Experimentalterocyte-based metabolism and intestinal lymphatic transport
Surgery, 5th Ed, Williams and Wilkins, Baltimore, MD,of halofantrine. J. Pharm. Sci. (2001) in press.
1964.[37] D.G. White, M.J. Story, S.G. Barnwell, An experimental[53] K.G. Kagan, E.M. Breznock,Variations in the canine thoracicmodel for studying the effects of a novel lymphatic drug
duct system and the effects of surgical occlusion demon-delivery system for propranolol, Int. J. Pharm. 69 (1991)strated by rapid aqueous lymphography, using an intestinal169.lymphatic trunk, Am. J. Vet. Res. 40 (1979) 948–958.[38] T.T. Kararli, Comparison of the gastrointestinal anatomy,
[54] W.N. Charman, T. Noguchi, V.J. Stella, An experimentalphysiology and biochemistry of humans and commonly usedsystem designed to study the in situ intestinal lymphaticlaboratory animals, Biopharm. Drug Dispos. 16 (1995) 351–transport of lipophilic drugs in anaesthetised rats, Int. J.380.Pharm. 33 (1986) 155–164.[39] L.T. Jensen, H.P. Oleson, J. Risteli, I. Lorenzen, External
[55] H.E. Gallo-Torres, O.N. Miller, A modified Bollman’sthoracic duct-venous shunt in conscious pigs for long termtechnique for cannulation of the rats thoracic duct: lymphstudies of connective tissue metabolites in lymph, Lab.flow standardization, Proc. Soc. Exp. Biol. Med. 130 (1972)Anim. Sci. 40 (1990) 620–624.552–555.[40] S.A. Chen, R.J. Sawchuk, R.C. Brundage, C. Horvath, H.V.
[56] T. DeMarco, R. Levin, Role of the lymphatics in theMendenhall, R.A. Gunther, R.A. Braeckman, Plasma andintestinal absorption and distribution of drugs, J. Pharmacol.lymph pharmacokinetics of recombinent human interleukin-2Exp. Ther. 169 (1969) 142–151.and polyethylene glycol-modified interleukin-2 in pigs, J.
[57] C.T. Ueda, M. Lemaire, G. Gsell, K. Nussbaumer, IntestinalPharmacol. Exp. Ther. 293 (2000) 248–259.absorption of cyclosporin A following oral administration in[41] S.A. Charman, A.M. Segrave, G.A. Edwards, C.J.H. Porter,an olive oil solution in rats, Biopharm. Drug Dispos 4 (1983)Systemic availability and lymphatic transport of human113–124.growth hormone administered by subcutaneous injection, J.
[58] S.-M. Khoo, R.J. Prankerd, G.A. Edwards C.J.H. Porter,Pharm. Sci. 89 (2000) 168–177.W.N. Charman, A physicochemical basis for the extensive[42] C.J.H. Porter, G.A. Edwards, A.S. Segrave, S.A. Charman,intestinal lymphatic transport of a poorly lipid solubleLymphatic transport of proteins after s.c. injection: implica-antimalarial, halofantrine hydrochloride, after post-prandialtion of animal model selection. Adv. Drug Deliv. Rev.administration to dogs, Submitted for publication.(2001) in press.
[59] G. Vassileva, L. Huwyler, K. Poirier, L.B. Agellon, M.J.[43] J.C. Fish, H.E. Sarles, A.T. Mattingly, M.U. Ross, A.R.Toth, The intestinal fatty acid binding protein is not essentialRemmers Jr., Preparation of chronic thoracic duct lymphfor dietary fat absorption in mice, FASEB J. 14 (2000)fistulas in man and animals, J. Surg. Res. 9 (1969) 101–106.2040–2046.[44] E.J. Gralla, F.M. Capprello, A.M. Jones, Technique for
[60] K.K. Buhman, M. Accad, S. Novak, R.S. Choi, J.S. Wong,chronic cannulation of the canine thoracic duct, Am. J. Vet.R.L. Hamilton, S. Turley, R.L. Farese, Resistance to diet-Res. 34 (1973) 285–287.induced hypercholesterolemia and gallstone formation in[45] D.D. Dedo, J.H. Ogura, Exteriorization of thoracic ductACAT2-deficient mice, Nature Med. 6 (2000) 1341–1347.lymph: Theoretical considerations and an experimental
[61] S.J. Smith, S. Cases, D.R. Jensen, H.C. Chen, E. Sande, B.model, Arch. Otolaryngol. 101 (1975) 671–674.Tow, D.A. Sanan, J. Raber, R.H. Eckel, R.V. Farese, Obesity[46] S.G. Rajpal, J.R. Kirkpatrick, Creation of a thoracic ductresistance and multiple mechanisms of triglyceride synthesisfistula: An improved technique, Surg. Res. 13 (1972) 260–in mice lacking Dgat, Nat. Genet. 25 (2000) 87–90.264.
[47] C.L. Witte, M.H. Witte, W.R. Cole, A simplified method for [62] S.G. Young, C.M. Cham, R.E. Pitas, B.J. Burri, A. Connolly,cannulation of the normal canine cervical thoracic duct, L. Flynn, A.S. Pappu, J.S. Wong, R.L. Hamilton, R.V. Farese,Lymphology 4 (1970) 159–161. A genetic model for absent chylomicron formation: mice

60 G.A. Edwards et al. / Advanced Drug Delivery Reviews 50 (2001) 45 –60
producing apolipoprotein B in the liver but not in the [65] P. Ionac, T. Laskay, D. Labahn, G. Geisslinger, W. Solbach,intestine, J. Clin. Invest. 96 (1995) 2932–2946. Improved technique for cannulation of the murine thoracic
[63] E. Kim, S.G. Young, Genetically modified mice for the study duct: a valuable tool for the dissection of immune responses,of apolipoprotein B, J. Lipid Res. 39 (1998) 703–723. J. Immunol. Methods 202 (1997) 35–40.
[64] P. Borst, N. Zelcer, A. van Helvoort, ABC transporters inlipid transport, Biochim. Biophys. Acta 1486 (2000) 128–144.














![Primary Mucinous Adenocarcinoma of the Ovary with ... · PDF fileseeding and lymphatic spread [14]. Most stage I invasive mucinous carcinomas of the intestinal type with expansile](https://img.dokumen.tips/doc/110x75/5ab668757f8b9a86428d9b6b/primary-mucinous-adenocarcinoma-of-the-ovary-with-and-lymphatic-spread-14.jpg)