Embed Size (px)
Citation preview
C H A P T E R
26
Neurotoxin 1-Methyl-4-phenyl-1,2,3,6-tetrahydropyridine-Induced
Animal Models for Parkinson’s DiseaseJiro Kasahara*, Mohammed Emamussalehin Choudhuryy, z,Hironori Yokoyama*, Naoto Kadoguchi*, Masahiro Nomotoy*Department of Neurobiology and Therapeutics, Graduate School of Pharmaceutical Sciences,
The University of Tokushima, Tokushima, JapanyDepartment of Therapeutic Medicine, Ehime University Graduate School of Medicine, Toon-shi, Ehime, Japan
zDepartment of Neurosciences, Centre de Recherche du CHUL (CHUQ), Ste-Foy, Quebec, Canada
A
h
O U T L I N E
Abbreviations
634Introduction
634Clinical Characteristics of PD and Their RelevantSymptoms in Animal Models
636nima
ttp://
Epidemiological Background 6
36 Clinical Stages of PD 6 36 Clinical Symptoms in PD Patients 6 37 Symptoms in Nonhuman Primates 6 37 Symptoms in Rodents 6 37Molecular Pathophysiology of PD
637Neurotoxins for Making PD Models
638 6-Hydroxydopamine 6 38 1-Methyl-4-phenyl-1,2,3,6-tetrahydropyridine 6 39 Pesticides 6 40 Others 6 40MPTP-Induced Mouse Model for PD
641 Animal Selection 6 41 Drug Administration 6 41 Behavioral Analysis 6 41 Catalepsy Test 6 42633l Models for the Study of Human Disease
dx.doi.org/10.1016/B978-0-12-415894-8.00026-9
Pole Test 6
42 Rota-Rod Test 6 43 Open-Field Test 6 43 Elevated Plus Maze 6 43 Beam-walking Test 6 43 Footprint and Stepping Test 6 43 Immunohistochemical and Biochemical Evaluations withRelevancy to PD 6
44 Functional Imaging in Mice 6 45MPTP-Induced Common Marmoset Model for PD
645 General Information for the Use of Common Marmosets 6 45 Housing and MPTP Administration 6 46 Progression of Abnormal Symptoms 6 46 Locomotor Activity 6 47 Scoring of Severity 6 47 Immunohistochemical, Biochemical Analyses 6 47 Functional Imaging in Common Marmosets 6 47Concluding Remarks
647Acknowledgment
647References
647Copyright � 2013 Elsevier Inc. All rights reserved.
26. MPTP MODELS FOR PARKINSON’S DISEASE634
ABBREVIATIONS
PD, Parkinson’s disease; SNpc, substantia nigra parscompacta; DA, dopamine; MSN, medial spiny neurons;GPe, external segment of globus pallidus; STN, subthala-mic nuclei; GPi, internal segment of globus pallidus; SNr,substantia nigra pars reticulate; L-dopa, L-3,4-dihydroxy-phenylalanine; AADC, L-amino acid decarboxylase;MAO-B, monoamine oxidase B; COMT, catechol-O-methyl transferase; MPTP, 1-methyl-4-phenyl-1,2,3,6-tet-rahydropyridine; UPDRS, Unified Parkinson’s DiseaseRating Scale; ADL, activities of daily life; TH, tyrosinehydroxylase; ROS, reactive oxygen species; RNS, reactivenitrogen species; TNF-a, tumor necrosis factor-a; iNOS,inducible nitric oxide synthase; COX-2, cyclooxygenase 2;6-OHDA, 6-hydroxydopamine; BBB, blood brain barrier;NAT, noradrenaline transporter; DAT, dopamine trans-porter; MPPþ, 1-methyl-4-phenyl-pyridinium; IL-1b,interleukin 1b;, IL-6, interleukin 6; NO, nitric oxide;PQ, 1,1’-dimethyl-4-4’-bipyridinium (paraquat); VMAT,vesicle monoamine transporter; AMPT, a-methyl p-tyro-sine; JNK, c-Jun N-terminus kinase; DMSO, dimethylsuf-oxide; DOPAC, 3,4-dihydroxy-phenylacetic acid; HVA,homovanillic acid; LTF, latency to fall; NeuN, neuralnuclei; GFAP, glial fibrillary acidic protein; NF-kB,nuclear factor-kB; SOD, superoxide dismutase; GSH-PX, glutathione peroxidase; MDA, malondialdehyde;BDNF, brain derived neurotrophic factor; GDNF,glial cell line-derived neurotrophic factor; FGF-2, basicfibroblast growth factor 2; HPLC, high performanceliquid chromatography; Cdk-5, cyclin-dependent proteinkinase 5; [11C]CIT-FP, N-3-fluoropropyl-2-b-[O-meth-yl-11C]carbomethoxy-3-b-(4-iodophenyl)-tropane; [18F]FECNT, 2b-carbomethoxy-3b-(4-chlorophenyl)-8-(2-[18F]-fluoroethyl)-nortropane; [18F]-DTBZ (AV-133), 9-fluoro-propyl-(+)-dihydrotetrabenazine.
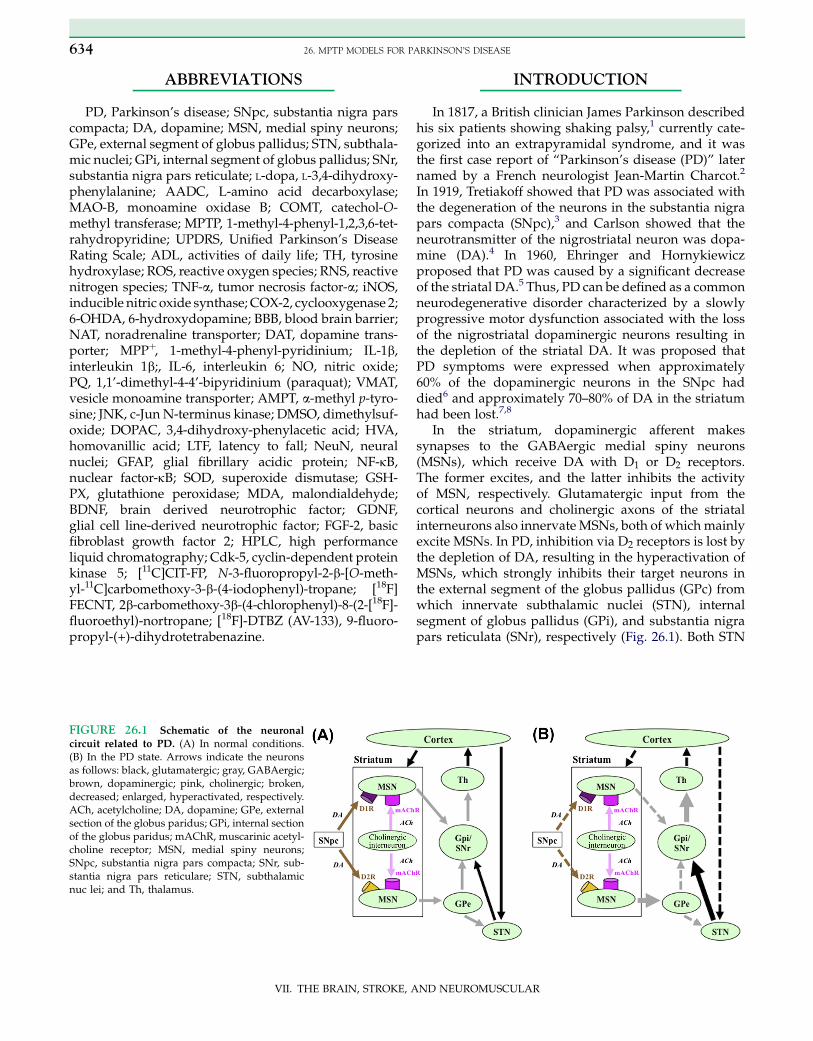
FIGURE 26.1 Schematic of the neuronal
circuit related to PD. (A) In normal conditions.(B) In the PD state. Arrows indicate the neuronsas follows: black, glutamatergic; gray, GABAergic;brown, dopaminergic; pink, cholinergic; broken,decreased; enlarged, hyperactivated, respectively.ACh, acetylcholine; DA, dopamine; GPe, externalsection of the globus paridus; GPi, internal sectionof the globus paridus; mAChR, muscarinic acetyl-choline receptor; MSN, medial spiny neurons;SNpc, substantia nigra pars compacta; SNr, sub-stantia nigra pars reticulare; STN, subthalamicnuc lei; and Th, thalamus.
VII. THE BRAIN, STROKE, A
INTRODUCTION
In 1817, a British clinician James Parkinson describedhis six patients showing shaking palsy,1 currently cate-gorized into an extrapyramidal syndrome, and it wasthe first case report of “Parkinson’s disease (PD)” laternamed by a French neurologist Jean-Martin Charcot.2
In 1919, Tretiakoff showed that PD was associated withthe degeneration of the neurons in the substantia nigrapars compacta (SNpc),3 and Carlson showed that theneurotransmitter of the nigrostriatal neuron was dopa-mine (DA).4 In 1960, Ehringer and Hornykiewiczproposed that PD was caused by a significant decreaseof the striatal DA.5 Thus, PD can be defined as a commonneurodegenerative disorder characterized by a slowlyprogressive motor dysfunction associated with the lossof the nigrostriatal dopaminergic neurons resulting inthe depletion of the striatal DA. It was proposed thatPD symptoms were expressed when approximately60% of the dopaminergic neurons in the SNpc haddied6 and approximately 70–80% of DA in the striatumhad been lost.7,8
In the striatum, dopaminergic afferent makessynapses to the GABAergic medial spiny neurons(MSNs), which receive DA with D1 or D2 receptors.The former excites, and the latter inhibits the activityof MSN, respectively. Glutamatergic input from thecortical neurons and cholinergic axons of the striatalinterneurons also innervateMSNs, both of which mainlyexcite MSNs. In PD, inhibition via D2 receptors is lost bythe depletion of DA, resulting in the hyperactivation ofMSNs, which strongly inhibits their target neurons inthe external segment of the globus pallidus (GPc) fromwhich innervate subthalamic nuclei (STN), internalsegment of globus pallidus (GPi), and substantia nigrapars reticulata (SNr), respectively (Fig. 26.1). Both STN
ND NEUROMUSCULAR
INTRODUCTION 635
and GPi are known as targets for the electrodes of deep-brain stimuli therapy in PD.9
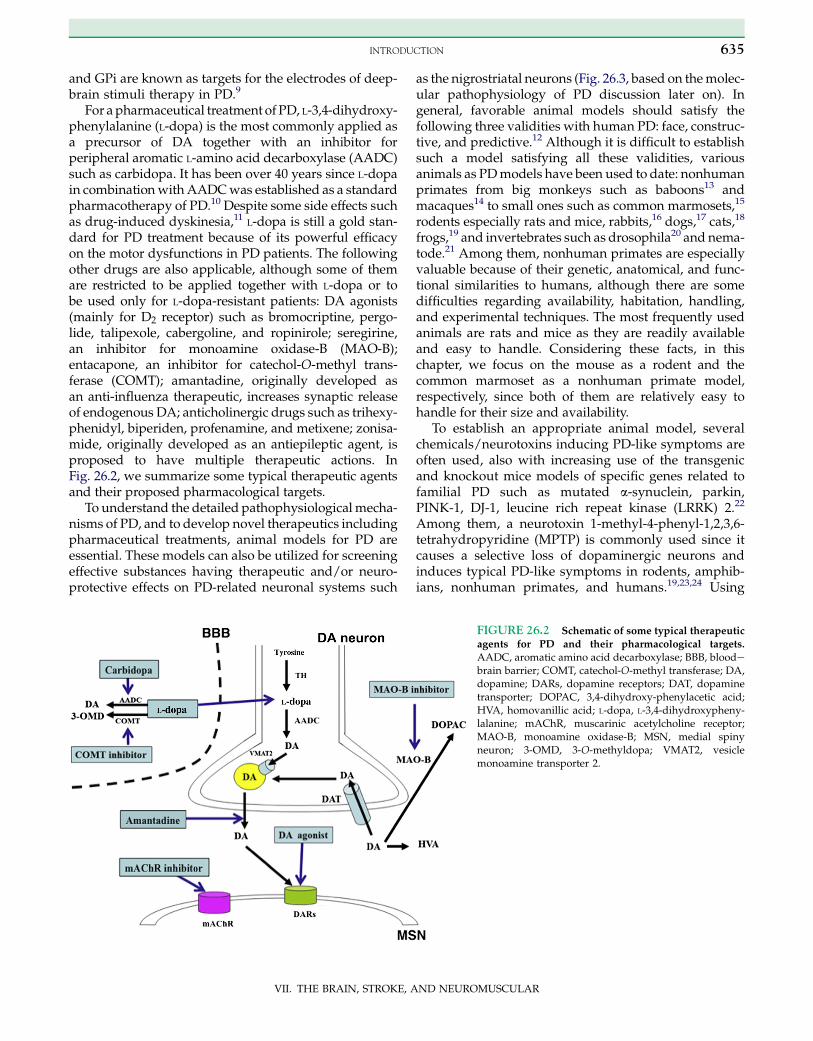
For apharmaceutical treatment of PD, L-3,4-dihydroxy-phenylalanine (L-dopa) is the most commonly applied asa precursor of DA together with an inhibitor forperipheral aromatic L-amino acid decarboxylase (AADC)such as carbidopa. It has been over 40 years since L-dopain combinationwithAADCwas established as a standardpharmacotherapy of PD.10 Despite some side effects suchas drug-induced dyskinesia,11 L-dopa is still a gold stan-dard for PD treatment because of its powerful efficacyon the motor dysfunctions in PD patients. The followingother drugs are also applicable, although some of themare restricted to be applied together with L-dopa or tobe used only for L-dopa-resistant patients: DA agonists(mainly for D2 receptor) such as bromocriptine, pergo-lide, talipexole, cabergoline, and ropinirole; seregirine,an inhibitor for monoamine oxidase-B (MAO-B);entacapone, an inhibitor for catechol-O-methyl trans-ferase (COMT); amantadine, originally developed asan anti-influenza therapeutic, increases synaptic releaseof endogenous DA; anticholinergic drugs such as trihexy-phenidyl, biperiden, profenamine, and metixene; zonisa-mide, originally developed as an antiepileptic agent, isproposed to have multiple therapeutic actions. InFig. 26.2, we summarize some typical therapeutic agentsand their proposed pharmacological targets.
To understand the detailed pathophysiologicalmecha-nisms of PD, and to develop novel therapeutics includingpharmaceutical treatments, animal models for PD areessential. These models can also be utilized for screeningeffective substances having therapeutic and/or neuro-protective effects on PD-related neuronal systems such
VII. THE BRAIN, STROKE, A
as the nigrostriatal neurons (Fig. 26.3, based on themolec-ular pathophysiology of PD discussion later on). Ingeneral, favorable animal models should satisfy thefollowing three validities with human PD: face, construc-tive, and predictive.12 Although it is difficult to establishsuch a model satisfying all these validities, variousanimals as PDmodels have been used to date: nonhumanprimates from big monkeys such as baboons13 andmacaques14 to small ones such as common marmosets,15
rodents especially rats and mice, rabbits,16 dogs,17 cats,18
frogs,19 and invertebrates such as drosophila20 and nema-tode.21 Among them, nonhuman primates are especiallyvaluable because of their genetic, anatomical, and func-tional similarities to humans, although there are somedifficulties regarding availability, habitation, handling,and experimental techniques. The most frequently usedanimals are rats and mice as they are readily availableand easy to handle. Considering these facts, in thischapter, we focus on the mouse as a rodent and thecommon marmoset as a nonhuman primate model,respectively, since both of them are relatively easy tohandle for their size and availability.
To establish an appropriate animal model, severalchemicals/neurotoxins inducing PD-like symptoms areoften used, also with increasing use of the transgenicand knockout mice models of specific genes related tofamilial PD such as mutated a-synuclein, parkin,PINK-1, DJ-1, leucine rich repeat kinase (LRRK) 2.22
Among them, a neurotoxin 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) is commonly used since itcauses a selective loss of dopaminergic neurons andinduces typical PD-like symptoms in rodents, amphib-ians, nonhuman primates, and humans.19,23,24 Using
FIGURE 26.2 Schematic of some typical therapeutic
agents for PD and their pharmacological targets.
AADC, aromatic amino acid decarboxylase; BBB, bloodebrain barrier; COMT, catechol-O-methyl transferase; DA,dopamine; DARs, dopamine receptors; DAT, dopaminetransporter; DOPAC, 3,4-dihydroxy-phenylacetic acid;HVA, homovanillic acid; L-dopa, L-3,4-dihydroxypheny-lalanine; mAChR, muscarinic acetylcholine receptor;MAO-B, monoamine oxidase-B; MSN, medial spinyneuron; 3-OMD, 3-O-methyldopa; VMAT2, vesiclemonoamine transporter 2.
ND NEUROMUSCULAR

26. MPTP MODELS FOR PARKINSON’S DISEASE636
MPTP, the authors have studied the molecular details ofPD and actions of some therapeutic/neuroprotectivedrugs in mice and in common marmosets.15,25–29
In this chapter, we first overview the clinical symp-toms and characteristics observed in PD patients andin animal models, followed by summarizing the neuro-toxins used to establish PD models. Then, we describethe practical experimental methods and applicationswith some results relevant to PD both in mice and incommon marmosets.
CLINICAL CHARACTERISTICS OF PDAND THEIR RELEVANT SYMPTOMS IN
ANIMAL MODELS
To evaluate the animal models of human disease, it isessential to understand the clinical characteristics andsymptoms of the disease. In this section, we summarizethe epidemiological and clinical characteristics of PDbriefly, comparing with behavioral and molecular char-acteristics of animal models for PD.
Epidemiological Background
PD is the second most common neurodegenerativedisorder after Alzheimer’s disease.30 The prevalence ofPD is about 0.3% of the whole population in first-worldcountries. PD is more common in the elderly, and itsprevalence rises from 1% in those over 60 years of ageto 4% in the population over 80 years of age.30 Themean age of onset is around 60 years, although 5–10%of cases, classified as young onset, begin between theages of 20 and 50.31 Based on these facts, the use of adultanimals rather than juvenile ones for PD models soundsreasonable. Some studies have proposed that PD is morecommon in men than in women, but others failed todetect any differences between the two sexes.30
Many risk factors and protective factors have beenproposed, sometimes in relation to the theories concern-ing possible mechanisms of the disease; however, nonehave been conclusively related to PD by empiricalevidence. When epidemiological studies have beencarried out in order to test the relationship betweena given factor and PD, they have often been flawed,and their results have in some cases been contradic-tory.30 The most frequently replicated relationships arean increased risk of PD in those exposed to pesticidessuch as rotenone, paraquat, and maneb.30 Exposure tothese pesticides can double the risk of PD, and indirectmeasures of exposure, such as living in rural environ-ments, have also been found to increase the risk of PD.As we describe later, in fact, these pesticides are success-fully used to produce a PD model in experimentalanimals.
VII. THE BRAIN, STROKE, A
On the other hand, it was reported that the risk of PDwas reduced in smokers down to a third whencompared to that in nonsmokers.30 The basis for thiseffect is not known, but possibilities include an effectof nicotine as a DA stimulant.30,32 Tobacco smokecontains compounds that act as MAO inhibitors thatalso might contribute to this effect.33 Other substancesreported to reduce PD risk were caffeine,34 estrogens,anti-inflammatory drugs, and so on.30
Clinical Stages of PD
Although clinical experts describe the symptoms andstages of PD differently, it is sometimes classified basedon the daily-life disabilities with three stages as early,moderate, or advanced: Early represents the stagewhen a person has a mild tremor or stiffness but isable to continue work or other normal daily activities.This often refers to a person who has been newly diag-nosed with PD; Moderate refers to the stage whena person begins to experience limited movement. Aperson with moderate PD may have a mild to moderatetremor with slow movement; Advanced refers to thestage when a person is significantly limited in his orher activity, despite treatment. Daily changes in symp-toms, medicinal side effects that limit treatment, andloss of independence in the activities of daily living(ADLs) are common. A person with advanced PD mayhave significant and frequent changes in posture andmovement with speech difficulties.
The severity of PD may also fall into the followingfive stages known as Hoehn and Yahr’s scale: Stage I,symptoms affect only one side of the body; Stage II,both sides of the body are affected, but posture remainsnormal; Stage III, both sides of the body are affected, andthere is a mild imbalance during standing or walking,but the person remains independent; Stage IV, both sidesof the body are affected, and there is disabling instabilitywhile standing or walking. The person in this stagerequires substantial help; Stage V, severe, fully devel-oped disease is present. The person is restricted toa bed or chair. Dementia is also observed in 20–30% ofPD patients, although it only appears in the later stage.
Further a detailed classification established in 1987known as Unified Parkinson’s Disease Rating Scale(UPDRS), a world wide standard scale of PD, evaluatesboth motor and nonmotor symptoms subdivided intototal 42 subjects, rating each of them with five stages.UPDRS consists of five parts: I, evaluation of mentation,behavior and mood; II, self-evaluation of the ADLs suchas speech, swallowing, handwriting, dressing, hygiene,falling, salivating, turning in bed, walking, cuttingfood; III, evaluation of motor function scored by clini-cian; IV, Hoehn and Yahr’s scaling of PD severity; V,ADL scaling of Schwab and England. Although it takes
ND NEUROMUSCULAR

MOLECULAR PATHOPHYSIOLOGY OF PD 637
time for scoring all the subjects, it is also utilized to eval-uate drugs in clinical trial or the result of surgery.
Clinical Symptoms in PD Patients
The most common symptoms in PD include thefollowing five: (1) Tremor, or shaking, often in a hand,arm, or leg. Tremor caused by PD occurs when theperson is awake and sitting or standing still (restingtremor) and subsides when the person moves theaffected body part. It is often the first symptom thatpeople with PD or their family members notice. Initially,the tremor may appear in just one arm or leg or only onone side of the body. The tremor also may affect the chin,lips, and tongue. As the disease progresses, the tremormay spread to both sides of the body. But in some cases,the tremor remains on just one side. Emotional andphysical stresses tend to make the tremor more notice-able. Sleep, complete relaxation, and intentional move-ment or action usually reduce or stop the tremor.Although tremor is one of the most common signs ofPD, not everyone with tremor has PD. Unlike tremorcaused by PD, tremor caused by other conditions getsbetter when your arm or hand is not moving and getsworse when you try to move it. The most common causeof non-Parkinson’s tremor is an essential tremor, a treat-able condition that is often wrongly diagnosed as PD; (2)Stiff (rigidity) and aching muscles. One of the mostcommon early signs of PD is a reduced arm swing onone side when the person is walking that is caused byrigid muscles. Rigidity can also affect the muscles ofthe legs, face, neck, or other parts of the body and maycause muscles to feel tired and achy; (3) Slow, limitedmovement (bradykinesia), especially when the persontries to move from a resting position. For instance, itmay be difficult to get out of a chair or turn over inbed; (4) Weakness of face and throat muscles. Talkingand swallowing may become more difficult, and theperson may choke, cough, or drool. Speech becomessofter and monotonous. Loss of movement in themuscles in the face can cause a fixed, vacant facialexpression, often called the “Parkinson’s mask”; (5)Difficulty in walking (gait disturbance) and balance(postural instability). A person with PD is likely totake small steps and shuffle with his or her feet closetogether, bend forward slightly at the waist (stoopedposture), and have trouble turning around. Balanceand posture problems may cause frequent falls. Butthese problems usually do not develop until later inthe course of the disease.
Symptoms in Nonhuman Primates
Many clinical symptoms described above can bereproduced in the experimental nonhuman primates
VII. THE BRAIN, STROKE, A
probably because they are in the same species with us.Parameters to be analyzed are tremor, freezing, locomo-tion, fine motor skills, akinesia, balance, posture, startleresponse, gross motor skills, and so on.34 They areusually classified into subclasses from 0 (normal) to3–5 according to the severity. Alternatively, a scale ofclinical rating that ranges from 0 to 32 is also appli-cable.35 In some cases, fine motor skills are evaluatedwith computerized touch-panel systems.35 Detailedexamples of an MPTP-treated common marmoset willbe described in a later section.
Symptoms in Rodents
Although it is well known that rodent models forhuman diseases are favorable with genetic, biochemical,and anatomical studies, it does not always reflect exactbehavioral parameters with symptoms of the disease,because of the differential anatomy, biochemistry, andfunctions with human. Despite this discrepancy,researchers have developed many useful paradigms toassess motor dysfunctions of rodents as we describe ina later section. It is important to be aware that one exper-imental paradigm does not always reflect exactly onespecific parameter of human. For this reason, multipleparadigms are recommended to examine in each exper-imental project.
After administrating neurotoxins or chemicals des-cribed later, animals exhibit akinesia- and/or brady-kinesia-like symptoms, such as freezing, and abnormalmovement of limbs with tremor, slowness, rigidity,and so on. Behavioral tasks to analyze these motordysfunctions will be described later.
MOLECULAR PATHOPHYSIOLOGY OF PD
As we mentioned in the previous sections, PD is asso-ciated with the degeneration of the nigrostriatal dopami-nergic neurons. This means that a significant reductionof the striatal DA with its metabolites and molecularmarkers for dopaminergic neurons, such as tyrosinehydroxylase (TH), is observed with anatomical and/orbiochemical analysis.36 It is also known that the forma-tion of the acidophilic inclusions called Lewy bodieswith a high amount of a-synuclein and ubiquitinproteins is observed in the cytoplasm of the remainingbut degenerated neurons, together with some character-istic small projections called Lewy neurites.37 In fact,increasing evidence suggested that impaired proteolyticsystems of ubiquitin proteasome and/or lysosomecontributed to the accumulation of a-synuclein, caus-ing endoplasmic reticulum (ER) stress with progres-sion of the dopaminergic cell death.38,39 Mitochondrial
ND NEUROMUSCULAR
26. MPTP MODELS FOR PARKINSON’S DISEASE638
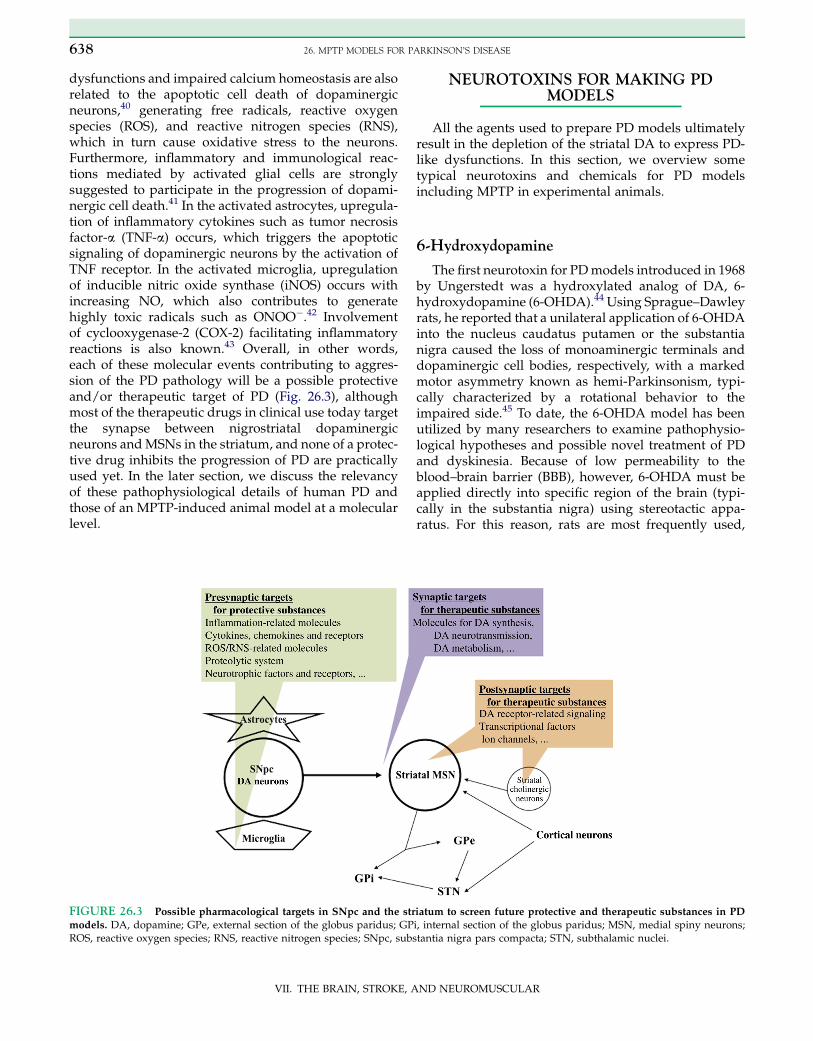
dysfunctions and impaired calcium homeostasis are alsorelated to the apoptotic cell death of dopaminergicneurons,40 generating free radicals, reactive oxygenspecies (ROS), and reactive nitrogen species (RNS),which in turn cause oxidative stress to the neurons.Furthermore, inflammatory and immunological reac-tions mediated by activated glial cells are stronglysuggested to participate in the progression of dopami-nergic cell death.41 In the activated astrocytes, upregula-tion of inflammatory cytokines such as tumor necrosisfactor-a (TNF-a) occurs, which triggers the apoptoticsignaling of dopaminergic neurons by the activation ofTNF receptor. In the activated microglia, upregulationof inducible nitric oxide synthase (iNOS) occurs withincreasing NO, which also contributes to generatehighly toxic radicals such as ONOO�.42 Involvementof cyclooxygenase-2 (COX-2) facilitating inflammatoryreactions is also known.43 Overall, in other words,each of these molecular events contributing to aggres-sion of the PD pathology will be a possible protectiveand/or therapeutic target of PD (Fig. 26.3), althoughmost of the therapeutic drugs in clinical use today targetthe synapse between nigrostriatal dopaminergicneurons andMSNs in the striatum, and none of a protec-tive drug inhibits the progression of PD are practicallyused yet. In the later section, we discuss the relevancyof these pathophysiological details of human PD andthose of an MPTP-induced animal model at a molecularlevel.
FIGURE 26.3 Possible pharmacological targets in SNpc and the str
models. DA, dopamine; GPe, external section of the globus paridus; GPROS, reactive oxygen species; RNS, reactive nitrogen species; SNpc, sub
VII. THE BRAIN, STROKE, A
NEUROTOXINS FOR MAKING PDMODELS
All the agents used to prepare PD models ultimatelyresult in the depletion of the striatal DA to express PD-like dysfunctions. In this section, we overview sometypical neurotoxins and chemicals for PD modelsincluding MPTP in experimental animals.
6-Hydroxydopamine
The first neurotoxin for PDmodels introduced in 1968by Ungerstedt was a hydroxylated analog of DA, 6-hydroxydopamine (6-OHDA).44 Using Sprague–Dawleyrats, he reported that a unilateral application of 6-OHDAinto the nucleus caudatus putamen or the substantianigra caused the loss of monoaminergic terminals anddopaminergic cell bodies, respectively, with a markedmotor asymmetry known as hemi-Parkinsonism, typi-cally characterized by a rotational behavior to theimpaired side.45 To date, the 6-OHDA model has beenutilized by many researchers to examine pathophysio-logical hypotheses and possible novel treatment of PDand dyskinesia. Because of low permeability to theblood–brain barrier (BBB), however, 6-OHDA must beapplied directly into specific region of the brain (typi-cally in the substantia nigra) using stereotactic appa-ratus. For this reason, rats are most frequently used,
iatum to screen future protective and therapeutic substances in PD
i, internal section of the globus paridus; MSN, medial spiny neurons;stantia nigra pars compacta; STN, subthalamic nuclei.
ND NEUROMUSCULAR
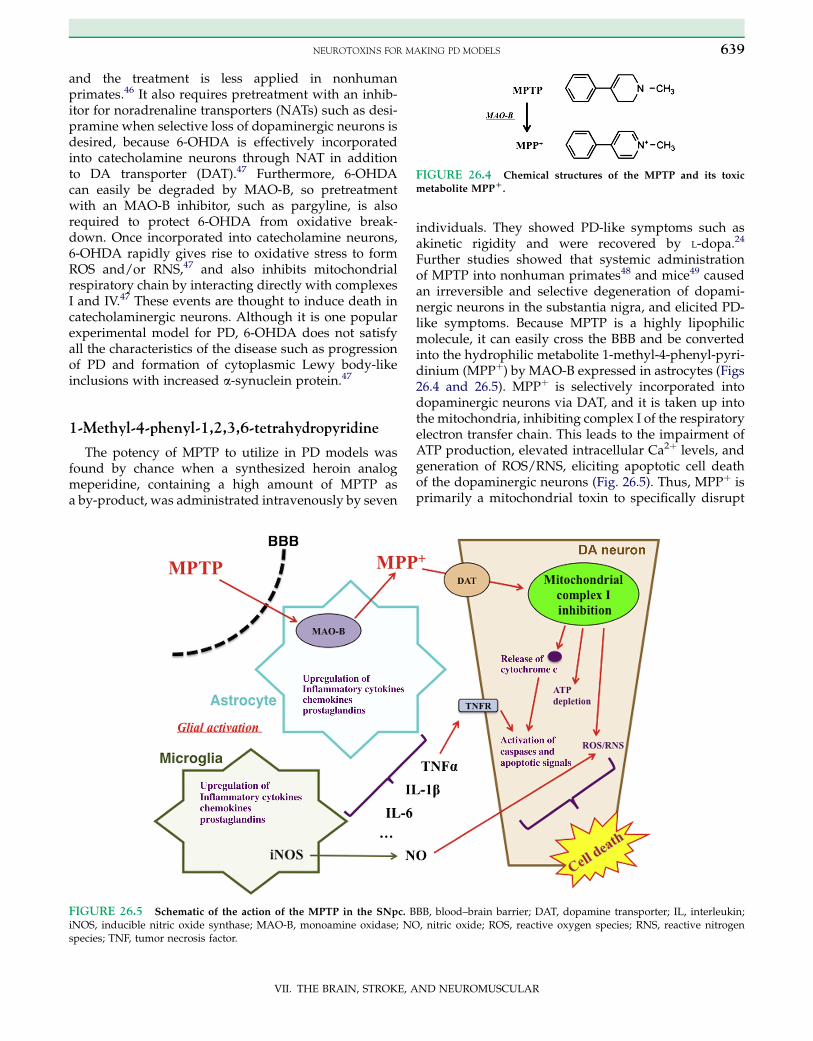
FIGURE 26.4 Chemical structures of the MPTP and its toxic
metabolite MPPD.
NEUROTOXINS FOR MAKING PD MODELS 639
and the treatment is less applied in nonhumanprimates.46 It also requires pretreatment with an inhib-itor for noradrenaline transporters (NATs) such as desi-pramine when selective loss of dopaminergic neurons isdesired, because 6-OHDA is effectively incorporatedinto catecholamine neurons through NAT in additionto DA transporter (DAT).47 Furthermore, 6-OHDAcan easily be degraded by MAO-B, so pretreatmentwith an MAO-B inhibitor, such as pargyline, is alsorequired to protect 6-OHDA from oxidative break-down. Once incorporated into catecholamine neurons,6-OHDA rapidly gives rise to oxidative stress to formROS and/or RNS,47 and also inhibits mitochondrialrespiratory chain by interacting directly with complexesI and IV.47 These events are thought to induce death incatecholaminergic neurons. Although it is one popularexperimental model for PD, 6-OHDA does not satisfyall the characteristics of the disease such as progressionof PD and formation of cytoplasmic Lewy body-likeinclusions with increased a-synuclein protein.47
1-Methyl-4-phenyl-1,2,3,6-tetrahydropyridine
The potency of MPTP to utilize in PD models wasfound by chance when a synthesized heroin analogmeperidine, containing a high amount of MPTP asa by-product, was administrated intravenously by seven
FIGURE 26.5 Schematic of the action of the MPTP in the SNpc. BiNOS, inducible nitric oxide synthase; MAO-B, monoamine oxidase; NOspecies; TNF, tumor necrosis factor.
VII. THE BRAIN, STROKE, A
individuals. They showed PD-like symptoms such asakinetic rigidity and were recovered by L-dopa.24
Further studies showed that systemic administrationof MPTP into nonhuman primates48 and mice49 causedan irreversible and selective degeneration of dopami-nergic neurons in the substantia nigra, and elicited PD-like symptoms. Because MPTP is a highly lipophilicmolecule, it can easily cross the BBB and be convertedinto the hydrophilic metabolite 1-methyl-4-phenyl-pyri-dinium (MPPþ) by MAO-B expressed in astrocytes (Figs26.4 and 26.5). MPPþ is selectively incorporated intodopaminergic neurons via DAT, and it is taken up intothe mitochondria, inhibiting complex I of the respiratoryelectron transfer chain. This leads to the impairment ofATP production, elevated intracellular Ca2þ levels, andgeneration of ROS/RNS, eliciting apoptotic cell deathof the dopaminergic neurons (Fig. 26.5). Thus, MPPþ isprimarily a mitochondrial toxin to specifically disrupt
BB, blood–brain barrier; DAT, dopamine transporter; IL, interleukin;, nitric oxide; ROS, reactive oxygen species; RNS, reactive nitrogen
ND NEUROMUSCULAR

26. MPTP MODELS FOR PARKINSON’S DISEASE640
the respiratory system of dopaminergic neurons.50
MPPþ also triggers inflammatory reactions startingfrom activation and proliferation of astrocyte and micro-glia.51 It facilitates synthesis and secretion of inflamma-tion-related molecules including cytokines such asTNF-a, interleukin 1b (IL-1b) and IL-6, chemokines,and prostaglandins. In microglia, the upregulation ofiNOS also occurs, resulting in the increase and releaseof NO, which attacks neurons with generating toxicROS and RNS. These events are well consistent withwhat happened in the brain of PD patients mentionedabove.
To date, a wide variety of animals including nema-todes,52 frogs,19 mice,53 rats,54 rabbits,16 cats,18 dogs,17
and nonhuman primates25 were demonstrated to havesensitivity to MPTP. Among them, nonhuman primateswith the highest MPTP sensitivity are ideal to use,though rodents are still the most widely used becauseof convenience. Mice are more favorably used than arerats because the latter exhibit a relatively high periph-eral MAO activity,55 causing conversion of MPTP toMPPþ before crossing the BBB, failing to enter the brain.If a researcher prefers to use MPTP in rats, it is necessaryto inject MPTP or MPPþ directly into the brain witha stereotactic apparatus as for 6-OHDA.56 Alternatively,intranasal administration of MPTP has been developedrecently,57 though its efficiency and specificity shouldbe examined in detail.
It should be noted that one significant difference ofthe MPTP model with human PD is the absence ofLewy bodies. Even by examining three different sched-ules of MPTP administration (acute, semichronic, andchronic), none of an obvious Lewy body-like inclusionwas found in mouse brain.58 It was also reported ina study that two monkeys survived over 10 years,demonstrating severe PD-like symptoms after MPTPtreatment in their youth and had no Lewy body-likeinclusions in their brains, even though the expressionof a-synuclein protein was increased significantly.59
We will discuss this discrepancy in a later section.
Pesticides
As we described in the previous section, exposure topesticides such as rotenone, paraquat, and maneb wasshown to have a positive correlation to the risk of PD.Rotenone is a lipophilic phenylpropanoid compound.Because of its selective inhibitory effect on the mitochon-drial respiratory complex I similar to MPPþ (but has nocell-type specificity), it was expected to be utilized asa chemical for PD models. In fact, chronic, but notacute, systemic administration of rotenone in rats at2.5 mg/kg/day for 7–33 days caused a loss of nigrostria-tal dopaminergic neurons, appearance of cytoplasmicinclusions reminiscent to Lewy body, which contained
VII. THE BRAIN, STROKE, A
a-synuclein and ubiquitin proteins, and motor dysfunc-tions including hypokinesis, hunched posture, rigidity,and tremor.60 This is quite an attractive model withmatching face and constructive validities with humanPD; however, rotenone also has a cardiovascular andother systemic toxicities in addition to the toxicity forcentral neurons, probably because of its cell-typenonspecific inhibition of mitochondrial complex I,resulting in a relatively high rate of mortality (w30%)with the results tending to vary.47
Different from rotenone, paraquat (1,10-dimethyl-4-40-bipyridinium:PQ)does not cross theBBB. It is transportedinto the brain by a neutral amino acid transporter and isincorporated into dopaminergic neurons with a sodium-dependent uptake system.61 As its chemical structureresembles that of MPPþ, it is thought to inhibit mitochon-drial respiratory complex I, resulting in a mild loss of thenigrostriatal dopaminergic neurons, although paraquatwas reported to have no specificity to DAT.62 On the otherhand, however, a recent report showed that paraquatcould be incorporated via DATwhen it was converted toamonovalent cationPQ(þ) rather than toanativedivalentcation state PQ(2þ).63 This and further studies areexpected to clarify the precise mechanism of the selectivetoxicity of paraquat on dopaminergic neurons.
Manganese ethylene-bis-dithiocarbamate, also calledmaneb, is known to inhibit mitochondrial respiratorycomplex III.64 It is frequently used in geographically over-lappingareaswithparaquat, and itwas reported that theircombined administration enhanced the toxicity than didtheir sole use, in fact.65 In addition, 30 mg/kg of manebwas reported to enhance the neurotoxicity induced by50 mg/kg of MPTP in mice examined with locomotoractivities and catalepsy test.66 Thus, it can be consideredthat a combination of neurotoxins usually enhances theexpression and progression of PD-like symptoms withdegenerating the nigrostriatal dopaminergic neurons,although an exception was also reported.67
Others
Chemicals other than neurotoxins listed abovedmainly interacting with molecules for dopaminergicneurotransmission, biosynthesis, and metabolismdarealso used for PD models, although many of their effectsare transient and do not cause a selective degenerationof dopaminergic neurons: Reserpine, an inhibitor forvesicle monoamine transporter (VMAT), causes thedepletion of synaptic DA; Methamphetamine also causesthe depletion of the striatal DA at synaptic terminals;Haloperidol, an inhibitor for D2 receptor typically causesthe antipsychotic drug-induced extrapyramidal syn-drome; and a-methyl p-tyrosine, an inhibitor for TH,causes depletion of L-dopa which in turn results in lossof dopamine.
ND NEUROMUSCULAR

MPTP-INDUCED MOUSE MODEL FOR PD 641
MPTP-INDUCED MOUSE MODEL FOR PD
Here, we describe practical methods to produce anMPTP-induced PD model of mice and how to analyzethem in a behavioral, immunohistochemical, andbiochemical manner. We also discuss the relevance ofmolecular details between the human PD model andthis model.
Animal Selection
Among the strains of mice examined (e.g. CD-1,C57BL/6, BALB-c, CBA/Ca, NMRI, and SwissWebster),C57BL/6 is now considered to exhibit the highest sensi-tivity to MPTP.53,68–71 Some researchers tried to explainthe reasons for the differential sensitivity among thestrains with difference of molecular details, includingthe activity of MAO-B,72 c-Jun N-terminus kinasesignaling with COX-2 expression,73 glial functions,74
and so on, although no conclusive result has beenobtained yet.
For the age of mice used, adult mice ranging from 7 to8 weeks to much older micedup to approximately12 monthsdare favored, and older animals exhibitedhigher MAO-B activity causing their increased sensi-tivity to MPTP.72
Drug Administration
Researchers should carefully handle MPTP in a safetycabinet by wearing gloves, a goggle, and amask to avoidunexpected inhalation. MPTP can be dissolved in wateror saline (150 mM NaCl) up to 10 mg/ml. It can also bedissolved in dimethyl-sulfoxide. Subcutaneous or intra-peritoneal administration of MPTP is generally per-formed using a 1 ml disposable syringe. Variousschedules and amounts of MPTP administration arereported; this may be roughly classified into three cate-gories: acute, subacute (semichronic), and chronic. Thefollowing is the frequently used dosing pattern:10–20 mg/kg given four times at 1–2 h intervals as anacute model; 30 mg/kg/day for 4–5 days as a subacutemodel; 25 mg/kg given 2 times with 250 mg/kg ofprobenecid in a week for 5 weeks as a chronic model.58
In fact, various substances including clinically approvedones were successfully evaluated with this model. Someof the typical substances analyzed by us are as follows:L-dopa, cabergoline, perindopril, riluzole, 7-nitroinda-zole, benzamide, zonisamide, and so on.15,25–29,75 Acuteand subacute models are especially favorable forscreening therapeutic substances efficiently byanalyzing their molecular details of pharmacology. Onthe other hand, subacute and chronic administration ofMPTP would reflect the processes of PD progression,suitable to analyze its molecular pathophysiology and
VII. THE BRAIN, STROKE, A
screening protective substances. In the case of a protec-tive substance to be applied chronically, the subacute(semichronic) protocol of MPTP administrationdescribed above is also applicable.
It should be noted that differential dosing results indifferential effects on behavioral, anatomical, and neuro-chemical parameters. For example, our previous study76
with various schedules and dosings of MPTP to maleC57BL/6N mice 8 weeks old resulted in differen-tial amounts of the striatal DA and its metabolites 3,4-dihydroxy-phenylacetic acid (DOPAC) and homova-nillic acid (HVA), even in the cases of the same total80 mg/kg dosing with four different schedules.76 Inthis study, we scheduled as follows: (1) 4 � 10 mg/kg/day for two consecutive days; (2) 1 � 20 mg/kg/day forfour consecutive days; (3) 2 � 20 mg/kg/day for twoconsecutive days; (4), 4 � 20 mg/kg in a day. The striatawere dissected out in 1, 2, and 3 weeks after MPTPadministration. As a result, reduction of the amount ofstriatal DA varied between the four groups: (1) showeda constant reduction to approximately 40% throughoutthe periods of examination; (2) only decreased toapproximately 70% in 1 week, then recovered to approx-imately 85%; (3) decreased to approximately 35% in1 week, but recovered to approximately 70% after2 weeks; (4) significantly decreased to approximately20%, and the effect was sustained throughout the3 weeks examined. The magnitude of reduction was(2) < (3) < (1) < (4), showing that acute administrationwith frequent injections resulted in the most effectiveand prolonged reduction of the striatal DA.
Behavioral Analysis
After administrating MPTP, evaluations of the func-tional motor coordination and/or balance are usuallyperformed with various behavioral tasks. As wementioned above, multiple tasks are recommended toexamine in each experimental project.
Generally, behavioral assessments are performedfrom a few hours to days after MPTP treatment. Itshould be noted that MPTP sometimes has an acuteinhibitory effect on skeletal muscles, probably by inhib-iting peripheral nicotinic acetylcholine receptors in theneuromuscular junctions.77 For this reason, it is highlyrecommended to start analysis at least with a 24 hinterval after the final MPTP treatment, especiallywhen a researcher wants to examine a therapeutic effectof a substance or so. We usually perform behavioralevaluations on or over 3 days after MPTP administration(20 mg/kg � four times, total 80 mg/kg with 2 h inter-vals in a day) when we want to examine a therapeuticeffect of a substance such as L-dopa, because the numberof the nigrostriatal dopaminergic neurons becomesminimum and that of activated astrocytes and microglia
ND NEUROMUSCULAR

26. MPTP MODELS FOR PARKINSON’S DISEASE642
becomes maximum.78 Also in our case examininga protective substance, we usually apply MPTP with10 mg/kg � four times at 1 h intervals (total 40 mg/kg) and apply the substance to be examined 30 minbefore and 90 min after the first administration ofMPTP, then perform behavioral tasks and biochemicalexaminations on or over the next day of MPTP adminis-tration.79 Alternatively, MPTP may be administered at30 mg/kg/day for 4–5 days, and the substance to beexamined would be started 1 day before startingMPTP administration, followed by daily applicationuntil stopping MPTP administration. Another issue isa behavioral recovery despite significant neurodegener-ative changes on the nigrostriatal dopaminergicneurons. A study showed that the differential timecourse of recovery was seen between the differentstrains of mice.69 This may also depend on which typeof behavioral tasks to apply. Thus, researchers shouldoptimize the schedule of dosing, type of the tasksapplied, and the timing to analyze carefully by a pilotexperiment. The following behavioral tasks arefrequently used to evaluate PD-like motor dysfunctionsin mice. We show some pictures of typical experimentalapparatuses in Fig. 26.6.
Catalepsy Test
This requires a relatively simple apparatus consistingof a horizontal bar (typically ranging from a 0.2 to 1 cmdiameter) made of wood or a stainless steel wire, span-ning between two pillars with a typical height of5–20 cm from the grounding platform. The periodduring which the mice maintain an immobile posturewhen putting their forepaws on the bar and hind pawson the ground, known as catalepsy, is recorded until
FIGURE 26.6 Experimental apparatuses to assess
motor dysfunctions of mice. (A) Pole test. (B) Rota-rodtest with a falling mouse on the right. (C) Open-fieldtest. (D) Beam-walking test.
VII. THE BRAIN, STROKE, A
they quit keeping the posture.80 A similar paradigmcalled the grip test is also applicable.69 Usually, naiveor vehicle-treated animals show a few seconds of a cata-lepsy period, while MPTP-treated mice show a typicallyprolonged period that is three to five folds.80 When themice quit the immobile posture, some of them may putall their paws on the ground, may lift their hind pawsup on the bar, and may move on it. The difficulty ofthis task is a relatively large variation of individualsespecially in MPTP-treated animals, which causesa failure to detect significance, even though the resultsshow a good tendency. Finally, researchers should alsonote that catalepsy not only reflects an extrapyramidalsyndrome but it is also caused by psychotic andhypnotic conditions in some cases.
Pole Test
This paradigm was originally developed to detectMPTP-induced bradykinesia, in 1987,81 and was alsoproven to be effective especially for detecting the anti-psychotic drug-induced extrapyramidal syndromewith D2R inhibition.82 The apparatus used consists ofa vertical pole fully taped with gauze typically ofa 40–50 cm height standing on a basement platform(Fig. 26.6A). Mice are first settled on the top of the polewith their heads looking upward. Mice then turn theirheads downward within a few seconds, and the latencyof this is called T-turn. Mice are subsequently moveddown along with the pole, and the latency to reach theground platform is called T-total. Although both T-turnand T-total can be parameters to be evaluated, the latterismore frequently used.MPTP prolongs both the param-eters significantly such as two to three times longer, andis recovered by a therapeutic drug such as L-dopa.81
ND NEUROMUSCULAR

MPTP-INDUCED MOUSE MODEL FOR PD 643
Rota-Rod Test
This is a frequently applied paradigm to assess themotor coordination of rodents (Fig. 26.6B).29 The rota-rod apparatus with constant and/or variable speedscan be purchased from many companies selling behav-ioral apparatuses. It consists of a rotating rod witha diameter of a few centimeters and is usually coveredby a rubber on its surface, and divided into 4–5 indi-vidual sections so that multiple animals can be assessedin one trial. Mice are put on the rotating rod witha constant speed, typically ranging from 15 to 32 rpmin a trial session, for an appropriate cutoff durationsuch as 10 min, and the latency to fall (LTF) on theground is recorded. Alternatively, the rotating speedmay be increased during the session, such as from 5 to30 rpm, with a constant increment. A well-trainedmouse without drugs can endure to keep walking onthe rod for >10 min even with 32 rpm. MPTP usuallyshortens the LTF significantly to the extent such asfrom half to one-third of the control. It requires sometraining sessions to minimize the variable of individ-uals. For this purpose, 1–2 training sessions per dayfor successive 2–3 days with a relatively lower speedthan that of the trial session should be performed beforeMPTP administration.
Open-Field Test
This is one of the most popular apparatus to evaluatelocomotor activity and exploratory behavior of rodentsin an open box surrounded by walls (Fig. 26.6C).69 Thefield is usually approximately 2500 cm2 (50 cm � 50 cm)divided into 25 areas by drawing lines onto it. There area wide variety of apparatuses and analyzes used, thoughessentially evaluating the spontaneous activity of theanimals with horizontal (distance traveled) and vertical(rearing) directions for various durations. Automatedrecording systems using an infrared beam and/orvideo-based tracing are convenient to use. Alternatively,just counting the number of transitions between thedivided areas and of rearing frequencies is also accept-able. To minimize the variety of individuals and toexclude an exploratory behavior in a novel field, pretrialhabitations may be required. When the effect of MPTP inmice is fully expressed, both horizontal and vertical activ-ities are decreased. This paradigm, however, is highlyaffected by emotional biases,83 so researchers have tomake surewhether the results are caused only by alterna-tion of motor functions.
Elevated Plus Maze
This paradigm is often used for screening anxiolyticdrugs such as benzodiazepines.83 As with the open-field
VII. THE BRAIN, STROKE, A
test, it can also be used to evaluate spontaneous loco-motor and exploratory activities, and is highly affectedby emotional biases. The maze is settled with a heightsuch as 45 cm with pillars standing from the groundfloor. The maze consists of four arms of pathwayscrossing at the center stage with a right angle, and thetwo paths facing each other have walls, while the othertwo have no wall. The number of arm entry and of rear-ing are convenient indexes of the horizontal and verticalactivities, respectively. When the mouse feels anxious, ittends to remain in the arm with a wall, so the time spentin each arm is also recorded. Frequencies of arm entriesdecrease in mice with motor impairment.
Beam-walking Test
The purpose of this test is to measure the traversingspeed of mice on a horizontal bar (Fig. 26.6D), evalu-ating a sensorimotor coordination and the integrity ofthe vestibular senses.84,85 A bar with a square ora circular shape, typically 50–60 cm in length, is posi-tioned at a height of 50 cm and is supported by twopillars, having a box at the goal end so that the micecan take rest after traversing. This requires sometraining sessions (e.g. three trials in a day for two succes-sive days) before the trial. In the training session, the barwith a relatively large diameter or width, such as12–16 mm, is used. In the trial session after MPTPadministration, mice are settled at the starting end ofthe bar with a diameter of 6–8 mm, and the time spentto reach the box is measured. The traversing speed ofMPTP-treated mice tends to be delayed and will berecovered by administering a therapeutic drug such asL-dopa. This seems to have a higher sensitivity thanother paradigms do, although some mice especiallythose treated with MPTP stop traversing in the middleof the bar (freezing)several times, which is also consid-ered to reflect one aspect of akinesia.
Footprint and Stepping Test
As described above in the section “Clinical symptomsin PD patients,” a PD patient tends to have troublewalking and balancing, taking small steps with his orher feet close together with abnormal balance. Similarsymptoms are also observed in MPTP-treated mice.Footprint test and a recently developed stepping testevaluate these abnormalities.86,87
In the footprint test, mice are trained to walk alonga straight line on a white paper before the trial. Afteradministrating drugs, mice with their forepaws placedin black ink walk on paper and the length of forepawsteps is measured. Stride length, usually 5–6 cm, isdetermined by measuring the distance between each
ND NEUROMUSCULAR

26. MPTP MODELS FOR PARKINSON’S DISEASE644
step on the same side of the body. MPTP decreases thelength from a half to a third compared to that of thecontrol mice.
In the stepping test,87 a mouse is allowed to settle atone edge of the table with a 1.2-m length, typicallywith all limbs on the table. The experimenter lifts thehind legs by pulling the tail up with only the forepawstouching the table. At a steady pace of approximately1 m in 3–4 s (for a total distance of 1 m), the experimenterpulled the animal backward by the tail, down towardthe other edge of the table, and the number of adjustingsteps from both forepaws is computed. A significantdecrease in this is observed in MPTP-treated micewhen compared to the saline-treated group of mice.
Immunohistochemical and BiochemicalEvaluations with Relevancy to PD
Anatomical and immunohistochemical evaluationscan be applied after mice have been fixed with 4% para-formaldehyde, by preparing paraffin-embed, frozen orfree-float sections, according to the researcher’s choice.
Most of the anatomical studies are performed in SNpcand in the striatum where dopaminergic neurons withtheir axons are lost by MPTP treatment. In SNpc, immu-nostaining with antibodies for TH, DAT, or neural nucleireliably detect the significant decrease in the number ofdopaminergic neurons after MPTP treatment. Ourprevious study in the case of acute MPTP administeredfour times as 20 mg/kg at 2 h intervals in a day (total80 mg/kg) resulted in nearly 60% of TH-positiveneurons being lost within 3 days, although around10% were recovered in 3 weeks after MPTP treatment,probably showing a recovery of TH protein expressionin the remaining neurons.78 Similarly, in the striatum,the density of TH-positive fibers was decreased signifi-cantly, indicating a degeneration of the dopaminergicaxons after MPTP administration.29
The neuronal death in SNpc includes apoptosisbecause the immunoreactive neurons to the antibodyfor single-strand DNA, one of a marker for apoptosis,significantly increased within 5 h till 3 days afterMPTP treatment.78 It was also reported that in theSNpc MPTP increased the protein expression of cleavedcaspase-3, one of the critical executers of apoptosis, andthe effects of MPTP were significantly decreased whenthe gene coding caspase-3 was disrupted.88 Many otherstudies also reported MPTP-induced apoptosis of thedopaminergic neurons in SNpc, and the apoptoticneurons were also found in SNpc of the postmortembrain of PD patients,89 showing a good relevancybetween this model and human PD.
MPTP also affects the activation of glial cells. Thenumber of both astrocytes detected by antiglial fibrillaryacidic protein (GFAP) or S100b antibodies and microglia
VII. THE BRAIN, STROKE, A
detected by isolectin B4 or anti-Iba-1 antibodywere significantly increased in the same conditionsgiven above.29,78,90 These glial cells abundantly expresscytokines and chemokines, such as IL-1b, IL-6, andTNF-a, related to inflammatory and immunological reac-tions, possibly mediating progression of neurodegenera-tion in both the human model and this model. Similarityof the time courses of p65 nuclear factor-kB (NF-kB)expression in the reactive astrocytes and ssDNAimmunoreactivity in neurons was observed after MPTPtreatment.78 Because NF-kB activation was found inboth postmortem PD brains and neurotoxin-inducedanimal models, it is also thought to be a key moleculeto induce neuronal apoptosis.91,92
MPTP also elicits oxidative stress, which is anotherfactor that causes dopaminergic degeneration(Fig. 26.2). In fact, the activities of superoxide dismu-tases and glutathione peroxidase were decreased, andmalondialdehyde, the end product of lipid peroxidation,was significantly increased after MPTP administra-tion.93 Involvement of the oxidative stress on PD isreported as mentioned above,40 so this is another rele-vant factor between animal models and human disease.
As we described in the previous section, the forma-tion of Lewy body including accumulated a-synucleinprotein oligomers and ubiquitin probably caused byabnormal ubiquitin–proteasome systems is a character-istic pathology in PD. In contradiction, however,many reports denied the formation of a Lewy body-likeinclusion in MPTP-treated mice.23,44,46,58,59 In addition,a proteasome inhibitor failed to induce or enhance neuro-toxicity on the nigrostriatal dopaminergic neurons.94,95
From these results, researchers may suspect thatMPTP cannot mimic the steps of protein degenerationcaused by ER stress in PD. However,MPTP, when admin-istered chronically using an osmotic minipump, but notwith sporadic administration, was reported to form neur-onal inclusions containing both increased a-synucleinand ubiquitin proteins.96 Although further examinationswill be necessary, it will open new insight to supportthe validity of MPTP model reproducing impairment ofproteolytic system and ER stress elicited in PD.
Many researchers have been interested in the protec-tive potency of neurotrophic factors including the brain-derived neurotrophic factor (BDNF)97–99 and glial cellline-derived neurotrophic factor (GDNF)100 with theirreceptors. In the mesolimbic dopaminergic pathwayoriginates from the ventral tegmental area innervatingthe nucleus accumbens showed less vulnerability toMPTP than the nigrostriatal pathway, and the expres-sion of mRNA of BDNF was higher in the former thanin the latter pathway, possibly explaining the differentialsensitivity to the neurotoxin.98 Furthermore, a studyusing Fluoro-Jade, a fluorescent detector of neurodegen-eration, and other antibodies showed that the neurons
ND NEUROMUSCULAR

MPTP-INDUCED COMMON MARMOSET MODEL FOR PD 645
expressing both TH and TrkB, a receptor of BDNF, wereless sensitive to MPTP than were other TH-positiveneurons in SNpc.99 Mouse-transplanted bone marrowstem cells expressing recombinant GDNF showed resis-tance to MPTP on behavioral, immunohistochemical,and biochemical levels,101 demonstrating successfuldelivery of GDNF in a macrophage-mediated mannerhad a protective effect on MPTP neurotoxicity. Nicotinewas reported to upregulate both basic fibroblast growthfactor 2 and BDNF in the striatum, showing protectiveeffects on MPTP-induced neurotoxicity.102 This suggeststhe reason why smokers show a lower risk of PDmentioned above. All these studies utilized an MPTPmodel, suggesting the possibility of future therapeuticsusing exogenous or endogenous neurotrophic factors.
In association with the loss of nigrostriatal dopami-nergic neurons, amounts of the striatal DA and itsmetabolites, DOPAC and HVA, are significantlydecreased. They are usually quantified by high-performance liquid chromatography (HPLC).29,76 Turn-over rate of DA is expressed with DA/(DOPAC þHVA), which can also be regarded as an indirect indexof the released DA (because it is degraded after releasefrom synaptic vesicles),103 although inhibition ofMAO-B and/or COMT also increases this value. Thisis also utilized to assess TH activity indirectly. L-Dopacould be an indirect index of TH activity under thecondition of AADC converting L-dopa to DA beinginhibited.104 NSD-1015A, a BBB-permeable AADC,when applied on mice 30 min prior to sacrifice, caninhibit TH in the brain; thus, L-dopa is accumulated.The accumulated L-dopa is decreased significantly byMPTP treatment, indicating that activity of TH wasdecreased in association with reduction of TH proteinexpression.104 HPLC is also combinedwith amicrodialy-sis to quantitate DA and its metabolites in the extracel-lular fluids of a specific brain region such as thestriatum in living animals, which enables researchersto measure the released DA directly.105
Changes of the protein amount are easily quantifiedby Western blot analysis with a higher sensitivity thanthat of histochemical methods. It is frequently used todetect the toxicity of MPTP in SNpc and a presynapticcomponent of the striatum with downregulation ofmarkers for the dopaminergic neurons TH, DAT, andVMAT2, together with the upregulation of the glialmarkers, such as GFAP and Iba-1,29 although it shouldbe combined with an immunohistochemical analysiswhen the information of cellular and subcellular locali-zation of themolecule is also necessary. Finding a proteinmarker reflecting MPTP toxicity in postsynaptic MSNshould also be considered because they will be a goodindex for the resulting effects of the loss of DA in thestriatum. Moreover, it will be a possible therapeutictarget in MSN (Fig. 26.3). For example, c-Fos protein is
VII. THE BRAIN, STROKE, A
one of the products of immediate early genes inducedby neuronal activity.106 We have recently found thata phosphorylated form of cyclin-dependent proteinkinase 5 (Cdk-5) was abundantly expressed in the stria-tal matrix compartment, suggesting the possibility ofthis molecule to be a marker reflecting activity ofMSN.107
Because MPTP affects both sides of brain hemi-spheres, researchers can utilize each hemisphere fordifferent purposes: one side for HPLC and the otherside for Western blot or reverse transcription poly-merase chain reaction (RT-PCR), for example.
Thus, the MPTP-induced mice model for PD showsmost of the pathological characteristics with humanPD, except for the formation of Lewy bodies, and hasbeen frequently utilized for drug screening and analysisof pathophysiological and pharmacological mechanismsof PD, its protection, and therapeutics.
Functional Imaging in Mice
Recent advances in imaging technologies haveenabled one to apply positron emission tomography(PET) to MPTP-treated mice. The first study that appliedPET in MPTP mice was reported in 2001,108 showingdecreased presynaptic ligand–DAT binding with N-3-fluoropropyl-2-b-[O-methyl-11C]carbomethoxy-3-b-(4-iodophenyl)-tropane ([11C]CIT-FP) and compensatoryupregulation of postsynaptic D2 receptors with [3H]raclopride after MPTP treatment. Since then, studiesusing PET have been gradually increasing, especiallywithin the past few years. This has been primarilyutilized to visualize the process of progressive degener-ation of dopaminergic neurons by MPTP treatment witha DAT ligand 2b-carbomethoxy-3b-(4-chlorophenyl)-8-(2-[18F]-fluoroethyl)-nortropane ([18F]FECNT)109 anda VMAT2 ligand 9-fluoropropyl-(þ)-dihydrotetrabena-zine ([18F]-DTBZ or AV-133).110,111 Although its applica-tion is still limited, PET imaging will be a powerful toolto understand the molecular events of PD and pharma-cology of therapeutics in living animals.
MPTP-INDUCED COMMON MARMOSETMODEL FOR PD
General Information for the Use of CommonMarmosets
Common marmoset is a nonhuman primate belong-ing to Cebidae Callitrichinae, a family of New Worldmonkeys, having a body length of approximately20 cm with a tail of about 25 cm, and an adult bodyweight >240 g. Because of its size, easiness of handl-ing compared to that of other monkeys and good
ND NEUROMUSCULAR

26. MPTP MODELS FOR PARKINSON’S DISEASE646
reproduction, it is a useful and favorable animal modelfor human diseases. A recent study of gene expressionanalysis comparing 26 genes between mice and com-mon marmosets distinguished some shared and differ-ent molecules expressed during the developmentalstages of the brain,112 possibly causing structural andfunctional differences between them.
Housing and MPTP Administration
Animals should be purchased from a reliable dealer ofexperimental animals. In general, both male and femaleanimals aged 2–4 years and weighing 240–400 g areused for experiments. Usually two animals per cage arehoused under controlled temperature (28 � 1 �C) andhumidity (50 � 5%) with a 12 h light–dark cycle. Beforestarting MPTP treatment, the animals are maintainedwith free access to food and water. After MPTP treat-ment, each animalmust be fedwithmilk artificially twicedaily when it is unable to voluntarily ingest sufficientfood. After MPTP administration, the behavioral studiesof Parkinsonism usually are performed by close observa-tion with video camera. MPTP administration is usuallydone with a variety of doses by a subcutaneous injection.Repeated administration at 24 h intervals is usually per-formed. According to the doses injected, the followingsymptoms are observed:
Progression of Abnormal Symptoms
The acute effects of MPTP include abnormal move-ments and alterations of motor behavior and posture.These effects may be observed after two or three dosesof MPTP (0.33 mg/kg) have been administered at 24 hintervals. The abnormalities become more striking aftereach successive dose. They occur within 5 min of drugadministration and, initially, may last for 15–30 min.After four or five doses, some of the acute motor effectsmay persist. The first motor signs to appear, usuallyafter the third dose, will be intermittent eyelid closure,a decrease in spontaneous movements, including lossof facial expression, and postural tremor. The animalswill be awake, however, andmay respond to loud noises
FIGURE 26.7 Common marmosets. (A) Normalcondition. (B) 14 days after MPTP treatment at a doseof 2.5 mg/kg given subcutaneously three times at inter-vals of 24 h.
VII. THE BRAIN, STROKE, A
by opening their eyes, looking at the examiner, andmaking weak threatening movements. The tremor willbe intermittently present, moderate in amplitude, andslow in frequency, and involve the proximal musclesof the extremities. A postural tremor of the head orjaw may be observed in some animals. These acutemotor effects may last up to 30 min. Motor signs thatappear only after four or five doses include abnormalfacial movements and changes in posture, muscle tone,and deglutition. Twitching of the facial muscles andfacial grimacing may be prominent effects seen in allthe animals. Extension of the head, rigidity of the upperand lower extremities may be demonstrated by passiverange-of-motion testing and may be sustained (turningto one side were observed in some of the animals).Some animals also may have difficulty in swallowing,as may be evidenced by drooling and the accumulationof food biscuits in their mouth pouches. Rotatory move-ments of the eyes may be observed in some animals. Inall the animals, eyelid closure, decreased spontaneousmotor activity, rigidity, postural tremor, and difficultyswallowing may persist with a cumulative dose of about1.7 mg/kg. Abnormal facial movements, head exten-sion, and rotatory eye movements, however, may beobserved only during the 30 min immediately afterdrug administration. After the 5-day period of drugadministration, other signs of motor impairment mayappear. These include general slowness of movement,a flexed posture, loss of hand dexterity, and “freezing”episodes. The animals remain seated, with markedflexion of the neck, thoracic spine, and upper and lowerextremities. There may be evident difficulty in pickingup food biscuits, which may be subsequently droppedwhile being carried to the animal’s mouth. Episodes of“freezing” or stopping in the middle of a motion maybe observed in some animals. Motor function deficitsmay appear to increase during the initial 2-week periodafter the last dose of the drug.
When a researcher wants to get a short-term maximaleffect of MPTP, it will be administered at a dose of2.5 mg/kg subcutaneously three times at intervalsof 24 h.15 In Fig. 26.7, we show a picture of normaland MPTP-treated common marmosets.
ND NEUROMUSCULAR

CONCLUDING REMARKS 647
Locomotor Activity
Evaluation is usually performed in a monitoring cageunit for locomotor activity with multiple infrared beamscovering the inside of the entire cage to automaticallydetect spontaneous activity of the animal. After a habitu-ation period of approximately 1 h, an interruption of aninfrared beam by a moving marmoset was automaticallyrecorded as a single locomotor count, accumulated over10 min for up to 8 h.
Scoring of Severity
The akinesia-like symptom develops, which can beclassified as 0–5: 0¼ The animal shows normal behavior;1 ¼ The animal appears quiet but exhibits a normalrepertoire of movements; 2 ¼ The animal can movefreely, but is clumsy when making complicated move-ment; 3 ¼ The animal makes few slower movementsand is obviously clumsy in executing complex move-ment; 4 ¼ The animal makes few movements unlessdisturbed, and then movement is slow and limited toa small region of the cage; 5 ¼ The animal is akineticand does not move even when disturbed.113 A well-trained observer scores while the locomotor activity isrecorded through a one-way mirror.
Immunohistochemical, Biochemical Analyses
Basically the same protocols as mice can be appliedfor immunohistochemical and biochemical analyzes,namely, immunostaining, HPLC, western blot, RT-PCR.
Functional Imaging in Common Marmosets
Although PET studies using MPTP on nonhumanprimates have been reported, any functional imagingstudy on MPTP-treated common marmosets has yet tobe reported. As various radiolabeled analogs interactingwith molecules of dopaminergic systems have beendeveloped,114 they will be examined in commonmarmo-sets in the near future.
CONCLUDING REMARKS
Here, we have described the characteristics andmeth-odological details of MPTP-induced mouse andcommon marmoset models for PD. As we have seen,these reliable models have a lot of merits compared tothat of other models, well satisfying the face, construc-tive, and predictive validities of human PD. As a facevalidity, bilateral motor dysfunctions related to extrapy-ramidal syndrome have been well reproduced espe-cially in nonhuman primates including the common
VII. THE BRAIN, STROKE, A
marmoset, and many behavioral tasks for mice alsohave been developed. As constructive validities, thefollowing characteristics observed in human PD arewell reproduced: specific cell death of nigrostriataldopaminergic neurons; decrease of the striatal DA andits metabolites; activation of astrocytes and microglia;oxidative stress caused by both mitochondrial dysfunc-tion and activated glial cells; inflammatory reactions.Although only one exception that does not matchhuman PD in the MPTP model is the formation ofLewy-like inclusion bodies containing a-synuclein andubiquitin proteins, it may also be reproduced undera certain condition of MPTP administration, probablyby continuous delivery with an osmotic minipump. Asa predictive validity, many of the drugs in clinical usefor PD are also effective in the MPTP model. To under-stand pathophysiological and pharmacological details,to develop novel therapeutics, and to screen possiblesubstances for protective and therapeutic drugs forPD, its applications including functional imaging willcontinue to expand further.
Acknowledgment
JK, HY, and NK would like to dedicate this chapter to the late Prof. T.Araki for his pioneering studies and warm encouragement.
References
1. Parkinson J. An Essay on the Shaking Palsy. London: Sherwood,Neely and Jones; 1817.
2. Chacot JM. Lecon sur les Maladies du Systeme Nerveux. 4th ed.Paris: Tome Premier; 1880.
3. Tretiakoff C. Contribution of a I’Etude de I’Anatomie Pathologiquedu Locus Niger. These de Paris; 1919.
4. Carlsson A. The occurrence, distribution and physiological roleof catecholamines in the nervous system. Pharmacol Rev
1959;11:490–3.5. Ehringer H, Hornykiewicz O. Distribution of noradrenaline and
dopamine (3-hydroxytyramine) in the human brain and theirbehavior in diseases of the extrapyramidal system. Klin
Wochenshr 1960;38:1236–9.6. German DC, Manaye K, Smith WK, et al. Ann Neurol
1989;26:507–14.7. Ma Y, Dhawan V, Mentis M, et al. Parametric mapping of [18F]
FPCT binding in early stage Parkinson’s disease: a PET study.Synapse 2002;45:125–33.
8. Jankovic J, Marsden CD. Parkinson’s Disease and Movement
Disorders. Baltimore: Urban/Schwarzenberg; 1988.9. Krack P, Hariz MI, Baunez C, et al. Deep brain stimulation: from
neurology to psychiatry? Trends Neurosci 2010;33:474–84.10. Rascol O, Lozano A, Stern M, et al. Milestones in Parkinson’s
disease therapeutics. Mov Disord 2011;26:1072–82.11. Encarnacion EV, Hauser RA. Levodopa-induced dyskinesias in
Parkinson’s disease: etiology, impact on quality of life, andtreatments. Eur Neurol 2008;60:57–66.
12. Trivedi MS, Jarbe T. A brief review on recent developments inanimal models of schizophrenia. Indian J Pharmacol 2011;43:375–80.
ND NEUROMUSCULAR

26. MPTP MODELS FOR PARKINSON’S DISEASE648
13. Kishima H, Poyot T, Bloch J, et al. Encapsulated GDNF-pro-ducing C2C12 cells for Parkinson’s disease: a pre-clinical studyin chronic MPTP-treated baboons. Neurobiol Dis 2004;16:428–39.
14. Saiki H, Hayashi T, Takahashi R, et al. Objective and quantita-tive evaluation of motor function in a monkey model of Par-kinson’s disease. J Neurosci Methods 2010;190:198–204.
15. Choudhury ME, Moritoyo T, Yabe H, et al. Zonisamide atten-uates MPTP neurotoxicity in marmosets. J Pharmacol Sci 2010;114:298–303.
16. Ghiribi O, Herman MM, Pramoonjago P, et al. MPPþ inducesthe endoplasmic reticulum stress response in rabbit braininvolving activation of the ATF-6 and NF-kappaB signalingpathways. J Neuropathol Exp Neurol 2003;62:1144–53.
17. Choi CB, Kim SY, Lee SH, et al. Assessment of metabolicchanges in the striatum of a MPTP-intoxicated canine model: invivo 1H-MRS study of an animal model for Parkinson’s disease.Magn Reson Imaging 2011;29:32–9.
18. Schneider JS, Rothblat DS. Neurochemical evaluation of thestriatum in symptomatic and recovered MPTP-treated cats.Neuroscience 1991;44:421–9.
19. Barbeau A, Dallaire L, Buu NT, et al. New amphibian modelsfor the study of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine(MPTP). Life Sci 1985;36:1125–34.
20. Park J, Kim SY, Cha GH, et al. Drosophila DJ-1 mutants showoxidative stress-sensitive locomotive dysfunction. Gene 2005;361:133–9.
21. Braungert E, Gerlach M, Riederer P, et al. Caenorhabditis elegansMPPþ model of Parkinson’s disease for high-throughput drugscreenings. Neurodegener Dis 2004;1:175–83.
22. Crabtree DM, Zhang J. Genetically engineered mouse models ofParkinson’s disease. Brain Res Bull 2012;88:13–32.
23. Blandini F, Armentero MT. Animal models of Parkinson’sdisease. FEBS J 2012;279:1156–66.
24. Langston JW, Ballard P, Terud JW, et al. Chronic parkinsonismin humans due to a product of meperidine-analog synthesis.Science 1983;219:979–80.
25. Nomoto M, Kita S, Iwata SI, et al. Effects of acute or prolongedadministration of cabergoline on parkinsonism induced byMPTPin common marmosets. Pharmacol Biochem Behav 1998;59:717–21.
26. Araki T, Kumagai T, Tanaka K, et al. Neuroprotective effect ofriluzole in MPTP-treated mice. Brain Res 2001;918:176–81.
27. Muramatsu Y, Kurosaki R, Mikami T, et al. Therapeutic effect ofneuronal nitric oxide synthase inhibitor (7-nitroindazole) againstMPTP neurotoxicity in mice. Metab Brain Dis 2002;17:169–82.
28. Yokoyama H, Kuroiwa H, Tsukada T, et al. Poly(ADP-ribose)polymerase inhibitor can attenuate the neuronal death after1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-induced neuro-toxicity in mice. J Neurosci Res 2010;88:1522–36.
29. Yokoyama H, Kuroiwa H, Yano R, et al. Therapeutic effectof a novel anti-Parkinsonian agent zonisamide against MPTP(1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) neurotoxicity inmice. Metab Brain Dis 2010;25:135–43.
30. de Lau LM, Breteler MM. Epidemiology of Parkinson’s disease.Lancet Neurol 2006;5:525–35.
31. Samii A, Nutt JG, Ransom BR. Parkinson’s disease. Lancet 2004;363:1783–93.
32. Quik M, Huang LZ, Parameswaran N, Bordia T, Campos C,Perez XA. Multiple roles for nicotine in Parkinson’s disease.Biochem Pharmacol 2009;78:677–85.
33. Castagnoli K, Murugesan T. Tobacco leaf, smoke and smoking,MAO inhibitors, Parkinson’s disease and neuroprotection: arethere links? Neurotoxicology 2004;25:279–91.
34. Bankiewicz KS, Sanchez-Pernaute R, Oiwa Y, et al. Preclinicalmodels of Parkinson’s disease. Curr Protocol Neurosci 1999;9.4.1–9.4.32.
VII. THE BRAIN, STROKE, A
35. Swanson CR, Joers V, Bondarenko V, et al. The PPAR-g agonistpioglitazone modulates inflammation and induces neuro-protection in parkinsonian monkeys. J Neuroinflammation2011;8:91–104.
36. Nagatsu T, Sawada M. Biochemistry of postmortem brains inParkinson’s disease: historical overview and future prospects. JNeural Transm Suppl 2007;(72):113–20.
37. Forno LS. Neuropathology of Parkinson’s disease. J Neuropathol
Exp Neurol 1996;55:259–72.38. Wang HQ, Takahashi R. Expanding insights on the involvement
of endoplasmic reticulum stress in Parkinson’s disease. AntioxidRedox Signal 2007;9:553–61.
39. Cachon-Gonzalez Cox T. The cellular pathology of lysosomaldisease. J Pathol 2012;226:241–54.
40. Calı T, Ottolini D, Brini M. Mitochondria, calcium, and endo-plasmic reticulum stress in Parkinson’s disease. Biofactors 2011;37:228–40.
41. Collins LM, Toulouse A, Connor TJ, et al. Contributions ofcentral and systemic inflammation to the pathophysiology ofParkinson’s disease. Neuropharmacology 2012;62:2154–68.
42. Tieu K, Ischiropoulos H, Pzedborski S. Nitric oxide and reactiveoxygen species in Parkinson’s disease. IUBMB Life 2003;55:329–35.
43. Minghetti L. Cyclooxygenase-2 (COX-2) in inflammatory anddegenerative brain diseases. J Neuropathol Exp Neurol 2004;63:901–10.
44. Ungerstedt U. 6-hydroxy-dopamine induced degeneration ofcentral monoamine neurons. Eur J Pharmacol 1968;5:107–10.
45. Ungerstedt U, Arbuthnott GW. Quantitative recording of rota-tional behavior in rats after 6-hydroxy-dopamine lesions of thenigrostriatal dopamine system. Brain Res 1970;24:485–93.
46. Betarbet R, Sherer TB, Greenamyre JT. Animal models of Par-kinson’s disease. Bioessays 2002;24:308–18.
47. Duty S, Jenner P. Animal models of Parkinson’s disease:a source of novel treatments and clues to the cause of thedisease. Br J Pharmacol 2011;164:1357–91.
48. Langston JW, Forno LS, Rebert CS, et al. Selective nigral toxicityafter systemic administration of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyrine (MPTP) in the squirrel monkey. Brain Res 1984;292:390–4.
49. Ricaurte GA, Irwin I, Forno LS, et al. Aging and 1-methyl-4-phenyl-1,2,3,6-tetrahydropyrine-induced degeneration ofdopaminergic neurons in the substantia nigra. Brain Res 1987;403:43–51.
50. Yokoyama H, Kuroiwa H, Kasahara J, et al. Neuropharmaco-logical approach against MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyrine)-induced mouse model of Parkinson’sdisease. Acta Neurobiol Exp 2011;71:1–13.
51. Yokoyama H, Uchida H, Kuroiwa H, et al. Role of glial cells inneurotoxin-induced animal models of Parkinson’s disease.Neurol Sci 2011;32:1–7.
52. Wang YM, Pu P, Le WD. ATP depletion is the major cause ofMPPþ induced dopamine neuronal death and worm lethality inalpha-synuclein transgenic C. elegans. Neurosci Bull 2007;2007(23):329–35.
53. Sunderstrom E, Fredriksson A, Archer T. Chronic neurochem-ical and behavioral changes in MPTP-lesioned C57BL/6 mice:a model for Parkinson’s disease. Brain Res 1990;528:181–8.
54. Laret ML, San Millian JA, Fabre E, et al. Deprenyl protects fromMPTP-induced Parkinson-like syndrome and glutathioneoxidation in rat striatum. Toxicology 2002;170:165–71.
55. Kakaria RN, Mitchell MH, Harik SI. Correlation of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine neurotoxicity with blood–-brain barrier monoamine oxidase activity. Proc Natl Acad Sci
USA 1987;84:3521–5.
ND NEUROMUSCULAR
CONCLUDING REMARKS 649
56. Heikkila RE, Niclas WJ, Duvoisin RC. Dopaminergic toxicityafter the stereotaxic administration of the 1-methyl-4-phenyl-pyridinium ion (MPPþ) to rats. Neurosci Lett 1985;59:135–40.
57. Predinger RD, Nguiar Jr AS, Matheus FC, et al. Intranasaladministration of neurotoxicants in animals: support for theolfactory vector hypothesis of Parkinson’s disease. Neurotox Res
2012;21:90–116.58. Shimoji M, Zhang L, Mandir AS, et al. Absence of inclusion
body formation in the MPTP mouse model of Parkinson’sdisease. Brain Res Mol Brain Res 2005;134:103–8.
59. Halliday G, Herrero MT, Murphy K, et al. No Lewy pathologyin monkeys with over 10 years of severe MPTP parkinsonism.Mov Disord 2009;24:1519–23.
60. Betarbet R, Sherer TB, MacKenzie G, et al. Chronic systemicpesticide exposure reproduces features of Parkinson’s disease.Nat Neurosci 2000;3:1301–6.
61. Shimizu K, Ohtaki K, Matsubara K, et al. Carrier-mediatedprocesses in blood–brain barrier penetration and neural uptakeof paraquat. Brain Res 2001;906:135–42.
62. Richardson JR, Quan Y, Sherer TB, et al. Paraquat neurotoxicityis distinct from that of MPTP and rotenone. Toxicol Sci 2005;88:193–201.
63. Rappold PM, Cui M, Chesser AS, et al. Paraquat neurotoxicity ismediated by the dopamine transporter and organic cationtransporter-3. Proc Natl Acad Sci USA 2011;108:20766–71.
64. Zhang J, Fitsanakis VA, Gu G, et al. Manganese ethylene-bisdithiocarbamate and selective dopaminergic neurodegenerationin rat: a link through mitochondrial dysfunction. J Neurochem
2003;84:336–46.65. ThiruchelvamM, Brockel BJ, Richfield EK, et al. Potentiated and
preferential effects of combined paraquat and maneb onnigrostriatal dopamine systems: environmental risk factors forParkinson’s disease? Brain Res 2000;873:225–34.
66. Takahashi RN, Rogerio R, Zanin M. Maneb enhances MPTPneurotoxicity in mice. Res Commun Chem Pathol Pharmacol
1989;66:167–70.67. Aoki E, Yokoyama H, Kimoto H, et al. Chronic administration
with rotenone does not enhance MPTP neurotoxicity in C57BL/6 mice. J Mol Neurosci 2010;41:17–24.
68. Muthane U, Ramsay KA, Jiang H, et al. Differences in nigralneuron number and sensitivity to 1-methyl-4-phenyl-1,2,3,6-te-trahydropyridine in C57/bl and CD-1 mice. Exp Neurol 1994;126:195–204.
69. Sedelis M, Hofele K, Auburger GW, et al. MPTP susceptibility inthe mouse: behavioral, neurochemical, and histological analysisof gender and strain differences. Behav Genet 2000;30:171–82.
70. Filipov NM, Norwood AB, Sistrunk SC. Strain-specific sensi-tivity to MPTP of C57BL/6 and BALB/c mice is age dependent.Neuroreport 2009;20:713–7.
71. Sunderstrom E, Stromberg I, Tsushumi T, et al. Studies on theeffect of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)on central catecholamine neurons in C57BL/6 mice.Comparison with three other strains of mice. Brain Res 1987;405:26–38.
72. Walsh LS, Wanger GC. Age-dependent effects of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP): correlation withmonoamine oxidase-B. Synapse 1989;3:308–14.
73. Boyd JD, Jang H, Shepherd KR, et al. Response to 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) differs in mousestrains and reveals a divergence in JNK signaling and COX-2induction prior to loss of neurons in the substantia nigra parscompacta. Brain Res 2007;1175:107–16.
74. Smeyne M, Goloubeva O, Smeyne RJ. Strain-dependentsusceptibility to MPTP and MPP(þ)-induced parkinsonism isdetermined by glia. Glia 2001;34:73–80.
VII. THE BRAIN, STROKE, A
75. Kurosaki R, Muramatsu Y, Imai Y, et al. Neuroprotective effectof the angiotensin-converting enzyme inhibitor perindopril inMPTP-treated mice. Neurol Res 2004;26:644–57.
76. Kuroiwa H, Yokoyama H, Kimoto H, et al. Biochemical alter-ations of the striatum in an MPTP-treated mouse model ofParkinson’s disease. Metab Brain Dis 2010;25:177–83.
77. Hsu KS, Fu WM, Lin-Shiau SY. Blockade by MPTP of thenicotinic acetylcholine receptor channels in embryonic xenopusmuscle cells. Neuropharmacology 1994;33:35–41.
78. Aoki E, Yano R, Yokoyama H, et al. Role of nuclear transcriptionfactor kappa B (NF-kappaB) for MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahyropyridine)-induced apoptosis in nigral neuronsof mice. Exp Mol Pathol 2009;86:57–64.
79. Yano R, Yokoyama H, Kuroiwa H, et al. A novel anti-Parkin-sonian agent, zonisamide, attenuates MPTP-induced neurotox-icity in mice. J Mol Neurosci 2009;39:211–9.
80. Watanabe Y, Kato H, Araki T. Protective action of neuronal nitricoxide synthase inhibitor in the MPTP mouse model of Parkin-son’s disease. Metab Brain Dis 2008;23:51–69.
81. Ogawa N, Mizukawa K, Hirose Y, et al. MPTP-inducedParkinsonian model in mice: biochemistry, pharmacology andbehavior. Eur Neurol 1987;26:16–23.
82. Ohno Y, Ishida K, Ikeda K, et al. Evaluation of bradykinesiainduction by SM-9018, a novel 5-HT2 and D2 receptor antago-nist, using the mouse pole test. Pharmacol Biochem Behav 1994;49:19–23.
83. BelzungC,GriebelG.Measuringnormal andpathological anxiety-like behaviour in mice: a review. Behav Brain Res 2001;125:141–9.
84. Dean RL, Scozzafava J, Goas JA, et al. Age-related differences inbehavior across the life span of the C57BL/6J mouse. Exp Aging
Res 1981;7:427–51.85. Sato K, Sumi-Ichinose C, Kaji R, et al. Differential involvement
of striosome and matrix dopamine systems in a transgenicmodel of dopa-responsive dystonia. Proc Natl Acad Sci USA
2008;105:12551–6.86. Mohanasundari M, Srinivasan MS, Sethupathy S, et al.
Enhanced neuroprotective effect by combination of bromocrip-tine and Hypericum perforatum extract against MPTP-inducedneurotoxicity in mice. J Neurol Sci 2006;249:140–4.
87. Blume SR, Cass DK, Tsueng KY. Stepping test in mice: a reliableapproach in determining forelimb akinesia in MPTP-inducedparkinsonism. Exp Neurol 2009;219:208–11.
88. Yamada M, Kida K, Amutuhaire W, et al. Gene disruption ofcaspase-3 prevents MPTP-induced Parkinson’s disease in mice.Biochem Biophys Res Commun 2010;402:312–8.
89. Mochizuki H, Goto K, Mori H, et al. Histochemical detection ofapoptosis in Parkinson’s disease. J Neurol Sci 1996;137:120–3.
90. Himeda T, Watanabe Y, Tounai H, et al. Time dependent alter-ations of co-localization of S100beta and GFAP in the MPTP-treated mice. J Neural Transm 2006;113:1887–94.
91. Langston JW. Parkinson’s disease: current and future chal-lenger. Neurotoxicol 2002;23:443–50.
92. Ghosh A, Roy A, Liu X, Kordower JH, et al. Selective inhibitionof NF-kappaB activation prevents dopaminergic neuronal lossin a mouse model of Parkinson’s disease. Proc Natl Acad Sci USA2007;104:18754–9.
93. Li S, Pu XP. Neuroprotective effect of kaempferol againsta 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-induced mousemodel of Parkinson’s disease. Biol Pharm Bull 2011;34:1291–6.
94. Kadoguchi N, Umeda M, Kato H, et al. Proteasome inhibitordoes not enhance MPTP neurotoxicity in mice. Cell Mol Neuro-
biol 2008;28:971–9.95. Kadoguchi N, Kimoto H, Yano R, et al. Failure of acute
administration with proteasome inhibitor to provide a model ofParkinson’s disease in mice. Metab Brain Dis 2008;23:147–54.
ND NEUROMUSCULAR

26. MPTP MODELS FOR PARKINSON’S DISEASE650
96. Fornai F, Schluter OM, Lenzi P, et al. Parkinson-like syndromeinduced by continuous MPTP infusion: convergent roles of theubiquitin-proteasome system and alpha-synuclein. Proc NatlAcad Sci USA 2005;102:3413–8.
97. Nagahara AH, Tuszynski MH. Potential therapeutic uses ofBDNF in neurological and psychiatric disorders. Nat Rev Drug
Discov 2011;10:209–19.98. Hung HC, Lee EH. The mesolimbic dopaminergic pathway is
more resistant than the nigrostriatal dopaminergic pathway toMPTP and MPPþ toxicity: role of BDNF gene expression. BrainRes Mol Brain Res 1996;41:14–26.
99. Ding YX, Xia Y, Jiao XY, et al. The TrkB-positive dopaminergicneurons are less sensitive to MPTP insult in the substantia nigraof adult C57/BL mice. Neurochem Res 2011;36:1759–66.
100. Rangasamy SB, Soderstrom K, Bakay RA, et al. Neurotrophicfactor therapy for Parkinson’s disease. Prog Brain Res 2010;184:237–64.
101. Biju K, Zhou Q, Li G, et al. Macrophage-mediated GDNFdelivery protects against dopaminergic neurodegeneration:a therapeutic strategy for Parkinson’s disease. Mol Ther 2010;18:1536–44.
102. Maggio R, Riva M, Vaglini F, et al. Nicotine prevents experi-mental parkinsonism in rodents and induces striatal increase ofneurotrophic factors. J Neurochem 1998;71:2439–46.
103. Hollerman JR, Grace AA. The effects of dopamine-depletingbrain lesions on the electrophysiological activity of rat sub-stantia nigra dopamine neurons. Brain Res 1990;533:203–12.
104. Perrin D, Mamet J, Scarna H, et al. Long-term prenatal hypoxiaalters maturation of brain catecholaminergic systems and motorbehavior in rats. Synapse 2004;54:92–101.
105. Olive MF, Mehmert KK, Hodge CW. Microdialysis in the mousenucleus accumbens: a method for detection of monoamine andamino acid neurotransmitters with simultaneous assessment oflocomotor activity. Brain Res Brain Res Protoc 2000;5:16–24.
VII. THE BRAIN, STROKE, A
106. Chen JY, Hsu PC, Hsu IL, et al. Sequential up-regulation of thec-fos, c-jun and bax genes in the cortex, striatum and cerebelluminduced by a single injection of a low dose of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) in C57BL/6 mice.Neurosci Lett 2001;314:49–52.
107. Morigaki R, SakoW,Okita S, et al. Cyclin-dependent kinase 5withphosphorylation of tyrosine 15 residue is enriched in striatalmatrix compartment in adult mice. Neuroscience 2011;189:25–31.
108. Ishiwata K, Koyanagi Y, Abe K, et al. Evaluation of neurotox-icity of TIQ and MPTP and of parkinsonism-preventing effect of1-MeTIQ by in vivo measurement of pre-synaptic dopaminetransporters and post-synaptic dopamine D(2) receptors in themouse striatum. J Neurochem 2001;79:868–76.
109. Honer M, Hengerer B, Blagoev M, et al. Comparison of [18F]FDOPA, [18F]FMT and [18F]FECNT for imaging dopaminergicneurotransmission in mice. Nucl Med Biol 2006;33:607–14.
110. Chao KT, Tsao HH, Weng YH, et al. Quantitative analysis ofbinding sites for 9-fluoropropyl-(þ)-dihydrotetrabenazine([(18F)]AV-133) in a MPTP-lesioned PD mouse model. Synapse2012;66:823–31.
111. Toomey JS, Bhatia S, Moon LT, et al. PET Imaging a MPTP-induced mouse model of Parkinson’s disease using the fluo-ropropyl-dihydrotetrabenazine analog [(18)F]-DTBZ (AV-133).PLoS One 2012;7:e39041.
112. Mashiko H, Yoshida AC, Kikuchi SS, et al. Comparativeanatomy of marmoset and mouse cortex from genomic expres-sion. J Neurosci 2012;32:5039–53.
113. Rose S, Nomoto M, Jackson EA, et al. Age-related effects of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine treatment ofcommon marmosets. Eur J Pharmacol 1993;230:177–85.
114. Minuzzi L, Olsen AK, Bender D, et al. Quantitative autoradi-ography of ligands for dopamine receptors and transporters inbrain of Gottingen minipig: comparison with results in vivo.Synapse 2006;59:211–9.
ND NEUROMUSCULAR









![ChronicandAcuteModelsofRetinalNeurodegeneration · 2,6-dioxo-1,2,3,6-tetrahydro-purin-7-yl)-acetyl]-urea) was by coupling theophylline-7-acetic acid to N , N -diisopropyl car- bodiimide](https://img.dokumen.tips/doc/110x75/5b9e8b5909d3f2d7748cb267/chronicandacutemodelsofretinal-26-dioxo-1236-tetrahydro-purin-7-yl-acetyl-urea.jpg)









![Tetrahydropyridine: a promising heterocycle for ...antiinflammatory activity.46 4,5,6,7-Tetrahydrothieno[2,3-c]pyridine derivatives were synthesized by Fujita et al. and evaluated](https://img.dokumen.tips/doc/110x75/60d5bc575f680b4fdb5a8441/tetrahydropyridine-a-promising-heterocycle-for-antiinflammatory-activity46.jpg)








