Embed Size (px)
Citation preview

lACC Vol. 3. NO.3March 1984:845-9
REPORTS ON THERAPY
Angioplasty in Total Coronary Artery Occlusion
845
DAVID R. HOLMES, Jr., MD, FACC, RONALD E. VLIETSTRA, MD, FACC, GUY S. REEDER, MD,
JOHN F. BRESNAHAN, MD, HUGH C. SMITH, MD, FACC, ALFRED A. BOVE, MD,
HARTZELL V. SCHAFF, MD
Rochester. Minnesota
Percutaneous transluminal coronary angioplasty was attempted without streptokinase in 24 patients with totalcoronary artery occiusion but without acute transmuralmyocardial infarction. The maximal duration of occlusion was estimated to be 1 week or less in 10 patients,more than 1 to 4 weeks in 6, more than 4 to 12 weeksin 3 and more than 12 weeks in 5. Dilation of the occludedartery was attempted in the left anterior descendingcoronary artery in 17 patients, in the right coronaryartery in 4 and in the circumflex coronary artery in 3.Angioplasty was successful in 13 patients (54%): leftanterior descending coronary artery in 59 %, right coronary artery in 50% and circumflex coronary artery in
Since its introduction in 1977, percutaneous transluminalcoronary angioplasty has been used with increasing frequency in patients with symptomatic coronary artery disease(1-7). Although the technique was initially reserved forpatients with a single discrete stenosis, experience has shownthat it may be applied in selected patients with left maincoronary artery narrowing, coronary artery bypass graft stenosis and multiple vessel coronary artery disease (4,8-13).Current criteria for elective coronary angioplasty, however,still include the presence of high-grade but subtotal coronaryobstruction.
This study deals with the feasibility of coronary angioplasty alone in a selected group of patients with total coronary artery occlusion without associated acute myocardialinfarction in whom the duration of occlusion could beestimated.
From the Division of Cardiovascular Diseases and Internal Medicine.and the Section of Thoracic. Cardiovascular. Vascular and General Surgery, Mayo Clinic and Mayo Foundation. Rochester. Minnesota. Manuscript received May 12. 1983; revised manuscript received September 20.1983. accepted September 21. 1983.
Address for reprints: David R. Holmes Jr.. MD. Division of Cardiovascular Diseases and Internal Medicine, Mayo Clinic. 200 First StreetSW. Rochester, Minnesota 55905.
© 1984 by the American College of Cardiology
33%. In patients with successful dilation, there was amean decrease in coronary artery stenosis from 100 to23%. In the 19 patients whose occlusion was estimatedto be of 12 weeks' duration or less, angioplasty wassuccessful in 68%. In the five patients whose occlusionwas estimated to be of more than 12 weeks' duration,dilation was not successful in any (p = 0.006).
It is concluded that in selected patients with symptomatic coronary artery disease and recent coronary artery occlusion without associated acute myocardial infarction, percutaneous transluminal coronary angioplastyalone may be effective in restoring patency.
MethodsStudy group. Patient selection. From October 1979 to
the end of November 1982, percutaneous transluminal coronary angioplasty was attempted after informed consent in24 patients with total coronary artery occlusion without associated acute transmural myocardial infarction. No patientreceived streptokinase therapy. These 24 patients represent10.4% of all patients undergoing attempted coronary angioplasty during this period at the Mayo Clinic. There were20 men and 4 women with a mean age of 58.4 years (range48 to 75).
Clinical findings. All patients had prior angina pectoris(mean duration 50.5 weeks; range I to 260). Fifteen patientshad had angina pectoris for 6 months or less. Thirteen patients were in New York Heart Association functional classIV, eight were in class III and three were in class II. Twelvepatients had a definite increase in frequency and severity ofangina pectoris within I month before evaluation. Althoughno patient had a documented evolving transmural acute myocardial infarction, four had a recent myocardial infarctionfrom I week to I month before attempted dilation-threewith a subendocardial infarction and one with a transmuralmyocardial infarction. No patient had documented coronaryartery spasm.
0735-1097/84/$3.00
846 HOLMES ET AL.ANGIOPLASTY IN CORONARY OCCLUSION
lACC Vol. 3. No.3March 1984:845-9
Results
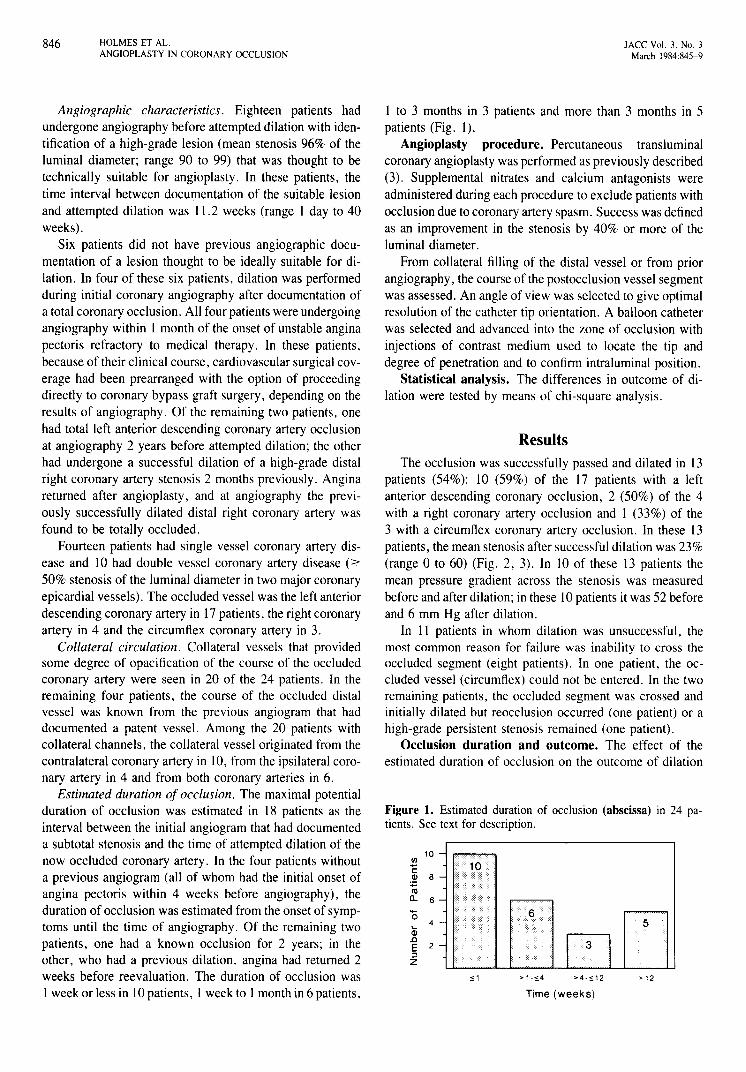
Figure 1. Estimated duration of occlusion (abscissa) in 24 patients. See text for description.
>12
Time (weeks)
> 1 ~'5.4",1
10rnc:Ql 8
:;::roa. 6
'05... 4
Ql.cE 2::lZ
The occlusion was successfully passed and dilated in 13patients (54%): 10 (59%) of the 17 patients with a leftanterior descending coronary occlusion, 2 (50%) of the 4with a right coronary artery occlusion and I (33%) of the3 with a circumflex coronary artery occlusion. In these 13patients, the mean stenosis after successful dilation was 23%(range 0 to 60) (Fig. 2, 3). In 10 of these 13 patients themean pressure gradient across the stenosis was measuredbefore and after dilation; in these 10 patients it was 52 beforeand 6 mm Hg after dilation.
In II patients in whom dilation was unsuccessful, themost common reason for failure was inability to cross theoccluded segment (eight patients). In one patient, the occluded vessel (circumflex) could not be entered. In the tworemaining patients, the occluded segment was crossed andinitially dilated but reocclusion occurred (one patient) or ahigh-grade persistent stenosis remained (one patient).
Occlusion duration and outcome. The effect of theestimated duration of occlusion on the outcome of dilation
I to 3 months in 3 patients and more than 3 months in 5patients (Fig. I).
Angioplasty procedure. Percutaneous transluminalcoronary angioplasty was performed as previously described(3). Supplemental nitrates and calcium antagonists wereadministered during each procedure to exclude patients withocclusion due to coronary artery spasm. Success was definedas an improvement in the stenosis by 40% or more of theluminal diameter.
From collateral filling of the distal vessel or from priorangiography, the course of the postocclusion vessel segmentwas assessed. An angle of view was selected to give optimalresolution of the catheter tip orientation. A balloon catheterwas selected and advanced into the zone of occlusion withinjections of contrast medium used to locate the tip anddegree of penetration and to confirm intraluminal position.
Statistical analysis. The differences in outcome of dilation were tested by means of chi-square analysis.
Angiographic characteristics. Eighteen patients hadundergone angiography before attempted dilation with identification of a high-grade lesion (mean stenosis 96% of theluminal diameter; range 90 to 99) that was thought to betechnically suitable for angioplasty. In these patients, thetime interval between documentation of the suitable lesionand attempted dilation was 11.2 weeks (range I day to 40weeks).
Six patients did not have previous angiographic documentation of a lesion thought to be ideally suitable for dilation. In four of these six patients, dilation was performedduring initial coronary angiography after documentation ofa total coronary occlusion. All four patients were undergoingangiography within I month of the onset of unstable anginapectoris refractory to medical therapy. In these patients,because of their clinical course, cardiovascular surgical coverage had been prearranged with the option of proceedingdirectly to coronary bypass graft surgery, depending on theresults of angiography. Of the remaining two patients, onehad total left anterior descending coronary artery occlusionat angiography 2 years before attempted dilation; the otherhad undergone a successful dilation of a high-grade distalright coronary artery stenosis 2 months previously. Anginareturned after angioplasty, and at angiography the previously successfully dilated distal right coronary artery wasfound to be totally occluded.
Fourteen patients had single vessel coronary artery disease and 10 had double vessel coronary artery disease (2:50% stenosis of the luminal diameter in two major coronaryepicardial vessels). The occluded vessel was the left anteriordescending coronary artery in 17 patients, the right coronaryartery in 4 and the circumflex coronary artery in 3.
Collateral circulation. Collateral vessels that providedsome degree of opacification of the course of the occludedcoronary artery were seen in 20 of the 24 patients. In theremaining four patients, the course of the occluded distalvessel was known from the previous angiogram that haddocumented a patent vessel. Among the 20 patients withcollateral channels, the collateral vessel originated from thecontralateral coronary artery in 10, from the ipsilateral coronary artery in 4 and from both coronary arteries in 6.
Estimated duration of occlusion. The maximal potentialduration of occlusion was estimated in 18 patients as theinterval between the initial angiogram that had documenteda subtotal stenosis and the time of attempted dilation of thenow occluded coronary artery. In the four patients withouta previous angiogram (all of whom had the initial onset ofangina pectoris within 4 weeks before angiography), theduration of occlusion was estimated from the onset of symptoms until the time of angiography. Of the remaining twopatients, one had a known occlusion for 2 years; in theother, who had a previous dilation, angina had returned 2weeks before reevaluation. The duration of occlusion wasI week or less in 10 patients, I week to I month in 6 patients,
JACC Vol. 3, No.3March 1984:845-9
HOLMES ET AL.ANGIOPLASTY IN CORONARY OCCLUSION
847
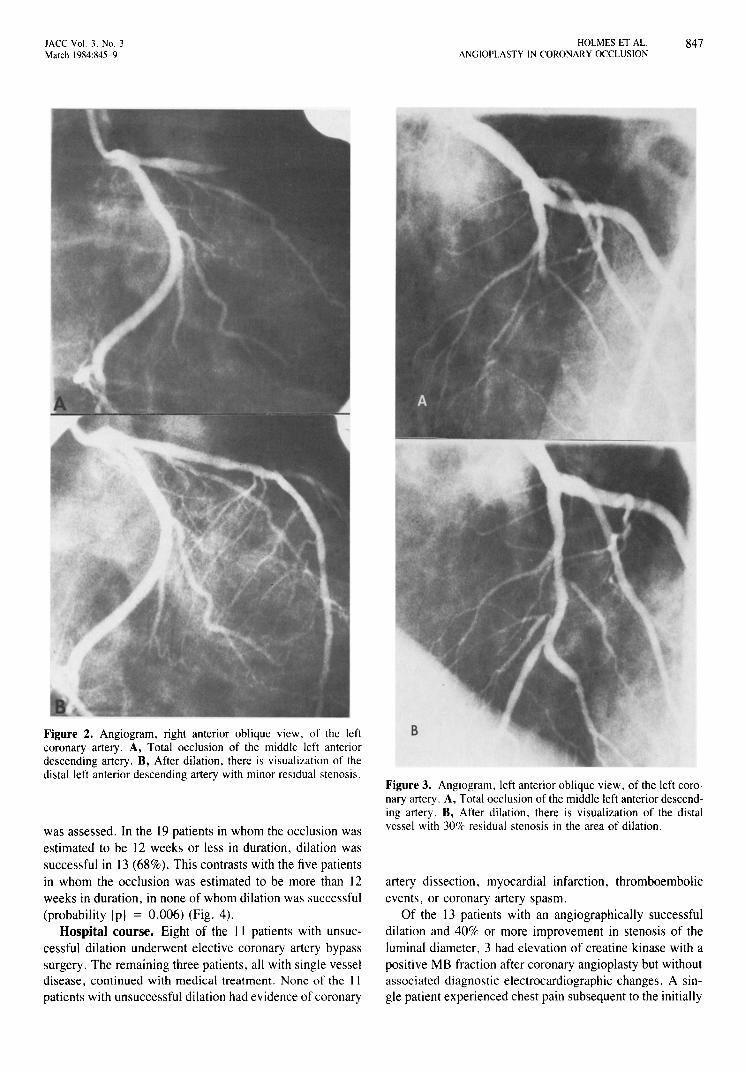
Figure 2. Angiogram, right anterior oblique view, of the leftcoronary artery. A, Total occlusion of the middle left anteriordescending artery. B, After dilation, there is visualization of thedistal left anterior descending artery with minor residual stenosis.
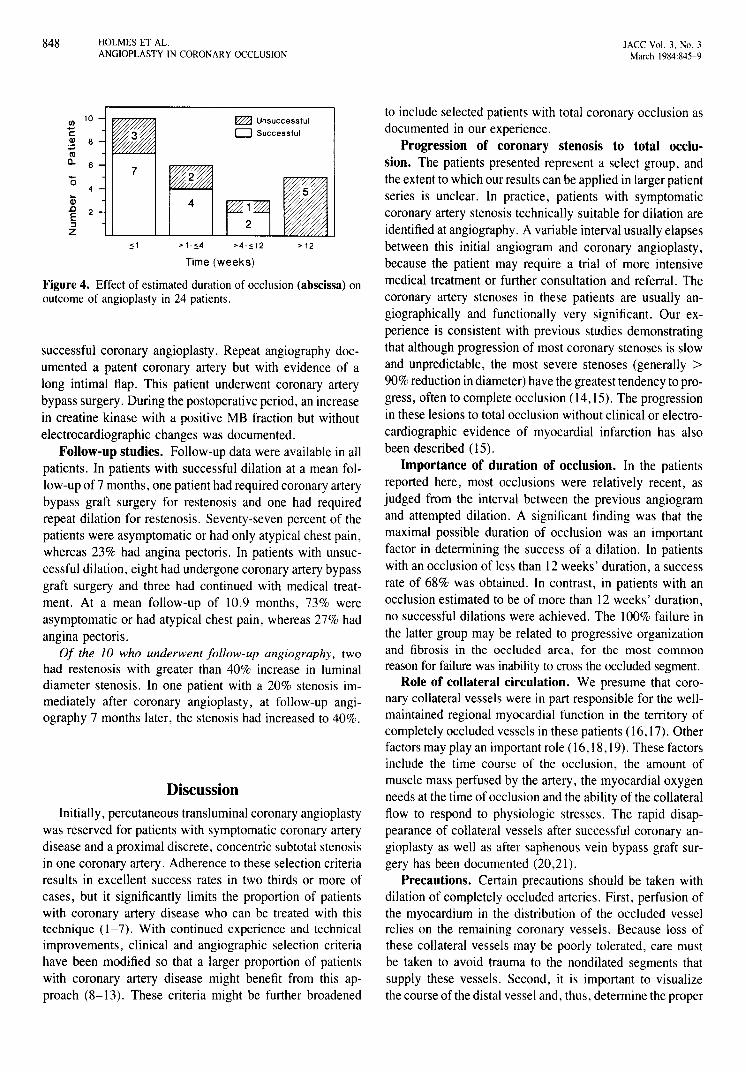
was assessed. In the 19 patients in whom the occlusion wasestimated to be 12 weeks or less in duration, dilation wassuccessful in 13 (68%). This contrasts with the five patientsin whom the occlusion was estimated to be more than 12weeks in duration, in none of whom dilation was successful(probability [p] = 0.006) (Fig. 4).
Hospital course. Eight of the 11 patients with unsuccessful dilation underwent elective coronary artery bypasssurgery, The remaining three patients, all with single vesseldisease, continued with medical treatment. None of the IIpatients with unsuccessful dilation had evidence of coronary
Figure 3. Angiogram, left anterior oblique view, of the left coronary artery. A, Total occlusion of the middle left anterior descending artery. B, After dilation, there is visualization of the distalvessel with 30% residual stenosis in the area of dilation.
artery dissection, myocardial infarction, thromboembolicevents, or coronary artery spasm,
Of the 13 patients with an angiographically successfuldilation and 40% or more improvement in stenosis of theluminal diameter, 3 had elevation of creatine kinase with apositive MB fraction after coronary angioplasty but withoutassociated diagnostic electrocardiographic changes, A single patient experienced chest pain subsequent to the initially
848 HOLMES ET AL.ANGIOPLASTY IN CORONARY OCCLUSION
JACC Vol. 3. No.3March 1984:845-9
Time (weeks)
Figure 4. Effect of estimated duration of occlusion (abscissa) onoutcome of angioplasty in 24 patients.
DiscussionInitially, percutaneous transluminal coronary angioplasty
was reserved for patients with symptomatic coronary arterydisease and a proximal discrete, concentric subtotal stenosisin one coronary artery. Adherence to these selection criteriaresults in excellent success rates in two thirds or more ofcases, but it significantly limits the proportion of patientswith coronary artery disease who can be treated with thistechnique (1-7). With continued experience and technicalimprovements, clinical and angiographic selection criteriahave been modified so that a larger proportion of patientswith coronary artery disease might benefit from this approach (8-13). These criteria might be further broadened
to include selected patients with total coronary occlusion asdocumented in our experience.
Progression of coronary stenosis to total occlusion. The patients presented represent a select group, andthe extent to which our results can be applied in larger patientseries is unclear. In practice, patients with symptomaticcoronary artery stenosis technically suitable for dilation areidentified at angiography. A variable interval usually elapsesbetween this initial angiogram and coronary angioplasty,because the patient may require a trial of more intensivemedical treatment or further consultation and referral. Thecoronary artery stenoses in these patients are usually angiographically and functionally very significant. Our experience is consistent with previous studies demonstratingthat although progression of most coronary stenoses is slowand unpredictable, the most severe stenoses (generally >90% reduction in diameter) have the greatest tendency to progress, often to complete occlusion (14,15). The progressionin these lesions to total occlusion without clinical or electrocardiographic evidence of myocardial infarction has alsobeen described (15).
Importance of duration of occlusion. In the patientsreported here, most occlusions were relatively recent, asjudged from the interval between the previous angiogramand attempted dilation. A significant finding was that themaximal possible duration of occlusion was an importantfactor in determining the success of a dilation. In patientswith an occlusion of less than 12 weeks' duration, a successrate of 68% was obtained. In contrast, in patients with anocclusion estimated to be of more than 12 weeks' duration,no successful dilations were achieved. The 100% failure inthe latter group may be related to progressive organizationand fibrosis in the occluded area, for the most commonreason for failure was inability to cross the occluded segment.
Role of collateral circulation. We presume that coronary collateral vessels were in part responsible for the wellmaintained regional myocardial function in the territory ofcompletely occluded vessels in these patients (16,17). Otherfactors may play an important role (16,18,19). These factorsinclude the time course of the occlusion, the amount ofmuscle mass perfused by the artery, the myocardial oxygenneeds at the time of occlusion and the ability of the collateralflow to respond to physiologic stresses. The rapid disappearance of collateral vessels after successful coronary angioplasty as well as after saphenous vein bypass graft surgery has been documented (20,21).
Precautions. Certain precautions should be taken withdilation of completely occluded arteries. First, perfusion ofthe myocardium in the distribution of the occluded vesselrelies on the remaining coronary vessels. Because loss ofthese collateral vessels may be poorly tolerated, care mustbe taken to avoid trauma to the nondilated segments thatsupply these vessels. Second, it is important to visualizethe course of the distal vessel and, thus, determine the proper
>12
~ Unsuccessful
o Successful
>4-';:12
4
>1-s4
7
,;:1
<fl 10
C~ 8COQ. 6
successful coronary angioplasty. Repeat angiography documented a patent coronary artery but with evidence of along intimal flap. This patient underwent coronary arterybypass surgery. During the postoperative period, an increasein creatine kinase with a positive MB fraction but withoutelectrocardiographic changes was documented.
Follow-up studies. Follow-up data were available in allpatients. In patients with successful dilation at a mean follow-up of 7 months, one patient had required coronary arterybypass graft surgery for restenosis and one had requiredrepeat dilation for restenosis. Seventy-seven percent of thepatients were asymptomatic or had only atypical chest pain,whereas 23% had angina pectoris. In patients with unsuccessful dilation, eight had undergone coronary artery bypassgraft surgery and three had continued with medical treatment. At a mean follOW-Up of 10.9 months, 73% wereasymptomatic or had atypical chest pain, whereas 27% hadangina pectoris.
Of the 10 who underwent follow-up angiography, twohad restenosis with greater than 40% increase in luminaldiameter stenosis. In one patient with a 20% stenosis immediately after coronary angioplasty, at fOllow-up angiography 7 months later, the stenosis had increased to 40%.

JACC Vol. 3. No.3March 1984:845-9
HOLMES ET AL.ANGIOPLASTY IN CORONARY OCCLUSION
849
route for the dilating catheter. This may be possible byreviewing films before the time of complete occlusion orby visualizing the distal vessel by way of collateral channels.
Clinical implications. Criteria for patient selection andrecommendations for coronary angioplasty continue to evolve.The patients reported here are a select group. In these patients, on the basis of our experience, total occlusion is notby itself a contraindication to coronary angioplasty. Successful dilation can be achieved in approximately two thirdsof selected patients with recent « 12 weeks) total occlusion.In our experience, this situation occurs most commonlywhen a subtotal lesion suitable for dilation progresses tototal occlusion in the interval between angiography and dilation. In these patients, if the interval is less than 12 weeks,dilation can be attempted with a reasonable chance of success and low likelihood of complications. The role of percutaneous transluminal coronary angioplasty without priorangiography in patients with the recent onset of unstableangina and a totally occluded artery (four patients in ourseries) requires further evaluation. For patients who have arecent onset of unstable angina that is refractory to medicalmanagement and who are scheduled for surgical revascularization immediately after angiography, dilation of thetechnically suitable coronary artery occlusions may be areasonable alternative.
ReferencesI. Griintzig A. Transluminal dilatation of coronary-artery stenosis (letter
to the editor). Lancet 1978; I :263.
2. Griintzig AR, Senning A, Siegenthaler WE. Nonoperative dilatationof coronary-artery stenosis: percutaneous transluminal coronary angioplasty. N Engl J Med 1979;30 1:61-8.
3. Vlietstra RE, Holmes DR Jr, Smith HC, Hartzler GO. Orszulak TA.Percutaneous transluminal coronary angioplasty: initial Mayo Clinicexperience. Mayo Clin Proc 1981;56:287-93.
4. Kent KM, Bentivoglio LG, Block PC, et al. NHLBI pcrcutaneoustransluminal coronary angioplasty (PTCA) registry: four years experience (abstr). Am J Cardiol 1982;42:904.
5. Kent KM, Bentivoglio LG, Block PC. et al. Percutaneous transluminalcoronary angioplasty: report from the registry of the National Heart,Lung, and Blood Institute. Am J Cardiol 1982:49:2011-20.
6. Cowley MJ, Vetrovec GW, Wolfgang Te. Efficacy of percutaneoustransluminal coronary angioplasty: technique. patient selection, sal-
utary results, limitations and complications. Am Heart J1981 ;101 :272-80.
7. Williams DO, Riley RS, Singh AK, Gewirtz H, Most AS. Evaluationof the role of coronary angioplasty in patients with unstable anginapectoris. Am Heart J 1981;102:1-9.
8. Stertzer SH, Wallsh E, Bruno MS. Evaluation oftransluminal coronaryangioplasty in left main coronary artery stenosis (abstr). Am J Cardiol1981 ;47:396.
9. Ford WB, Wholey MH, Zikria EA, Somadani SR, Sullivan ME.Percutaneous transluminal dilation of aortocoronary saphenous veinbypass grafts. Chest 1981;79:529-35.
10. Block PC, Palacios IF, Wholey MH, O'Toole 1. Percutaneous transluminal angioplasty of stenotic coronary artery bypass grafts (abstr).Circulation 1981 ;64(suppl IV):IV-I09.
II. Douglas JS Jr, Griintzig AR, King SB III, Hollman 1. Long-termresults of percutaneous transluminal angioplasty for aorto-coronarysaphenous vein graft stenosis (abstr). Circulation 1982;66(suppl 11):11124.
12. Hartzler GO, Rutherford BD, McConahay DR, McCallister SH. Simultaneous multiple lesion coronary angioplasty-a preferred therapyfor patients with multiple vessel disease (abstr). Circulation 1982;66(suppl11):11-5.
13. Stertzer S, Dorros G, Myler R, Cowley M, Williams D, Kent K.Complex transluminal angioplasty in multivessel coronary artery disease (abstr). Am J Cardiol 1982;49:904.
14. Gensini GG, Esente P. Kelly A. Natural history of coronary diseasein patients with and without coronary bypass graft surgery. Circulation1974;50(supplll):11-98-101.
15. Shub C. Vlietstra RE. Smith He. Fulton RE, Elveback LR. Theunpredictable progression of symptomatic coronary artery disease: aserial clinical-angiographic analysis. Mayo C1in Proc 1981 ;56: 155-60.
16. Frye RL, Gura GM, Chesebro JH, Ritman EL. Complete occlusionof the left main coronary artery and the importance of coronary collateral circulation. Mayo Clin Proc 1977;52:742-5.
17. Schwarz F, Schaper 1. Becker V, Kubler W, Flaming W. Coronarycollateral vessels: their significance for left ventricular histologic structure. Am J Cardiol 1982;49:291-5.
18. Kolibash AJ, Bush CA, Wepsic RA, Schroeder DP, Tetalman MR,Lewis RP. Coronary collateral vessels: spectrum of physiologic capabilities with respect to providing rest and stress myocardial perfusion, maintenance of left ventricular function and protection againstinfarction. Am J Cardiol 1982;50:230-8.
19. Khouri EM, Gregg DE, McGranahan GM Jr. Regression and reappearance of coronary collaterals. Am J Physiol 1971 :220:655-61.
20. Bourassa MG. Campeau L, Lesperance I. Regression and appearanceof coronary collaterals after aortocoronary bypass surgery. In: Kaltenbach M, Lichtlen P. Bakon R. Bussmann W-D, eds. CoronaryHeart Disease. Stuttgart: Georg Thieme Publishers, 1978:40-7.
21. Griintzig A. Pyle R. Goebel N. Schlumpf M. The fate of collateralsafter percutaneous trans luminal coronary angioplasty (PTCA) (abstr).Circulation 1980;62(suppl III):I1I-161.





























