Embed Size (px)
Citation preview

ANATOMY AND PHYSIOLOGY OF THE ABDOMINAL WALL
CARLOS E. CARRIQUIRY, MD
The abdominal wall is a multilayered, complex structure that is frequently operated on with reconstructive and cosmetic objectives. A better understanding of the surgical implications of its components is essential to improve techniques and results. Anatomic and physiological aspects pertinent to cosmetic and transverse rectus abdominis musculo-cutaneous (TRAM) flap donor site closure is reviewed both in the superficial and musculoaponeurotic layers. Anatomic elements are examined as components of a functional system rather than as isolated units. The superficial anatomy is described as related to cosmetic procedures. Several underlying components of the abdominal wall are reviewed. Current concepts on the subcutaneous fat and Scarpa's fascia are presented. At the musculoaponeurotic plane, the importance of the rectus sheath and linea alba as the dynamic center of the abdominal wall is underlined, and consequently, their importance in terms of TRAM flap closure. The transversus muscle as a circular compressor of the abdomen is discussed, as well as its potential use for better waist definition. Copyright �9 1996 by W.B. Saunders Company
KEY WORDS: abdominal wall anatomy, surgical anatomy, functional anatomy
Abdominal contour is the result of the structural and functional status of several anatomical layers that consti- tute the abdominal wall. The abdominal contents can also influence overall abdominal shape. This article will focus on the anatomic structures that can be surgically modified to improve abdominal shape. Both structural and func- tional aspects will be analyzed to obtain a better under- standing of the contribution each part can make to the overall result. Comprehensive anatomic descriptions of all the structures referred to is beyond the scope of this article. Subsequently, detail is reserved for specific points that are deemed particularly significant or that have not been adequately appreciated until now.
SURFACE ANATOMY
Before analyzing the different layers that make up the abdominal wall, attention must be given to the overall morphological appearance that results from these interre- lated layers. The ideal external configuration of the female abdomen would be difficult to establish in absolute terms. Additionally, most anatomy and surgical texts describe the surface anatomy of the muscular male. In the female, the general contour as well as the definition of the superficial landmarks differ from those in the male. Therefore, some basic features of the female must be taken into account when aesthetic remodeling is planned.
In the male, the costochondral margin and the upper diameter of the bony pelvis are grossly equivalent, so that from the front, the lateral limits of the abdomen are straight
From the Division of Plastic Surgery, School of Medicine, Universidad de la Republica, Montevideo, Uruguay.
Address reprint requests to Carlos E. Carriquiry, MD, 21 de Setiembre 2353, apt 201, Montevideo 11200, Uruguay.
Copyright �9 1996 by W.B. Saunders Company 1071-0949/96/0301-0001 $5.00/0
and the waist has little definition. The paramedian promi- nence of the rectus muscles bind the mild median depres- sion of the linea alba from xiphoid to umbilicus. The bulge of the recti is interrupted by a few transverse inscriptions. Just lateral to the rectus, there is another mild depression, the linea semilunaris, slightly concave medially and fading toward the pubis. It shows the transition between the flat muscles and the rectus sheath. The lower limit of the flat muscles at the inguinal ligament can be perceived as an oblique sulcus from the pubis to the anterosuperior iliac spine.
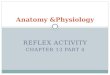
In the female, the transverse diameter of the pelvis is larger than that of the costochondral margin, and the waist becomes clearly defined as an important feature of the female trunk contour. The lesser muscular development and proportionally thicker subcutaneous layer tend to soften muscular reliefs. However, the aesthetically pleas- ing female abdomen does not look uniformly rounded or flat, but presents nuances of contour that suggest the underlying anatomy (Fig 1). The transverse inscriptions of the recti and digitations of the external oblique are nor- mally not apparent, and the transition between the abdo- men and the thigh at the inguinal region is smooth. The subcutaneous fat is normally thicker below and around the umbilicus and laterally overlaps the vertical prominence of the recti, originating a lyre-shaped relief 1 limited laterally by the semilunar lines and tapering toward the pubis. If this fat deposit becomes larger, a suprapubic fold is formed and becomes particularly conspicuous (and unpleasant to the patient) in the sitting position. 2
The umbilicus is a focal point in the abdominal surface anatomy. Alterations in its location must be avoided or, if necessary, very carefully planned. On a general frontal view, it is in the middle of a vertical line drawn from xiphoid to pubis. Practical relationships have been estab- lished with palpable osseous landmarks: the umbilicus is
2 Operative Techniques in Plastic and Reconstructive Surgery, Vol 3, No 1 (February), 1996: pp 2-6

Fig 1. (A) Nuances of light and shadow characteristic of the superficial configuration of the female abdomen, as adapted from Botticelli's "Birth of Venus." (B) The corresponding underlying anatomy: 1, the external oblique; 2, the transition between the flat muscles and the rectus abdominis (linea semilunaris); 3, the rectus abdominis; and 4, the linea alba. Subcutaneous fat deposits are shown as shaded/dotted areas.
located on a line joining the highest points of the iliac crests, about 6.3 cm above the line of the anterosuperior iliac spines and about 15 cm above the symphysis pubis. 3 A limited downward displacement of up to 2 or 3 cm, as performed in "mini" abdominoplasties is aesthetically acceptable. 1,2
Hair growth patterns in the trunk show gender differ- ences and become a significant secondary sexual character- istic in the pubic region. 4 Hair growth is generally less dense in the female and limited to the mons pubis. Its upper limit tends to be well defined, about 2 to 3 cm above the pubic bones. 2 Although this pubic triangle is just below the limits of the abdomen proper, it bears a strong aesthetic relationship to the latter, which should not be distorted by excessive tension when closing an abdominoplasty.
SUPERFICIAL PLANES
The skin, subcutaneous connective tissues, and adipose tissues constitute the superficial layer of the abdominal wall. The abdominal skin is rather thick (0.75 to 2 mm) as compared with other regions. The fibrous and elastic bundles of the dermis are arranged in patterns that result in relaxed tension lines. In the abdomen, they are oriented transversely and slightly concave upward. The elastic potential of abdominal skin is of paramount importance in planning remodeling procedures. It is subjected to changes related to aging, pregnancy, and changes in weight. Disrup- tion of the fibrous structure of the dermis can show as striae, which indicate poor elastic potential.
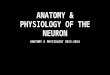
The subcutaneous fat layer is made up of fatty lobules contained within delicate fibrous trabecullae and lamellae. The amount of fatty tissue in the abdominal wall is large compared with other regions. It represents one of the main reserves of body fat. Its thickness and distribution strongly influence abdominal shape (Fig 2). There are areas within the abdomen where fat deposits tend to accumulate and may persist to a variable degree despite overall body weight loss. They show gender differences. In women, fat deposits tend to be more prominent around and below the umbilicus and following the iliac crests. In men, fat deposits tend to be thicker from the umbilicus toward the epigastrium.
Two distinct layers can be found within the subcutane- ous fat. 5,6 The superficial layer is composed of smaller lobules, encased in multiple perpendicular septa (Fig 2). The deep layer (Gallaudet's fascia) lobules are larger and lay within a looser connective framework. This arrange- ment gives the superficial layer a more compact texture. Although both layers can vary in thickness depending on multiple factors, the superficial layer has been found to be more consistent in thickness. 6
A connective sheet divides these two adipose layers. It is particularly distinct at the lower abdomen, where it is known as Scarpa's fascia. Although its existence has been questioned, 7 recent reappraisals 5,6 and systematic clinical observation confirm its existence as a consistent structure. Meticulous studies can show several microscopic superim- posed connective sheets making up this layer. Phylogeneti- cally, it can be traced to the panniculus carnosus found in loose-skinned mammals. The subcutaneous vascular net- work is most dense close to Scarpa's fascia. If sharp
ABDOMINAL WALL FUNCTIONAL ANATOMY 3

Fig 2. Two distinct layers of subcutaneous fatty tis- sue as observed in surgi- cal incision in the lower abdomen. The superficial layer is composed of tightly packed, smaller Iobules (s), as opposed to the loose lamellar con- formation of the deep layer or Gallaudet's fas- cia (d).
defatting is performed, it should not extensively disrupt this layer to avoid increased bleeding and possible isch- emia of the flap. s
The point of maximal attachment between these layers is variable. It is loose in the lower abdomen, where subcuta- neous tissues can be dissected off the rectus sheath and the external oblique with relative ease. As one proceeds to- ward the xiphoid, the attachments become firmer and render dissection more difficult. At the iliac crest and inguinal ligament, the fibrous framework of the subcutane- ous layer becomes more dense again and adheres firmly to the underlying structures. These attachments are espe- cially firm at the inguinal area constituting P6trequin's ligament as described by French anatomists.
The vessels supplying the superficial tissues can also be considered as elements attaching to the deep plane. Many must be severed during an abdominoplasty. At the start of the operation, when the low abdominal incision is made, the superficial inferior epigastric and branches of the superficial exterior pudendal and superficial circumflex iliac vessels are readily encountered as they run from their origin at the common femoral vessels into the plane of Scarpa's fascia. As dissection proceeds in the lower abdo- men, where attachments are looser, a few isolated musculo- cutaneous perforators are found. On approaching the umbilicus, perforators become larger and more numerous. They can be identified and coagulated before being sev- ered, lest they retract into the rectus sheath and demand tedious suture ligation. Laterally, perforators from the external oblique are encountered close to the limits of the standard dissection.
MUSCULOAPONEUROTIC PLANE
To properly manipulate the abdominal wall for cosmetic and reconstructive purposes, muscular and fascial struc- tures must be considered as components of a complex structural and functional system. Emphasis will be placed
on the analysis of some aspects of this musculoaponeurotic system, both from a structural and functional point of view.
The Rectus Abdominis Muscles and Shea ths
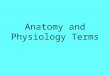
These muscles stretch as two paramedian muscular bands from costochondral margin to pubis, each one encased in a strong aponeurotic sheath. A solid connection between both sheaths is established at the linea alba, a median fibrous raphe that is slightly wider in its upper half. The structure of the linea alba and the sheaths is complex. The latter are composed of the aponeuroses of the three flat muscles of the abdomen. Above the linea semicircularis, the internal oblique (IO) aponeurosis splits into two layers: one which fuses with the external oblique (EO) aponeuro- sis as it passes in front of the rectus, the other fuses with the transversus abdominis (TA) aponeurosis to form the poste- rior layer of the sheath. Below the linea semicularis, the three join to pass in front of the rectus, so the posterior layer of the sheath is composed of only the fascia transver- salis. It must be noted that the EO does not fuse with the IO at the lateral border of the sheath but more medially, so that in its lateral half the anterior sheath consists of two layers (Fig 3); this is particularly accentuated in the lower abdomen and is most relevant in terms of TRAM flap donor site closure. In fact, when a TRAM flap is elevated, the lateral remnant of the anterior sheath must be closed in two layers. The deeper one must not be overlooked to prevent a weak reconstruction of the abdominal wall. 9,1~
Decussations and continuities in tendinous fibers from aponeuroses of the flat muscles are established at the linea alba creating a plywood arrangement. Criss-crossing fibers from the deep aspect of the EO aponeurosis are continuous with those from the superficial aspect of the contralateral IO. 11,12 Multiple digastric arrangements are thus created 9,n so that the sheaths and linea alba can be compared with the central tendon of the diaphragm. 13
4. CARLOS E. CARRIQUIRY

Fig 3. Transverse section of anterior abdominal wall in anatomic specimen, showing: rectus abdomi- nis muscle and sheath (R), linea alba (L), exter- nal oblique (EO), and in- ternal oblique (IO) mus- cles. A clamp holds the external oblique aponeu- rosis, illustrating that the fusion with the internal oblique does not take place at the lateral border of the sheath but more medially, at its middle third.
From a dynamic point of view, this anatomic arrange- ment means that strong centrifugal forces of up to 40 pounds with a predominant transverse vector 14 act on these central fibrous structures (Fig 4). If they are vertically interrupted, as in rectus abdominis flap elevation, a strong and meticulous reconstruction will be needed to counter the centrifugal pull on the margins of the defect. For the same dynamic reasons, strong sutures are needed
Fig 4. The forces applied on the rectus sheath and linea alba by the external oblique (eo), internal oblique (io), and transver- sus abdominis (ta) muscles are shown schematically on one side of the diagram. The resultant force, with a transverse direction, is shown on the other side.
to approximate medially both sheaths for contour correc- tion.
On the other hand, the rectus abdominis muscles seem to be less important than their sheaths as support elements of the central abdominal wall. McVay 14 considers the TA, which is the main component of the posterior sheath above the linea semicircularis, as the "most important bulwark against the development of an incisional hernia," whereas the rectus "can be sectioned within its sheath with impu- nity" as long as the latter is properly closed. Basmajian and De Luca, is based on electromyographic studies, also con- sider rectus activity of little importance with regard to hernia prevention. On the contrary, it is the basic role of the sheath. Accordingly, preservation of a strip of rectus muscle for a safer closure of the TRAM flap donor defect would not make a substantial contribution. Additionally, this muscle strip usually becomes denervated because the motor endplates are removed with the central portion of the muscle, 16 and subsequent atrophies.
Rectus function is mainly related to trunk flexion against resistance, is If appropriate abdominal wall reconstruction has been performed after TRAM flap elevation, little change is perceived by the patients with regard to these movements. Specific tests, however, can show quantitative functional impairment. 17
The Flat Muscles
The three flat muscles that constitute the anterolateral abdominal wall are oriented as to form a grid with two oblique components (the EO and IO) and a transverse one (the TA). This results in a significant strengthening of the abdominal wall. It also allows, within certain limits, expansion of the abdominal contents without great in- crease in abdominal wall tension. This is accomplished by angles of decussation between fibers of different layers and separation of parallel fibers in the same layer. TM
A comparative study of the flat muscles shows some anatomic differences that can have surgical implications.
ABDOMINAL WALL FUNCTIONAL ANATOMY 5

The three flat muscles reach the rectus sheath medially, but the more posterior fibers of the EO and IO course from the lower ribs to the iliac crest wi thout reaching the rectus sheath. Almost all of the TA fibers fuse with the rectus sheath. The EO and IO fibers approach the rectus sheath obliquely, whereas the TA does so perpendicularly. At the posterior abdominal wall, the IO and the TA fuse with another aponeurotic structure, the lumbodorsal fascia. This in turn inserts on the spinous and transverse lumbar vertebral processes. Thus, the fibers of the middle third of both TA muscles constitute a continuous musculoaponeu- rotic girdle that circumscribes the abdomen in a transverse plane. This anatomic arrangement gives the TA muscles a clear mechanical advantage as circular compressors of the abdominal wall, which is reinforced by the fact that they originate from the inner surface of the costal cage. 13 The projection of the umbilicus and the waistline are included in this middle segment of the TA.
All these anatomic factors point to the TA potential in terms of abdominal contour remodeling, particularly in waist definition. Plication of the anterior rectus sheaths has proven useful in most cases of abdominal muscular laxity. However, some feel it does not achieve good waist defini- tion and epigastric fullness correction. 19 This may be caused by the fact that it only tightens the EO and part of the IO, but has little or no effect on the TA. Plication of both the anterior and posterior walls of the rectus sheath, and thus t ightening the TA, has been reported. 2~ However, it has the relative disadvantage of requiring incision of the anterior rectus sheath. In fact, the main obstacle to taking advantage of the TA is that it is not easily accessible. Endoscopic techniques may help to reach the TA more directly.
Spinal stability is affected by the functional status of the abdominal muscles. This is attributed to their effect on intraabdominal pressure. TM Recently, another mechanism has been proposed. 21 It is based on the fact that the lumbodorsal fascia is firmly attached to the lumbar spi- nous processes, the ribs, and the iliac crest. Thus, forward flexion of the spine (increase in its vertical diameter) should result in compensatory narrowing of the fascia (decrease in transverse diameter). Actually, this narrowing does not occur as expected, probably because of the lateral pull that the IO and TA muscles exert on the fascia. In this way, these muscles convey a certain amoun t of longitudi- nal tension to the spine by means of their lateral traction on the lumbodorsal fascia.
Concern about spinal stability and lower back pain ensuing remodelling by plication of the abdominal wall or TRAM flap harvesting has been expressed, but has not been confirmed by postoperative results. 22 In fact, there are reports of back pain alleviation following these proce-
dures. 17,23 Increased tension on the lumbodorsal fascia by the medial mobilization of the flat muscles effected by these procedures could be the explanation for this symp- tomatic relief. 23
REFERENCES
1. Bozola AR, Psillakis JM: Abdominoplasty: A new concept and classification for treatment. Plast Reconstr Surg 82:291-293, 1988
2. Elbaz JS, Flageul G: Liposuction et chirurgie plastique de l'abdomen. Paris, France, Masson, 1990
3. Dubou R, Ousterhout DK: Placement of the umbilicus in an abdomi- noplasty. Plast Reconstr Surg 61:291-293, 1978
4. Mann C: Modigliani. London, United Kingdom, Thames & Hudson, 1980, pp 135-159
5. Pearl RM, Johnson D: The vascular supply to the skin: An anatomical and physiological reappraisal. Part I. Ann Plast Surg 2:99-105, 1983
6. Markman B, Barton FE: Anatomy of the subcutaneous tissue of the trunk and lower extremity. Plast Reconstr Surg 80:248-254, 1987
7. Tobin CE, Benjamin JA: Anatomic and clinical re-evaluation of Camper's, Scarpa's and Colles" fasciae. Surg Gynecol Obstet 88:545- 559, 1949
8. Grotting JC, Carriquiry C, Vasconez LO: Abdomen, in Jurkiewicz MJ, Krizek TJ, Mathes SJ, Ariyan S (eds): Plastic Surgery. Principles and Practice, vol 2. St Louis, MO, Mosby, 1990, pp 1139-1167
9. Drever JM, Hodson-Walker N: Closure of the donor defect for breast reconstruction with rectus abdominis myocutaneous flaps. Plast Reconstr Surg 76:558-562, 1985
10. Kroll SS, Marchi M: Comparison of strategies for preventing abdomi- nal-wall weakness after TRAM flap breast reconstruction. Plast Reconstr Surg 89:1045-1051, 1992
11. Askar OM: Surgical anatomy of the aponeurotic expansions of the abdominal wall. Ann R Coll Surg Eng159:313-321, 1977
12. Rizk NK: A new description of the abdominal wall. Anat Rec 184:515, 1976
13. Walmsley R: The sheath of the rectus abdominis. J Anat 71:404-414, 1936
14. McVay ChB: Anson and McVay's Surgical Anatomy (ed 6). Philadel- phia, PA, Saunders, 1984, pp 510-515
15. Basmajian JV, De Luca C: Muscles Alive (ed 5). Baltimore, MD, Williams & Wilkins, 1985, pp 389-398
16. Duchateau J, Declety A, Lejour M: Innervation of the rectus abdomi- nis muscle: Implications for rectus flaps. Plast Reconstr Surg 82:223- 227, 1988
17. Lejour MD, Dome M: Abdominal wall function after rectus abdominis transfer. Plast Reconstr Surg 87:1054-1068, 1991
18. Hollinshead WH, Rose C: Textbook of Anatomy (ed 4). Philadelphia, PA, Harper & Row, 1985, pp 580-591
19. Psillakis JM: Plastic surgery of the abdomen with improvement in the body contour. Clin Plast Surg 2:465-477, 1984
20. Pina DP de: Aesthetic abdominal deformities: A personal approach to the posterior rectus sheath and rectus muscles. Plast Reconstr Surg 75:660-666, 1985
21. Gracov etsky S, Farfan H, Helleur C: The abdominal mechanism. Spine 10:317-324,1985
22. Hartrampf CR, Bennett GK: Autogenous tissue reconstruction in the mastectomy patient: A critical review of 300 patients. Ann Surg 205:508-518, 1987
23. Toranto IR: Resolution of back pain with wide abdominal rectus plication abdominoplasty. Plast Reconstr Surg 81:777-779, 1988
6 CARLOS E. CARRIQUIRY