Embed Size (px)
Citation preview

KNEE
Anatomic anterior cruciate ligament (ACL) reconstruction:a global perspective. Part 1
K. K. Middleton • T. Hamilton • J. J. Irrgang •
J. Karlsson • C. D. Harner • F. H. Fu
Received: 30 September 2013 / Accepted: 10 January 2014
� Springer-Verlag Berlin Heidelberg 2014
Abstract
Purpose In August 2011, orthopaedic surgeons from
more than 20 countries attended a summit on anatomic
anterior cruciate ligament (ACL) reconstruction. The
summit offered a unique opportunity to discuss current
concepts, approaches, and techniques in the field of ACL
reconstruction among leading surgeons in the field.
Methods Five panels (with 36 panellists) were conducted
on key issues in ACL surgery: anatomic ACL reconstruc-
tion, rehabilitation and return to activity following ana-
tomic ACL reconstruction, failure after ACL
reconstruction, revision anatomic ACL reconstruction, and
partial ACL injuries and ACL augmentation. Panellists’
responses were secondarily collected using an online
survey.
Results Thirty-six panellists (35 surgeons and 1 physical
therapist) sat on at least one panel. Of the 35 surgeons
surveyed, 22 reported performing ‘‘anatomic’’ ACL
reconstructions. The preferred graft choice was hamstring
tendon autograft (53.1 %) followed by bone-patellar ten-
don-bone autograft (22.8 %), allograft (13.5 %), and
quadriceps tendon autograft (10.6 %). Patients generally
returned to play after an average of 6 months, with return
to full competition after an average of 8 months. ACL
reconstruction ‘‘failure’’ was defined by 12 surgeons as
instability and pathological laxity on examination, a need
for revision, and/or evidence of tear on magnetic resonance
imaging. The average percentage of patients meeting the
criteria for ‘‘failure’’ was 8.2 %.
Conclusions These data summarize the results of five
panels on anatomic ACL reconstruction. The most popular
graft choice among surgeons for primary ACL recon-
structions is hamstring tendon autograft, with allograft
being used most frequently employed in revision cases.
Nearly half of the surgeons surveyed performed both sin-
gle- and double-bundle ACL reconstructions depending on
certain criteria. Regardless of the technique regularly
employed, there was unanimous support among surgeons
for the use of ‘‘anatomic’’ reconstructions using bony and
soft tissue remnant landmarks.
Level of evidence V.
Keywords Anatomic � ACL reconstruction � Global
perspectives � Summit
Introduction
Anterior cruciate ligament (ACL) injuries are among the
most common knee ligament injuries in the world. It fol-
lows that ACL reconstruction (ACL-R) is one of the most
commonly performed orthopaedic surgeries [10]. The ACL
is comprised of two functional bundles, the anteromedial
(AM) and posterolateral (PL) bundles. Together, they
synergistically provide anterior–posterior and rotational
stability to the knee. Until recently, methods to reconstruct
the ACL focused on using a single graft. Such techniques
have been demonstrated to have high success rates despite
30 % of patients experiencing persistent knee pain and/or
instability [9]. Double-bundle ACL reconstruction methods
K. K. Middleton � T. Hamilton � J. J. Irrgang �C. D. Harner � F. H. Fu (&)
Department of Orthopaedic Surgery, University of Pittsburgh
School of Medicine, Kaufman Medical Building, Suite 1011,
3941 Fifth Avenue, Pittsburgh, PA 15203, USA
e-mail: [email protected]
J. Karlsson
Department of Orthopaedics, Gotenborg University, Goteborg,
Sweden
123
Knee Surg Sports Traumatol Arthrosc
DOI 10.1007/s00167-014-2846-3

were developed to reconstruct both the AM and PL bun-
dles. Some studies have demonstrated superior outcomes
and improved rotational stability with double-bundle
reconstruction compared with single-bundle reconstruc-
tions. However, as of late, there have been reports of no
difference in outcome measures between the two tech-
niques [3, 26], particularly when the reconstruction is
‘‘anatomic’’. Anatomic ACL-R is defined as functional
restoration of the ACL to its native dimensions, collage
orientation, and insertion sites [29]. Anatomic ACL-R
(regardless of technique) has been shown to yield better
clinical and biomechanical results compared with non-
anatomic reconstruction [12].
The evolution of anatomic ACL-R has occurred globally
due to the dissemination of scientific evidence as well as
open communication between surgeons across the world.
In August 2011, nearly 200 orthopaedic surgeons, sports
medicine physicians, and experts in the field of rehabili-
tation representing over twenty countries convened in
Pittsburgh, Pennsylvania, to discuss current concepts in
anatomic ACL reconstructive surgery. Of those in atten-
dance, 36 experts in the field of ACL surgery presented on
panels to discuss current concepts, techniques, advance-
ments, and future directions in the field of anatomic ACL-
R. The purpose of this descriptive study was to present the
responses to panel questions, thus providing a global per-
spective on the current approaches used around the world.
Materials and methods
Panels and panellist profile
Five panels were conducted on the topics of anatomic
ACL-R, rehabilitation and return to activity following
anatomic ACL-R, failure after ACL-R, revision anatomic
ACL-R, and partial ACL injuries and ACL augmentation.
Thirty-four orthopaedic surgeons with extensive expe-
rience in orthopaedic sports medicine and ACL-R partici-
pated in at least one of the five panels. Among the 34
panellists, fifteen represented the USA, three each repre-
sented Brazil and Japan, two each represented Germany
and Australia, and the following countries were each rep-
resented by one surgeon: China, France, Finland, Italy, the
Netherlands, South Africa, South Korea, Sweden, and the
United Arab Emirates. On average, the panellists have been
in practice for 22 ± 10.1 years (range 5–42 years). The
mean total number of ACL reconstructions performed over
the surgeon’s career was 2,143.9 ± 1,857.4 (range
100–7,800 surgeries).
Panellists were asked to prepare a 6-min presentation
answering questions pertaining to practice setting, patient
profile, surgical considerations, current techniques, and
clinical outcomes. For each topic, their responses to the
questions were presented followed by a 30-min question–
answer session. During the question–answer discussion, the
panellists’ responses were tabulated and results were
summarized. Following the summit, responses were sec-
ondarily collected and recorded using an online survey [28]
for final analysis. See ‘‘Appendix’’ for survey questions.
Patient profile
The majority of patients undergoing ACL-R were female
(57 %) and between 19 and 24 years old (Fig. 1). This age
group comprised 30.5 ± 10.6 % of the patient population.
The age group between 25 and 34 years made up
27.9 ± 11 % of the population, followed by the 14–18-
year-old age group (18.2 ± 7.9 %) and the 35–50-year-old
age group (16.4 ± 7.1 %). Less than 8 % of the patients
undergoing ACL-R were under 14 years of age
(2.5 ± 3.4 %) or over 50 years of age (4.6 ± 3.7 %).
Level of sports participation varied among patients who
underwent primary ACL-R: 44.9 ± 19.5 % were recrea-
tional athletes, 20.7 ± 12.3 % were college athletes,
19.8 ± 11.5 % were high school athletes, and 5.2 ± 4.3 %
were professional athletes. Approximately 9 % of the
patients did not participate in athletics at any of the above-
mentioned levels (Fig. 2).
Results
Panel I: Anatomic ACL reconstruction
Criteria for single-bundle ACL-R versus double-bundle
ACL-R
All panellists agreed upon the indications for surgical
management of a torn ACL, whether single or double
bundle. These include a history of trauma or injury
(contact vs. non-contact) resulting from a plant-twist
mechanism; subjective complaints of instability; clinical
examination findings of laxity as evidenced by a positive
pivot shift, Lachman, and or anterior drawer; and con-
firmed disruption of the ACL on magnetic resonance
(MR) imaging.
Four surgeons (13.7 %) reported that they performed
single-bundle reconstructions for ‘‘all ACL tears’’ unless
the patient requested a ‘‘double-bundle’’ reconstruction
or more ‘‘rotational control’’ with surgery, the patient
was a professional athlete requesting a ‘‘double-bundle’’
procedure, or if the patient had a large body habitus
(Fig. 3). One surgeon who performed ‘‘mostly double-
bundle’’ reconstructions elected to perform single-bundle
procedures in patients who were non-athletes, in
Knee Surg Sports Traumatol Arthrosc
123

augmentation cases, or if the patient already had evidence
of osteoarthritis.
Fourteen panellists (48.3 %) performed both SB and DB
techniques depending on certain criteria (defined in
Table 1). For one surgeon in particular, the graft choice
dictated his reconstruction technique. For instance, SB
reconstructions were performed whenever a BTB graft was
used, and DB reconstructions were always performed with
hamstring tendons. Other surgeons used criteria that
included graft size, insertion site size and notch size, knee
size and/or body habitus, level of activity prior to surgery,
amount of laxity during the physical examination, and
subjective complaints of rotatory instability.
Preferred technique
Remnant preservation and intraoperative measure-
ments Preservation of the tibial remnant during ACL
reconstruction is believed to help restore the proprioceptive
function of the ACL [1], accelerate revascularization and
ligamentization of the intra-articular graft [7, 23], and
enhance the biological environment for graft healing within
the tibial tunnel [32]. However, some studies have shown
no such benefit [23] and encourage continued studies
evaluating the clinical efficacy of remnant preservation
techniques. Of the 29 surgeons on the panel, 21 (72.4 %)
mentioned preserving ACL remnants with the hopes of
Fig. 1 Patient age distribution
Fig. 2 Patient level of sports
participation
Fig. 3 Panellists’ technique:
single bundle or double bundle.
SB single bundle, DB double
bundle
Knee Surg Sports Traumatol Arthrosc
123

providing near or complete restoration of the native func-
tion of the ACL and thus improving surgical outcome.
Twenty-three of 29 surgeons (88.5 %) obtained various
measurements during arthroscopy. Time is an important
consideration for those not commonly using intraoperative
measurements. Of those surgeons who obtained measure-
ments during surgery, five (17.2 %) measure the intra-
articular size of the ACL at its mid-portion. Thirteen
(44.8 %) measure the size of the ACL insertion sites, and
nine (31 %) measure intercondylar notch width. Surgeons
employing arthroscopic measuring devices during surgery
believe that measurements help guide surgical decision-
making and ensure adherence to the anatomic concept.
Three surgeons, in particular, have published articles
demonstrating the process and utilization of intraoperative
measurements [8, 25, 29]. Interestingly, nearly half of the
panellists (13 of 29) also measure tunnel aperture size prior
to passing the graft. Measurement of the tibial tunnel
aperture size is more difficult for those who utilize remnant
preservation techniques. Though soft tissue can obscure the
boundaries of the tunnel, these measurements were said to
help confirm desired tunnel size.
Tunnel placement, femoral drilling, and documentation of
location Anatomic ACL reconstruction is defined as the
functional restoration of the ACL to its native dimensions,
collagen orientation, and insertion sites [29]. Tunnel
placement is deemed ‘‘anatomic’’ if the tunnel dimensions
lie within the native insertion site. For the purposes of this
study, tunnel location was considered anatomic if surgeons
specifically reported ‘‘anatomic’’ placement, one that was
‘‘in the centre of the footprint’’, or a single tunnel located at
the junction ‘‘between the AM and PL insertion sites’’.
Twenty-six of 29 surgeons (89.7 %) reported placing
their femoral tunnels anatomically. Several also mentioned
that if they had to err with respect to femoral tunnel
placement, they would do so towards the AM insertion site.
Many specified that they used ACL remnants, bony land-
marks such as the lateral bicondylar and lateral bifurcate
ridges, and/or estimation of notch wall height (placing the
tunnels ‘‘lower on the lateral side of the notch’’) to help
determine anatomic placement. ACL insertion sites are
depicted in Fig. 4. The three surgeons who did not
explicitly indicate ‘‘anatomic’’ placement described their
femoral tunnel location as such:
• Below the lateral intercondylar ridge, centred posteri-
orly to the middle of the lateral femoral condyle wall.
• Eight millimetres vertical above the tibial plateau in the
mid-portion of the notch with the knee in 90� of flexion
and back in the notch, halfway to the posterior over-
the-top position.
• Seven to eight millimetres above the inferior articular
cartilage margin of the intercondylar notch with the
knee in 90� of flexion, slightly deep in the notch to the
bifurcate ridge.
Nearly 70 % of the surgeons utilize the anterior–medial
(AM) portal to drill the femoral tunnel. Five surgeons
(21.7 %) used both the AM portal technique and the tran-
stibial technique to drill the femoral tunnel depending on
whether or not anatomic tunnel placement can be achieved
with the transtibial technique. No surgeon used only the
transtibial drilling technique.
On the tibial side, 25 of 29 surgeons (86.2 %) reported
placing their tibial tunnels anatomically, that is, in the
native footprint. Additionally, five panellists (17.2 %)
reported using bony and soft tissue landmarks to help guide
Table 1 Criteria for single- and double-bundle ACL reconstructions
based on surgeon responses
Single bundle Double bundle
Graft choice: Bone-tendon-bone Graft choice: Hamstring
Normal history and physical
examination findings for an
ACL rupture with AP
translation being the primary
problem
Normal history and physical
examination findings for an
ACL rupture in addition to the
rotatory component being more
dominant problem than AP
translation
Small knee, recreational athlete,
additional procedures required
(e.g. meniscal surgery),
skeletally immature patient
Large knee, professional athlete,
high-grade pivot shift on
physical examination, patient
request
Open physes Big body habitus, those who non-
specifically request or require
more rotatory stability
Insertion site length less than
14 mm, notch width less than
12 mm. Criteria based on the
need of insertion site coverage
and technical feasibility given
anatomic constraints
Insertion sites larger than 18 mm
in length. Either a single- or
double-bundle procedure can
be performed for insertion sites
between 14 and 18 mm in
length
Grade II pivot shift on
examination, smaller insertion
sites, small hamstring grafts
Grade III pivot shift, tibial
insertion greater than 16 mm in
length, femoral insertion site
greater than 18 mm in length,
larger hamstring grafts (PL
bundle graft must be 5.5 mm in
diameter or larger)
Older patients, non-high-
performance athletes
Younger patients, high-
performance athletes
ACL insertion site less than
14 mm in length
ACL insertion site larger than
14 mm in length
Small graft size Subjective complaints of
rotational instability, relatively
high athletic demand
Small knee, thin hamstring
tendons, non-athlete, or
recreational athlete
Large knee, high-level athlete,
athletes involved in pivoting
sports, large hamstring tendons
Criteria table based on individual surgeon responses. ‘‘Insertion site’’
is referring to the tibial insertion site unless specified
Knee Surg Sports Traumatol Arthrosc
123

tunnel placement, including the medial tibial eminence,
posterior border of the lateral meniscus, and cartilage of the
medial tibial plateau. The four surgeons who did not spe-
cifically report ‘‘anatomic’’ placement described placing
their tibial tunnels using the following criteria:
• Five to six millimetres anterior to the posterior cruciate
ligament (posterior placement).
• Tunnel position is based on notch size, so as not to
impinge the graft.
• Posterior edge of the anterior horn of the lateral
meniscus.
As with drilling the femoral tunnels, accurate tibial
tunnel placement is not without error. One surgeon men-
tioned that he places his single tunnel in the ‘‘central region
of tibial footprint’’, but that he prefers to ‘‘err posteriorly
rather than anteriorly to avoid impingement’’.
A variety of systems are used to confirm and document
tunnel position intraoperatively, including pictures and
video, radiography/fluoroscopy, navigation, and measure-
ments (Fig. 5). Post-operative determination of tunnel
position can be challenging; however, it serves as a useful
metric to help guide surgical technique, and it also provides
a simple, radiographic measure for objective outcome
evaluation. Five surgeons (17.2 %) used magnetic reso-
nance (MR) imaging, and eight (27.6 %) used computed
tomography (CT) scans after primary reconstructions to
document tunnel location. Three surgeons did not obtain
any radiographic studies to verify tunnel location. Illing-
worth et al. [13] demonstrated that flexion weight-bearing
posterior–anterior radiographs and sagittal magnetic reso-
nance imaging (MRI) can aid in the evaluation of femoral
tunnel position after ACL reconstruction using femoral
tunnel and inclination angles. CT scans are not routinely
performed post-operatively unless there is a clear indica-
tion. To minimize risks associated with radiation, clinical
indications for CT scans (particularly three-dimensional
reconstructions) following ACL surgery include reinjury
and pre-operative planning if revision surgery is necessary
[30].
Graft choice, size, and fixation methods varied between
surgeons. The major graft choices for ACL reconstruction
have evolved over the past decade, with allografts being
prohibited in many countries. Patella tendon autografts
were once the standard of care for all ACL reconstructions.
Now, hamstring autografts, quadriceps tendon autografts,
and Achilles and patella tendon allografts with and without
bone blocks are becoming more popular. Consistent with
these trends, hamstring tendon autografts were used 53 %
of the time, followed by bone-patellar tendon-bone auto-
grafts 23 % of the time (Fig. 6). Allografts are being used
13 % of the time, and quadriceps tendon autograft recon-
structions are being performed 11 % of the time. Though a
variety of graft choices are being used, each of the 29
Fig. 4 Femoral (A) and tibial
(B) ACL insertion sites. Black
line demarcates lateral
intercondylar ridge. Asterisk:
approximate centre of the AM
and PL insertion sites. Of note,
ACL insertion site anatomy and
size vary from individual to
individual
Fig. 5 Documentation of
tunnel location following
primary ACL-R. Surgeons
could have used more than one
method to document tunnel
location. Fluoro fluoroscopy,
XR X-ray, MRI magnetic
resonance imaging, CT
computed tomography
Knee Surg Sports Traumatol Arthrosc
123

panellists clearly has a preferred graft choice. Three sur-
geons use only one graft type (two use only bone-patellar
tendon-bone (BTB) autografts, and only one surgeon uses
hamstring autografts). Nine surgeons use the same graft in
over 90 % of patients, with seven preferring hamstring, one
preferring BTB, and one preferring quadriceps tendon
autografts. Five surgeons use the same graft in 75–85 % of
cases, with four preferring hamstring tendon autografts and
one using quadriceps tendon autografts 80 % of the time.
The remaining surgeons used multiple grafts, but still had a
predominant graft type.
The median graft size for single-bundle reconstructions
was 8.0 mm in diameter (ranging from 6 to 10 mm;
Fig. 7), which is important given the findings of recent
clinical studies suggesting that graft size can predict ACL
failure [18, 24]. Though grafts 8.0 mm and larger are
recommended based on the above studies, one can argue
that there is no ‘‘ideal’’ graft size, only an ‘‘average’’, since
graft size varies depending on the size of the native ACL
insertion site size and the patients’ needs. Three surgeons
indicated that they base their graft size on the native
insertion site size and that the goal of ACL-R is to
‘‘maximally occupy the native ACL footprint’’.
Graft fixation is variable and depends on graft type,
femoral versus tibial tunnel, and surgeon preference. For
graft fixation in the femoral tunnel, suspensory fixation was
the primary method (39 %) followed by interference
screws (bioabsorbable 21 %; metal 3 %). Five of 29 sur-
geons (18 %) varied their fixation method depending on
graft type. An interference screw was mostly used for BTB
reconstructions, and a suspensory device or transfix was
used for hamstring reconstructions. The most commonly
used fixation device on the tibial side was a bioabsorbable
screw. Fifteen of 29 surgeons (51.7 %) preferred this
method. Four surgeons (13.8 %) used multiple methods
depending on the type of graft and skeletal maturity of the
patient. For instance, one surgeon preferred use of a bio-
absorbable interference screw for hamstring grafts and used
a metal interference screw for all BTB grafts; another
preferred suture mini-discs for hamstring grafts and
Fig. 6 Primary ACL-R graft
choice. BTB, bone-patellar
tendon bone, HS hamstrings,
Quad quadriceps tendon
Fig. 7 Distribution of typical
single-bundle graft sizes. The
type of hamstring graft
(quadruple semitendinosus vs.
semitendinosus and gracilis)
utilized was not specified
Knee Surg Sports Traumatol Arthrosc
123

bioabsorbable interference screws for BTB grafts. For
patients with open physes, pneumatic staples were used by
one surgeon. The remaining ten surgeons used metal
interference screws, peek screws, staples, suture mini-
discs, a fixation post, or two methods combined to further
ensure stable fixation (e.g. use of a bioabsorbable inter-
ference screw and staple, or a bioabsorbable interference
screw with a spike and washer).
Surgical outcomes
A large majority of panellists reported closely following
their patients after surgery. Though follow-up protocols
varied between surgeons, the average number of post-
operative visits during the first 12 months was 5.0 ± 1.2.
Fourteen of 29 surgeons (48.3 %) re-examine their patients
within one week of surgery, with many surgeons requiring
that patients see them at least three times during the first
year. Fifteen surgeons (51.7 %) continued following their
patients annually.
With respect to evaluating clinical outcomes, all 29
surgeons reported using ROM during physical examination
as an assessment tool. Twenty-six of 29 surgeons (89.7 %)
also used manual and/or instrumented assessment of laxity
to evaluate clinical outcomes. Many surgeons also used
imaging to assess clinical outcomes. Twenty-five surgeons
(86.2 %) consistently used post-operative radiographs, nine
(31 %) occasionally used magnetic resonance (MR)
imaging, and eight (27.6 %) occasionally used CT scans.
Additional methods used for outcome evaluation included
ultrasound when needed, functional hop tests, and robotic
knee testing. Twenty-six of 29 surgeons (89.7 %) consid-
ered patient-reported outcome measures; however, these
were never the sole determining factor in assessing surgical
outcome.
Eighty-seven perscent of all pooled surgical cases were
complication free. In other words, the complication rate for
all reported surgeries was 13 %. The majority of compli-
cations were related to graft failure greater than 6 months
after surgery (5.2 %); 2.3 % of the reported complications
were related to stiffness or scar tissue. Other reported
complications were infection (1 %), DVT (0.9 %), graft
failure less than 6 months after surgery (1.1 %), or a
combination of factors (2.3 %).
Panel II: Return to activity after anatomic ACL
reconstruction
Patients generally return to sports (starting with practice)
after an average of 6 months (range 3–9), with return to
full competition after an average of 8 months (range 4–12).
At 12 months following surgery, the panellists reported
that 75.3 % of their patients had returned to full sports
participation to a pre-injury level of activity.
The most recent study by the same group of researchers
found that 31 % of 187 athletes returned to their pre-injury
level of sport at 12 months and suggested that this low
return to competitive sports was likely influenced by psy-
chological factors [4]. Of the panellists’ patients who had
not returned to full activity at 12 months, 34.8 % of the
patients reported a fear of reinjury or a lack of confidence.
Just over a third (34.7 %) of the patients had problems
related to the knee (persistent instability, pain and/or
swelling, and rerupture) that kept them from achieving
their pre-injury level of activity and 30.5 % of the patients
simply changed their lifestyle due to family/work obliga-
tions or lost interest in active sports.
Panel III: Failure after ACL reconstruction: How
do you define it and what is your rate?
Ten of 12 panellists see their patients in the office for a
1-year post-operative visit and then on a yearly basis. Half
also reported using a yearly survey (in office or phone call)
as a part of their evaluation of surgical outcomes. Close
follow-up of patients is critical when evaluating long-term
outcomes. Just as important is the use of a consistent def-
inition of ‘‘failure’’ following ACL reconstruction, since no
strict definition of failure currently exists.
Clinical failure has generally been defined as an MRI-
documented ACL graft failure and a need for revision, or a
combination of a positive Lachman and pivot shift tests,
and/or a KT-1000 side-to-side difference of 5 mm or
greater. On this panel, ten of 12 surgeons reported using ‘‘a
need for revision’’ to define failure in the most general
sense. Regarding the indications for revisions, all 12 sur-
geons were in agreement, citing patient-reported episodes
of instability and pathological laxity on clinical examina-
tion. Eleven of 12 surgeons also used MRI evidence of a
ruptured or absent ACL graft to define failure.
The average percentage of ACL reconstructions per-
formed by the panellists that met their definition of failure
was 6.2 % (ranging from 2 to 13 %). Of these failures, the
panellists ultimately revised 4.6 % (ranging from 2 to
10 %). The 1.6 % discrepancy between the cases that met
criteria for failure and those that were actually revised
demonstrates the importance of considering multiple fac-
tors when evaluating failure, not only the need for revision.
Of the failure cases experienced by the panellists,
41.1 % were thought to be due to technical error. Another
28.3 % were related to a traumatic event or knee reinjury;
5.3 % of the cases failed because of poor graft healing and/
or incorporation; and 25.3 % of the failures resulted from a
combination of factors.
Knee Surg Sports Traumatol Arthrosc
123

Panel IV: Revision anatomic ACL reconstruction
With the number of ACL reconstructions growing annu-
ally, revision ACL surgery is also increasing and continues
to pose a challenge for all surgeons. In accordance with the
surgeons on Panel III, the surgeons of this panel attributed
the majority of their failures (39.2 %) to technical error.
Another 31.2 % were thought to be caused by a traumatic
event or knee reinjury, 7.9 % were attributed to failure of
graft healing and/or incorporation, and 21.7 % of the cases
failed due to a combination of factors.
The success of revision surgery depends on pre-opera-
tive planning. When considering revision surgery, all 12
panellists perform a thorough history and physical exami-
nation and obtain radiographs and MRI for pre-operative
planning. Nine (75 %) also use previous surgical reports,
and ten (83.3 %) obtained CT scans with or without three-
dimensional (3D) reconstructions for further characteriza-
tion of previous tunnels. One surgeon also occasionally
used a bone scan.
Surgeons preferred a one-stage revision surgery 83.7 %
of the time. Of the 12 panellists, one clearly preferred two
stages to one (4:1). Two surgeons performed both proce-
dures at comparable rates, preferring the one-stage proce-
dure slightly more than half the time. The remaining nine
surgeons performed one-stage revisions 90–100 % of the
time.
Graft choice for revisions is highly variable, even
among individual surgeons. On average, allograft was used
33.8 % of the time. Three surgeons did not use allografts at
all for revision cases. Those who did use allografts selected
from a variety of choices including bone-patellar tendon
bone, quad tendon soft tissue, Achilles tendon, tibialis
anterior, tibialis posterior, peroneus longus, and semiten-
dinosus. BTB and hamstring autografts were used 29 and
27.8 % of the time, respectively, from either the contra-
lateral leg or the ipsilateral leg if not used.
With respect to the technique used for ACL revisions,
82.2 % of the panellists’ cases are revised using a single-
bundle technique. Double-bundle techniques were utilized
17.8 % of the time. Concomitant knee injuries are com-
monly associated with ACL graft failure. Hence, many
additional procedures are performed during ACL revision.
As demonstrated in Fig. 8, nearly one-third (29.1 %) of all
revision cases require meniscectomy, 16.3 % require a
meniscal repair, and 2.6 % require meniscal transplant.
Articular cartilage procedures were performed in 16.4 % of
the cases, collateral ligament surgery in 6.8 % of the cases,
posterolateral corner reconstruction in 5 % of the cases,
and osteotomies in 6 % of the cases on average.
Panel V: Partial ACL injuries and ACL augmentation
Because only seven panellists presented on this panel, they
will remain anonymous
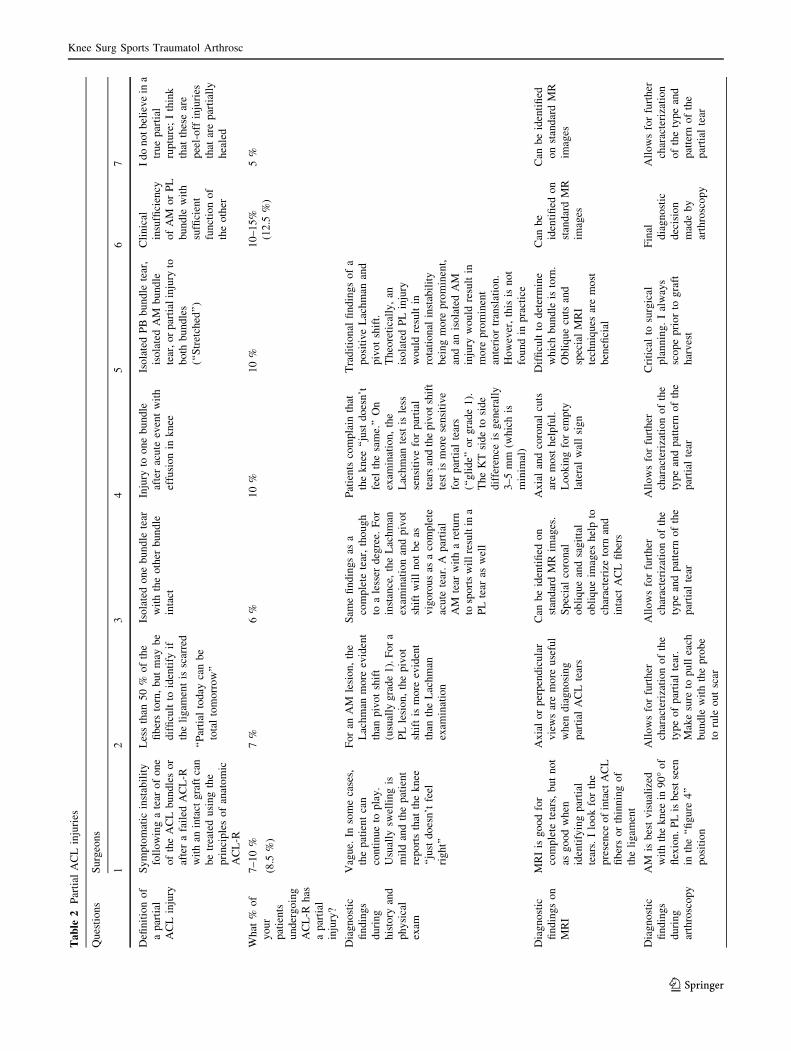
Six of seven surgeons define partial ACL injuries as an
isolated injury of the AM bundle or PL bundle—the other
being intact—resulting in clinical symptoms and episodes
of instability. Specific definitions used by each surgeon are
reported in Table 2. Interestingly, one surgeon ‘‘does not
believe in a true partial rupture’’. He suggests that diag-
nosed partial injuries are actually ‘‘peel-off injuries that
have partially healed’’. Under the consensus definition,
however, partial ACL tears are identified in 8.4 % of the
patients who undergo ACL reconstruction by the panel of
surgeons. This is a slightly lower rate of partial ACL injury
than that reported in the literature (10–20 % of all ACL
injuries) [22, 27, 33].
Regarding the preferred technique for isolated bundle
reconstruction, all seven surgeons agree that the femoral
tunnel for the bundle being reconstructed should lie in the
centre of the native insertion site of that bundle. They used
anatomic landmarks such as the intercondylar ridge, lateral
bifurcate ridge, and soft tissue remnants. On the tibial side,
the surgeons again place the isolated bundle graft in the
centre of the native insertion site. Landmarks used include
Fig. 8 Percentage of ACL
revisions that require additional
procedures
Knee Surg Sports Traumatol Arthrosc
123
Ta
ble
2P
arti
alA
CL
inju
ries
Qu
esti
on
sS
urg
eon
s
12
34
56
7
Defi
nit
ion
of
ap
arti
al
AC
Lin
jury
Sy
mp
tom
atic
inst
abil
ity
foll
ow
ing
ate
aro
fo
ne
of
the
AC
Lb
un
dle
so
r
afte
ra
fail
edA
CL
-R
wit
han
inta
ctg
raft
can
be
trea
ted
usi
ng
the
pri
nci
ple
so
fan
ato
mic
AC
L-R
Les
sth
an5
0%
of
the
fib
ers
torn
,b
ut
may
be
dif
ficu
ltto
iden
tify
if
the
lig
amen
tis
scar
red
‘‘P
arti
alto
day
can
be
tota
lto
mo
rro
w’’
Iso
late
do
ne
bu
nd
lete
ar
wit
hth
eo
ther
bu
nd
le
inta
ct
Inju
ryto
on
eb
un
dle
afte
rac
ute
even
tw
ith
effu
sio
nin
kn
ee
Iso
late
dP
Bb
un
dle
tear
,
iso
late
dA
Mb
un
dle
tear
,o
rp
arti
alin
jury
to
bo
thb
un
dle
s
(‘‘S
tret
ched
’’)
Cli
nic
al
insu
ffici
ency
of
AM
or
PL
bu
nd
lew
ith
suffi
cien
t
fun
ctio
no
f
the
oth
er
Id
on
ot
bel
iev
ein
a
tru
ep
arti
al
rup
ture
;I
thin
k
that
thes
ear
e
pee
l-o
ffin
juri
es
that
are
par
tial
ly
hea
led
Wh
at%
of
yo
ur
pat
ien
ts
un
der
go
ing
AC
L-R
has
ap
arti
al
inju
ry?
7–
10
%
(8.5
%)
7%
6%
10
%1
0%
10
–1
5%
(12
.5%
)
5%
Dia
gn
ost
ic
fin
din
gs
du
rin
g
his
tory
and
ph
ysi
cal
exam
Vag
ue.
Inso
me
case
s,
the
pat
ien
tca
n
con
tin
ue
top
lay
.
Usu
ally
swel
lin
gis
mil
dan
dth
ep
atie
nt
rep
ort
sth
atth
ek
nee
‘‘ju
std
oes
n’t
feel
rig
ht’
’
Fo
ran
AM
lesi
on
,th
e
Lac
hm
anm
ore
evid
ent
than
piv
ot
shif
t
(usu
ally
gra
de
1).
Fo
ra
PL
lesi
on
,th
ep
ivo
t
shif
tis
mo
reev
iden
t
than
the
Lac
hm
an
exam
inat
ion
Sam
efi
nd
ing
sas
a
com
ple
tete
ar,
tho
ug
h
toa
less
erd
egre
e.F
or
inst
ance
,th
eL
ach
man
exam
inat
ion
and
piv
ot
shif
tw
ill
no
tb
eas
vig
oro
us
asa
com
ple
te
acu
tete
ar.
Ap
arti
al
AM
tear
wit
ha
retu
rn
tosp
ort
sw
ill
resu
ltin
a
PL
tear
asw
ell
Pat
ien
tsco
mp
lain
that
the
kn
ee‘‘
just
do
esn
’t
feel
the
sam
e.’’
On
exam
inat
ion
,th
e
Lac
hm
ante
stis
less
sen
siti
ve
for
par
tial
tear
san
dth
ep
ivo
tsh
ift
test
ism
ore
sen
siti
ve
for
par
tial
tear
s
(‘‘g
lid
e’’
or
gra
de
1).
Th
eK
Tsi
de
tosi
de
dif
fere
nce
isg
ener
ally
3–
5m
m(w
hic
his
min
imal
)
Tra
dit
ion
alfi
nd
ing
so
fa
po
siti
ve
Lac
hm
anan
d
piv
ot
shif
t.
Th
eore
tica
lly
,an
iso
late
dP
Lin
jury
wo
uld
resu
ltin
rota
tio
nal
inst
abil
ity
bei
ng
mo
rep
rom
inen
t,
and
anis
ola
ted
AM
inju
ryw
ou
ldre
sult
in
mo
rep
rom
inen
t
ante
rio
rtr
ansl
atio
n.
Ho
wev
er,
this
isn
ot
fou
nd
inp
ract
ice
Dia
gn
ost
ic
fin
din
gs
on
MR
I
MR
Iis
go
od
for
com
ple
tete
ars,
bu
tn
ot
asg
oo
dw
hen
iden
tify
ing
par
tial
tear
s.I
loo
kfo
rth
e
pre
sen
ceo
fin
tact
AC
L
fib
ers
or
thin
nin
go
f
the
lig
amen
t
Ax
ial
or
per
pen
dic
ula
r
vie
ws
are
mo
reu
sefu
l
wh
end
iag
no
sin
g
par
tial
AC
Lte
ars
Can
be
iden
tifi
edo
n
stan
dar
dM
Rim
ages
.
Sp
ecia
lco
ron
al
ob
liq
ue
and
sag
itta
l
ob
liq
ue
imag
esh
elp
to
char
acte
rize
torn
and
inta
ctA
CL
fib
ers
Ax
ial
and
coro
nal
cuts
are
mo
sth
elp
ful.
Lo
ok
ing
for
emp
ty
late
ral
wal
lsi
gn
Dif
ficu
ltto
det
erm
ine
wh
ich
bu
nd
leis
torn
.
Ob
liq
ue
cuts
and
spec
ial
MR
I
tech
niq
ues
are
mo
st
ben
efici
al
Can
be
iden
tifi
edo
n
stan
dar
dM
R
imag
es
Can
be
iden
tifi
ed
on
stan
dar
dM
R
imag
es
Dia
gn
ost
ic
fin
din
gs
du
rin
g
arth
rosc
op
y
AM
isb
est
vis
ual
ized
wit
hth
ek
nee
in9
0�
of
flex
ion
.P
Lis
bes
tse
en
inth
e‘‘
fig
ure
4’’
po
siti
on
All
ow
sfo
rfu
rth
er
char
acte
riza
tio
no
fth
e
typ
eo
fp
arti
alte
ar.
Mak
esu
reto
pu
llea
ch
bu
nd
lew
ith
the
pro
be
toru
leo
ut
scar
All
ow
sfo
rfu
rth
er
char
acte
riza
tio
no
fth
e
typ
ean
dp
atte
rno
fth
e
par
tial
tear
All
ow
sfo
rfu
rth
er
char
acte
riza
tio
no
fth
e
typ
ean
dp
atte
rno
fth
e
par
tial
tear
Cri
tica
lto
surg
ical
pla
nn
ing
.I
alw
ays
sco
pe
pri
or
tog
raft
har
ves
t
Fin
al
dia
gn
ost
ic
dec
isio
n
mad
eb
y
arth
rosc
op
y
All
ow
sfo
rfu
rth
er
char
acte
riza
tio
n
of
the
typ
ean
d
pat
tern
of
the
par
tial
tear
Knee Surg Sports Traumatol Arthrosc
123

the soft tissue stump, the medial and lateral tibial spines,
and the posterior root of the lateral meniscus. All but one
surgeon preserve the remnants of the isolated bundle being
reconstructed.
When drilling the femoral tunnel, six surgeons prefer
using the accessory medial portal. One surgeon also
occasionally uses an inside-out technique. Six of seven
used intraoperative pictures to document tunnel location.
Four surgeons use intraoperative measurements to confirm
and document femoral tunnel location, and three are doing
the same for the tibial tunnel location. Only one uses
intraoperative radiographs (fluoroscopy) to document
femoral and tibial tunnel location, and no one is using
computer navigation. Post-operatively, five use standard
lateral and anterior–posterior knee radiographs for tunnel
documentation. Three use post-operative CT scans, and
one uses post-operative MRI.
For ACL augmentation surgery, allografts are used only
11 % of the time by the seven surgeons surveyed. Com-
monly used allografts include semitendinosus, tibialis
anterior, tibialis posterior, peroneus longus, and Achilles
tendon. Of all autografts, hamstring tendons are the most
commonly used (72.7 % of the time) followed by bone-
patellar tendon bone (14.6 %) and quadriceps tendon
(1.7 %).
The surgeons report that the complications following
ACL augmentation surgery are the same as those of pri-
mary ACL reconstruction (e.g. DVT, stiffness). In fact,
four of seven surgeons reported that they have yet to
experience any complications following augmentation, but
are currently collecting data given the increasing number of
augmentation procedures performed. Regarding outcomes,
59 % of the pooled cases have ‘‘very good’’ results and
33 % have ‘‘good’’ results. Only 8 % of the cases resulted
in ‘‘fair’’ (5 %) or ‘‘poor’’ (3 %) outcomes. No cases have
resulted in ‘‘very poor’’ (wore than post-injury) outcomes.
Discussion
The panther global summit provided a unique opportunity
for orthopaedic surgeons, physical therapists, and sports
medicine specialist to discuss current concepts, approa-
ches, and techniques in anatomic ACL reconstruction
surgery with representative perspectives from around the
world. ‘‘Anatomic’’ tunnel placement, graft choice, revi-
sion surgery, and return to sports were among the key
topics discussed.
Nearly half of the orthopaedic surgeons on Panel I
perform both single- and double-bundle techniques based
on certain patient characteristics and criteria, including
insertion site sizes, notch size, and graft size. Regarding
tunnel positioning, many surgeons use bony landmarks
such as the intercondylar ridge and the native soft tissue
insertion site on the femoral side and the medial tibial
eminence, posterior border of the lateral meniscus, and
cartilage of the medial tibial plateau on the tibial side.
Accurate femoral and tibial tunnel placement is not without
error. Some surgeons reported erring posteriorly for the
tibial footprint to reduce the risk of impingement. A recent
study by Matsubara et al. [20] evaluated the incidence of
roof impingement after anatomic placement of an ACL
graft in hyperextensible knees compared with the native
ACL in hyperextensible knees using virtual anatomic sin-
gle- and double-bundle ACL reconstructions on 3D mag-
netic resonance imaging bone models. They found that the
native ACL bows posteriorly, resulting in contact with the
intercondylar notch when the knee is hyperextended, sug-
gesting that the anterior–medial bundle roof impingement
may be unavoidable when the knee is hyperextended. The
authors supported the use of a centre-centre single-bundle
ACL reconstruction. However, other studies have demon-
strated no risk of impingement against the intercondylar
roof of the graft after anatomic double-bundle placement
[14, 15]. Furthermore, a graft in the anatomic position may
be able to remodel to account for contact with the interc-
ondylar notch, circumventing the risk for impingement.
As demonstrated by Panel II results, the time to return to
sports varied slightly among surgeons and was dependent
on individual patient progress. Panellists reported that at
12 months post-operative, 75 % of their patients returned
to full sports participation at a pre-injury level of activity.
Interestingly, Ardern et al. in a study of 503 patients who
participated in a competitive level of sports found that
67 % of patients attempted some form of sports activity by
12 months post-operatively; however, only one-third
attempted sports at a competitive level [5].
One of the most conversed issues in ACL reconstruction
surgery is the definition of failure, which is strongly
influenced by the degree of patient follow-up. Some sur-
geons closely follow patients and employ objective means
of evaluating outcomes to define ACL ‘‘failure’’. The
average percentage of failed ACL reconstructions of the
surgeons on panel III was 6.2 %, with 4.6 % of these
failures requiring revision.
The majority of the surgeons on Panel IV preferred
single-staged revisions. However, there have been no sig-
nificant differences reported—clinically or radiographi-
cally—between the two procedures [19]. Complications
such as tunnel widening, improper tunnel position, limited
range of motion, or existent hardware may necessitate a
two-stage procedure. Though clinical outcomes following
revision ACL surgery have been shown to be inferior to
those for primary ACL reconstruction [2, 11, 31], an
average of 82.2 % of the revision cases had ‘‘very good’’ or
‘‘good’’ clinical outcomes per the surgeons on Panel IV.
Knee Surg Sports Traumatol Arthrosc
123

Only 12.6 % of the revisions resulted in ‘‘fair’’ outcomes
with ‘‘no change clinically from the reinjury condition’’,
and 5.3 % resulted in ‘‘poor’’ or ‘‘very poor’’ outcomes
reflecting a clinical outcome ‘‘worse than the reinjury
condition’’.
On average, the surgeons of Panel V perform 9.7
(ranging from 5 to 20) primary AM bundle augmentations
or PL bundle reconstructions and 7.3 (ranging from 3 to 15)
primary PL bundle augmentations or AM bundle recon-
structions, annually. Only two surgeons perform revision
PL bundle augmentations: one and two per year, respec-
tively. ACL augmentation surgery is gaining in popularity
with increasing knowledge of partial injuries, more
advanced radiographic methods to detect individual bundle
tears including special oblique MRI sequences, and
research findings supporting the preservation of one intact
ACL bundle and stump for increased biomechanical sta-
bility, strength, and function; revascularization; proprio-
ceptive innervation; and graft healing, incorporation, and
remodelling [1, 6, 16, 17, 21].
Conclusions
This article summarizes the results of five panels on ana-
tomic ACL reconstruction from the 2011 panther global
summit on anatomic ACL reconstruction held in Pitts-
burgh, Pennsylvania. The data presented reflect the opin-
ions and experiences of panellists from 13 different
countries, providing an overarching global perspective on
current topics in ACL reconstruction. Though a large
majority of surgeons are performing anatomic ACL
reconstruction, variation exists for preferred technique
(single vs. double bundle), femoral and tibial tunnel posi-
tion, femoral tunnel drilling technique, and graft selection
and fixation in primary, revision, and ACL augmentation
surgery. Based on the results of this study, the majority of
surgeons prefer ‘‘anatomic’’ graft placement with tunnels
drilled in the centre of the individual bundle footprints or
between the two bundles when using a single-bundle
technique. However, a few surgeons mention that they
would place tibial tunnels slightly posterior to obviate the
risk of graft impingement on the intercondylar notch. For
primary reconstructions, most surgeons preserve ACL
remnants and the most popular graft choice is hamstring
(quadrupled semitendinosus or semitendinosus and graci-
lis) autografts. Allograft was used nearly one-third of the
time for revision surgeries, and most revision surgeries
were carried out using a single-bundle technique.
Continued prospective randomized controlled trials will
ultimately determine whether and how the controversial
topics addressed play a significant role in the long-term
outcomes following anatomic ACL reconstruction,
revision, and ACL augmentation surgery. We conclude that
symposia such as this will help further advance research,
stimulate development of solutions to common problems in
our field, and facilitate collaboration between researchers,
surgeons, and physical therapist around the world to better
serve the respective patient populations.
Acknowledgments We gratefully acknowledge each and every
panellist for their participation in this endeavour, including their
participation at the Panther Global Summit and their verification of
the data presented in this article. We would also like to acknowledge
the efforts of all University of Pittsburgh Sports Medicine research
fellows who assisted in data collection and Sara Herold for her
assistance with statistics. Finally, we would like to thank Dr. Pau
Golano for the femoral and tibial ACL insertion site dissections.
Appendix: Panel and survey questions
All responses were open ended unless specified.
General information
Demographic survey
1. Surgeon information:
a. Name
b. Company
c. City/Town
d. State/Province
e. Country
f. E-mail address
2. Total years of experience?
3. Total years of experience with primary ACL
reconstructions?
4. Total number of ACL reconstruction performed over
career?
5. Total number of ACL reconstructions performed per
year?
6. Total number of anatomic single-bundle ACL recon-
structions performed per year?
7. Total number of anatomic double-bundle ACL recon-
structions performed per year?
8. Patient demographic characteristics:
a. Age: percent in each of the following categories.
(total 100 %)
i. \14 years
ii. 14–18 years
iii. 19–24 years
iv. 25–34 years
v. 35–50 years
vi. [50 years
Knee Surg Sports Traumatol Arthrosc
123

b. Gender: percent in each of the following catego-
ries. (total 100 %)
i. Female
ii. Male
c. Level of sports participation: percent in each of the
following categories. (total 100 %)
i. High school athlete
ii. College athlete
iii. Professional athlete
iv. Recreational athlete
v. Non-athlete
d. List specific criteria for single-bundle ACL
reconstruction
e. List specific criteria for double-bundle ACL
reconstruction
Panel I: Anatomic ACL reconstruction
1. List specific indications for anatomic single and dou-
ble-bundle ACL reconstruction.
2. Preferred technique:
a. List specific criteria for location of femoral
tunnel(s).
b. List specific criteria for location of tibial tunnel(s).
c. Do you perform the following intraoperative
measurements?
i. ACL mid-substance size? Yes/no
ii. ACL insertion site size? Yes/no
iii. Intercondylar notch width? Yes/no
iv. Tunnel aperture? Yes/no
v. I do not perform any intraoperative
measurements.
d. Do you preserve ACL remnants? Yes/no
e. Do you use the following methods to create your
femoral tunnel:
i. Accessory medial portal? Yes/no
ii. Transtibial drilling? Yes/no
iii. Both techniques? Yes/no
f. Do you use the following methods to document
femoral tunnel location:
i. Intraoperative pictures/video? Yes/no
ii. Intraoperative radiographs/fluoroscopy? Yes/
no
iii. Intraoperative measurements? Yes/no
iv. Navigation? Yes/no
v. Post-operative radiographs? Yes/no
vi. Post-operative MRI? Yes/no
vii. Post-operative CT scan? Yes/no
g. Do you use the following methods to document
tibial tunnel location:
i. Intraoperative pictures/video? Yes/no
ii. Intraoperative radiographs/fluoroscopy? Yes/
no
iii. Intraoperative measurements? Yes/no
iv. Navigation? Yes/no
v. Post-operative radiographs? Yes/no
vi. Post-operative MRI? Yes/no
vii. Post-operative CT scan? Yes/no
h. What percentage of the time do you use: (total
100 %)
i. Allograft?
1 Please specify type.
ii. Autograft bone patellar tendon bone?
iii. Autograft hamstring?
iv. Autograft quad tendon?
i. What is a typical graft size you use?
j. How do you fix the graft on the femoral side?
k. How you fix the graft on the tibial side?
l. What biological methods do you use to enhance
graft healing?
i. None.
ii. PRP.
iii. Fibrin clot.
iv. Other. Please specify.
3. Results:
a. How often and when do you routinely see patients
for follow-up? List the time from surgery for all
office visits.
b. Of all surgical complications, what percentage is
due to: (total 100 %)
i. Infection.
ii DVT.
iii. Stiffness or arthrofibrosis.
iv. Graft failure at a time point less than
6 months.
v. Graft failure at a time point greater than
6 months.
vi. Other. Please specify.
vii. Percent of surgeries without complications.
c. Do you use the following methods to assess
outcome?
i. Range of motion? Yes/no
ii. Manual/instrumented laxity? Yes/no
Knee Surg Sports Traumatol Arthrosc
123

iii. Radiographs? Yes/no
iv. MRI? Yes/no
v. CT scan? Yes/no
vi. Patient reported outcomes? Yes/no
vii. Other? Please specify.
Panel II: Rehabilitation and return to activity: When
do you allow your athletes to return to sports?
1. Do you use the following criteria to determine readi-
ness for return to sports activity?
a. Time from surgery? Yes/no
b. Absence of pain and swelling? Yes/no
c. Range of motion? Yes/no
d. Laxity upon examination? Yes/no
e. Strength? Yes/no
f. Functional testing? Yes/no
g. Other. Please specify.
2. Do you consider graft healing when making the return
to play decision? Yes/no
3. If yes, how do you determine graft healing? Check all
that apply.
a. Time from surgery.
b. Laxity.
c. Graft appearance on MRI.
d. Other. Please specify.
4. When do you allow your athletes to return to the
following activities? Respond in months.
a. Running?
b. Jumping, cutting, and pivoting?
c. Practice?
d. Competition?
e. Physical work/labor?
5. At 12 months after surgery, what percentage of your
patients return to: (total 100 %)
a. Full participation?
b. Partial participation?
c. No participation at 12 months?
6. For those patients who do not return to full activity,
what is the reason? (total 100 %)
a. Problems related to the knee?
b. Fear of re-injury/lack of confidence?
c. Personal choice: changes in lifestyle due to family
or work obligations?
d. Other. Please specify.
Panel III: Failure after anatomic ACL reconstruction
1. Do you use the methods below to follow your patient’s
to evaluate your rate of failure after primary anatomic
ACL reconstruction?
a. Yearly survey or phone call? Yes/no
b. Yearly office visit? Yes/no
c. Recommendations to return to the office as
needed? Yes/no
2. Do you use the following criteria to identify failure
after anatomic ACL reconstruction?
a. Complaints of instability? Yes/No
b. Pathological laxity? Yes/No
c. MRI evidence of graft failure? Yes/No
d. Need for revision? Yes/No
e. Other. Please specify.
3. What is your definition of ACL reconstruction ‘‘fail-
ure?’’ Please be specific.
4. What percentage of your own anatomic ACL recon-
structions meets your definition of failure?
5. What percentage of your own anatomic ACL recon-
structions do you revise?
6. Of all failure cases that you see, what percentage is due
to: (total 100 %)
a. Technical error?
b. Trauma or re-injury?
c. Failure of graft healing/incorporation?
d. Combination of above factors?
Panel IV: Revision anatomic ACL reconstruction
1. Do you consider the following factors in preoperative
planning?
a. History and physical exam? Yes/no
b. Prior operative report? Yes/no
c. Radiographs? Yes/no
d. MRI? Yes/no
e. CT Scan? Yes/no
f. Other. Please specify.
2. What percentage of your revisions is: (total 100 %)
a. One staged?
b. Two staged?
3. What percentage of the time do you use: (total 100 %)
a. Allograft?
Knee Surg Sports Traumatol Arthrosc
123

i. Please specify type.
b. Autograft bone patellar tendon bone?
c. Autograft hamstring?
d. Autograft quad tendon?
4. What percent of revisions are: (total 100 %)
a. Single-bundle?
b. Double-bundle?
5. What percent of your ACL reconstruction require:
(total does not have to be 100 %)
a. Meniscectomy?
b. Meniscus repair?
c. Meniscal transplant?
d. Collateral ligament surgery?
e. Posterolateral corner surgery?
f. Articular cartilage procedure?
g. Osteotomy?
h. Other: please specify.
6. What complications have you observed with revision
ACL reconstruction?
7. How would you qualify your outcomes? (total 100 %)
a. Very good (like pre-primary injury condition)?
b. Good (same as pre-re-injury condition)?
c. Fair?
d. Poor (no change from re-injury condition)?
e. Very poor (worse than re-injury condition)?
Panel V: Partial ACL injuries and ACL augmentation
1. What is your definition of a partial ACL injury?
2. Explain how you make your diagnosis using each of
the modalities below:
a. History and Physical exam.
b. MRI.
c. Arthroscopy.
3. What percentage of patients undergoing ACL surgery
has a partial ACL injury?
4. How many of the following ACL augmentation types
do you perform a year?
a. Primary augmentation of the AM bundle (PL
reconstruction)?
b. Primary augmentation of the PL bundle (AM
reconstruction)?
c. Revision augmentation of the AM bundle (PL
reconstruction)?
d. Revision augmentation of the PL bundle (AM
reconstruction)?
5. List your specific criteria for location of femoral
tunnel(s).
6. List your specific criteria for location of tibial
tunnel(s).
7. Do you use the following intraoperative
measurements?
a. ACL mid-substand size? Yes/no
b. ACL insertion site size? Yes/no
c. Intercondylar notch width? Yes/no
d. Tunnel aperture? Yes/no
e. I do not use intraoperative measurements.
8. Do you preserve ACL remnants? Yes/no
9. Do you preserve the ACL stump? Yes/no
10. Do you use the following methods to create the
femoral tunnel?
a. Accessory medial portal? Yes/no
b. Transtibial drilling? Yes/no
c. Both techniques? Yes/no
11. Do you use the following methods to document
femoral tunnel location:
a. Intraoperative pictures/video? Yes/no
b. Intraoperative radiographs/fluoroscopy? Yes/no
c. Intraoperative measurements? Yes/no
d. Navigation? Yes/no
e. Post-operative radiographs? Yes/no
f. Post-operative MRI? Yes/no
g. Post-operative CT scan? Yes/no
12. Do you use the following methods to document tibial
tunnel location:
a. Intraoperative pictures/video? Yes/no
b. Intraoperative radiographs/fluoroscopy? Yes/no
c. Intraoperative measurements? Yes/no
d. Navigation? Yes/no
e. Post-operative radiographs? Yes/no
f. Post-operative MRI? Yes/no
g. Post-operative CT scan? Yes/no
13. Please specify your tunnel location and method for
creating tunnels.
14. What percentage of the time do you use: (total
100 %)
a. Allograft?
i. Please specify type.
b. Autograft bone patellar tendon bone?
c. Autograft hamstring?
d. Autograft quad tendon?
Knee Surg Sports Traumatol Arthrosc
123

15. What complications have you encountered?
16. How would you qualify your outcomes? (total
100 %)
a. Very good (like pre-primary injury condition)?
b. Good (same as pre-re-injury condition)?
c. Fair?
d. Poor (no change from re-injury condition)?
e. Very poor (worse than re-injury condition)?
References
1. Adachi N, Ochi M, Uchio Y, Sumen Y (2000) Anterior cruciate
ligament augmentation under arthroscopy. A minimum 2-year
follow-up in 40 patients. Arch Orthop Trauma Surg
120(3–4):128–133
2. Ahlden M, Samuelsson K, Sernert N, Forssblad M, Karlsson J,
Kartus J (2013) The Swedish national anterior cruciate ligament
register: a report on baseline variables and outcomes of surgery
for almost 18,000 patients. Am J Sports Med 40(10):2230–2235
3. Ahlden M, Sernert N, Karlsson J, Kartus J (2013) A prospective
randomized study comparing double- and single-bundle tech-
niques for anterior cruciate ligament reconstruction. Am J Sports
Med 41(11):2484–2491
4. Ardern CL, Taylor NF, Feller JA, Whitehead TS, Webster KE
(2013) Psychological responses matter in returning to pre-injury
level of sport after anterior cruciate ligament reconstruction
surgery. Am J Sports Med 41(7):1549–1558
5. Ardern CL, Webster KE, Taylor NF, Feller JA (2011) Return to
sport following anterior cruciate ligament reconstruction surgery:
a systematic review and meta-analysis of the state of play. Br J
Sports Med 45(7):596–606
6. Borbon CA, Mouzopoulos G, Siebold R (2012) Why perform an
ACL augmentation? Knee Surg Sports Traumatol Arthrosc
20(2):245–251
7. Bray RC, Leonard CA, Salo PT (2002) Vascular physiology and
long-term healing of partial ligament tears. J Orthop Res
20(5):984–989
8. Brown CH Jr, Spalding T, Robb C (2013) Medial portal tech-
nique for single-bundle anatomical anterior cruciate ligament
(ACL) reconstruction. Int Orthop 37(2):253–269
9. Buoncristiani AM, Tjoumakaris FP, Starman JS, Ferretti M, Fu
FH (2006) Anatomic double-bundle anterior cruciate ligament
reconstruction. Arthroscopy 22(9):1000–1006
10. Gianotti SM, Marshall SW, Hume PA, Bunt L (2009) Incidence
of anterior cruciate ligament injury and other knee ligament
injuries: a national population based study. J Sci Med Sport
12(6):622–627
11. Gifstad T, Drogset JO, Viset A, Grontvedt T, Hortemo GS (2013)
Inferior results after revision ACL reconstructions: a comparison
with primary ACL reconstructions. Knee Surg Sports Traumatol
Arthrosc 21(9):2011–2018
12. Hussein M, van Eck CF, Cretnik A, Dinevski D, Fu FH (2012)
Prospective randomized clinical evaluation of conventional sin-
gle-bundle, anatomic single-bundle, and anatomic double-bundle
anterior cruciate ligament reconstruction: 281 cases with 3- to
5-year follow-up. Am J Sports Med 40(3):512–520
13. Illingworth KD, Hensler D, Working ZM, Macalena JA, Tash-
man S, Fu FH (2011) A simple evaluation of anterior cruciate
ligament femoral tunnel position: the inclination angle and fem-
oral tunnel angle. Am J Sports Med 39(12):2611–2618
14. Iriuchishima T, Horaguchi T, Kubomura T, Morimoto Y, Fu FH
(2011) Evaluation of the intercondylar roof impingement after
anatomical double-bundle anterior cruciate ligament reconstruc-
tion using 3D-CT. Knee Surg Sports Traumatol Arthrosc
19(4):674–679
15. Iriuchishima T, Tajima G, Ingham SJ, Shen W, Smolinski P, Fu
FH (2010) Impingement pressure in the anatomical and non-
anatomical anterior cruciate ligament reconstruction: a cadaver
study. Am J Sports Med 38(8):1611–1617
16. Kazusa H, Nakamae A, Ochi M (2013) Augmentation technique
for anterior cruciate ligament injury. Clin Sports Med
32(1):127–140
17. Lee BI, Min KD, Choi HS, Kwon SW, Chun DI, Yun ES, Lee
DW, Jin SY, Yoo JH (2009) Immunohistochemical study of
mechanoreceptors in the tibial remnant of the ruptured anterior
cruciate ligament in human knees. Knee Surg Sports Traumatol
Arthrosc 17(9):1095–1101
18. Magnussen RA, Lawrence JT, West RL, Toth AP, Taylor DC,
Garrett WE (2012) Graft size and patient age are predictors of
early revision after anterior cruciate ligament reconstruction with
hamstring autograft. Arthroscopy 28(4):526–531
19. Marquass B, Engel T, Hepp P, Theopold JD, Josten C (2007)
One- and two-stage procedure for revision after failure of anterior
cruciate ligament reconstruction. Z Orthop Unfall
145(6):712–718
20. Matsubara H, Okazaki K, Tashiro Y, Toyoda K, Uemura M,
Hashizume M, Iwamoto Y (2013) Intercondylar roof impinge-
ment after anatomic double-bundle anterior cruciate ligament
reconstruction in patients with knee hyperextension. Am J Sports
Med 41(12):2819–2827
21. Murray MM, Martin SD, Martin TL, Spector M (2000) Histo-
logical changes in the human anterior cruciate ligament after
rupture. J Bone Joint Surg Am 82-A(10):1387–1397
22. Ochi M, Adachi N, Deie M, Kanaya A (2006) Anterior cruciate
ligament augmentation procedure with a 1 incision technique:
anteromedial bundle or posterolateral bundle reconstruction.
Arthroscopy 22(4):e461–e465
23. Papalia R, Franceschi F, Vasta S, Di Martino A, Maffulli N,
Denaro V (2012) Sparing the anterior cruciate ligament remnant:
is it worth the hassle? Br Med Bull 104:91–111
24. Park SY, Oh H, Park S, Lee JH, Lee SH, Yoon KH (2012) Factors
predicting hamstring tendon autograft diameters and resulting
failure rates after anterior cruciate ligament reconstruction. Knee
Surg Sports Traumatol Arthrosc
25. Siebold R (2011) The concept of complete footprint restoration
with guidelines for single- and double-bundle ACL reconstruc-
tion. Knee Surg Sports Traumatol Arthrosc 19(5):699–706
26. Song EK, Seon JK, Yim JH, Woo SH, Seo HY, Lee KB (2013)
Progression of osteoarthritis after double- and single-bundle
anterior cruciate ligament reconstruction. Am J Sports Med
41(10):2340–2346
27. Sonnery-Cottet B, Barth J, Graveleau N, Fournier Y, Hager JP,
Chambat P (2009) Arthroscopic identification of isolated tear of
the posterolateral bundle of the anterior cruciate ligament.
Arthroscopy 25(7):728–732
28. Survey monkey (1999–2012). http://www.surveymonkey.com.
Accessed 9 Sep 2012
29. van Eck CF, Lesniak BP, Schreiber VM, Fu FH (2010) Anatomic
single- and double-bundle anterior cruciate ligament reconstruc-
tion flowchart. Arthroscopy 26(2):258–268
30. van Eck CF, Schreiber VM, Liu TT, Fu FH (2010) The anatomic
approach to primary, revision and augmentation anterior cruciate
ligament reconstruction. Knee Surg Sports Traumatol Arthrosc
18(9):1154–1163
31. Weiler A, Schmeling A, Stohr I, Kaab MJ, Wagner M (2007)
Primary versus single-stage revision anterior cruciate ligament
Knee Surg Sports Traumatol Arthrosc
123

reconstruction using autologous hamstring tendon grafts: a pro-
spective matched-group analysis. Am J Sports Med 35(10):
1643–1652
32. Wu B, Zhao Z, Li S, Sun L (2013) Preservation of remnant
attachment improves graft healing in a rabbit model of anterior
cruciate ligament reconstruction. Arthroscopy 29(8):1362–1371
33. Zantop T, Brucker PU, Vidal A, Zelle BA, Fu FH (2007) Intra-
articular rupture pattern of the ACL. Clin Orthop Relat Res
454:48–53
Knee Surg Sports Traumatol Arthrosc
123












![The Evolution of Anatomic Anterior Cruciate Ligament ... · The Evolution of Anatomic Anterior Cruciate Ligament Reconstruction ... tunnel placement in the axial plane [23]. These](https://img.dokumen.tips/doc/110x75/5f03ed437e708231d40b74ae/the-evolution-of-anatomic-anterior-cruciate-ligament-the-evolution-of-anatomic.jpg)
















