Embed Size (px)
Citation preview

Cancer Immun 1424
Cancer Immunity (27 Copyright © 2008 by V
-9634Academy of Cancer Immunology
www.cancerimmunity.org
080207
Commentary
An unusual case of metastatic melanoma sensitive to chemotherapy and immunotherapy, with late immune escape in the brain
Verena Voelter1*, Alessia Pica2, Julien Laurent3, Donata Rimoldi4, Hanifa Bouzourene5, Ali Sajadi6, Maurice Matter7, PedroRomero4, Nathalie Rufer3,8** and Daniel E. Speiser4,8**1Multidisciplinary Oncology Center, University of Lausanne Hospitals (CHUV), Lausanne, Switzerland2Department of Radio-Oncology, CHUV, Lausanne, Switzerland3Division of Experimental Oncology, Multidisciplinary Oncology Center, CHUV, Lausanne, Switzerland4Division of Clinical Onco-Immunology, Ludwig Institute for Cancer Research, Lausanne Branch, Lausanne, Switzerland5Department of Pathology, CHUV, Lausanne, Switzerland6Centre Universitaire Romand de Neurochirurgie, CHUV, Lausanne, Switzerland7Department of Surgery, CHUV, Lausanne, Switzerland8Swiss National Center of Competence in Research (NCCR) Molecular Oncology, Lausanne, Switzerland*Present address: Celgene International, Route de Perreux 1, 2017 Boudry, Switzerland**These authors contributed equally to this work
March 2008) Vol. 8, p. 6 erena Voelter
Keywords: human, melanoma, cellular immunity, tumor escape
IntroductionThe incidence of skin melanoma is increasing worldwide with
little or no improvement in mortality despite intensive research and treatment. Following the appearance of distant metastases overall survival rarely exceeds one year. For metastatic disease, single agent chemotherapy with dacarbazine (DTIC) or temozolomide (TMZ) remains the standard of care and combination with cisplatin (CDDP) or biochemotherapy, including interleukin-2 and interferon-alpha, has failed to improve survival in randomized trials (1-3). Nevertheless, a role for the patients' immune system has long been advocated based on observations of spontaneous disease remissions and immune responses (4). Here, we report on an unusual course of metastatic melanoma with documentation of a tumor antigen-specific immune response and synergy with chemotherapy, as well as the subsequent intracranial tumor escape.
Case reportPatient LAU 672, a 34-year old man, was diagnosed with a thin
nodular melanoma in the left lower back in 1999. The tumor was resected with a 1 cm margin and the tumor stage classified as IA. During the following 5 years, the disease recurred six times, always in the left iliac and inguinal lymph node region, and was treated repeatedly with resection and irradiation. In addition, repeated Melan-A vaccines were administered (see below). In early 2004, the disease entered an accelerated phase and, within a few weeks, metastatic involvement of multiple sites (lung, liver, bone, lymph nodes and subcutaneous tissue) was documented (Figure 1A). Systemic chemotherapy with DTIC and CDDP promptly induced tumor regression. A partial remission was radiologically confirmed after 3 cycles, which converted into a complete remission (CR) after 8 cycles. Surprisingly, until the patient's death in 2007, the disease never recurred at locations
that had been previously infiltrated by large tumor masses, including the left inguinal area which harbored a mass of almost 10 cm, as well as the lung and liver. A lytic bone lesion in the second vertebra completely consolidated after irradiation, chemotherapy and treatment with biphosphonates.
This exquisite and unusual chemosensitivity was counterbalanced by rapid disease recurrence as soon as systemic therapy was suspended. In spring 2005, 10 weeks after the last chemotherapy treatment, new disease progression was noted with rapidly growing subcutaneous (s.c.) metastases. A synchronous cerebral metastasis in the left hemisphere was treated with radiosurgery and subsequently completely disappeared and never recurred. In parallel, second line chemotherapy was started using TMZ and CDDP leading, again, to swift tumor response with regression of s.c. nodules in a few days. After 3 cycles, the patient reached a partial remission and continued on TMZ (150 mg/m2, 5 days every 4 weeks) for another year until September 2006, when a new brain metastasis in the right cerebral hemisphere appeared. This metastasis did not respond to immunotherapy (see below), nor to repeated surgery. Finally, in July 2007, the patient died of cerebral edema due to progressive metastatic involvement (Figure 1A) and brain stem compression, but without evidence of extracranial disease.
Correlative immunological findingsIn addition to the particular chemosensitivity of the disease,
there is evidence that the patient's immune system contributed to successful disease control. In 2002, a spontaneous antitumor immune response was detected, with approximately 0.03% of CD8 T cells specific for the melanoma antigen Melan-A/Mart-1 (Figure 1B). These cells expanded vigorously in vitro. Vaccination with the Melan-A peptide and incomplete Freund's adjuvant (IFA) in 2002 (5), further supplemented with CpG oligonucleotides in 2003/2004 (6), induced strong proliferation of Melan-A specific T cells also in vivo (Figure 1B), resulting in high T cell frequencies (i.e. comparable to the frequencies
1 of 4
Cancer Immunity (27 March 2008) Vol. 8, p. 6
Figure 1
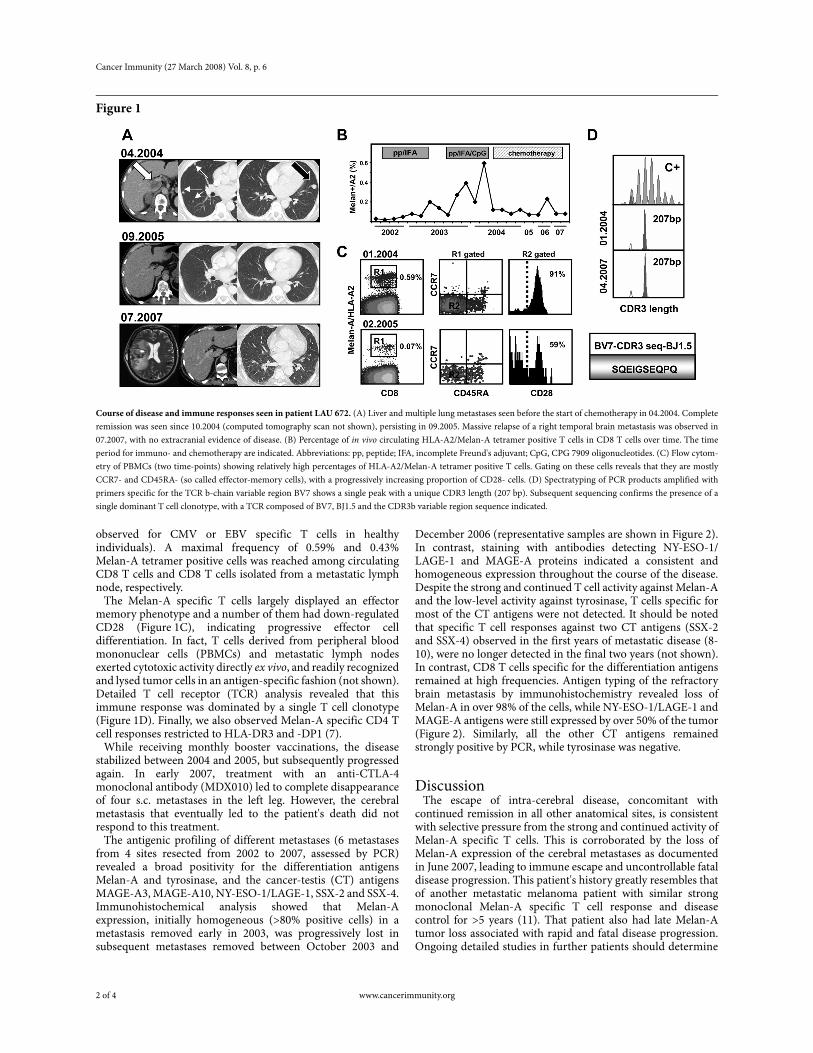
Course of disease and immune responses seen in patient LAU 672. (A) Liver and multiple lung metastases seen before the start of chemotherapy in 04.2004. Complete remission was seen since 10.2004 (computed tomography scan not shown), persisting in 09.2005. Massive relapse of a right temporal brain metastasis was observed in 07.2007, with no extracranial evidence of disease. (B) Percentage of in vivo circulating HLA-A2/Melan-A tetramer positive T cells in CD8 T cells over time. The time period for immuno- and chemotherapy are indicated. Abbreviations: pp, peptide; IFA, incomplete Freund's adjuvant; CpG, CPG 7909 oligonucleotides. (C) Flow cytom-etry of PBMCs (two time-points) showing relatively high percentages of HLA-A2/Melan-A tetramer positive T cells. Gating on these cells reveals that they are mostly CCR7- and CD45RA- (so called effector-memory cells), with a progressively increasing proportion of CD28- cells. (D) Spectratyping of PCR products amplified with primers specific for the TCR b-chain variable region BV7 shows a single peak with a unique CDR3 length (207 bp). Subsequent sequencing confirms the presence of a single dominant T cell clonotype, with a TCR composed of BV7, BJ1.5 and the CDR3b variable region sequence indicated.
observed for CMV or EBV specific T cells in healthy individuals). A maximal frequency of 0.59% and 0.43% Melan-A tetramer positive cells was reached among circulating CD8 T cells and CD8 T cells isolated from a metastatic lymph node, respectively.
The Melan-A specific T cells largely displayed an effector memory phenotype and a number of them had down-regulated CD28 (Figure 1C), indicating progressive effector cell differentiation. In fact, T cells derived from peripheral blood mononuclear cells (PBMCs) and metastatic lymph nodes exerted cytotoxic activity directly ex vivo, and readily recognized and lysed tumor cells in an antigen-specific fashion (not shown). Detailed T cell receptor (TCR) analysis revealed that this immune response was dominated by a single T cell clonotype (Figure 1D). Finally, we also observed Melan-A specific CD4 T cell responses restricted to HLA-DR3 and -DP1 (7).
While receiving monthly booster vaccinations, the disease stabilized between 2004 and 2005, but subsequently progressed again. In early 2007, treatment with an anti-CTLA-4 monoclonal antibody (MDX010) led to complete disappearance of four s.c. metastases in the left leg. However, the cerebral metastasis that eventually led to the patient's death did not respond to this treatment.
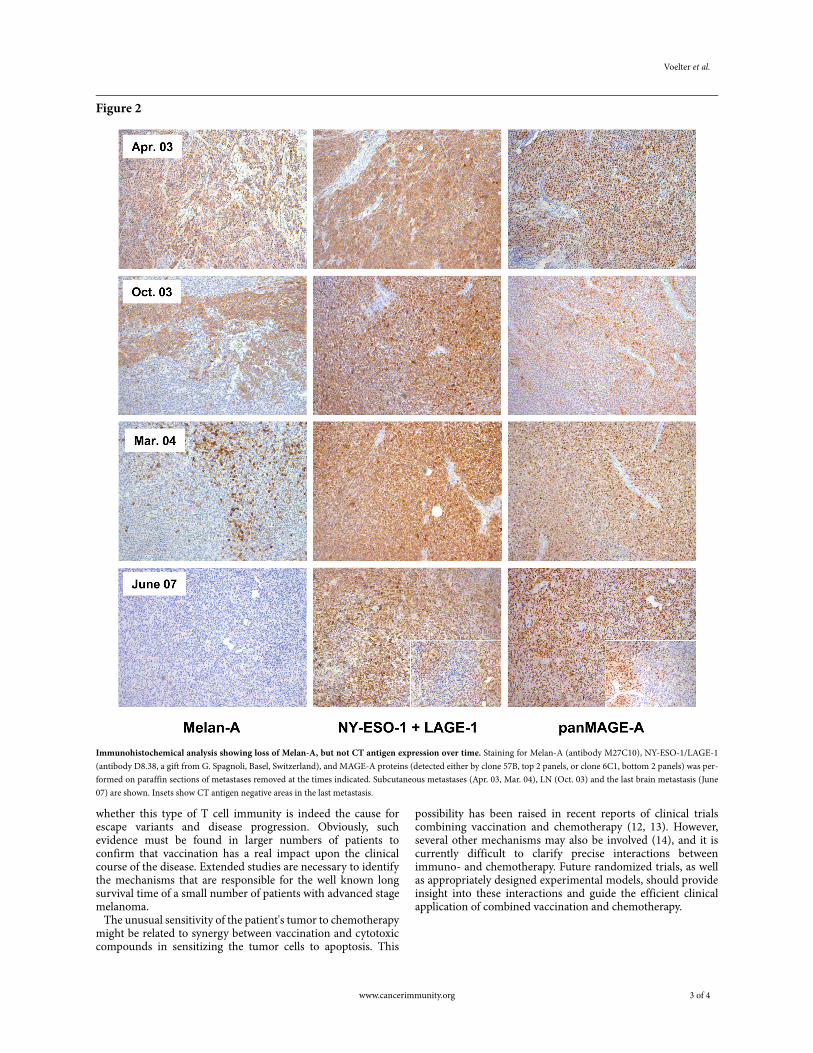
The antigenic profiling of different metastases (6 metastases from 4 sites resected from 2002 to 2007, assessed by PCR) revealed a broad positivity for the differentiation antigens Melan-A and tyrosinase, and the cancer-testis (CT) antigens MAGE-A3, MAGE-A10, NY-ESO-1/LAGE-1, SSX-2 and SSX-4. Immunohistochemical analysis showed that Melan-A expression, initially homogeneous (>80% positive cells) in a metastasis removed early in 2003, was progressively lost in subsequent metastases removed between October 2003 and
December 2006 (representative samples are shown in Figure 2). In contrast, staining with antibodies detecting NY-ESO-1/LAGE-1 and MAGE-A proteins indicated a consistent and homogeneous expression throughout the course of the disease. Despite the strong and continued T cell activity against Melan-A and the low-level activity against tyrosinase, T cells specific for most of the CT antigens were not detected. It should be noted that specific T cell responses against two CT antigens (SSX-2 and SSX-4) observed in the first years of metastatic disease (8-10), were no longer detected in the final two years (not shown). In contrast, CD8 T cells specific for the differentiation antigens remained at high frequencies. Antigen typing of the refractory brain metastasis by immunohistochemistry revealed loss of Melan-A in over 98% of the cells, while NY-ESO-1/LAGE-1 and MAGE-A antigens were still expressed by over 50% of the tumor (Figure 2). Similarly, all the other CT antigens remained strongly positive by PCR, while tyrosinase was negative.
DiscussionThe escape of intra-cerebral disease, concomitant with
continued remission in all other anatomical sites, is consistent with selective pressure from the strong and continued activity of Melan-A specific T cells. This is corroborated by the loss of Melan-A expression of the cerebral metastases as documented in June 2007, leading to immune escape and uncontrollable fatal disease progression. This patient's history greatly resembles that of another metastatic melanoma patient with similar strong monoclonal Melan-A specific T cell response and disease control for >5 years (11). That patient also had late Melan-A tumor loss associated with rapid and fatal disease progression. Ongoing detailed studies in further patients should determine
2 of 4 www.cancerimmunity.org
Voelter et al.
Figure 2
Immunohistochemical analysis showing loss of Melan-A, but not CT antigen expression over time. Staining for Melan-A (antibody M27C10), NY-ESO-1/LAGE-1 (antibody D8.38, a gift from G. Spagnoli, Basel, Switzerland), and MAGE-A proteins (detected either by clone 57B, top 2 panels, or clone 6C1, bottom 2 panels) was per-formed on paraffin sections of metastases removed at the times indicated. Subcutaneous metastases (Apr. 03, Mar. 04), LN (Oct. 03) and the last brain metastasis (June 07) are shown. Insets show CT antigen negative areas in the last metastasis.
whether this type of T cell immunity is indeed the cause for escape variants and disease progression. Obviously, such evidence must be found in larger numbers of patients to confirm that vaccination has a real impact upon the clinical course of the disease. Extended studies are necessary to identify the mechanisms that are responsible for the well known long survival time of a small number of patients with advanced stage melanoma.
The unusual sensitivity of the patient's tumor to chemotherapy might be related to synergy between vaccination and cytotoxic compounds in sensitizing the tumor cells to apoptosis. This
possibility has been raised in recent reports of clinical trials combining vaccination and chemotherapy (12, 13). However, several other mechanisms may also be involved (14), and it is currently difficult to clarify precise interactions between immuno- and chemotherapy. Future randomized trials, as well as appropriately designed experimental models, should provide insight into these interactions and guide the efficient clinical application of combined vaccination and chemotherapy.
www.cancerimmunity.org 3 of 4

Cancer Immunity (27 March 2008) Vol. 8, p. 6
AcknowledgementsWe are particularly grateful to the patient and his family who
remained optimistic and positive during all these years of relapsing-remitting disease. He was always convinced of the necessity of clinical and translational research and supported every available research program. During the last months of his life he consented to the publication of his extraordinary story.
References1. Chapman PB, Einhorn LH, Meyers ML, Saxman S, Destro AN,
Panageas KS, Begg CB, Agarwala SS, Schuchter LM, Ernstoff MS, Houghton AN, Kirkwood JM. Phase III multicenter randomized trial of the Dartmouth regimen versus dacarbazine in patients with metastatic melanoma. J Clin Oncol 1999; 17: 2745-2751. (PMID: 10561349)
2. Middleton MR, Grob JJ, Aaronson N, Fierlbeck G, Tilgen W, SeiterS, Gore M, Aamdal S, Cebon J, Coates A, Dreno B, Henz M, Scha-dendorf D, Kapp A, Weiss J, Fraass U, Statkevich P, Muller M, Thatcher N. Randomized phase III study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant melanoma. J Clin Oncol 2000; 18: 158-166. (PMID: 10623706)
3. Keilholz U, Punt CJ, Gore M, Kruit W, Patel P, Lienard D, ThomasJ, Proebstle TM, Schmittel A, Schadendorf D, Velu T, Negrier S, Kleeberg U, Lehman F, Suciu S, Eggermont AM. Dacarbazine, cis-platin, and interferon-alfa-2b with or without interleukin-2 in meta-static melanoma: a randomized phase III trial (18951) of the European Organisation for Research and Treatment of Cancer Mel-anoma Group. J Clin Oncol 2005; 23: 6747-6755. (PMID: 16170182)
4. Rosenberg SA. Shedding light on immunotherapy for cancer. N Engl J Med 2004; 350: 1461-1463. (PMID: 15070799)
5. Lienard D, Rimoldi D, Marchand M, Dietrich PY, van Baren N, Geldhof C, Batard P, Guillaume P, Ayyoub M, Pittet MJ, ZippeliusA, Fleischhauer K, Lejeune F, Cerottini JC, Romero P, Speiser DE. Ex vivo detectable activation of Melan-A-specific T cells correlating with inflammatory skin reactions in melanoma patients vaccinated with peptides in IFA. Cancer Immun 2004; 4: 4. URL: http://www.cancerimmunity.org/v4p4/040404.htm
6. Speiser DE, Lienard D, Rufer N, Rubio-Godoy V, Rimoldi D, Lejeune F, Krieg AM, Cerottini JC, Romero P. Rapid and strong human CD8+ T cell responses to vaccination with peptide, IFA, and CpG oligodeoxynucleotide 7909. J Clin Invest 2005; 115: 739-746. (PMID: 15696196)
7. Bioley G, Jandus C, Tuyaerts S, Rimoldi D, Kwok WW, Speiser DE, Tiercy JM, Thielemans K, Cerottini JC, Romero P. Melan-A/MART-1-specific CD4 T cells in melanoma patients: identification of new epitopes and ex vivo visualization of specific T cells by MHC class II tetramers. J Immunol 2006; 177: 6769-6779. (PMID: 17082590)
8. Ayyoub M, Rimoldi D, Guillaume P, Romero P, Cerottini JC, Val-mori D, Speiser D. Tumor-reactive, SSX-2-specific CD8+ T cells are selectively expanded during immune responses to antigen-express-ing tumors in melanoma patients. Cancer Res 2003; 63: 5601-5606. (PMID: 14500401)
9. Ayyoub M, Hesdorffer CS, Montes M, Merlo A, Speiser D, RimoldiD, Cerottini JC, Ritter G, Scanlan M, Old LJ, Valmori D. An immu-nodominant SSX-2-derived epitope recognized by CD4+ T cells in association with HLA-DR. J Clin Invest 2004; 113: 1225-1233. (PMID: 15085202)
10. Ayyoub M, Merlo A, Hesdorffer CS, Rimoldi D, Speiser D, CerottiniJC, Chen YT, Old LJ, Stevanovic S, Valmori D. CD4+ T cell responses to SSX-4 in melanoma patients. J Immunol 2005; 174: 5092-5099. (PMID: 15814740)
11. Speiser DE, Baumgaertner P, Barbey C, Rubio-Godoy V, Moulin A, Corthesy P, Devevre E, Dietrich PY, Rimoldi D, Lienard D, Cerot-tini JC, Romero P, Rufer N. A novel approach to characterize clonality and differentiation of human melanoma-specific T cell responses: spontaneous priming and efficient boosting by vaccina-tion. J Immunol 2006; 177: 1338-1348. (PMID: 16818795)
12. Wheeler CJ, Das A, Liu G, Yu JS, Black KL. Clinical responsiveness of glioblastoma multiforme to chemotherapy after vaccination. Clin Cancer Res 2004; 10: 5316-5326. (PMID: 15328167)
13. Antonia SJ, Mirza N, Fricke I, Chiappori A, Thompson P, WilliamsN, Bepler G, Simon G, Janssen W, Lee JH, Menander K, Chada S, Gabrilovich DI. Combination of p53 cancer vaccine with chemo-therapy in patients with extensive stage small cell lung cancer. Clin Cancer Res 2006; 12: 878-887. (PMID: 16467102)
14. Gabrilovich DI. Combination of chemotherapy and immunother-apy for cancer: a paradigm revisited. Lancet Oncol 2007; 8: 2-3. (PMID: 17196504)
ContactAddress correspondence to:
Verena Voelter, MDCelgene InternationalRoute de Perreux 12017 BoudrySwitzerlandE-mail: [email protected]
4 of 4 www.cancerimmunity.org





























